
Abstract
Introduction
Pneumonia caused by multidrug-resistant Acinetobacter baumannii (MDRAB) often leads to prolonged hospitalization, increased treatment costs and high death rates.1–3 Moreover, hospital-acquired A. baumannii infection rates have increased rapidly in recent years, particularly in intensive care units (ICU), possibly because of the high prevalence of MDRAB strains.1,4–7
Tigecycline (TC) is a glycylcycline antibiotic developed to address the globally emerging crisis of antibiotic resistance; it was first approved for clinical use in 2005.8,9 Although clinical data on TC are sparse and its effects are often modified by other concurrently used antibiotics,10–12 in vitro analyses have shown that TC has antibacterial activity against A. baumannii.13–15 Susceptibility testing has also demonstrated that TC can be used for the treatment of drug-resistant bacteria.16, Indeed, some retrospective studies involving small sample sizes have shown that TC is effective in MDRAB nosocomial and hospital acquired pneumonia.16,17 However, studies comparing the clinical efficacy of TC with other antibiotics in the treatment of MDRAB infection in patients with hospital-acquired pneumonia are few and prognostic indicators have not been defined.
The aim of this retrospective study was to evaluate outcomes and prognostic risk factors of TC-based treatment by comparison with those of other antibiotic-based treatments in the treatment of hospital-acquired pneumonia caused by MDRAB.
Patients and methods
This retrospective study included all patients ≥18 years who were consecutively admitted to the ICU at Xiangya Hospital, Central South University, Changsha, China between January 2016 and June 2017 with hospital-acquired pneumonia involving monomicrobial MDRAB. Patient data were collected from the hospital’s electronic medical records system. The study was approved by the Ethics committee of Xiangya Hospital, Central South University and because of the study’s retrospective design, there was no requirement for patients’ informed consent.
Hospital-acquired pneumonia was defined as pneumonia that occurred 48 h or more after admission.18,19 MDRAB was defined as the A. baumannii isolate was resistant to representative antibiotics from at least three different classes of antimicrobial agents such as aminoglycosides, β-lactams, quinolones, and/or tetracyclines. 19
Depending on their antibiotic treatment, patients were separated into a ‘TG’ and a ‘non-TG’ group. Patients in the TG group had received TG alone or in combination with other antibiotics. TG had been administered for five days with a 100 mg IV loading dose followed by 50 mg IV every 12 h. Patients in the non-TG group had received carbapenem-based (i.e., imipenem-cilastatin, 500mg IV every 6 h or meropenem, 1 g IV every 8 h) and/or cefoperazone/sulbactam-based (i.e., 3g IV every 8 h for at least five days) regimens.
Baseline demographic data, laboratory test results, Acute Physiology and Chronic Health Evaluation II (APACHE II) scores, 20 Glasgow Coma Scale (GCS) scores 21 and presence of sepsis were recorded. The diagnosis of sepsis had been made according to established criteria. 22 Other risk factors recorded were: antibiotic use in the previous three months; bedsores; mechanical ventilation, urethral and/or deep vein catheterisation; immunosuppressive drug use; sepsis; primary infection site; mixed infections; treatment details; length of hospitalization; ICU duration; death; microbial and clinical outcomes.
Clinical prognosis at the end of treatment was defined as good (complete or partial resolution of symptoms/signs of infection) or poor (no improvement or deterioration of signs/symptoms of infection). Primary bacteraemia was defined as bacteraemia associated with catheter-related infections, whereas secondary bacteraemia was defined as bacteraemia that developed subsequent to the primary infection. 23
Statistical analyses
Data were analysed using the Statistical Package for Social Sciences (SPSS®) for Windows® release 22.0 (IBM Corp., Armonk, NY, USA). All tests were two-sided and a P-value <0.05 was considered to indicate statistical significance. Quantitative data were expressed as median and interquartile range and were analysed using the Mann-Whitney test. Numerical data were expressed as a percentage and were analysed using the χ2 test. Odd ratios (ORs) and 95% confidence intervals (CIs) were calculated for all potential risk factors for poor prognosis. All variables were included in the univariate analysis and those with a P value of 0.05 were included in a logistic regression model for multivariate analysis.
Results
Of the 86 MDRAB-positive patients with hospital-acquired pneumonia that were identified for the study, 59 were in the TC group and 27 were in the non-TC group. In terms of baseline demographic data, there were no significant differences between groups in median age, sex and concomitant diseases, apart from coronary heart disease which was significantly more prevalent in the TC group (51% vs. 26%, P = 0.03; Table 1).
Pre-treatment demographic characteristics of patients with hospital-acquired pneumonia involving multidrug-resistant A. baumannii.
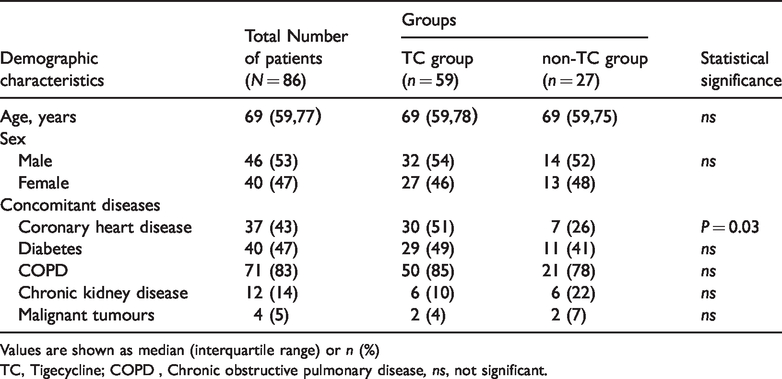
Values are shown as median (interquartile range) or n (%)
TC, Tigecycline; COPD , Chronic obstructive pulmonary disease, ns, not significant.
There were also no differences between groups in baseline risk factors. These included: the proportion of patients who had used antibiotics in the previous three months; occurrence of bedsores; mechanical ventilation use (approximately 90% of patients); patients who underwent deep vein catherization; long-term immunosuppressive drug use (Table 2). However, fewer patients in the non-TC group had urethral catherization compared with the TC group (82% vs. 97%; P = 0.029).
Pre-treatment risk factors of patients with hospital-acquired pneumonia involving multidrug-resistant A. baumannii.

