
Abstract
Objective
To evaluate clinical and microbiological features in patients with nursing and healthcare-associated pneumonia (NHCAP), admitted to the intensive care unit (ICU).
Methods
Demographic, clinical and microbiological data were retrospectively reviewed from patients with NHCAP admitted to a respiratory ICU. Patients were categorized into one of four NHCAP groups: (A) residence in a long-term nursing-home setting or healthcare home; (B) hospital discharge in the preceding 90 days; (C) elderly or physically disabled patients who stay at home but require healthcare; (D) continuously receiving outpatient endovascular therapy including chronic dialysis, anticancer drugs, and immunosuppressants. Pneumonia severity index (PSI), CURB-65, duration of ICU stay and 30-day mortality were evaluated.
Results
Out of 428 patients reviewed (male, 67.1%; mean age, 71.2 ± 11.9 years), 30-day mortality was 25.5%, and duration of ICU stay was 13.8 ± 13.3 days. Mortality rate was not significantly different between the four NHCAP groups; duration of ICU stay was significantly longer in groups C and D. PSI score, serum HCO3– level, duration of ICU stay, extended spectrum β-lactamase (ESBL)-producing Klebsiella pneumoniae and multidrug resistant (MDR) Acinetobacter baumannii were significantly associated with 30-day mortality.
Conclusion
ESBL-producing K. pneumoniae, MDR A. baumannii and PSI score should be considered in ICU patients with NHCAP.
Introduction
Healthcare-associated pneumonia (HCAP) is defined as pneumonia that is present on admission, and occurs in patients who have recently been hospitalized, reside in a nursing home or have other recent healthcare exposures. In 2005, guidelines for the diagnosis and treatment of HCAP were published by the American Thoracic Society and the Infectious Disease Society of America. 1
Patients with pneumonia admitted to hospital from nursing homes are considered to have nursing home-acquired pneumonia. 2 The British Thoracic Society guidelines state that patients with nursing home-acquired pneumonia, which is usually categorized with HCAP, should be treated as having community-acquired pneumonia, because there is no difference in the distribution of causative pathogens between patients with nursing home-acquired pneumonia and other older adults with community-acquired pneumonia.2,3
Studies have argued that HCAP should be distinguished from community-acquired pneumonia, however, because of the higher prevalence of multidrug resistant (MDR) pathogens such as Pseudomonas aeruginosa and methicillin-resistant Staphylococcus aureus (MRSA) in HCAP.4,5 Consequently, guidelines recommend empirical antibiotic therapy with activity against these pathogens. 6 Despite these guidelines, there is disagreement about whether current HCAP criteria clearly identify patients at risk for MDR, and concerns that overtreatment with broad-spectrum antibiotics may produce selection pressure for MDR.7–9 Patients with HCAP have been shown to receive inappropriate initial antibiotic treatment more often than patients with community-acquired pneumonia,9,10 and inappropriate initial antibiotic treatment has been clearly associated with poor outcomes. 11
In 2011, the Japan Respiratory Society guidelines documented a new pneumonia category, known as nursing and healthcare-associated pneumonia (NHCAP), which is distinct from community-acquired pneumonia, relates to the pattern of drug-resistant pathogens and is relevant to healthcare insurance systems, including the nursing-care system.12,13 Similar healthcare/nursing-care systems exist in the Republic of Korea and many patients with NHCAP are admitted to tertiary hospitals that have an intensive care unit (ICU). Limited studies exist, however, relating to NHCAP requiring ICU admission; some studies12,13 suggest that NHCAP could be categorized into several groups according to patients’ comorbid diseases and clinical characteristics.
The aim of the present study was to identify the clinical and microbiological features of patients with severe NHCAP requiring ICU treatment, and to clarify the prognostic factors for 30-day mortality. The study focused on the patients’ background, clinical characteristics, disease severity including pneumonia severity index (PSI) and CURB-65,14,15 the pathogen profile, and patient outcomes.
Patients and methods
Study design and population
This retrospective, observational cohort study included patients with NHCAP (aged ≥20 years) who were admitted to the ICU in a respiratory centre of Yonsei University Wonju Severance Christian hospital (an 850-bed tertiary hospital), Wonju, Korea between January 2008 and December 2012. Pneumonia was defined according to the criteria of the US Centers for Disease Control and Prevention. Diagnosis required two or more of the following criteria to be met: fever increase of ≥1℃ or body temperature >38.3℃; leukocytosis (25% increase in leukocytes and ≥10 × 109/l) or leukopenia (25% decrease in leukocytes and ≤5 × 109/l); and purulent tracheal secretion (>25% neutrophils per high-power field). Diagnosis also required one of the following criteria to be met: new or persistent infiltration on chest radiography; some microorganisms isolated from pleural effusion and tracheal secretion; radiographic cavitation or histological evidence of pneumonia pathogens; or positive sputum culture from a quantitative bacterial bronchoalveolar lavage (BAL) culture.
