
Abstract
Objectives
To evaluate the effectiveness of topical eutectic mixture of local anaesthetics (EMLA®) cream in reducing the pain associated with vaccination injections.
Methods
This was a randomized, double-blind, placebo-controlled study that included children who presented for routine immunization. Eligible children were randomly assigned to receive either EMLA® or placebo cream. The Modified Behavioural Pain Scale (MBPS) was used to assess baseline and postvaccination pain scores, while a visual analogue scale (VAS) was used to assess pain at the time of the needle prick and at the end of the injection.
Results
A total of 107 children were enrolled in the EMLA® group and 109 children in the placebo group. The difference between the pre- and postvaccination MBPS scores was significantly lower in the EMLA group than in the placebo group (2.56 ± 1.96 versus 3.95 ± 2.20, respectively). The VAS scores at the time of the needle prick and after the injection were significantly lower in the EMLA® group compared with the placebo group (1.60 ± 1.67 versus 3.24 ± 2.01; 3.29 ± 2.27 versus 4.86 ± 2.20; respectively).
Conclusions
Application of EMLA® cream can be effectively incorporated as a routine pain-relieving intervention within routine vaccination appointments.
Keywords
Introduction
Pain in children is underestimated globally and continues to be suboptimally managed.1–3 Currently, vaccine injections are considered to be the most common source of iatrogenic pain in childhood.3,4 They are repeatedly administered to almost all children throughout infancy, childhood and adolescence. Vaccine injections cause pain, anxiety and fear in paediatric patients.5,6 The pain associated with such injections is not only a source of distress for children, but also for their parents and the individuals administering the injections. 4 This pain can lead to preprocedural anxiety in the future, needle phobias and healthcare avoidance behaviours. 5 It is estimated that up to 25% of adults have a fear of needles, with most fears developing in childhood. 6 Conversely, more positive experiences during vaccine injections would promote and maintain trust in healthcare providers. 5
Eutectic mixture of local anaesthetics (EMLA®) cream is a topical anaesthetic mixture of lidocaine (2.5%) and prilocaine (2.5%) in a cream base. 7 Eutectic mixtures are combinations of two or more substances that solidify at a lower temperature than their individual ingredients. Given its safety profile and proven efficacy, the application of EMLA® cream before vaccination of children to reduce pain at the time of injection is recommended by the Canadian guidelines for reducing the pain of childhood vaccination (grade A recommendation, based on level I evidence). 8 However, many paediatricians and healthcare providers report that one of the major barriers against the routine implementation of such pain-relieving interventions is insufficient time to incorporate them within the busy office workflow, because of the delayed onset of the anaesthetic effect (60 min).3,9 The aim of the present study was to evaluate the effectiveness of implementing EMLA® cream application as a routine pain-relieving strategy during childhood vaccination appointments.
Patients and methods
Study design and patient population
The present study was a prospective, randomized, double-blind, placebo-controlled analysis conducted at the Well-baby Paediatric Clinic, King Khalid University Hospital, King Saud University, Riyadh, Saudi Arabia over a 1-week period during January 2012. All study participants were healthy children, aged 2 months to 6 years, who presented for routine immunization. The exclusion criteria were as follows: a history of allergy to local anaesthetics or to any component of the EMLA® cream; a history of uncertain drug sensitivities; active dermatitis or an open wound at the application site; receipt of an analgesic, anaesthetic or sedative <12 h before the time of vaccination; congenital or idiopathic methaemoglobinaemia; glucose-6-phosphate dehydrogenase deficiency; severe hepatic or renal disease; cardiac disease; use of class I antiarrhythmic drugs.
The study protocol was approved by the Ethical Review Board of the College of Medicine, King Saud University, Riyadh, Saudi Arabia. The parents/legal guardians of the children provided written informed consent for their participation in the study.
Study protocol
Based on a computer-generated schedule, children were randomized at study entry to receive either ∼0.5 g EMLA® (AstraZeneca, London, UK) or placebo cream (an inert cream that could not be visually differentiated from EMLA®; Bepanthen® Cream, Bayer HealthCare, Leverkusen, Germany) applied to an area of approximately 1 cm2 of each vaccination site (the lateral region of the right or left thigh for infants aged <1 year; the right or left deltoid for children aged ≥1 year) before vaccination. Note that no intervention was performed with regard to the time of application prior to vaccination. A nontoxic marker was used to outline the area(s) of application. The applied cream was covered with an occlusive dressing and the time of application was recorded. The child was subsequently enrolled in the normal routine process of paediatrician interview in the examination room followed by vaccination. In the vaccination room, the cream was wiped off and the areas were disinfected with alcohol. The time of vaccine administration was recorded and vaccine injections were administered as per the routine protocol, according to the National Immunization Programme of Saudi Arabia. 10 The time of application of the cream prior to vaccination was calculated from the moment of cream application until the child received the first vaccine injection. The total vaccination appointment time was calculated from when the child arrived in the Well-baby Paediatric Clinic until the child received the first vaccine injection.