Values are shown n (%)
TC, Tigecycline, ns, not significant.
Although there were no significant differences between the two groups in the incidence of fever, disease severity (i.e., APACHE II and GCS scores) and most baseline laboratory measures, patients in the non-TC group had higher median serum creatinine levels compared with the TC group (86 vs 68 µmol/l, P = 0.032; Table 3). Furthermore, sepsis was more common in the TC group than the non-TC group (61% vs. 22%, P = 0.001).
Pre-treatment clinical characteristics of patients with hospital-acquired pneumonia involving multidrug-resistant A. baumannii.

Values are shown as median (interquartile range) or n (%)
TC, Tigecycline, GCS, Glasgow Coma score; APACHE II score, acute physiology and chronic health evaluation II score, ns, not significant.
Pre-treatment microbial records showed that the respiratory tract was the most common site of primary infections in both groups (Table 4). However, primary bacteraemia (defined as catheter related) was more common in the TC group compared with the non-TC group (29% vs. 7%). In addition, co-infection with other bacteria or fungi was present in most patients from both groups. Patients in the TC group showed a higher prevalence of Candida albicans co-infection and patients in the non-TC group patients had a higher prevalence of Pseudomona aeruginosa co-infection (P = 0.026) (Table 4).
Pre-treatment microbial characteristics of patients with hospital-acquired pneumonia involving multidrug-resistant A. baumannii.

Values are shown as n (%)
TC, Tigecycline.
In terms of outcomes following treatment of MDRAB caused hospital-acquired pneumonia, the median duration of treatment was shorter for the TC group compared with the non-TC group (12 vs. 14 days, P = 0.047) but the proportion of patients that required a change in antibiotic therapy was significantly greater in the TC group compared with the non-TC group (25 vs 9; P = 0.025; Table 5). However, there were no significant differences between groups in 28-day death rates, duration of hospital or ICU stay. For microbial outcome, the non-TC group had a higher A. baumannii clearance rate than the TC group (19% vs. 3%, P = 0.029). Nevertheless, the TC group had more patients with improved clinical symptoms than the non-TC group (73% vs. 48%, P = 0.026). Interestingly, approximately 50% of patients in each group had a poor response (Table 5).
Outcomes following treatment for hospital-acquired pneumonia involving multidrug-resistant A. baumannii.