For the present study, the eligibility of patients with NHCAP for ICU admission was determined by the attending physicians (S.H.K., S.J.Y, K.C.S., W.Y.L.), based on PSI score and other medical conditions. Pneumonia occurring among outpatients in contact with a nursing home, healthcare system or endovascular therapy was defined as NHCAP. Patients who met the following criteria were excluded: community-acquired pneumonia; cardiac disorders including uncontrolled heart failure or acute myocardial infarction within one month of ICU admission; transfer to another hospital during the admission process; patients between 18 and 20 years old (according to the recommendation of the Institutional Review Board that required written agreement to review patients <20 years of age). For analyses, patients were divided into four NHCAP groups, and survivor and nonsurvivor groups.
This research was conducted in compliance with the requirements and under the authorization of the Yonsei University Wonju Severance Christian Hospital Institutional Review Board (IRB No. CR313026). Patients included in the study provided verbal informed consent.
Categorization of NHCAP
Patients with NHCAP were categorized according to the following four groups: (A) residence in a long-term nursing-home setting or healthcare home; (B) hospital discharge in the preceding 90 days; (C) elderly or physically disabled patients who stay at home but require healthcare; (D) continuously receiving outpatient endovascular therapy including chronic dialysis, anticancer drugs, and immunosuppressants.1,12,13 Patients with NHCAP who met the criteria for more than one category were classified according to the most appropriate category prior to admission. All patients who underwent treatment with chronic dialysis, anticancer drugs or immunosuppressants prior to admission were classified into group D regardless of the other features. Any patient who was not already classified into group D and who had a history of hospitalization within 90 days of ICU admission, regardless of nursing-home or healthcare residence, was classified as group B. Remaining patients were classified as category A or C according to whether nursing-home/healthcare residence or stay at home status.
ICU admission and severity of illness assessment
American Thoracic Society/Infectious Disease Society of America guidelines were used to identify two major criteria to determine ICU admission: septic shock requiring vasopressor support; requirement for mechanical ventilation. The presence of at least three other minor criteria were also used to determine ICU admission: respiratory rate ≥30 breaths/min, PaO2/FiO2 ratio ≤250, multilobar infiltrates, confusion, blood urea nitrogen (BUN) ≥20 mg/dl; hypotension requiring fluid support. 16
Illness severity was assessed using the Acute Physiology and Chronic Health Evaluation II score, 17 PSI and CURB-65. The PSI is based on derivation and validation cohorts of outpatients hospitalized with community-acquired pneumonia, 14 and is calculated from data regarding age, complications, and physical examination and laboratory findings on admission. CURB-65 15 was identified by the following criteria; confusion, BUN, respiratory rate, blood pressure and age ≥65 years.
Microbiological investigation
Microbiological tests were performed for all patients with NHCAP on admission, to identify possible causative pathogens. Briefly, samples of sputum, tracheobronchial aspirates, BAL fluid, pleural fluid and blood were cultured in a semiquantitative manner. Sputum data were only evaluated when a Gram-stain test revealed numerous leukocytes (>25 in a × 100 magnification microscopic field) and few squamous epithelial cells (<10 in a × 100 magnification microscopic field). Serologic tests were performed to detect antibodies against Mycoplasma pneumoniae and Chlamydophila pneumoniae.18,19 Streptococcus pneumoniae and Legionella pneumophila serogroup 1 antigens in urine were tested by immunochromatography.20,21
Causative pathogens of pneumonia met one of the following criteria: sputum Gram stain showing phagocytic cells and bacteria equivalent to 103–105 colony-forming units (CFU)/ml in sputum culture; >106 CFU/ml bacteria in the sputum culture; blood culture-positive; positive urinary pneumococcal or urinary Legionella antigen-test results; positive antibody titers against M. pneumoniae and C. pneumoniae. 22
Susceptibility tests focused on antibiotics frequently prescribed or recommended for the treatment of pneumonia, including antipseudomonal penicillins, carbapenems, cephalosporins, aminoglycosides and quinolones. MRSA (oxacillin minimum inhibitory concentration ≥4 µg/ml), and resistant strains of P. aeruginosa, extended-spectrum β-lactamase (ESBL)-producing Klebsiella pneumoniae and other Gram-negative bacilli including Acinetobacter baumannii, were designated as antibiotic-resistant organisms. Bacteria were defined as MDR if they were found to be resistant to at least three antimicrobial classes. 23
Antibiotic treatment
Antibiotic therapy was initiated based on the American Thoracic Society/Infectious Disease Society of America guidelines, 1 but the detailed antibiotic regimen was defined by the attending physician (S.H.K. S.J.Y., K.C.S., W.Y.L.), taking into consideration patient risk factors and disease severity. Empirical antibiotic therapy was modulated according to the susceptibility test result for an identified pathogen, or the physician’s decision in response to the patient’s condition. Empirical antibiotic therapy was defined as inappropriate when the antibiotics used were not effective against the identified pathogens based on in vitro susceptibility tests.
