
Abstract
Objective
This observational cohort study aimed to evaluate ventilatory function (VF) and functional exercise capacity (FEC) in mild adolescent idiopathic scoliosis (AIS).
Methods
Seventy-three adolescents with idiopathic scoliosis, aged approximately 10 to 17 years (mean age: 13.43 ± 1.27 years), with a Cobb angle less than 20° (mean: 16.44° ± 1.59°), met the inclusion criteria and were assigned to group A. Another 34 healthy adolescents with normal VF and FEC served as controls (group B). Forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), maximum voluntary ventilation (MVV), and FEC (by the 6-minute walk test [6MWT]) were the main outcome measures.
Results
Post-study mean values of FVC, FEV1, FEV1/FVC, MVV, and the 6MWT were 2.42 ± 0.36 L and 3.26 ± 0.59 L, 2.14 ± 0.31 L and 3.03 ± 0.43 L, 88.13% ± 3.89% and 91.14% ± 4.67%, 76.96 ± 6.85 L/m and 107.61 ± 11.44 L/m, and 581.12 ± 12.25 m and 627.74 ± 15.27 m in groups A and B, respectively. Between-group comparisons showed significant differences in FVC, FEV1, FEV1/FVC, MVV, and the 6MWT.
Conclusion
Mild pulmonary and functional restrictions start early in mild AIS. This issue requires immediate intervention to prevent further deterioration.
Keywords
Introduction
Scoliosis is a common musculoskeletal disorder of the spine that is characterized by an observable lateral curvature, which produces direct effects on the thoracic cage. 1 Previous studies have reported variable and indecisive high prevalence rates of scoliosis in children locally 2 and globally. 3 The prevalence of adolescent idiopathic scoliosis (AIS) ranges from 0.47% to 5.2%, with a higher rate and severity of spinal curvature in girls than in boys. 4
Although the cause of scoliosis is unknown, idiopathic scoliosis (IS) is the most common type of scoliosis, accounting for approximately 85% of cases. 5 Based on the onset, childhood IS is initially classified into infantile, juvenile, and AIS. 6 AIS represents approximately 90% of diagnosed cases of IS, 7 and is defined as an abnormally laterally curved spine in apparently healthy children. 8 This curvature produces an angle >10o as evaluated through the Cobb method on a standing radiograph. 9 AIS is accompanied by vertebral rotation, resulting in a deformed spine in the sagittal, frontal, and transverse planes, 10 as well as geometric abnormalities in the rib cage. 11 AIS is subcategorized into mild (Cobb angle = 10°–20°), moderate (Cobb angle = 20°–30°), and severe (Cobb angle >30°), whereas a curvature less than 10° is considered as accepted normal variation because it has little tendency for progression. 12
Scoliosis is a common local and worldwide problem that is commonly accompanied by a restrictive pattern of respiratory abnormalities in nearly two-thirds of sufferers with sufficiently large scoliotic curves. 13 Restrictive pulmonary impairment is commonly found in patients with IS 14 and is accompanied by an increased risk of mortality in the long term. 15 This situation requires early detection of pulmonary disorders in patients with scoliosis. Respiratory disorders and exercise intolerance are common complications of IS secondary to weakness of respiratory muscles and reduced lung capacity. 16 Impaired exercise tolerance and physical deconditioning can be early manifestations in patients with mild scoliosis. 17 Abnormal ventilatory patterns and respiratory muscle involvement have been reported in patients with asymptomatic mild scoliosis who may be free of any respiratory dysfunction at rest. 18 However, these patients show reduced functional capacity 19 and reduced maximum oxygen uptake 20 during exercise training. Previous reports have shown that ventilatory abnormalities are secondary to rib cage deformation and vertebral rotation, 21 as well as respiratory muscle weakness16,20,22 and limited respiratory muscle functionality. 23 This in turn negatively affects the mechanics of rib cage motion and results in pulmonary complications. 21
Various complications, such as back pain, psychological problems, physical disability, pulmonary disorders, and even early mortality, have been reported in populations with mild,17,18,19,21,22 moderate, and severe scoliosis. 9 The effect of scoliosis on lung function has been recognized. However, little is known regarding the effect of mild scoliosis on pulmonary function because it has been dismissed as insignificant. 24 With constant advances in the understanding of the nature and complications of AIS, these complications need to be determined at an early stage to alleviate its effect on adolescent’s health before progressing. 10 Therefore, this study aimed to investigate the effects of mild AIS on ventilatory function (VF) and functional capacity (FC).
