
Abstract
Objectives
To assess pulmonary function and functional capacity in children and adolescents with mild or moderate idiopathic scoliosis who were included in a rehabilitation programme, and to observe some of their physical activity behaviours.
Methods
Forty children (aged 9–17 years) with mild or moderate idiopathic scoliosis (patients) and 40 sex- and age-matched healthy controls were included in the study. Physical activity behaviours (hours of time spent at a desk and at a computer, hours of competitive and non-competitive practice of exercise per week) were recorded. Patients were assessed before beginning rehabilitation and 12 weeks after an exercised-based programme by spirometry and functional capacity testing (6-minute walk test).
Results
All respiratory and functional capacity parameters were significantly increased after physical therapy compared with before beginning physical therapy in patients. However, there were still differences between patients and controls in all assessed parameters after therapy. Children and adolescents who were diagnosed with scoliosis spent a longer time at a computer, and had reduced regular and competitive physical exercise compared with controls.
Conclusions
In children and adolescents with mild/moderate idiopathic scoliosis, pulmonary parameters and functional capacity are improved after 12 weeks of supervised physical therapy.
Keywords
Introduction
Scoliosis is defined as sideways curvature of the spine that most frequently occurs during the growth spurt just before puberty. 1 In adolescents, the prevalence of idiopathic scoliosis ranges from 0.93% to 12% worldwide. 2
Scoliosis can cause decreased spinal movement, weakening of muscles near the spine, chronic pain, psychological suffering, reduced pulmonary function, and respiratory dysfunction. 3 Abnormal ventilatory patterns and respiratory muscle involvement have been reported in patients with asymptomatic mild scoliosis who may be free of any respiratory dysfunction at rest. 4 Impaired exercise tolerance and physical deconditioning can also be early manifestations in patients with mild scoliosis. 5 However, Diarbakerli et al. 6 showed that adolescents with idiopathic scoliosis have similar levels of self-reported physical activity as healthy individuals. Some authors have reported that staying in the sitting position for long periods of time and maintaining a static posture, without movement, and sometimes inadequate movement, can determine postural alterations of the spine, such as scoliosis. 7
This study aimed to assess pulmonary function and functional capacity in school children and adolescents with mild or moderate idiopathic scoliosis who were included in a rehabilitation programme. We also aimed to observe some of the physical activity behaviours in these patients.
Methods
Participants
Our study included 49 school children and adolescents with idiopathic scoliosis. The patients were selected from those who visited the Rehabilitation Department of Paediatric Surgery, Louis Turcanu Children’s Hospital Timisoara, Romania. Inclusion criteria were as follows: children and adolescents who attended school; and clinically and radiologically confirmed mild or moderate idiopathic scoliosis. Exclusion criteria were as follows: secondary scoliosis (congenital scoliosis, muscular scoliosis, and neurological scoliosis), obstructive ventilatory disorders, thoracic surgery, cardiovascular disease, psychiatric or psychological disorders, and recent infectious episodes within the last 2 months.
Three children met the exclusion criteria, including one each with asthma, depression, and acute bronchitis. We then enrolled 46 patients of whom six discontinued the rehabilitation programme. The remaining patients completed the final assessment and their data were analysed. There were no data missing from the training sessions. The subjects who dropped out did not have significantly different clinical characteristics at baseline from those who completed the study (data not shown). The data of the subjects who dropped out were not analysed. Sex and age-matched healthy controls (school children and adolescents) were recruited by posters placed at public schools nearby the hospital.
Participation in the study was voluntary. Written informed consent was obtained from all of the participants’ parents. The study was carried out in accordance with the Declaration of Helsinki and was approved by the Institutional Ethics Committee (Louis Turcanu Emergency Children’s Hospital, No. 56/05.10.2018).