Data collection
Comorbid diseases such as chronic respiratory disease, diabetes mellitus, and cardiac, liver, renal, malignant or central nervous system diseases were reviewed according to medical records. Patients’ age, sex and laboratory data on admission to ICU (including leukocyte counts, haemoglobin, arterial blood gas analyses, serum bicarbonate ion [HCO3–], albumin, C-reactive protein [CRP], serum BUN and creatinine data) were also reviewed. Patients were classified into three groups based on PSI score: I–III (<90 points), IV (91–130 points) and V (>131 points), 14 and were also classified into 3 groups based on CURB-65 score: 0 or 1, 2 and 3–5. 15
Endpoints
The primary endpoint was 30-day mortality following ICU admission. Secondary endpoints were duration of ICU stay and requirement for mechanical ventilation.
Statistical analyses
Statistical analyses were performed using SPSS®, version 18.0 (SPSS Inc., Chicago, IL, USA). χ2-test or Fisher’s exact test were used to analyse categorical variables and Student’s t-test or Mann–Whitney U-test was used to analyse continuous variables. One-way analysis of variance was used to compare continuous variables between three or more groups. To identify independent prognostic factors for 30-day mortality among the variables that showed statistically significant associations in univariate analysis, multivariate logistic regression analysis was performed. Relative risks were expressed as odds ratio (OR) and 95% confidence interval (CI). Continuous variables are presented as mean ± SD and a P-value >0.05 was considered to be statistically significant.
Results
Patient disposition
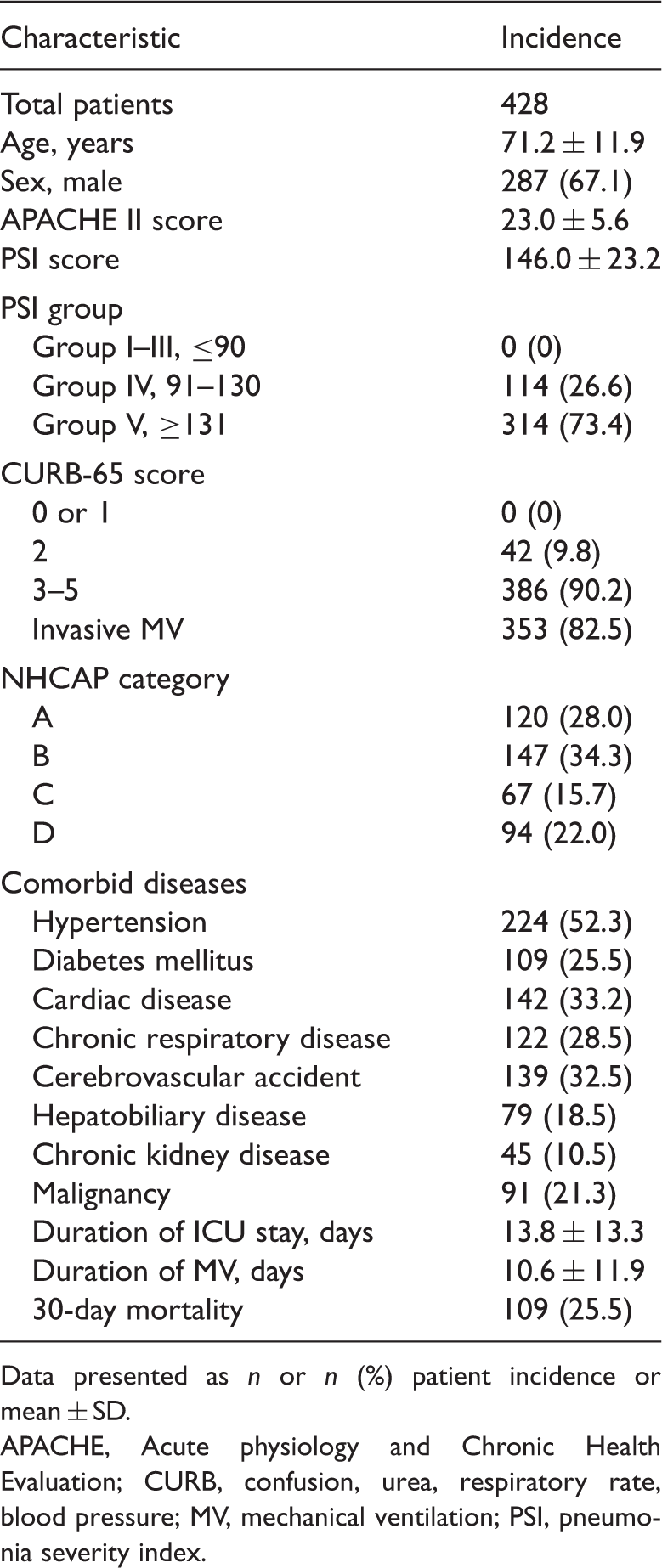
A total of 428 patients with NHCAP were included for analyses (Figure 1), with mean age, 71.2 ± 11.9 years and 287 (67.1%) male patients. Clinical characteristics and pneumonia severity on admission to ICU are shown (Table 1). Patients were divided into four NHCAP categories as follows: A, 120 patients (28.0%); B, 147 patients (34.3%); C, 67 patients (15.7%); and D, 94 patients (22.0%) (Table 2).