Patients and methods
Study population
This study included two groups: study group A and control group B. Both groups were age-matched (10–17 years). All participants of both groups were sedentary and were not involved in any previous conservative or surgical treatment programs prior to or during the study. The participants also had no recent infectious exacerbations within the last 2 months, with no history of cardiovascular, psychiatric, or psychological disorders.
A total of 82 adolescents with AIS were included who were free of symptoms or signs that could alert the physician that another diagnosis should be considered. These symptoms or signs included other structural abnormalities of the spine found on X-ray, infantile or juvenile-onset scoliosis, lower extremity deformities, and back pain and neurological signs or symptoms. These adolescents were recruited from orthopaedics and paediatrics outpatient clinics of governmental hospitals and were screened by an experienced physician for eligibility. Initially, seven patients were excluded because they were under exercise therapy and another two patients were excluded because they were asthmatics. Therefore, 73 subjects (17 boys and 56 girls) met the inclusion criteria and were involved in the study as group A.
Adolescents with a Cobb angle less than 10° or greater than 20°, those with obstructive pulmonary symptoms, and those with associated neuromuscular diseases, such as cerebral palsy, muscular dystrophy, spina bifida, or congenital myopathy, were excluded. Adolescents who had been previously or were already being managed for scoliosis by any type of treatment were excluded from the study. Participants with confirmed AIS who matched the inclusion criteria and had no exclusion criteria were assigned to study group A. Another 34 age-matched healthy adolescents (5 boys and 29 girls) who were free of scoliosis were assigned as controls (group B) (Figure 1). No diagnosis of scoliosis was determined as no signs of scoliosis upon screening or axial trunk rotation in the Adams test using a scoliometer, normal spinal alignment on screening, and no other musculoskeletal abnormalities. Additionally, adolescents in this group had normal VF and FC.
Flow chart of the patients.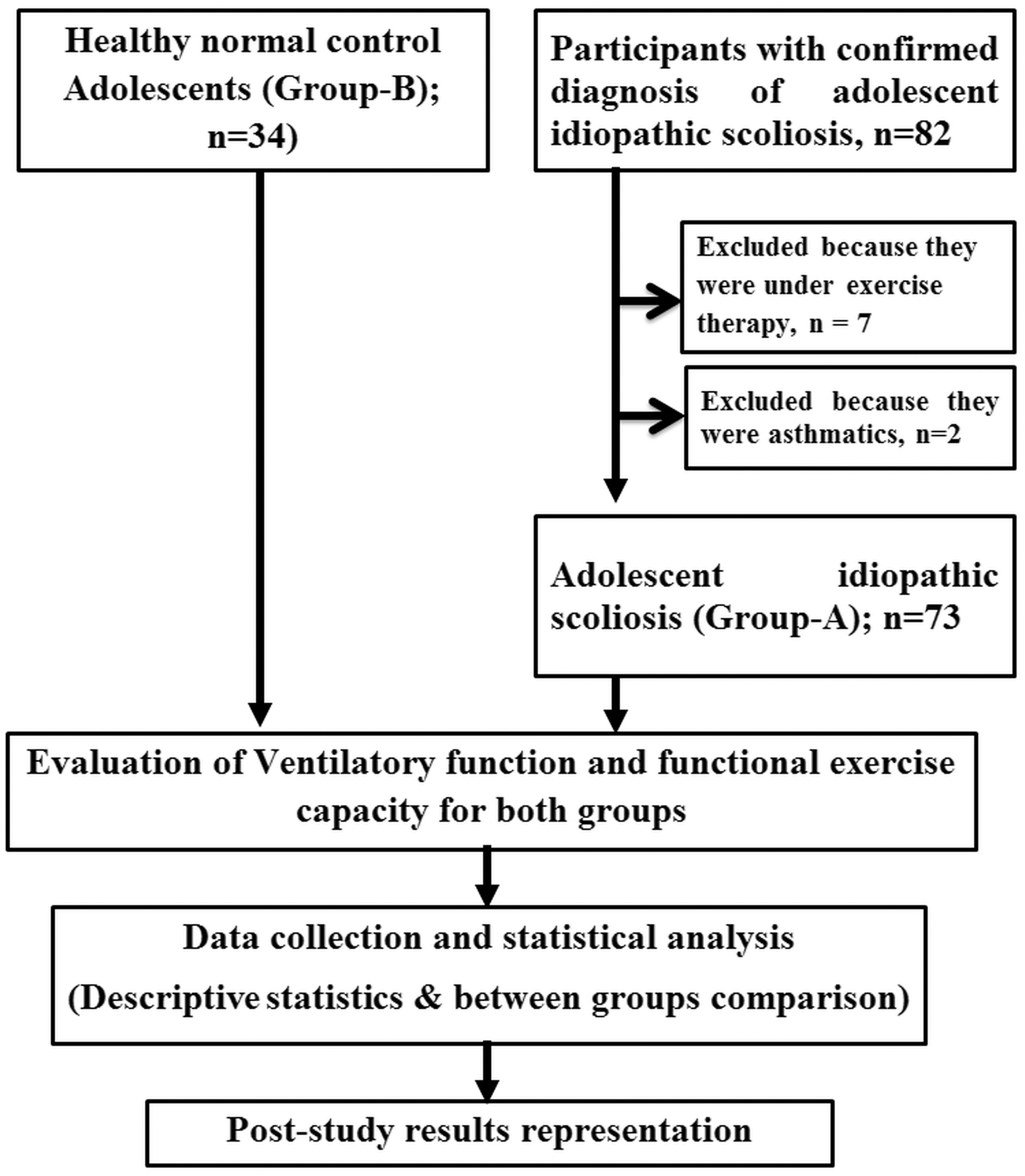
After exclusion of limb length discrepancies, screening via the Adams test using a scoliometer was conducted for all participants, followed by X-ray evaluative procedures only for participants with scoliosis (diagnosed by the Adams test and a scoliometer). All participants underwent evaluation of VF using a spirometer (Spirolab III: MIR Medical International Research, Italy) and evaluation of FC by the 6-minute walk test (6MWT). Participants with normal VF and FC were only assigned to group B. There were no exclusions or drop-outs in this group after assignment of participants.
