
Abstract
Objective
This study aimed to distinguish chest pain characteristics between patients with and without acute coronary syndrome (ACS) at Vietnam National Heart Institute.
Methods
A case-control study using a structured chest pain assessment questionnaire was performed to examine pain characteristics.
Results
Smoking, a history of heart attack, and a family history of cardiovascular disease were associated with increased ACS-related chest pain risk. Patients without ACS more frequently reported left or central chest pain, mild discomfort, pain triggered by activity, and relief with rest or nitroglycerin. ACS-related chest pain was more often characterized by pain radiating to the back, a sensation of tightness or severe discomfort, gradual intensity increase, occurrence at rest or with minimal exertion, and accompanying sweating. No significant sex differences were found in ACS-related chest pain symptoms.
Conclusions
Targeted assessment of chest pain features—such as pain radiation, pressure sensation, symptom escalation, duration, activity triggers, and relief factors—could improve public awareness and support the development of educational resources on ACS and non-ACS symptoms.
Keywords
Introduction
Chest pain is a leading reason for emergency department visits in the United States, accounting for more than 8 million visits. 1 Similarly, the Vietnam International Heart Institute has reported a significant increase in chest pain admissions. 2 However, only 5.1% of these patients are ultimately diagnosed with acute coronary syndrome (ACS). 3
For patients with ST-elevation myocardial infarction (STEMI), the best outcomes are achieved when diagnosis occurs within 10 minutes of first medical contact at a reperfusion-equipped hospital. 4 Pharmacological interventions, such as fibrinolytics, are most effective when administered within 30 minutes to 1 hour after symptom onset, while percutaneous coronary intervention achieves optimal results within 2 hours. In many low- to middle-income countries, however, treatment delays frequently exceed these timeframes.4,5 At the Vietnam National Heart Institute, patients experience an average pre-hospital delay of 4.8 hours, with over half of patients facing a delay of 6 hours or more. 6
Underdiagnosis, especially of STEMI, has serious consequences, with delayed treatment significantly reducing long-term survival rates (73% vs. 93% with early intervention). 7 The COVID-19 pandemic further highlighted this issue, as global delays in STEMI treatment lowered rates of primary percutaneous coronary interventions and increased mortality, along with complications such as re-infarction.8,9 Similarly, patients admitted during off-hours often face delays in percutaneous coronary intervention, leading to higher in-hospital mortality rates.10,11 Addressing these delays and ensuring timely treatment is essential to improve patient outcomes.
Pre-hospital delays in ACS can stem from factors related to patients, clinicians, and emergency medical transport. 12 For patients, downplaying cardiac risk and misinterpreting symptoms are key reasons for delaying timely care. 13 In clinical settings, evaluating chest pain in suspected ACS typically involves biochemical markers, electrocardiography, and imaging modalities.14–16 Furthermore, in Vietnam, the high prevalence of non-ACS chest pain causes, such as gastrointestinal disorders 17 and coronary microvascular dysfunction, adds complexity to the diagnosis, particularly given limited access to cardiac biomarkers, specialized equipment, and reliable transportation in district and commune hospitals. 18 In such settings, physicians must balance accurate cardiac assessment with the need for further testing while avoiding resource overuse and misdiagnosis. These challenges underscore the need for improved diagnostic tools and evidence-based guidelines for efficient chest pain assessment in Vietnam.
This research aims to raise awareness about non-ACS chest pain symptoms and highlight the need for prompt attention to ACS risks, especially in remote areas. Despite the variability in chest pain presentations, we seek to identify subtle differences between ACS and non-ACS causes. By sharing this knowledge, we aim to provide patients and healthcare professionals with a clearer understanding, ultimately improving ACS diagnosis and management in Vietnam. Additionally, sex-specific educational materials and clinical guidelines are essential because numerous studies have indicated significant differences in chest pain symptoms between men and women.14,19–23
The objective of this study was to evaluate variations in chest pain characteristics among individuals diagnosed with ACS and non-ACS at the Vietnam National Heart Institute – Bach Mai Hospital. The study also involved an investigation of the differences in ACS-related chest pain between male and female patients.
Methods
Study design and setting
This observational case-control study was conducted at the Vietnam National Heart Institute and followed the EQUATOR guidelines. The study reporting adheres to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. 24 A paper-based chest pain assessment questionnaire, developed according to the 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline and the NICE Guideline, was used to evaluate chest pain characteristics.25,26 The questionnaire provides a comprehensive assessment, covering all aspects of chest pain, including its nature, onset and duration, location and radiation, precipitating factors, relieving factors, and associated symptoms.
Sample size and sampling procedure
In total, 270 patients with a primary complaint of chest pain were consecutively selected between August and September 2023. For this unmatched case-control study, the sample size was calculated based on a case:control ratio of 1:4, with a power of 80% (Z = 0.80) and a significance level of 5% (Z = 1.96). The control group proportion of 19.4% exposed was referenced from research on Temporal Trends of the Prevalence of Angina With No Obstructive Coronary Artery Disease (ANOCA).