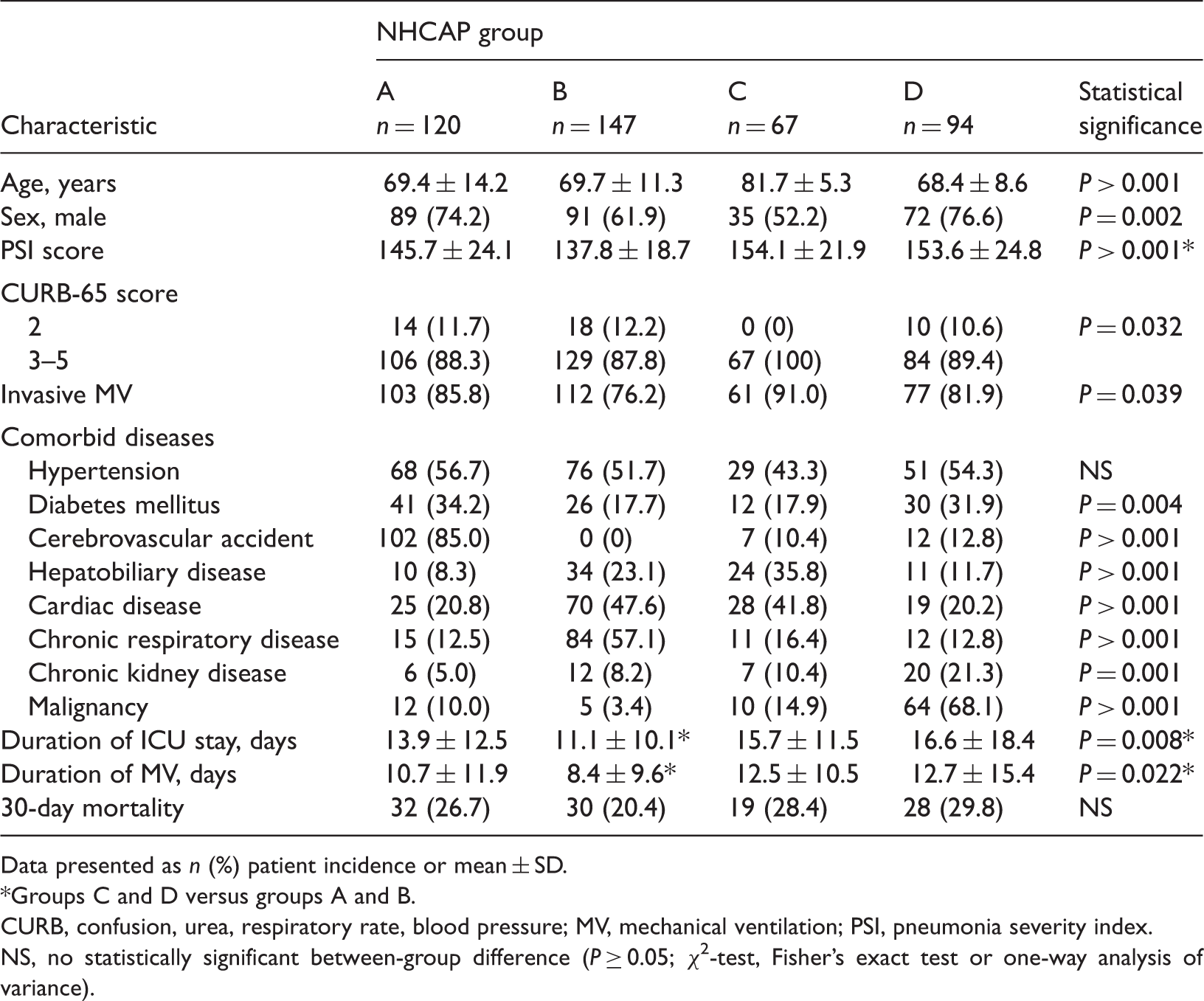
Flowchart showing identification of patients with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit (ICU). CHF, congestive heart failure; MI, myocardial infarction; MV, mechanical ventilation. Demographic and clinical characteristics of patients diagnosed with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit (ICU). Data presented as n or n (%) patient incidence or mean ± SD. APACHE, Acute physiology and Chronic Health Evaluation; CURB, confusion, urea, respiratory rate, blood pressure; MV, mechanical ventilation; PSI, pneumonia severity index. Characteristics of patients diagnosed with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit (ICU), categorized according to NHCAP group. Data presented as n (%) patient incidence or mean ± SD. Groups C and D versus groups A and B. CURB, confusion, urea, respiratory rate, blood pressure; MV, mechanical ventilation; PSI, pneumonia severity index. NS, no statistically significant between-group difference (P ≥ 0.05; χ2-test, Fisher’s exact test or one-way analysis of variance).
Clinical characteristics according to NHCAP category
Clinical characteristics were assessed according to NHCAP category (Table 2). Patients’ age (P < 0.001) and sex (P = 0.002) were significantly different between the four groups. PSI score (P < 0.001) was significantly higher, and duration of ICU stay (P = 0.008) and duration of mechanical ventilation (P = 0.022) were significantly longer in groups C and D compared with groups A and B. Underlying comorbid diseases were also significantly different between the four groups. There was no statistically significant between-group difference in 30-day mortality (P = 0.349; Table 2).