A preliminary power analysis was performed. The sample size was calculated based on an estimated medium Cohen effect size (F = 0.36) using a power of 95% and a 5% significance level that determined a realistic total sample size of 102 participants (in both groups) for this study. The total number of participants was 107 to allow for any withdrawal of participants. This study was approved by the scientific research ethics committee of the Faculty of Applied Medical Sciences, Umm Al-Qura University. After a detailed explanation of the study objectives and evaluation procedures, written informal parental consent was obtained from all of the participants. This study was conducted in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki principles 1975, revised in 2000). The study followed an observational cohort study design and was conducted between January and July 2016.
All subjects’ data were collected using standard laboratory procedures. Body weight was measured in light indoor clothes to the nearest 0.1 kg. For participants in group B, the patient’s corrected height was calculated using arm span. Arm span was measured as the distance between the tips of the middle fingers, with the individual standing with his/her back to the ruler. The arms were stretched horizontally, the elbows and wrists were extended, and the palms faced directly forward. For participants in group A, standing height without shoes was measured to the nearest 0.1 cm using a calibrated clinical weight scale and stadiometer. Body mass index (BMI) was calculated as weight (kg) divided by height squared (m2). All research materials (including data, sampling procedure, and participants’ information) were kept secure by the corresponding author.
After participants were assigned to either group A or group B, they underwent an identical battery of ventilatory function and functional capacity evaluations throughout the study.
Evaluation of VF
Evaluation of FVC, FEV1, and MVV was guided by previously published guidelines 27 using a computerized electronic spirometer (Spirolab III). Data are expressed as absolute values and as a percentage of the predicted normal values. Maximum effort was emphasized to gain the best results. For evaluation of FVC and FEV1, participants initially breathed normally for several cycles, followed by maximum forced expiration. For evaluation of MVV, after a sufficient rest time, participants inspired forcefully and rapidly as fast as he/she could for 15 seconds. FVC and MVV evaluation manoeuvres were repeated three times where the best-recorded trial results were used.
Evaluation of functional exercise capacity using the 6MWT
Functional exercise capacity (FEC) was evaluated for each participant using the 6MWT according to a previously described procedure. 28 In this test, each participant was asked to walk at his/her own maximal speed over a 40-m flat straight corridor and cover as much ground as possible, while maintaining a steady pace without running during 6 minutes.