Assessment
The following data related to patients and controls were collected: demographic characteristics (age, sex, weight, and height) and physical activity behaviours (hours of time spent at a desk and at a computer per week, and hours of competitive and non-competitive practice of exercise per week). The patients were assessed clinically by the same orthopaedic surgeon. An X-ray examination of the spinal column in the standing anterior–posterior view was then performed. The X-ray examination and Cobb angle measurement were performed by a single investigator who was a radiologist.8,9 Mild scoliosis was defined by a Cobb angle <20° and moderate scoliosis was characterized by a Cobb angle between 21° and 35°. 10
The protocol of our study consisted of two assessments for the study group. The first assessment was performed before beginning rehabilitation (T1) and the second assessment was at 12 weeks after an exercise-based rehabilitation programme (T2). Each evaluation consisted of spirometry tests and functional capacity testing (6-minute walk test [6MWT]). Assessment of pulmonary function and the 6MWT were performed by the same investigator who was a specialist in physical medicine and rehabilitation.
Pulmonary function was tested using SPIRODOC (MRI Medical Research International, Rome, Italy). The following parameters were recorded: forced vital capacity (FVC), forced expiratory volume in 1 second (FEV1), peak expiratory flow (PEF), and the FEV1/FVC ratio. All pulmonary function parameters were measured until three reproducible recordings were obtained and the best of three was used for analysis.
The 6MWT was conducted according to the standardized protocol. 11 The subject was instructed to walk up and down a measured corridor, covering as much ground as possible over a 6-minute period. The test was self-paced and the subject was allowed to rest if desired, although the clock continued to run. The wording of encouragement during the test was standardized (“keep going”, “you are doing fine”, and “everything is going well”) and provided by the same person at set times during the test. The 6-minute walk distance was also recorded.
The patients were also evaluated at T1 and T2 for back pain using the 10-unit colour Visual Analogue Scale (VAS). 12
Physical therapy
The patients performed a 12-week exercise programme that consisted of three sessions per week in the outpatient Rehabilitation Department. The goals of the rehabilitation treatment were to improve awareness of body alignment, axial elongation, derotation and stabilization of the spine, increase chest expansion, and enhance exercise capacity. The exercise programme consisted of stretching exercises on the concave side of scoliosis, strengthening exercises on the convex side of scoliosis, and breathing exercises. Some specific exercises for core stabilization were performed, including spider (patients faced the wall, leaned forward and walked with fingers up the wall rising to their toes, and after full extension, walked with the fingers back down), pelvic tilt, cat-camel pose, and basic trunk curl (crunch) exercises using a ball (back extensions, opposite arm, and leg rise), and quadriceps strengthening exercises, which are important in increasing work capacity. 13 Patients used rotational breathing respiratory exercises, such as contraction of convex areas of the trunk and directing inspired air in the concave areas. 14 The core stabilization programme was established according to the individual spinal characteristics.
Patients with moderate scoliosis also had the indication to wear a corrective orthosis (Chêneau brace) for 20 hours per day.
Statistical analysis
The sample size was calculated on the basis of results of Min-Jae and Dae-Sung using G*Power 3.1.9.2 (Universitat Kiel, Kiel, Germany) with the Wilcoxon signed-rank test. The effect size was 0.5, the type I error was α = 0.05, and power was 0.9. 15 A total sample size of 38 patients was required. Statistical analysis was performed using MedCalc Statistical Software version 17.9.5 (MedCalc Software, Mariakerke, Belgium). The distribution of continuous variables was tested for normality using the Shapiro–Wilk test. Descriptive statistics were calculated as mean and standard deviation for normally distributed data (general characteristics), and as median and interquartile range for non-normally distributed data (behavioural variables, respiratory parameters, 6-minute walk distance, and VAS).
Levene’s test was applied to test the homogeneity of variance between groups. One-way ANOVA and Fisher’s exact test were performed to compare demographic data (age, height, weight, and sex) between patients and controls.
The Wilcoxon signed-rank test was performed to compare respiratory and functional capacity parameters before and after 12 weeks of rehabilitation. Comparisons between the two groups were performed by the Mann–Whitney test. Spearman’s correlation coefficient was applied to investigate the relationships between pulmonary function, functional capacity, and pain. A p value <0.05 was considered statistically significant.
