
Abstract
Purpose
To determine retrospectively the prognostic factors for urinary incontinence following robot-assisted radical prostatectomy (RARP).
Methods
Altogether, 180 patients with localized prostate cancer underwent RARP (same surgeon). Preoperative physical status, disease characteristics, laboratory findings, and surgical technique were recorded and the patients checked 1, 6, 12, and 24 months after RARP regarding their contribution to predicting post-prostatectomy urinary incontinence (PPI).
Results
Overall, 114 (63.3%) patients had PPI 1 month after RARP and 19 patients (16.0%) at 24 months. Univariate analysis showed that age was a significant factor for predicting PPI at 1 month. PPI predictors at 24 months were age, body mass index, preoperative serum albumin level, previous transurethral resection of the prostate, total operative time, and bladder neck sparing. Multivariate analysis indicated that age and total operative time were significant predictors.
Conclusion
Older age and longer operative time were highly relevant to short- and long-term PPI occurrence after RARP.
Keywords
Introduction
Radical prostatectomy remains the most commonly used curative treatment for prostate cancer that is also intended to minimize collateral damage to surrounding tissues.1,2 Accurate tumor staging via pathologic examination of the surgical specimen is performed after radical prostatectomy. Currently, radical prostatectomy is routinely performed for localized advanced prostate cancer. Complications, however, are inevitable in some cases, although the overall early complication rate after radical prostatectomy is low when performed by experienced surgeons. 3 Among the late complications following radical prostatectomy, urinary incontinence is one of the most troublesome.
The physiologic mechanisms that contribute to urinary control after radical prostatectomy are not entirely understood. It is speculated, however, that damage to the internal sphincter and possibly the external sphincter during the surgery may contribute to post-prostatectomy incontinence (PPI).
Oefelein 4 and Van Kampen et al. 5 suggested that physical factors such as age, prostate size, and previous transurethral resection of the prostate (TURP) foreshadowed the development of PPI. Age is probably one of the most important previously mentioned predictor. Younger patients are more likely to regain urinary continence than older patients. Recognition of most factors only help us predict the possibility of PPI urinary incontinence, however. They do not prevent it.
This study evaluated possible predictors of PPI at 1, 6, 12, and 24 months after robot-assisted radical prostatectomy (RARP). It also attempted to identify the factors, if any, that not only predict PPI but also improve the outcome.
Materials and methods
The institutional review board of Chang Gung Memorial Hospital approved this study and waived the need for patient consent. We retrospectively enrolled patients who underwent RARP by a single surgeon from September 2008 through September 2014 in a tertiary teaching hospital. All patients underwent RARP for prostate adenocarcinoma at clinical stage T1–T3. A technique to preserve the neurovascular bundle was performed based on the surgeon's judgment. The patients were shown how to perform Kegel’s exercise and were advised to practice it daily as soon as possible after surgery regardless of whether incontinence is noted.
The following data were gathered from patient charts: preoperative physical status (age, height, weight, body mass index (BMI)); preoperative serum albumin level; history of TURP; history of using anti-androgenic drugs (including anti-androgens, luteinizing hormone-releasing hormone analogues or antagonists). Also noted were the disease characteristics, including prostate size, clinical and pathologic stage of the prostate cancer, and the Gleason score. Surgical events – operation time, intraoperative blood loss, preservation of the bladder neck, preservation of the neurovascular bundle – were also evaluated. The bladder neck-sparing technique was defined as the absence of bladder neck reconstruction before anastomosis between the bladder neck and urethral stump. Preservation of neurovascular bundles were recorded as “no preservation,” “unilateral preservation,” or “bilateral preservation.” PPI was defined as urination that required the use of more than one pad within a day after the operation. The PPI status was reported by the patient and evaluated by means of a 3-day voiding diary in the outpatient department by the same physician. The PPI data were obtained at 1, 6, 12, and 24 months after RARP.
The exclusion criteria were the following: incomplete data collection; patient lost to follow-up; patient missed first PPI evaluation at 1 month after RARP; patient with preoperative urinary incontinence; patient had already undergone an intervention (other than medication alone) for prostate cancer such as radiation therapy, cryotherapy, and/or high-intensity focus ultrasonography.
The χ 2 test and Fisher’s exact test were used for categorical comparisons of data. Differences in means of continuous measurements were tested using the independent t-test. Binary logistic regression was used for the multivariate analysis in the next step for all the significant factors analyzed with the χ 2 , Fisher’s exact test, and the independent t-test. A value of P < 0.05 was considered to indicate statistical significance.
All statistical analyses were performed on a personal computer with the statistical package SPSS for Windows (Version 17.0; SPSS, Chicago, IL, USA).
Results
Patients' characteristics.

The results are given as the number or the mean (range) or the number (%).
Abbreviations: BMI, body mass index; TURP transurethral resection of the prostate; PSA, prostate-specific antibody; NVB, neurovascular bundle; PPI, post-prostatectomy incontinence.