Statistical analysis
Statistical analysis was performed using the statistical package SPSS version 16 (Chicago, IL, USA). Data are presented as mean ± SD. All data were assessed for normal distribution using the Kolmogorov–Smirnov test. After testing for homogeneity of variance, the robust Brown–Forsythe test was considered. Descriptive statistics were used to represent the mean values of evaluated variables. Between-group comparisons were conducted via one-way analysis of variance. Pearson’s correlation was used to examine the relationship of each variable with the Cobb angle. The level of significance was set at P < 0.05.
Results
Characteristics of participants with mild adolescent idiopathic scoliosis (group A).

Values are mean ± SD.
BMI: body mass index.
Between-group comparisons of demographic characteristics, ventilatory function, and the 6MWT.

Values are mean ± SD.
BMI: body mass index, FVC: forced vital capacity, FEV1: forced expiratory volume in 1 second, MVV: maximum voluntary ventilation, 6MWT: 6-minute walk test.
Level of significance was at P < 0.05. **Non-significant; *significant.
FVC, FEV1, and MVV of group A were compared with predicted normal values of the same group and normal control values obtained from group B. In group A, the mean value of FVC was lower than 80% of the predicted normal value of 3.16 ± 0.48 L. FEV1 was mildly reduced in group A (below 80% of the predicted normal value of 2.75 ± 0.4 L). The FEV1/FVC ratio was normal in group A (>70% predicted). The mean value of MVV in group A was lower than 80% of the predicted normal value of 110.04 ± 10.4 L/m). VF in group A showed a restrictive pulmonary pattern.
Between-group comparisons showed that FVC, FEV1, MVV, and 6MWT mean values were significantly higher in group B compared with group A (P < 0.05, Table 2).
Pearson correlation analysis showed that spinal angulation represented by the Cobb angle was not correlated with FVC (r = 0.03, P = 0.78), FEV1 (r = 0.03, P = 0.75), MVV (r = 0.01, P = 0.9), and the 6MWT (r = 0.07, P = 0.45) in group A.
Discussion
There is an apparent dissociation between subjective symptoms and objective signs of pulmonary limitations in patients with AIS. However, appreciable functional and pulmonary deficits are associated with AIS that affect the body’s functionality, leading to serious disorders later in life. 29 The present study investigated the effect of asymptomatic mild AIS on VF and FC at an early stage of this disease. The current study showed that, for the first time in our region, patients with asymptomatic mild AIS were vulnerable to mild ventilatory and functional impairment. This finding is similar to that in patients with more severe scoliotic deformities.16,18,20,21
Mild to moderate scoliosis may not be accompanied by clear physical limitations in basal static situations. However, deconditioning may appear during activities because of exercise intolerance and ventilatory inefficiency, 20 which are related to the degree of spinal curvature in moderate and severe cases of scoliosis. 30 Furthermore, impairment of physical function secondary to ventilatory limitations is an important contributing factor to avoidance of activities and exercise training in patients with AIS. 31
Extra-pulmonary, as well as pulmonary factors, were previously assumed as possible mechanisms for explaining the effects of scoliosis on pulmonary function and exercise capacity. Changes in ventilatory mechanics and functional capacity in patients with scoliosis can be attributed to distortion of the rib cage and malalignment of the thorax. 32 This in turn impairs normal lung development during the early period, characterized by rapid lung growth. 33 Furthermore, the number of pulmonary vessels is also compromised and mismatched with the normal developmental stage in patients with scoliosis. 2 Previous studies have shown that the rib cage of patients with AIS scoliosis is narrower than that in non-scoliotic normal controls. 34 This abnormal narrowing causes the chest components to develop abnormally during growth because there is insufficient space for normal alveolar growth, which results in extrinsic restrictive pulmonary disorder. 35 Because scoliosis is a three-dimensional deformity, ventilatory impairment in patients with scoliosis is also attributed to vertebral rotation, a reduced sagittal diameter of the thoracic cage, 36 and altered chest wall compliance. 37