Results
Our study included 40 school children and adolescents with idiopathic scoliosis and 40 sex and age-matched healthy controls. The patients and control groups were homogenous in terms of anthropometrical characteristics (Levene’s test, p > 0.05) (Table 1). In patients, the Cobb angle at initial assessment was within 15° to 35° (mild or moderate scoliosis).
Baseline characteristics of patients and controls.

NS: not significant; SD: standard deviation.
Pulmonary function parameters and 6MWT results are shown in Table 2. In patients with scoliosis, all respiratory and functional capacity parameters were significantly improved after physical therapy (all p < 0.001). Before rehabilitation in patients, FVC, PEF, FEV1, FEV1/FVC, and the 6MWT showed significantly lower values compared with controls (all p < 0.05). In spite of the 12-week improvement, there were still significant differences between patients and controls in all of the assessed parameters (all p < 0.05, Table 2). Significant direct correlations were found between pulmonary function and functional capacity at T1 and T2 (all p < 0.001, Table 3).
Pulmonary function and functional capacity of patients and controls.

Parameters are shown as median and [interquartile range]. FVC: forced vital capacity; PEF: peak expiratory flow; FEV1: forced expiratory volume in 1 second; 6MWT: 6-minute walk test. T1: first evaluation, before rehabilitation; T2: second evaluation, after rehabilitation.Bold values: Any p < 0.05 indicates statistical significance.
Correlations between pulmonary function and functional capacity in patients.
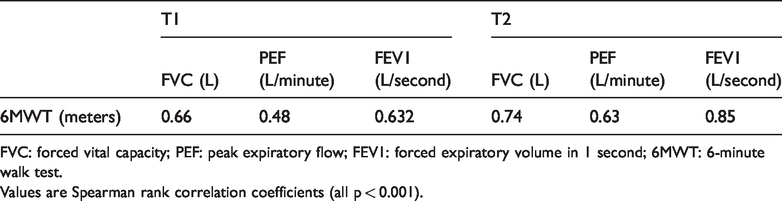
FVC: forced vital capacity; PEF: peak expiratory flow; FEV1: forced expiratory volume in 1 second; 6MWT: 6-minute walk test.
Values are Spearman rank correlation coefficients (all p < 0.001).
At the beginning of the study, 72.5% of patients had complaints of back pain. This pain was significantly decreased after the exercise programme compared with before beginning rehabilitation (T1: median VAS score = 2.50 [0–4]; T2: VAS score = 0.50 [0–2]; Z = −4.83, p < 0.001). None of the controls had any back pain.
With regard to physical activity behaviour, patients with scoliosis spent a significantly longer time at a computer and had less regular and competitive physical exercise compared with healthy children and adolescents (all p < 0.001, Table 4). Negative correlations between the hours of competitive and non-competitive practice of exercise per week and the VAS score indicated that when the time spent exercising was longer, the reported pain intensity was lower at T1 and T2 (T1: r = 0.49 for regular physical exercise time and r = 0.56 for competitive physical exercise time; T2: r = 0.49 for regular physical exercise time and r = 0.63 for competitive physical exercise time; all p < 0.001).
Behavioural variables in patients and controls.
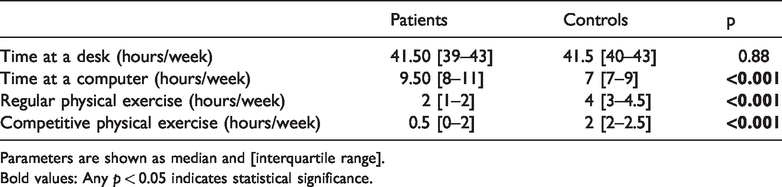
Parameters are shown as median and [interquartile range].Bold values: Any p < 0.05 indicates statistical significance.
Discussion
Our study assessed pulmonary function and functional capacity in children and adolescents with mild or moderate scoliosis (thoracic and thoraco-lumbar types). These patients performed a 12-week supervised physical exercise programme. We found that, in these children, pulmonary parameters and functional capacity were improved after 12 weeks of supervised physical therapy.