Pain assessments
In the vaccination room, pain was assessed by scoring facial expression, cry and body movements of the children using the Modified Behavioural Pain Scale (MBPS).11,12 Two trained observers, who were blinded to the study treatment, together assessed the vaccine injection-related pain in real time. They first established a baseline MBPS score for the 10 s period that preceded the injection, and rated another MBPS score within 10 s after the injection. For each child, differences between the MBPS scores after the injection and the score at baseline were calculated. Whether a cry occurred was noted and total crying time was measured. Infant pain during the vaccination was also assessed by the nurse administering the vaccine at two stages: at the moment of the needle prick, and after finishing the injection and removing the needle. The nurse assessed the pain using a 10-point visual analogue scale (VAS), in which 0 was designated ‘no pain’ and 10 ‘worst possible pain’. Pain was considered to be severe at scores ≥7. The reliability and validity of the VAS and MBPS in evaluating pain associated with vaccinations have previously been confirmed.12,13 Adverse events were evaluated for all children. These included local skin reactions, such as blanching and local erythema, which were assessed at the time of dressing removal and 15 min later.
Statistical analyses
All statistical analyses were performed using the SPSS® statistical package, version 19.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Data are expressed as mean ± SD, n of patients (%) or median (interquartile range). Student’s t-test was used to compare continuous data, Mann–Whitney U-test was used to compare pain scores (ordinal data), and χ2-test was used to compare categorical data. A P-value <0.05 was considered statistically significant.
Results
Over a 1-week period during January 2012, 239 children were seen at the Well-baby Paediatric Clinic, King Khalid University Hospital, for vaccination. The parents of 216 children (90.4%) agreed to participate in the study; the other 23 children were not enrolled in the study due to either lack of parental consent (n = 17) or because the injections were scheduled late after the paediatrician interview (n = 6).
Baseline characteristics of children who participated in a prospective, randomized, double-blind, placebo-controlled analysis of the effectiveness of implementing eutectic mixture of local anaesthetics (EMLA®) cream application as a routine pain-relieving strategy prior to injected vaccination appointments (n = 216).

Data presented as mean ± SD or n of patients (%).
DTP, diphtheria–tetanus–pertussis; HAV, hepatitis A virus; IPV, inactivated polio vaccine; MCV, meningococcal conjugated vaccine; MMR, measles–mumps–rubella; PCV13, pneumococcal 13-valent conjugated vaccine; HBV, hepatitis B virus; Hib, Haemophilus influenzae type B; MBPS, Modified Behavioural Pain Scale.
No statistically significant between-group differences (P ≥ 0.05); Student’s t-test was used to compare continuous data, Mann–Whitney U-test was used to compare pain scores and χ2-test was used to compare categorical data
Significantly fewer infants and children cried after the vaccination in the EMLA® group than in the placebo group: 22.4% of children (n = 24) in the EMLA® group did not cry at all compared with 7.3% (n = 8) in the placebo group (P = 0.002). Total crying time after the injection was significantly shorter in the EMLA® group compared with the placebo group (24.8 ± 20.6 s versus 43.3 ± 20.5 s, respectively; P < 0.001). Eight children (7.5%) in the EMLA® group cried severely to the extent of breath-holding, compared with 24 children (22.0%) in the placebo group (P = 0.003).
Visual analogue scale (VAS) and Modified Behavioural Pain Scale (MBPS) scores before and after injected vaccinations in children who received either eutectic mixture of local anaesthetics (EMLA®) cream or placebo cream application prior to routine vaccination (n = 216).