27
To estimate the proportion of cases exposed, we use the following calculations: Pcases exposed = OR ×Pcontrols exposed; Pcontrols exposed = Pcases exposed ×2 = 0.194 × 4.0 = 0.776; and average proportion exposed = [(0.32 + 0.18)/2] = 0.485. The elements were applied in the following formula:

The inclusion criteria for this study were patients who presented with chest pain, underwent invasive coronary angiography, and were diagnosed with ACS (STEMI, non-STEMI, or unstable angina) by cardiologists. Diagnosis was based on coronary artery images showing vulnerable plaque or vessel occlusion during angiography, along with other diagnostic tools such as 12-lead electrocardiography and initial biomarker tests. The cases comprised patients who presented with chest pain, underwent invasive coronary angiography, and were classified as non-ACS by interventional cardiologists. This classification was based on the absence of detectable coronary artery damage in imaging and findings from other diagnostic tools, including 12-lead electrocardiography and initial biomarker tests. The exclusion criteria were hemodynamic instability, ventilator dependence, and refusal to participate. The study used a total sampling technique, including all eligible patients who met the inclusion criteria. Trained nursing students conducted patient interviews 24 hours after coronary angiography in the Emergency Department of the Vietnam National Heart Institute. Based on these criteria, a sample size of 270 patients was obtained. The clinical workflow for this study is shown in Figure 1.
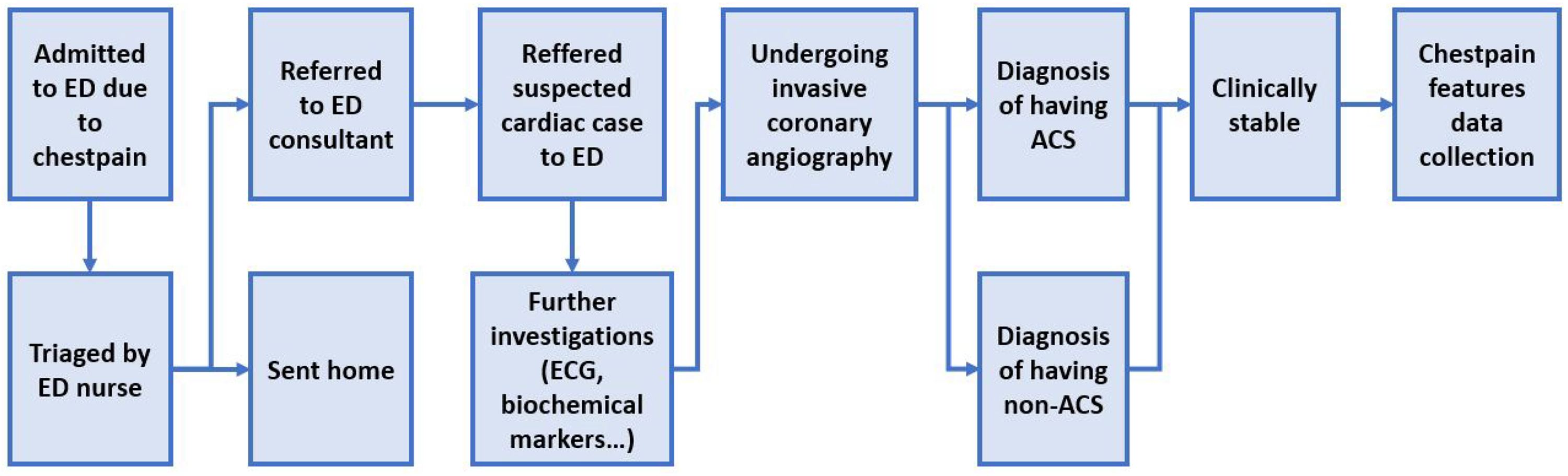
Clinical workflow of patients.
Patient consent and ethical approval
The study’s aims were explained to the participants, who provided written informed consent. All responses were processed anonymously, ensuring that data could not be linked to individual participants, in compliance with national personal data protection laws. The study was approved and accepted by the IRB Board of Vietnam National Heart Institute.
Data processing and analysis
Data analysis was performed using the IBM Statistical Package for Social Sciences (IBM SPSS) version 25.0 for Windows (IBM Corp., Armonk, NY, USA). Odds ratios (ORs) for chest pain characteristics were calculated using the crosstabs method. Additionally, multivariate logistic regression analysis with a significance level (alpha) of 0.05 was used to identify ORs for each question and develop the optimal model for chest pain assessment. Differences in chest pain characteristics between male and female patients with ACS were analyzed using the chi-square test.