Szopa and Domagalska-Szopa 16 showed that, for 75% of 68 patients with mild idiopathic scoliosis, the values of the basic ventilation indicator (percentage of lung vital capacity) were within the normal range. Our study showed that, before starting rehabilitation, patients with mild or moderate idiopathic scoliosis had significantly lower FVC values compared with controls. Although this ventilatory parameter improved after the 12-week exercise programme, there was still a significant difference between patients and controls.
A recent study evaluated ventilatory function and functional exercise capacity in 73 adolescents with mild idiopathic scoliosis. 17 This previous study showed that FVC, FEV1, and the 6MWT were significantly lower in patients with scoliosis than in healthy controls. Our study also showed a significantly lower FVC and 6MWT time in children and adolescents with mild or moderate idiopathic scoliosis before starting rehabilitation compared with controls. We observed a lower PEF value in patients compared with controls. After rehabilitation, PEF and the 6MWT time were still lower in patients compared with controls.
We consider that a follow-up of the study patients is necessary. We recommend that rehabilitation be continued for at least 12 weeks. Correction of scoliosis can be quantified by radiological assessment (performed at least 6 months after the initial diagnosis), as well as improvement of pulmonary function (PEF) and functional capacity (6MWT). A previous study by Sperandio et al. 18 also suggested that walking-based aerobic exercises should be encouraged in adolescents with idiopathic scoliosis.
Sedrez et al. 19 evaluated the risk factors associated with structural postural changes in the spinal column in 28 of 59 children and adolescents who had scoliosis. Half of them spent 0 to 3 hours per day watching TV and 0 to 3 hours per day at the computer, while 71% spent time reading and studying in bed. In our study, all 40 patients with scoliosis spent at least 1 hour per day at the computer. Ten (25%) of our patients did not perform any type of physical exercise. Furthermore, 21 (52.5%) children and adolescents with scoliosis did not participate in any type of competitive sport.
We also assessed back pain in patients with scoliosis. At the beginning of the study, approximately three quarters of the patients had back pain, and at the final evaluation, only 50% still had back pain. We found a significant decrease in back pain in patients after the 12-week exercise programme. A recent study by Zapata et al. 20 also showed that 8 weeks of weekly spinal stabilization exercises led to a significantly reduced Numeric Pain Rating Scale score in adolescents with idiopathic scoliosis and low back pain. A study by Gennari et al. 21 of 116 adolescents with spinal pain showed that thoracolumbar scoliosis was the second most frequent aetiology (26% of patients); the pain was initially muscular. In our study, back pain was benign and none of the patients had any “red flag” signs (duration of back pain >4 weeks, fever, chills, night sweats, awakening at night with bone pain, point tenderness, neurological symptoms, history of cancer, or radiation of the anterior abdomen).
The findings of our study have important implications for schools and school-based health professionals involved in prevention and early diagnosis of postural changes of the spine. Our results confirm the importance of treating scoliosis as soon as possible after diagnosis in a rehabilitation centre under medical qualified supervision. Correction of scoliosis is still possible in children and adolescents and should be achieved if a supervised physical therapy programme is performed for a long time. The Scientific Society on Scoliosis Orthopaedic and Rehabilitation Treatment recommends physiotherapeutic scoliosis-specific exercises as the first step for treating idiopathic scoliosis to prevent or limit progression of the deformity and bracing. Scoliosis-specific exercise programmes should also be designed by specifically trained therapists. These programmes must be individualized and performed regularly throughout treatment. 11
In our study, we observed a high disproportion between the time spent in sitting positions (at a desk and at a computer) and the duration of physical exercise. Therefore, we recommend an increase in leisure and competitive sport activities in children and adolescents of all age groups.
There are some limitations of the present study. These limitations include the small number of patients, the different types of scoliosis (mild and moderate types), and the relatively short-term follow-up.
Conclusion
In children and adolescents with mild or moderate idiopathic scoliosis, pulmonary parameters and functional capacity improve after a 12-week supervised physical therapy programme. However, all ventilatory parameters and functional capacity measures are still lower after rehabilitation in patients compared with controls. This finding indicates the need for follow-up of the physical exercise for correction of scoliosis and for improving respiratory function and overall functional capacity.