Comparison of clinical characteristics between survivor and nonsurvivor groups
Clinical characteristics of patients diagnosed with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit (ICU), categorized into survivor and nonsurvivor groups.

Data presented as n (%) patient incidence or mean ± SD.
Initial PCT results were available for 164 patients in the survivor group and 58 patients in the nonsurvivor group.
BUN, blood urea nitrogen; CI, confidence interval; CRP, C-reactive protein; CURB, confusion, urea, respiratory rate, blood pressure; HCO3−, serum bicarbonate ion; MV, mechanical ventilation; OR, odds ratio; PaO2, arterial oxygen pressure; PCT, procalcitonin; PSI, pneumonia severity index.
NS, no statistically significant between-group difference (P ≥ 0.05; χ2-test, Fisher’s exact test or Student’s t-test).
Microbiological distribution and antibiotic treatments in survivor and nonsurvivor groups
Microbiological distribution in patients diagnosed with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit, categorized into survivor and nonsurvivor groups.

Data presented as n (%) patient incidence.
Polymicrobial pathogens: MRSA and ESBL-producing K. pneumoniae (n = 2 in survivor, n = 3 in nonsurvivor group); MRSA and K. pneumoniae (n = 2 in survivor group); MRSA and A. baumannii (n = 2 in survivor, n = 3 in nonsurvivor group); P. aeruginosa and S. pneumoniae (n = 1 in survivor group); P. aeruginosa and ESBL-producing K. pneumoniae (n = 1 in nonsurvivor group); and MRSA and H. influenzae (n = 1 in survivor group).
Others: Moraxella catarrhalis (n = 1 in survivor, n = 1 in nonsurvivor group).
CI, confidence interval; ESBL, extended-spectrum β-lactamase; MDR, multidrug resistant; OR, odds ratio; MRSA, methicillin-resistant Staphylococcus aureus; MSSA, methicillin-sensitive Staphylococcus aureus.
NS, no statistically significant between-group difference (P ≥ 0.05; χ2-test and Fisher’s exact test).