Values are shown as median (interquartile range) or n (%)
#Total duration of antibiotic use
*Improvement resulting from all antibiotics used
TC, Tigecycline; HAP, hospital-acquired pneumonia, ns, not significant.
Univariate logistic regression analysis showed that predictors of a poor clinical prognosis were procalcitonin concentration, blood urea nitrogen concentration, sepsis, and APACHE II scores. As these variables were not co-linear, a multivariate logistic regression analysis was applied to the data to determine whether they independently affected the clinical prognosis. Results showed that sepsis (OR, 8.48), increased PCT concentration (OR, 1.11), and increased APACHE II scores (OR, 1.12) were risk factors associated with a poor clinical prognosis for patients with MDRAB related hospital-acquired pneumonia. In comparison, TC therapy was a protective factor (OR = 0.08) (Table 6).
Univariate and multivariate analyses of predictors for a poor clinical response following antibiotic treatment of hospital-acquired pneumonia involving multidrug-resistant A. baumannii.

TC, Tigecycline; COPD, Chronic obstructive pulmonary disease; ICU, intensive care unit; GCS, Glasgow Coma score; APACHE II score, acute physiology and chronic health evaluation II score; HAP, hospital-acquired pneumonia; MDRAB, multidrug-resistant Acinetobacter baumannii, ns, not significant.
Discussion
A. baumannii is a non-fermenting, gram-negative bacillus that is widely distributed in the hospital environment and can survive on artificial surfaces for long periods. 24 Accordingly, the pathogen is responsible for a significant percentage of hospital-acquired infections. 24 Strains of A. baumannii often display high levels of drug resistance, achieved via the expression of antibiotic-inactivating enzymes and mutation of antibiotic targets, which present a significant challenge for the control and treatment of this pathogen. 24 Although immunotherapy-based treatments for A. baumannii infection have shown promising activity,25,26 their potential therapeutic use remains to be determined. Treatment of A. baumannii infections typically include control measures aimed at reducing the invasive spread of infection. The antibiotic, TC has been shown to have activity against multidrug-resistant Acinetobacter species. 27 Moreover, a study from nine cities in China demonstrated that a majority of A. baumannii isolates were susceptible to TC. 28 However, while some studies have found that TC can be used successfully in hospital hospital-acquired pneumonia caused by MDRAB infection, 29 others have found that the clinical outcomes following TC treatment were suboptimal. 17 In addition, controversy exists regarding all-cause mortality rates and tissue concentration levels associated with TC.30,31
The findings of this retrospective review of cases showed that while the 28-day death rates, length of ICU and hospital stay were not significantly different between the two groups, the TC group had a better long-term clinical prognosis compared with the non-TC group. Nevertheless, the non-TC group showed a higher pathogen clearance rate compared with the TC group. Interestingly, significantly more patients in the TC group than in the non-TC group had switched their antibiotics. The observed lack of efficacy of TC in this current study may have been influenced by the fact that the majority of patients were in the terminal stages of severe infection prior to the administration of TC, and that TC was most likely used as a last-line antibiotic. We speculate that an increased dose of TC may have increased its efficacy, which is supported by the findings of a study in patients with ventilator-associated pneumonia who tended to have better clinical outcome if they were treated with a high-dose regimen of TC. 9
Although there were no differences between groups in procalcitonin levels and APACHE II scores, multivariate analysis showed that both these factors were prognostic markers for a poor clinical response. In addition, sepsis, which was more common in the TC group, and TC treatment were also prognostic markers for a poor clinical response in hospital-acquired pneumonia caused by MDRAB. Interestingly, antibiotic switch and pathogen clearance were non-significant prognostic factors
Further studies are required to evaluate our findings which were probably influenced by the retrospective design of the study based on information from patients who were receiving multidrug based TC regimens. Other limitations of our study included its small sample size, single centre design and the imbalance in study group numbers; more than twice as many patients were in the TC group compared with the non-TC group. More multicentre, prospective, controlled studies involving large number of patients are needed to examine the long-term efficacy and safety of TC for the treatment of hospital-acquired pneumonia caused by MDRAB.
In summary, our results show that TC based therapy was associated with a positive clinical response in the treatment of MDRAB caused hospital-acquired pneumonia and should perhaps be considered for use in severe cases as a last-line antibiotic as part of combination therapy.
Footnotes
Acknowledgements
We thank Tamsin Sheen, PhD, from Liwen Bianji, for editing the manuscript.
Declaration of conflicting interests
The authors declare that there are no conflicts of interest.
Funding
Project Supported by National Key R&D Program of China (2018YFC1311900) and National Natural Science Foundation of China (81770080).