The mean prostate volume was 44.1 cm3 (range 13.3–109.0 cm3). Before RARP, 9 of the 180 patients had stage cT1disease, 120 had stage cT2 disease, and 51 had stage cT3 disease. The pathology analysis showed that 117 of the patients had pT2 stage disease, 60 patients had pT3 stage disease, and the remaining 3 patients had lymph node metastasis. Of the 180 patients, 61 had Gleason scores of <7, another 89 had scores of 7, and 30 had scores of >7.
The mean operative time was 322 min (median 315 min, range 230–550 min). The average intraoperative blood loss was 147 ml. Bladder neck sparing was performed in 92 patients, unilateral neurovascular bundle sparing in 67 patients, and bilateral neurovascular bundle sparing in 58 patients.
Among the 180 patients enrolled in this study, 114 (63.3%) showed evidence of PPI at 1 month after RARP, and 42 (23.5%) showed evidence of PPI 6 months after RARP. The rates decreased to 18.1% and 16.0% at 12 and 24 months, respectively, after the surgery.
Univariate analysis (P values) of the parameters for predicting PPI occurrence at 1, 6, 12, and 24 months.

Results are given as P values.
Abbreviations: BMI, body mass index; TURP, transurethral resection of the prostate; NVB, neurovascular bundle.
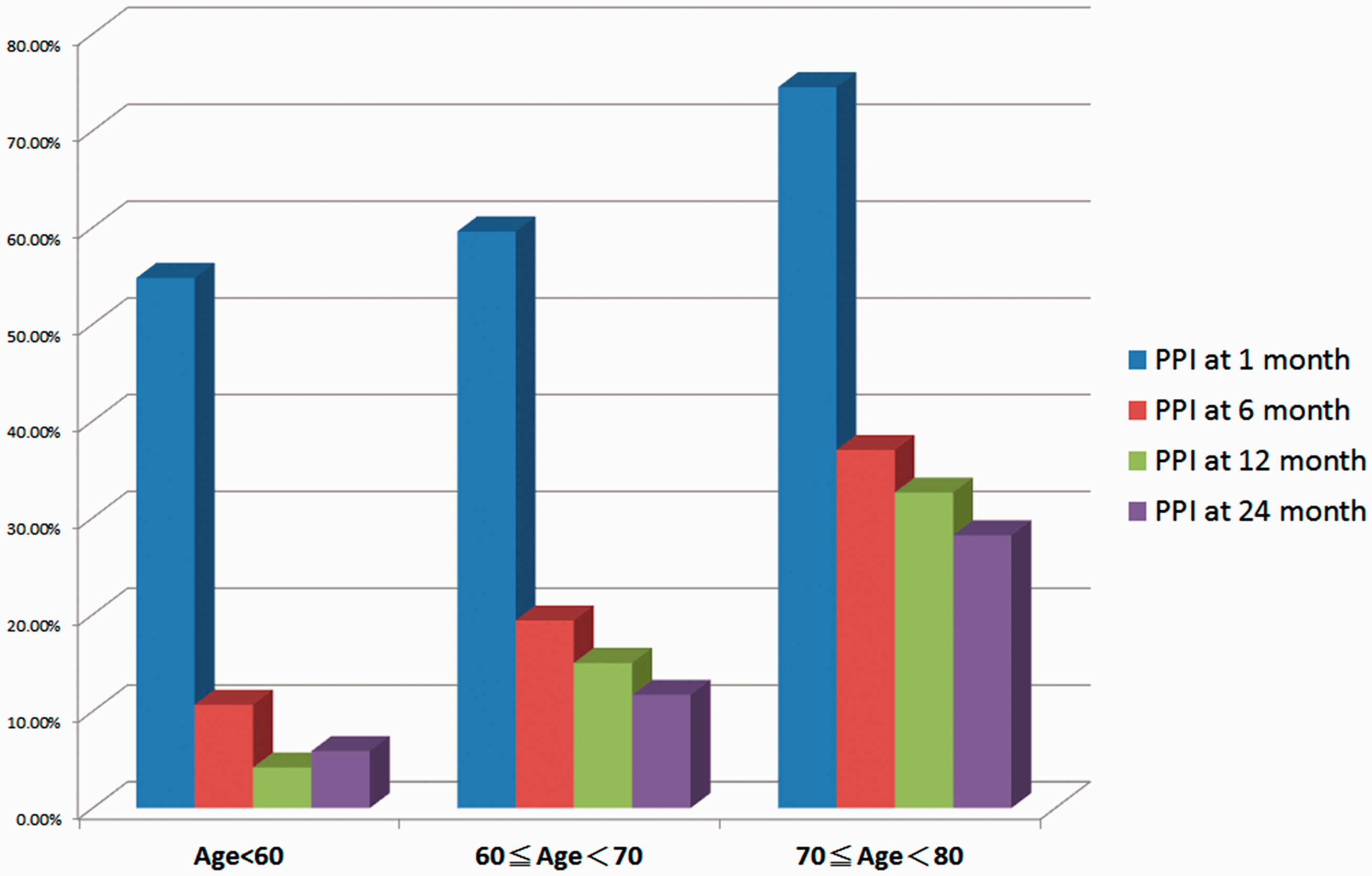
PPI occurrence following RARP in patients who were evaluated 1, 6, 12, and 24 months after surgery, by age group.