Because of a small Cobb angle in patients with mild scoliosis, observed ventilatory abnormalities cannot be merely attributed to mechanical changes in the chest wall. 38 Neither spirometric variables nor functional capacity was correlated with the degree of spinal curvature in the current study. One plausible explanation for this lack of correlation is the contribution of other factors, such as peripheral skeletal and respiratory muscle dysfunction, to ventilatory and functional capacity impairment. 16 Respiratory muscle weakness is a potent contributor to ventilatory impairment in mild, 39 moderate, and severe forms of scoliosis. 40 Physical deconditioning mainly contributes to ventilatory abnormalities, inspiratory and expiratory muscle weakness, 16 and disturbed gas exchange capacity in AIS. 41 Both force-generating elements, as well as passive supporting structures responsible for maintenance of postural control, are negatively affected in patients with AIS. 42 Trunk rotation and distortion of the rib cage, which are commonly observed in patients with AIS, result in abnormal configuration of the diaphragm and intercostal muscles. This reduces respiratory muscle capacity for force generation, finally ending in respiratory muscle weakness. 39 Smyth et al. 34 reported that a reduction in vital capacity was correlated with impairment in the force-generating units (i.e., the respiratory muscles) in patients with mild AIS. 43
Diaphragm and intercostal muscles are the most important components that are involved in mild scoliosis. 18 Alves et al. 21 introduced the concept of respiratory muscle weakness and showed a clear reduction in intercostal muscle force generation, mainly on the concave side. This reduces respiratory capacity, leads to ventilatory disorders, and hinders patients from being engaged in daily activities. An abnormal increase in pressure and mechanical load on respiratory muscles, as well as distortion of the length-tension relationship, are important factors that disrupt the normal activity pattern of respiratory muscles in patients with IS. 16
Ventilatory impairment and skeletal muscle dysfunction are the most important factors that limit physical performance in patients with AIS. 44 Martinez-Liorens et al. 16 reported that generalized muscle dysfunction in young patients with AIS predominates at relatively early stages of the disease, and is attributed to abnormally attenuated functional capacity at these early phases. Disturbed activity and functional asymmetry are well documented in abdominal and back muscles in patients with AIS.45–52 Asymmetrical activity patterns and morphological changes have been shown in the paraspinal and lateral abdominal muscles in patients with AIS.45,46,47 Scoliosis reduces strength and disturbs the symmetry of force generation from the abdominal muscles, 48 as well as the erector spinae muscles. 46 Kuo et al. 42 reported abnormal muscular activation patterns that negatively affected postural control and physical performance in patients with AIS. Furthermore, AIS is associated with a reduction in lateral abdominal muscles thickness compared with controls. 49 Altered abdominal muscles thickness has been found during rest, 47 the active straight leg raising test, 50 and during the abdominal drawing-in manoeuver 49 in patients with AIS.
Abnormal distribution of paraspinal muscle fibers 51 and initiation of myofilament disarray 52 occurring in patients with AIS can significantly alter paraspinal muscle functional performance. Furthermore, the cross-sectional area of the lumbar multifidus muscles is significantly reduced on the contra-lateral side of primary thoracic curve convexity and on the convex side of a lumbar or thoracolumbar curve in patients with AIS. 45 These findings explain in part the reduction in pulmonary function and functional exercise capacity that is found in patients with AIS.
This study has limitations that should be mentioned. This study lacked evaluation of skeletal muscle strength and psychological aspects (AIS is usually accompanied by disturbed skeletal muscle function and health-related quality of life). However, all of these factors were out of the scope of the current study. The main objective of this study was to evaluate the effect of AIS on pulmonary and functional aspects. Another potential limitation of this study is the disproportion of sex (girl:boy ratio). This does not reflect the global male/female ratio of AIS because a detailed study on the prevalence of AIS according to sex was out of the scope of this study. Further studies are required including larger numbers of patients and covering more extended geographic regions to overcome these limitations.
In conclusion, mild pulmonary and functional restrictions start in the early stage of mild AIS. This issue requires immediate intervention to prevent further deterioration. Additionally, spirometric and functional capacity restrictions are not correlated with the degree of spinal curvature in adolescents with mild AIS. Further investigations are warranted for better clarification of other contributing factors to AIS.
Footnotes
Acknowledgements
The authors would like to express their appreciation to all adolescents and their parents for their cooperation in this study. The authors would like to thank the King Abdulaziz City for Science and Technology, Kingdom of Saudi Arabia for their financial support. The authors are grateful to the Science and Technology unit in Umm Al-Qura University for its logistic support.
Declaration of Conflicting Interest
The authors declare that there is no conflict of interest.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Plan for Science, Technology and Innovation (MAARIFAH) - King Abdulaziz City for Science and Technology, Kingdom of Saudi Arabia (number: 13-MED1319-10).