
Abstract
Objective
To compare the knee shape and bone parameters between knee prosthesis products from overseas companies and a Chinese patient’s knee, and to apply the anatomical basis for Chinese knee prosthesis design.
Methods
Three-dimensional digital models were built, including prosthesis products for a normal adult. The relevant anatomy index was measured, and physical parameter, radiographic, geometric, knee kinematic, and distal geometry data were collected on the femur and tibia.
Results
The width of the femoral condyle (WFC), width of the medial femoral condyle (WMFC), width of the lateral femoral condyle (WLFC), depth of the intercondylar fossa (DICF), sagittal length of the medial femoral condyle (SLMFC), sagittal length of the lateral femoral condyle (SLLFC), angle of the medial femoral condyle (AMFC), and angle of the lateral femoral condyle (ALFC) in the femur and the transverse diameter (ML) and anteroposterior diameter (AP) of the tibial bone were measured. These parameters were significantly lower in the normal group compared with the prosthesis product model group.
Conclusion
When using an imported knee prosthesis, the osteotomy angle may not fit perfectly. Use of an imported prosthesis may be an important factor in the increasing failure of knee arthroplasty in China.
Keywords
Introduction
There is an increasing number of Chinese patients with osteoarthritis who undergo total knee arthroplasty (TKA).1,2 TKA is a precise procedure and requires accurate bone cutting, adequate balancing of the soft tissues and proper coverage of the resected bony surface on the components to achieve a successful outcome.3,4 It has become a frequent orthopedic operation for the Asian–Pacific population.
Compared with their Western counterparts, the Asian sub-population has a smaller construction and stature, leading to the problem of an implant size mismatch with the resected bony surface in Asian patients. Most prosthesis used in China come from Western countries, and the prosthesis size and shape are mainly for foreigners and not for Chinese people.5,6 It is known that Asians are often shorter and smaller than Caucasians. It is necessary to take measurement from Chinese knees to design and select the right knee prosthesis size.
Compared with the femoral component, the tibial prosthesis in TKA was more likely to induce complications.7,8 It is important to properly measure the size of the prosthesis to the cut surface of the distal femur and proximal tibia to achieve the highest stability and longevity for the implant. Anthropometric data are lacking for the distal femur and proximal tibia in Asian populations. An element that matches the anthropometrics of the Chinese population may improve the surgical effect.
Materials and methods
Inclusion criteria
The volunteers were healthy adults from the Han and Xinjiang Ugyur ethnic groups. X-ray examination of patients without congenital malformations and lesions included the length from the medial proximal tibia to the medial malleolus.9,10 The study was approved by the First Affiliated Hospital of Kashi Area. Written informed consent was obtained from all volunteers before starting experimental procedures.
Image acquisition
Volunteers underwent a double-helical CT scan of the knees in the supine position with an upward extension of the patella on both knees. A Siemens Somatom Sensation 16-slice multi-slice spiral CT (Siemens AG, Forchheim, Germany) was used, with scan conditions of 120 kV and 54 mA. Scan parameters were as follows: thickness, 0.75 mm; and total scan time, 10 to 12 seconds. Subjects’ knee CT scan range was from the knee gap at the centerline and the scan range was from the anterior superior iliac spine to the calcaneus. A 0° CT scan of the knee joint was peformed. 11 The angle of the sample (the knee joint distal to the femur) was assessed using a 3D image that was captured using Sante DICOM Editor Demo Version (Santesoft, Nicosia, Cyprus).
Data preservation
From 560 to 640 tomograms per subject were taken, and continuous images were stored on a Siemens Somatom Sensation (Siemens AG) workstation in DICOM format and burned onto a CD-ROM. 12 There were 300 subjects who were scanned, and CT images of their knee joints were obtained.
Construction of knee digital model
On a personal computer system, a continuous knee tomography (DICOM) image was imported into Mimics 10.0 software (Materialise HQ, Leuven, Belgium), resulting in a two-dimensional (2D) image with three planes (horizontal, coronal, and sagittal) that were defined as up and down, and left and right. The Mimics 10.0 three-dimensional (3D) reconstruction system (Materialise HQ) was used to establish a knee 3D motion pattern diagram. 13
Femur measurement