Antibiotic treatment in patients diagnosed with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit, categorized into survivor and nonsurvivor groups.
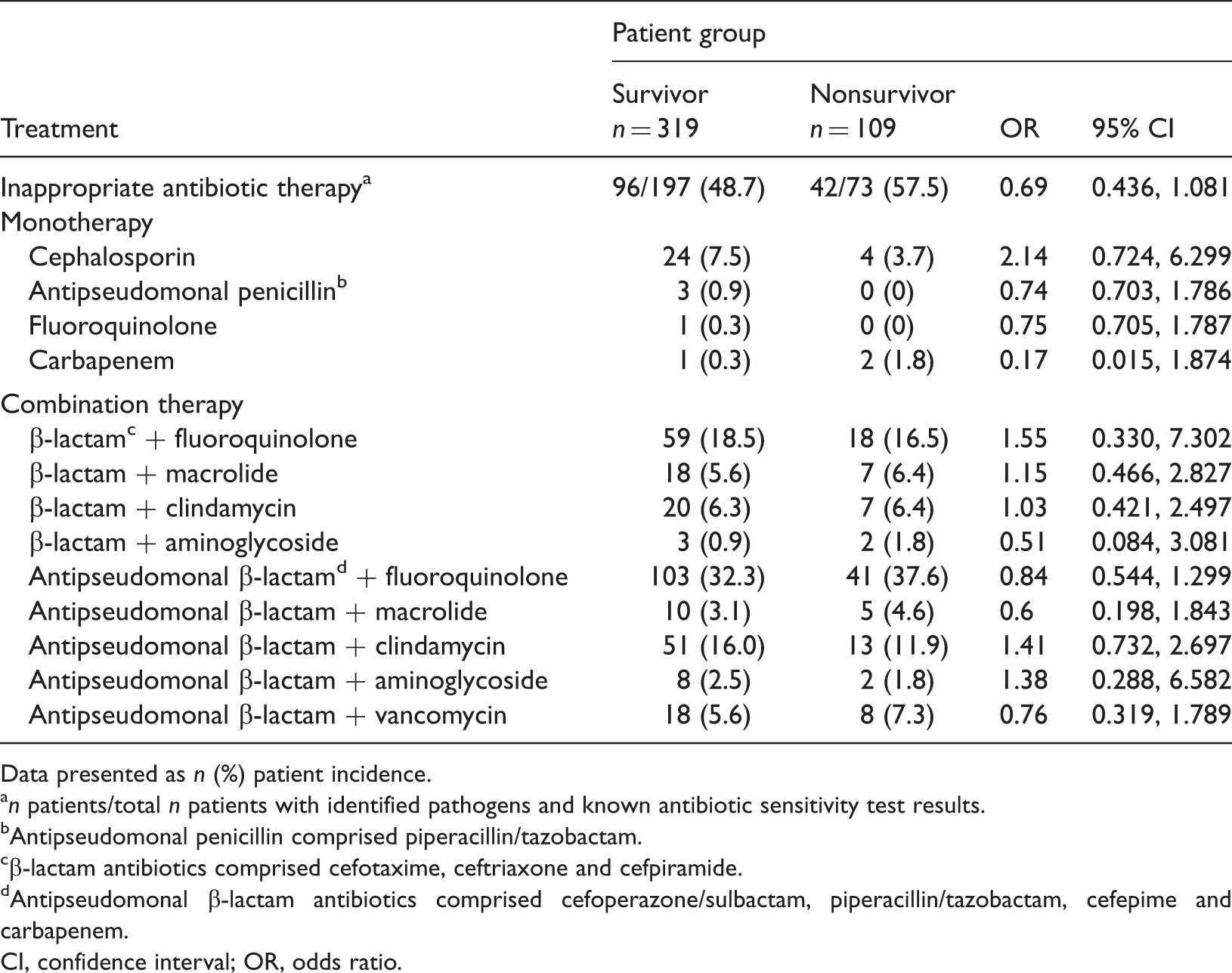
Data presented as n (%) patient incidence.
n patients/total n patients with identified pathogens and known antibiotic sensitivity test results.
Antipseudomonal penicillin comprised piperacillin/tazobactam.
β-lactam antibiotics comprised cefotaxime, ceftriaxone and cefpiramide.
Antipseudomonal β-lactam antibiotics comprised cefoperazone/sulbactam, piperacillin/tazobactam, cefepime and carbapenem.
CI, confidence interval; OR, odds ratio.