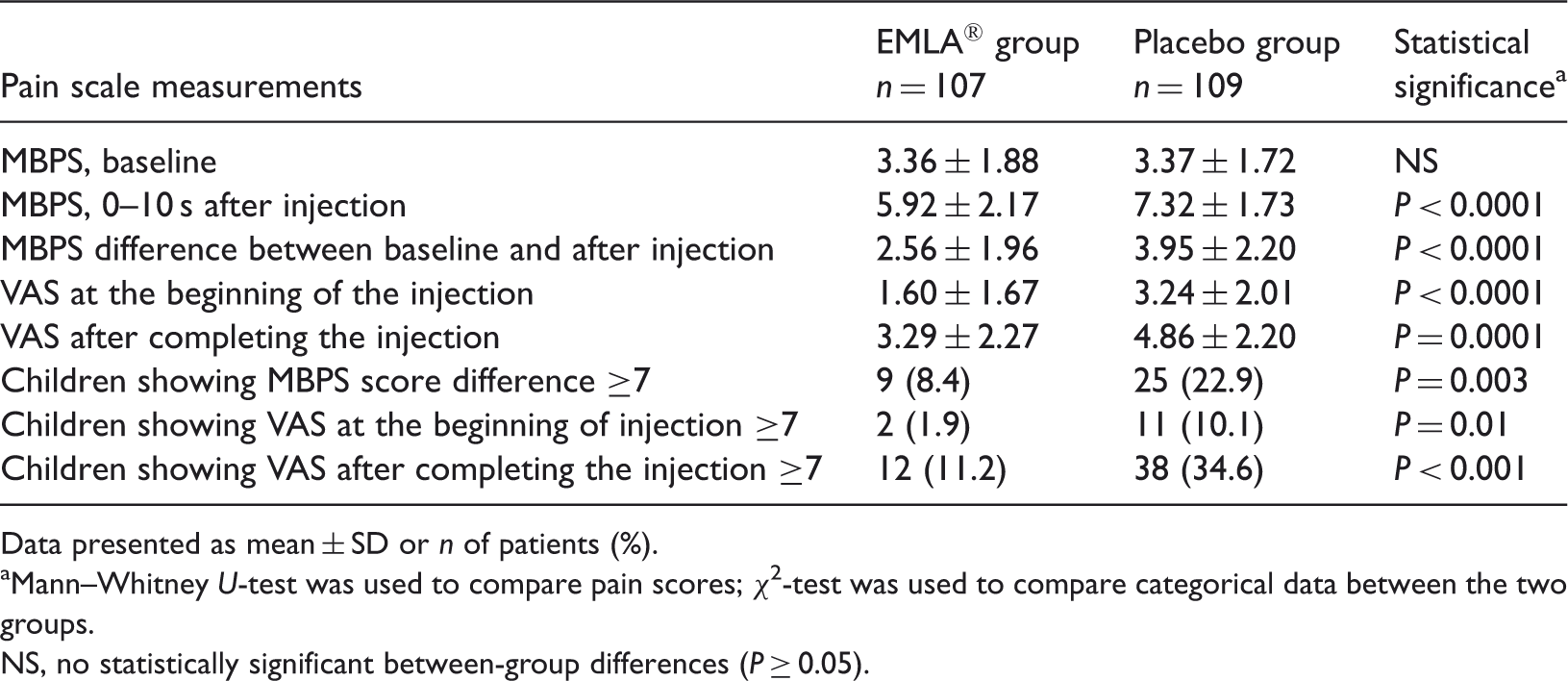
Data presented as mean ± SD or n of patients (%).
Mann–Whitney U-test was used to compare pain scores; χ2-test was used to compare categorical data between the two groups.
NS, no statistically significant between-group differences (P ≥ 0.05).
The median MBPS difference and the interquartile range, as well as the minimum and maximum values for each vaccine type compared with the overall are presented in Figure 1. The pain-relieving effect of the EMLA® cream appeared least evident with pneumococcal 13-valent conjugated vaccine compared with other vaccines.
Modified Behavioural Pain Scale score differences for each injected vaccine type compared with overall scores in children who received either eutectic mixture of local anaesthetics (EMLA®) cream (A) or placebo cream (B), applied prior to routine vaccination (n = 216). Central black horizontal lines represent the medians; extremities of the boxes show upper and lower quartiles of data; error bars represent minimum and maximum values. HAV, hepatitis A virus; IPV, inactivated polio vaccine; MCV, meningococcal conjugated vaccine; MMR, measles–mumps–rubella; PCV13, pneumococcal 13-valent conjugated vaccine; Penta, pentavalent diphtheria–tetanus–pertussis–hepatitis B virus-Haemophilus influenzae type B; Tetra, tetravalent diphtheria–tetanus–pertussis–Haemophilus influenzae type B. The colour version of this figure is available at: http://imr.sagepub.com.