The femur was measured using the width of the femoral condyle (WFC), width of the medial femoral condyle (WMFC), width of the lateral femoral condyle (WLFC), depth of the intercondylar fossa (DICF), and the anteroposterior diameter of the medial femoral condyle (SLM2FC); and the anteroposterior diameter of the lateral femoral condyle sagittal length of the lateral femoral condyle (SLLFC), angle of the lateral femoral condyle (ALFC), and angle of the medial femoral condyle (AM2FC). 14 To determine the femoral condyle articular surface, the distal sagittal superior femoral condyle, articular surface, tibial plateau articular surface, and femoral condyle articular surface at the highest point of the connection and the section of the knee fitting into two arcs were measured. Unified calibration measurements were taken from the femoral condyle from 0° to the maximum flexion of the joint with the tibial plateau section of the arc and the femoral condyle patellar surface fitting a circular arc. When scanning, the display field of view (DFOV) was selected based on the size of the observation site, and the length of the window level (WL) and window width (WW) were then measured.
Proximal tibia measurement
After modeling the proximal tibial osteotomy, the longest distance through the medial and lateral tibial cross-sections was defined as the transverse diameter (ML) that was parallel to the epicondyle axis of the femur. 15 The anterior−posterior distance that passed through ML midpoint and the vertical ML was defined as the middle anteroposterior diameter (AP) using software tools to measure the above data.
Formation and measurement of the osteotomy surface of the distal femur and proximal tibia in the three-dimensional model knee
A 3D digital model was created using Mimics 10.0 software and saved in STL format, then imported into Geomagic Studio 8 software system (Raindrop Geomagic, Research Triangle Park, NC, USA) for analysis. First use of the Geomagic Studio 8 software system comes with a swipe tool to simulate the distal femur and tibial osteotomy. The measurement indexes include femoral condyle osteotomy (anterior hip, anterior oblique hip, anterolateral femoral condyle, transverse diameter of the tibial plateau, anteroposterior diameter of the medial and lateral tibial plateau), and proximal tibial osteotomy.
The Pro/ENGINEER release system (American Parametric Technology Corporation, Addison, TX, USA) was used for 3D modeling of the prosthesis and virtual assembly with the distal osteotomy of the femur.
Measurement of the fit between the prosthesis and the proximal femur and proximal tibia
System tools were used to measure the area of the distal femur and proximal tibia, and the contact area of the prosthesis with the osteotomy surface. 16 The following two femoral components were used in the comparison: PFC Sigma tray (DePuy Synthes, Johnson and Johnson Ireland Ltd., Cork, Ireland) and Nexgen (Nexgen Flex Mobile Bearing Knee, Zimmer Inc., Warsaw, Poland). The coverage of the prosthesis was the calculated area/osteotomy area, and this was used to test the fit of each prosthesis. The femoral condyle prosthesis size analysis was determined to analyze whether there were differences in the femoral condyle anterior and posterior diameter/inner and outer diameter ratio, and to explore each artificial joint manufacturer to provide the femoral condylar prosthesis size that can meet the size measured in this study. The size analysis of tibial plateau prosthesis was to investigate whether the size of the tibial plateau of each artificial joint manufacturer met the size that was measured in this study.
Statistical analysis
Data are presented as the mean ± standard deviation (SD) and analyzed statistically using SPSS for Windows, Version 13.0 (SPSS Inc., Chicago, IL, USA). 17 A one-way ANOVA was used to detect the differences in the changes between the groups after establishing if the data were normally distributed and that the variance was equivalent. A p value of less than 0.05 was considered to be statistically significant.
Results
Baseline data
Among the healthy volunteers, 112 normal knees (52 men and 60 women) were screened. Xinjiang Ugyur counterparts (including colleagues, friends, or relatives) were also recruited. The overall average age was 55 years (range, 27−80 years), and the average age of men was 56.92 ±7.99 years and that of women was 56.50 ±5.98 years. The average height of men was 164.13 ± 8.95 cm (range, height range, 160 to 185 cm), while the average height of women was 156.96 ± 7.86 cm (range, 155 to 175 cm). The mean weight of men was 66.84 ± 5.19 kg and that of women was 51.85 ± 4.87 kg (Table 1). X-ray examination revealed no congenital malformations and lesions, and X-rays were used to measure the length of the tibia. The distance from the medial tibial plateau to the distal end of the inner tibia was recorded.
Study subjects’ baseline (x ± s) (n = 300).