Multivariate logistic regression analysis of factors associated with 30-day mortality
Univariate and multivariate logistic regression analyses of factors associated with 30-day mortality in patients diagnosed with nursing and healthcare-associated pneumonia (NHCAP) admitted to an intensive care unit (ICU).
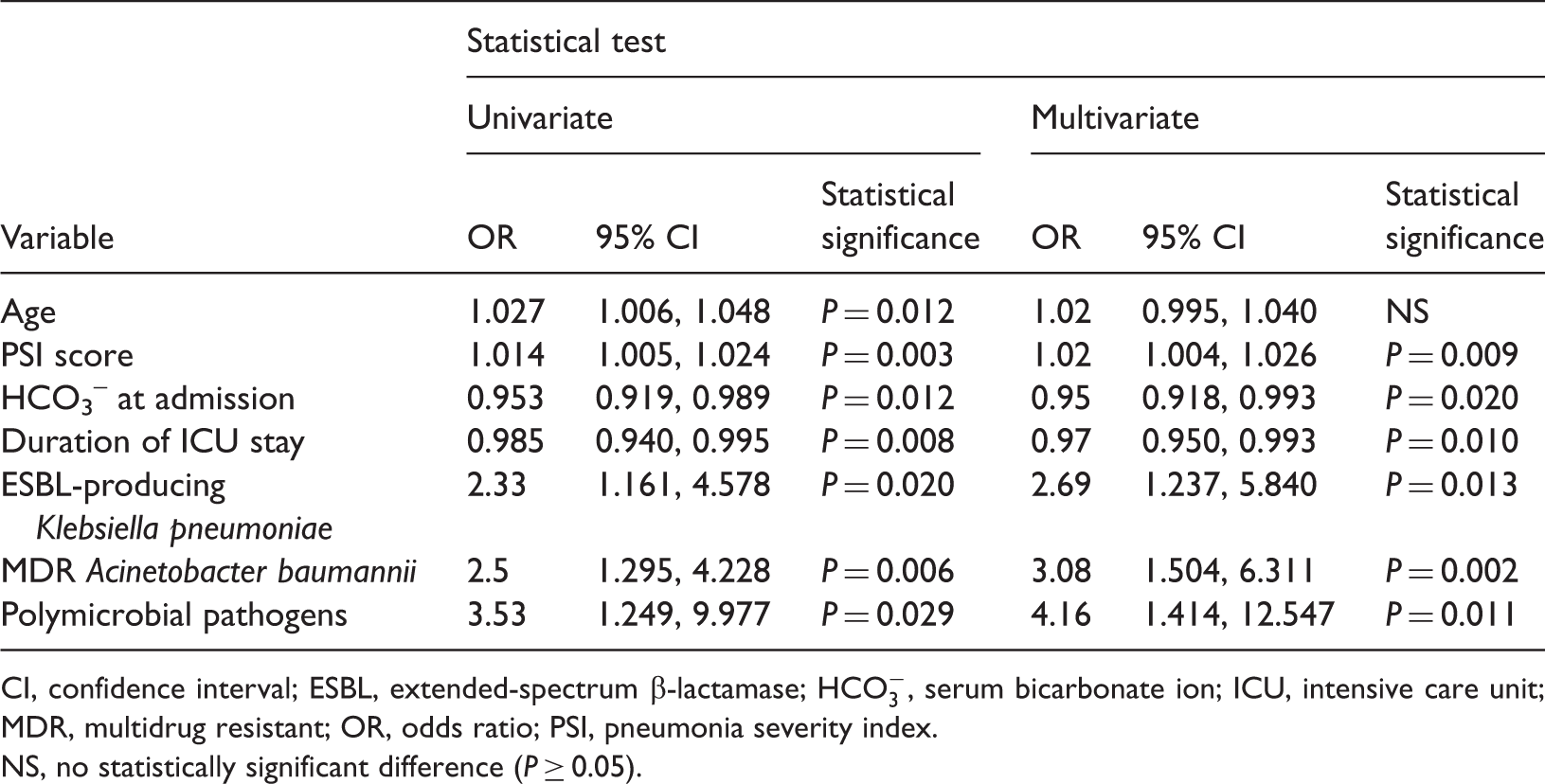
CI, confidence interval; ESBL, extended-spectrum β-lactamase;
NS, no statistically significant difference (P ≥ 0.05).