The univariate analysis revealed the significant predictors for PPI at 1, 6, 12, and 24 months after RARP (Table 2). The parameters that remained significant at 24 months after RARP were the age at surgery, BMI, preoperative serum albumin, history of TURP, total operation time, and bladder neck sparing. Figure 2 shows the incontinence prevalence of the various groups by the six significant parameters from the univariate analysis at 1, 6, 12, and 24 months. We then used these six predictors in the multivariate analysis Table 3, which indicated that patient age at the time of RARP was the most significant predictor throughout the first 2 years after RARP. A longer total operation time resulted in poor continence until 2 years after RARP. Patients with high BMIs and low albumin levels also tended to experience incontinence, but these variables lacked significance in the multivariate analysis.
PPI occurrence following RARP at 1, 6, 12, and 24 months according to possible risk factors for PPI. Prevalence of PPI at four postoperative time points (1, 6, 12, and 24 months after RARP), in regard to: age (a); BMI (b); serum albumin level (c); prior TURP (d); operative duration (e); bladder neck sparing (f). Multivariate analysis results of the predictors for PPI at 1–24 months after RARP. PPI, post-prostatectomy incontinence; RARP = robotic-assisted resection of the prostate; BMI, body mass index; Exp(B), odds ratio; TURP, transurethral resection of the prostate.

Discussion
Laparoscopic radical prostatectomy allows better visualization of the prostatic apex than traditional open surgery. The minimal bleeding and increased magnification of the operative field associated with the laparoscopic approach allow precise dissection of the prostatic apex with limited trauma to the periurethral striated sphincter and genitourinary diaphragm. 6
Few, if any, studies have provided definitive conclusions about whether laparoscopic radical prostatectomy is associated with a lower incidence of postoperative urinary incontinence than open surgical approaches.7–9 Most of the studies have shown that age, preoperative micturition disorders, 5 urethral length, 10 and factors that are related to the surgical technique (e.g., prostate size) 4 are predictive of PPI. One study focused on postoperative images to predict incontinence. 11
We found that the most significant predictor for PPI after RARP was the patient's age at the time of surgery. A prolonged total operation time also significantly contributed to poor continence status. This could be explained by the longer total surgical time required, representing more difficult surgery and dissection around the prostatic margin, thereby causing more damage to the pelvic floor and sphincter muscle.
Previous TURP for benign prostate hyperplasia was not correlated with the occurrence of PPI until 12 months after RARP. It is possible that patients who had undergone prior TURP may have had an easier recovery from PPI at 24 months after RARP. Only 5 of 14 patients with a previous TURP still had PPI at 24 months after RARP. More cases are required to support the relation between prior TURP and long-term PPI and whether patients with previous TURP could also enjoy satisfying continence after RARP.
The pelvic anatomy of the men undergoing radical prostatectomy may be similar to that of the female anatomy. In addition, the prevalence of stress incontinence is higher than in men who did not undergo radical prostatectomy. Intraoperative techniques that maintain anatomical and functional structures in the pelvis as normal as possible may bring early return of urinary continence after RARP. 11 Currently, the most common treatment strategy for men with PPI is similar to that for female stress urinary incontinence and includes pelvic floor muscle exercises12–14 and suburethral sling placement.6,12,13 Only patients with severe incontinence may require an artificial sphincter.
The results showed that the prevalence of incontinence was high (63%) 1 month after RARP. It then decreased to 23.5%, 18.1%, and 16.0% at 6, 12, and 24 months after RARP, respectively. These results suggest that PPI during the first postoperative month is in an acute phase of urinary incontinence, the 6–12 months after surgery is a recovery phase, and the 12–24 months after RARP is a stable PPI phase. Thus, any aggressive intervention to treat PPI within 1 year after RARP requires serious consideration, as the PPI could resolve without treatment if given more healing time.
Age and BMI are well-known risk factors for female stress incontinence.8,14,15 In the present study, these parameters have shown a notable relation with male incontinence after radical prostatectomy as well. In addition to age and BMI in this study, the univariate analysis showed that the albumin level was a significant predictor of PPI at 12 and 24 months after RARP, although it showed only a trend – without significance – in the multivariate analysis.
It is reasonable to assume that the albumin level represents the general nutritional status of a patient. Thus, patients with higher albumin levels are healthier and have healthier pelvic floor muscles than those with lower albumin levels. Thus, with adequate pelvic floor muscle training, these muscles could help protect against the development of incontinence after surgery. This could also explain why younger patients recover faster from PPI than older patients.
A larger sample size and a prospective study design are needed to confirm the roles of the albumin level and the BMI on PPI after RARP.
Conclusion
Most of the patients who experienced PPI after RARP recovered continence within 1 year after the operation. Old age at the time of surgery and a longer total operative time were highly associated with short-term and long-term PPI. Patients with lower albumin levels and higher BMIs also tended to have worse long-term outcomes for incontinence. Losing body weight before RARP and maintaining adequate albumin levels before and during pelvic floor exercise may potentially provide better PPI outcomes.
Footnotes
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.