The knee joint parameters of the distal femur were measured
Statistical analysis of the different observation indexes showed the mean and standard deviation of the overall measurement parameters and in both sexes. Knee osteotomy linear parameter size was compared in men and women, and the average measurements in men were larger compared with those of women (Table 2). The angle of the sample is shown in Figure 1.
Three-dimensional reconstruction model measurements (x ± s) (n = 300).

WFC, width of femoral condyle; WMFC, width of medial femoral condyle; WLFC, width of lateral femoral condyle; DICF, depth of intercondylar fossa; SLMZFC, sagittal length of medial zimmer femoral condyle; SLLFC, sagittal length of lateral femoral condyle; AMZFC, angle of medial zimmer femoral condyle; ALFC, angle of lateral femoral condyle.

Sample angle in the 3D image.
The knee joint parameters of the proximal tibia shape were measured
The tibial condyle before and after the diameter/diameter ratio in women was greater compared with that of men (p < 0.05) (Table 3). The angle of sample is shown in Figure 2.
Three-dimensional reconstruction and morphometry of the proximal 6 mm of the tibia (x ± s) (n = 300).

ML, transverse diameter; AP, anteroposterior diameter.

3D image of the sample.
The three-dimensional measurement of the distal femur simulating osteotomy and osteotomy anatomical measurements
Descriptive statistics (mean and standard deviation) of the different observation indicators were obtained for the distal femoral osteotomy measurement parameters (Table 4). The angle of the sample is shown in Figure 2.
Three-dimensional reconstruction and morphometry of the distal femur (x ± s) (n = 300).

AWFC, angle of width of femoral condyle; AOWFC, anatomical osteotomy width of femoral condyle; WLC, width of femoral condyle; WMFC, width of medial femoral condyle; WIFC, width of internal femoral condyle; WLFC, width of lateral femoral condyle; LMFC; length of medial femoral condyle; LLFC, length of lateral femoral condyle; PLFMC, plateau lateral of femoral medial condyle; PLLFC, plateau lateral lift of femoral condyle; APFC, anteroposterior of femoral condyle.
The three-dimensional analysis of 6 mm of the tibial proximal simulated osteotomy and osteotomy anatomical measurements
The ML value in men was significantly higher compared with that of women (p < 0.05) (Table 5). The angle of the sample is shown in Figure 2.
Three-dimensional reconstruction and morphometry of the proximal 6 mm of the tibia (x ± s) (n = 300).

ML, transverse diameter; AP, anteroposterior diameter.
Prognosis and degree of matching between the distal femur and the proximal tibia model
There was a significant difference (p < 0.001) between the ratio of the anteroposterior and internal diameters of the femur in foreign prostheses compared with that of Chinese people, and the ratio was large. There was no significant difference between the two prostheses that were used in this analysis. Among the femoral components of these two prostheses, PFC (DePuy Synthes) had slightly larger coverage compared with Nexgen (Nexgen Flex Mobile Bearing Knee, Zimmer Inc.) (Table 6). Additionally, a 2D sample is shown in Figures 3 and 4. Results of the prosthesis fitness and analysis of the coverage of the medial and lateral tibial plates are presented in Table 7. The coverage of the artificial knee tibial components from each prosthesis manufacturer (i.e. DePuy and Zimmer) was between 68% and 81% of the medial plateau, while the lateral plateau coverage was between 55% and 67%. Both of these tibial components were evaluated, and PFC (DePuy Synthes) had a slightly larger coverage compared with Nexgen (Nexgen Flex Mobile Bearing Knee, Zimmer Inc.).
Femoral prosthesis size analysis (x ± s).
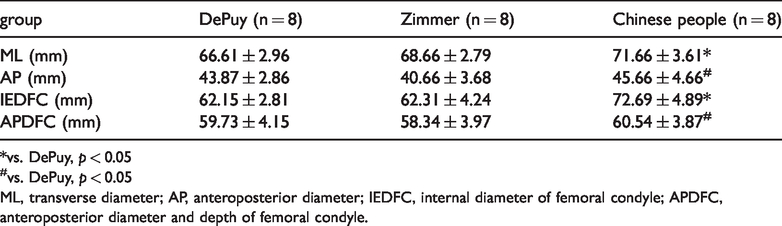
*vs. DePuy, p < 0.05
#vs. DePuy, p < 0.05
ML, transverse diameter; AP, anteroposterior diameter; IEDFC, internal diameter of femoral condyle; APDFC, anteroposterior diameter and depth of femoral condyle.