Discussion
Patients with HCAP may be at increased risk of infection with antibiotic-resistant organisms, and initial inadequate antibiotic coverage may increase the mortality rate. Patients with HCAP differ from those with community-acquired pneumonia in terms of microbial aetiology, antibiotic therapy and clinical outcomes, despite similar age and sex, due to the poorer functional status.5,24,25 In the present study, PSI score, low serum
Patients with NHCAP can be categorized into four groups. 13 In the present study, each group showed different characteristics in terms of age, sex, and comorbid diseases; groups A and B had significantly different PSI scores, duration of ICU stay, and duration of mechanical ventilation compared with groups C and D. Other studies have suggested that underlying comorbid diseases, including malignancy, may increase in-hospital mortality in patients with HCAP,24,25 however, the present investigation revealed no significant difference in 30-day mortality according to NHCAP category in ICU patients, although the comorbid diseases were found to differ between categories.
The PSI score and duration of ICU stay were found to be significantly associated with 30-day mortality in the present study. A previous report 26 showed prognostic scoring, including PSI, was good for predicting mortality in nonimmunocompromised patients with HCAP. Another study 27 also suggested that PSI could be applied to assess the severity of illness in the management of patients with HCAP, although the discriminatory powers of PSI for 30-day mortality were significantly lower in patients with HCAP compared with community-acquired pneumonia. Other studies6,8,28 have proposed that advanced care, or interventions including ICU admission and invasive mechanical ventilation, may be partially responsible for increased mortality in patients with HCAP. Studies also suggest that a longer duration of ICU stay may be associated with increased chance of invasive procedure, including nasogastric tube feeding or central catheterization, which may cause opportunistic infections such as MRSA, Escherichia coli, P. aeruginosa, or K. pneumoniae and increased in-hospital mortality rates.4,28
A lower serum
In the present study, the most frequently identified pathogen was MRSA rather than S. pneumoniae or P. aeruginosa, however, these pathogens did not affect 30-day mortality in ICU patients with NHCAP. Several studies30,31 have suggested that MRSA does not affect pneumonia-related mortality, particularly ventilator-associated pneumonia in ICU patients. Guideline-concordant HCAP therapy in cases of S. aureus or P. aeruginosa infection is also suggested to have no association with improved 30-day mortality. 6
Differences in initial antibiotic treatments between survivors and nonsurvivors were analysed in the present study and therapeutic regimens (including mono- or combination therapy) did not significantly differ between the two groups. There was no statistically significant difference in administration of inappropriate antibiotic treatment between the nonsurvivor and survivor groups, suggesting that inappropriate antibiotic treatment at admission in ICU patients with NHCAP does not affect 30-day mortality rates.
Conversely, the present study showed that ESBL-producing K. pneumoniae and MDR A. baumannii were significantly associated with infections in the nonsurvivor group, and that these two pathogens were associated with 30-day mortality. A recent study 32 suggested the MDR pathogens did not increase the mortality in patients with NHCAP, therefore, inappropriate overuse of broad-spectrum antibiotics should not be advised. Compared with patients with community-acquired pneumonia, however, those with HCAP were reported as frequently infected by MDR pathogens, 10 and the present data also showed that 13.8% of patients with NHCAP were identified with MDR pathogens. Risk factors including ICU care and poor performance score may be associated with potential MDR pathogens in patients with HCAP, 33 and the present study showed that ESBL-producing K. pneumoniae and MDR A. baumannii were significantly associated with 30-day mortality. These MDR pathogens are known to be significantly associated with severity of underlying disease, duration of prior hospital admission and prior use of third-generation cephalosporin.34,35 Limited antibiotic choice for treating MDR pathogens may also be associated with higher rates of in-hospital mortality, however there are few studies relating to MDR A. baumannii in patients with HCAP, even though these patients are at higher risk of potential MDR Acinetobacter species. 36
The results of the present study may be limited by several factors. First, given its retrospective nature, selection bias may have influenced the significance of the present findings and the possibility of recording errors related to baseline clinical data cannot be excluded. Secondly, the present study was performed in a single institution, thus a multicentre study is required to validate the results. Thirdly, the characteristics of the four NHCAP subcategories occasionally overlapped in some patients, therefore, a more robust classification system is required. Despite these limitations, the present study evaluated clinical features in patients with NHCAP requiring ICU treatment, categorized into four NHCAP groups, and identified prognostic factors associated with mortality.
In conclusion, 30-day mortality was not significantly different between four NHCAP subcategories
13
in ICU patients with NHCAP. PSI score, duration of ICU stay, serum
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Acknowledgements
The authors thank all members of the Department of Internal Medicine, Yonsei University Wonju College of Medicine, and Yonsei University Wonju Severance Christian hospital.