The mean ± SD application time was 56.52 ± 17.14 min for the EMLA® group (range 19 –103 min) versus 57.64 ± 16.15 min (range 32–97 min) for the placebo group (Table 1). Whereas the mean ± SD for the total vaccination appointment time (measured from when the child arrived in the Well-baby Paediatric Clinic until they received their first vaccine injection) was 57.08 ± 16.65 min for the total study population.
The only observed adverse event was pallor at the site of cream application, which was seen significantly more frequently in the EMLA® group compared with the placebo group (31/107 [29.0%] versus 5/109 [4.6%], respectively; P < 0.001); this resolved spontaneously. Neither erythema nor swelling was observed in either group.
Discussion
The present study provided evidence that the use of EMLA® cream for routine childhood vaccinations was as effective as previously reported in reducing the pain associated with either subcutaneous or intramuscular immunization.14–17 The possible effect of EMLA® on the immune response to live vaccine has been assessed previously and there was no evidence of interference from EMLA® with vaccine immunogenicity.15,16 In the current study, a significant reduction in VAS and MBPS scores was observed in the EMLA® group compared with the placebo group. Both the MBPS score recorded by the observer and the VAS score recorded by the nurse administering the vaccines correlated well to support the effectiveness of EMLA® in pain relief.
The efficacy of EMLA® in reducing overall injection pain is likely attributable to a decrease in pain as the needle penetrates the skin, as well as a reduction in the underlying muscle spasm that is associated with such pain.4,18 The pain-relieving effect of EMLA® was more pronounced at the time of the needle prick compared with after the needle was removed, as indicated by the VAS score, possibly due to the limited depth of penetration of EMLA® cream (or other factors related to vaccine composition). The effect of EMLA® on pain associated with the procedures was proven by the measured pain scores and the duration of crying. Only local pallor at the site of cream application was observed in just under one-third of participants in the EMLA® group.
In this present study, the mean ± SD total vaccination appointment time from when the child arrived in the Well-baby Paediatric Clinic until they received their first vaccine injection was 57.08 ± 16.65 min for the total study population, which was an adequate application time for EMLA®. Although the delayed onset of action of EMLA® cream was cited by healthcare providers as one of the major barriers against the routine use of this pain-relieving strategy for immunization in the office setting,3,9,19 the development of a protocol for cream application by the nurses on the child’s arrival helped to overcome this obstacle. In addition, the mean total vaccination appointment time after administering the EMLA® cream did not differ markedly from the mean ± SD waiting time at the King Khalid University Hospital, which was previously found to be 47.34 ± 20.47 min based on performance monitoring (personal communication). It is expected that as vaccination nurses become more familiar with the EMLA® application procedures, the time to first vaccination will decrease further toward the hospital’s baseline measurement time of 47.34 ± 20.47 min.
Taddio et al. 20 reported a comparable mean ± SD waiting time of 41.6 ± 28.7 min for childhood vaccination appointments in eight outpatient primary care clinics. This waiting time included the general waiting room time plus examination room time before the actual vaccine injection, without implementing any extra pain-relieving strategy. Therefore, whenever the typical wait time for a vaccine appointment exceeds 30 min, application of local anaesthetic could be incorporated within the process of vaccine injection without substantially prolonging the duration of the visit.
Studies have focused on evaluating pain associated with specific vaccine types in a particular age group.14–16 In contrast, the present study included all eligible children who presented to the Well-baby Paediatric Clinic for routine immunization. Furthermore, the pain associated with all vaccine injections given to the children was assessed. Thus, this may increase the generalizability of the present study for implementing EMLA® cream application as a routine pain-relieving strategy in clinical vaccination practice. However, because the present study was conducted in a relatively small number of children from a single centre, these findings may warrant further research in this regard.
The present study showed that infants and children receiving pre-treatment with EMLA® cream before their routine vaccinations manifested significantly lower pain scores compared with the placebo group, with little increase in the mean time between child arrival at the clinic and first vaccine injection. Therefore, we suggest that EMLA® cream be used routinely before vaccination, exploiting the significant advantages of alleviating the child’s pain and their parents’ anxiety levels.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
The authors are thankful to the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia for supporting the work through a Research Group Project Grant (RGP-VPP 181).
Acknowledgements
The authors are thankful to the Deanship of Scientific Research, King Saud University, Riyadh, Saudi Arabia for supporting the work. We also extend our thanks to the nursing staff at the Well-baby Paediatric Clinic, King Khalid University Hospital, King Saud University, Riyadh, Saudi Arabia.