2D image of a cross-section of the tibia.

2D image of a sagittal section of the tibia.
Prognosis fit analysis (x ± s).

LPCTP, lateral plateau coverage of tibial components; MPCTP, medial plateau coverage of tibial components; FC, femoral condyle
Discussion
In clinical practice, an excessively large knee prosthesis can cause bone and discomfort in the prosthesis contact area and weaken the fixation strength.18,19 It also increases the wear on the ligaments around the knee joint, especially the medial collateral ligament. The extensor knee device is advanced to extend the extensor muscles, affecting the postoperative knee flexion function and hindering closure of the incision. Similarly, if the prosthesis is too small, the lack of high-strength cortical bone surrounding the joint may result in incomplete coverage of the bone cross-section, which makes the joint prone to uneven internal and external forces and results in knee varus or prosthesis sinking that leads to surgical failure. Can it lead to postoperative difficulties because of cancellous bone coverage, resulting in increased blood loss? Can it also lead to postoperative invasion of cancellous bone because of polyethylene bone cement grinding, resulting in osteolysis and loosening of the prosthesis?
The feasibility of an adaptability analysis for the prosthesis and osteotomy can be confirmed using 3D digital technology. 20 With the development of computing technology, computer-aided design (CAD) and computer-aided manufacturing (CAM) technology provides a platform to accurately model the 3D knee and allow digital processing of the data. 21 3D computed tomography (CT) knee reconstruction can show a cross-section of the knee and its ligament complex spatial anatomy, and offer intuitive assessment of ligament injury. Virtual surgical equipment with force feedback for virtual knee arthroscopy as well as knee arthroscopic surgery training can reduce the risk of surgical errors. During joint replacement, researchers use a CT scan to measure the knee joint. 22 Surgical evaluation and mimicking myelopathy replacement surgery can improve the safety of replacement surgery. It has been reported that a virtual knee surgery system can simulate the number and angle of osteotomy preoperatively, select the appropriate knee prosthesis, shorten surgical time, and reduce surgical errors. 23 To establish a customized tibial plateau system, academics and physicians use X-ray film to determine the anatomy of the femur, which should be completed using computer-aided processing technology to design a customized femoral bone for clinical application.
We used the advanced laser scanner to scan the prosthesis and the scanning accuracy limit was 0.01 mm. This effectively avoids the CT scan artifacts caused by the prosthesis and facilitates 3D modeling. For 3D modeling of the prosthesis and virtual assembly with the distal osteotomy of the femur, we used the engineering software Pro/ENGINEER release system (American Parametric Technology Corporation, Addison, TX, USA)). This system shows good performance in dealing with point cloud data, constructing a surface model and smoothing the model. It can also meet the requirements of computer-aided design as well as generate a satisfactory surface curve model. To meet computer-aided manufacturing processing needs, the stereo lithography model that is generated by it can be directly imported into other powerful CAM software for analysis. It can also be used directly to generate a rapid prototype. Therefore, its application in joint prosthesis design research can speed up the knee prosthesis research and the development cycle.
Recently, the effect of tibial prosthesis in knee joint replacement has received increasing amounts of attention from researchers, and information on the geometry of the proximal tibia has been obtained.24,25 There are still many problems with the design and use of artificial joints in our country. 26 The use of artificial joints in our country started relatively late. Design and production quality and operation of artificial prostheses require improvement.
China has some background in artificial joint design, and we can learn from overseas experiences combined with the anatomical characteristics of the Chinese population to design Chinese artificial joints and improve the quality of the artificial joint manufacturing process and production of supporting surgical instruments. Knees have complex movements that require a good understanding of prosthetic design. Knee design for artificial knee bone morphological characteristics show problems with strength and loosening of the implanted prosthesis.
In addition to the mechanical properties of the prosthesis material, the structure, shape and size, and tibia of the patient, and the femoral and surrounding ligament soft tissue characteristics should also be considered. Choosing the appropriate prosthesis size will significantly affect the postoperative outcome.
However, many problems remain since artificial knee joint self-development began over 20 years ago. There has been no important changes in the main shape and design direction of knee prostheses in recent years. The manufacturers introduced knee joints, and there were repeated updates before the current prosthesis was developed. The manufacturers are working to improve the size or the size ratio to obtain the largest osteotomy coverage for knee reconstruction. How did they reduce the amount of stress, cover the tibia completely, and obtain good long-term results? The surgical tools are designed accurately, determination of a good match has improved, and the artificial knee is well-designed, which have allowed the prostheses to improve. Therefore, the correct knee prosthesis specifications include the geometric size, angle, and prosthesis group. The position of the correct knee prosthesis is very important for the successful replacement and long-term survival of the whole artificial knee joint. For the bone, practitioners must rely on prosthesis manufacturers to provide the correct size, and thus, the national orthopedists must be involved in the design and development of knee prostheses, especially with its early development so that it includes the characteristics of a knee-shaped prosthesis.
Based on the analysis of the femoral prosthesis in this study, the size provided by the manufacturer and that of the Chinese people for the anteroposterior diameter of the femoral skeletal/inner diameter ratio was significantly different. The choice of a femoral component in TKA can be difficult. The appearance before and after the femoral jazz prosthesis and osteotomy surface is very consistent. However, the inner and outer diameters tend to be smaller, while the anteroposterior diameter is larger when the transverse diameter is matched. To avoid affecting knee flexion and extension functions, the size of the prosthesis must be determined by the anteroposterior diameter of the bare femoral prosthesis, rather than by the coverage of the outer and inner diameter of the femoral bone. Internal and external femoral skeletal anastomosis may occur. If the bare femur before the bevel is too large or too small, it will have a significant impact on the width of the trochlear bone and structures surrounding trochlear bone. This is not conducive to restoration of the normal bone motion trajectory.
Artificial knee joints from different manufacturers have their own advantages and disadvantages. Performing geometric measurements of the proximal tibia can improve the prosthesis design and increase the coverage of the proximal tibial cross-section. 27 Incavo et al. 28 reported that the average tibial coverage of eight different tibial plateau prostheses was designed to range from 76.4% to 80.8%. The shape of the osteotomy was asymmetric at different levels of the proximal tibia, with an average coverage of 80.62% to 84.73%. 29
After our study assessed that a middle diameter of 60 to 80 mm and an anteroposterior diameter of 40 to 55 mm of the tibial prosthesis is more suitable for Chinese people, and a design was recommended that was consistent with the proximal tibial shape in Chinese people. Research and clinical application to women and asymmetric prostheses to reduce the phenomenon of prosthesis mismatch and improve the excellent rate of knee replacement surgery is increasing. Within the unique anatomic and kinematic limitations of the knee, it is impossible to design an artificial knee joint in which the sagittal and coronal planes are perfectly matched. It is unclear how to best meet the interface between the prosthesis and the osteotomy surface and to achieve ideal coverage and prolong the life of the prosthesis, which remains the goal of future research on improving the artificial knee joint design. If people use imported knee prostheses in a Chinese knee osteotomy patient, the osteotomy angle might not be a good match, making it difficult to accurately reconstruct the force line after surgery. This may lead to failure of a replacement or shortening of the service life of the prosthesis.
Conclusions
The prosthesis and surgery that are designed based on the anatomical parameters of knee joints for Caucasians are not suitable for the Chinese population. The anatomical characteristics of the knee joint significantly differ betweexn the distal femur and the tibial plateau. It is imperative to develop an artificial knee joint prosthesis that is suitable for the physical characteristics of Chinese patients.
Footnotes
Acknowledgement
We thank all the doctors and faculty and staff members who were working in the Department of Orthopedic and Department of CT, First People’s Hospital of Kashgar.
Declaration of conflicting interest
The authors declare that there is no conflict of interest.
Funding
This research was supported by grants from Xinjiang Tianshan Innovative Team Plan [No 2017D14015]; and National key research and development plan (No. 2017YFB1304205).