Results
Baseline characteristics
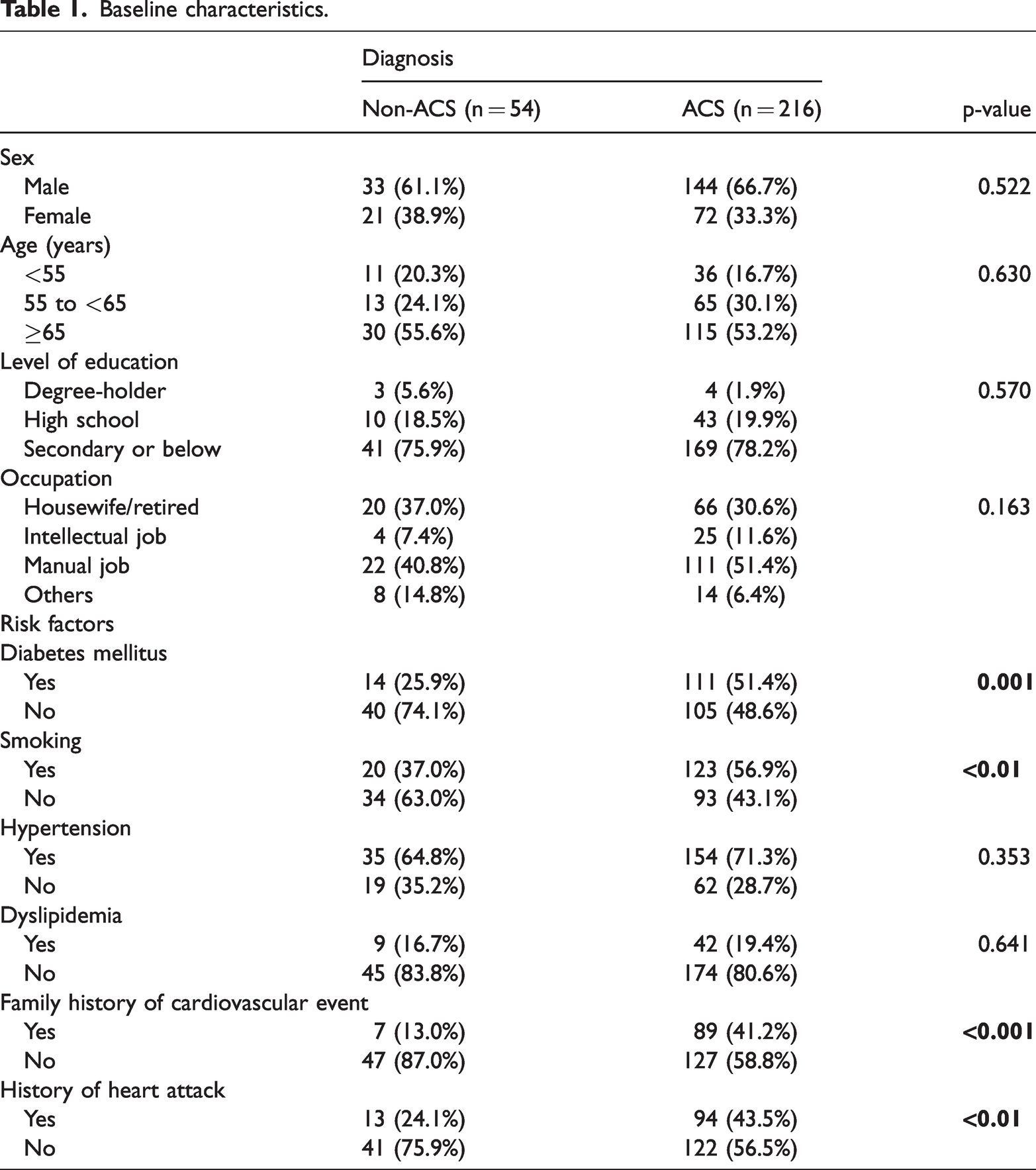
This study involved 270 patients (54 without ACS and 216 with ACS), with baseline characteristics detailed in Table 1, including demographic and clinical data. No significant differences were found in age, sex, education, or occupation. Chest pain in non-ACS and ACS patients showed no statistically significant differences in hypertension or dyslipidemia. However, the non-ACS group had significantly fewer classic ACS risk factors, such as type 2 diabetes, a family history of cardiovascular events, and a personal cardiovascular history (p < 0.05).
Baseline characteristics.
Chest pain characteristics of patients with non-ACS and ACS
Table 2 presents the chest pain characteristics of patients with and without ACS. Notably, patients without ACS showed distinct features, including left or middle chest pain, sensations of pain and discomfort, mild pain intensity, pain triggered by physical activity, and pain that subsided with rest or nitroglycerin. By contrast, patients with ACS reported pain radiating to the back, sensations of heaviness or tightness, squeezing sensations, severe pain intensity, pain that gradually intensified and persisted, and pain occurring at rest, often accompanied by diaphoresis.
Chest pain characteristics of patients with non-ACS and ACS.

Table 2 also shows the ORs for each question in the chest pain assessment questionnaire. The results indicated significant associations between specific chest pain characteristics and the likelihood of non-ACS and ACS-related pain. For example, left or middle chest pain (OR = 3.450, 95% confidence interval (CI) = 1.551–7.676, p = 0.002) and back-radiating pain (OR = 0.221, 95% CI = 0.051–0.954, p = 0.043), as well as sensations of pain and discomfort (OR = 4.458, 95% CI = 2.224–8.937, p < 0.001) and heaviness or tightness (OR = 0.232, 95% CI = 0.088–0.608, p = 0.003), were strongly linked to non-ACS and ACS chest pain, respectively.
Other noteworthy findings included associations between chest pain severity, duration, and specific triggers. Specifically, mild pain (OR = 3.430, 95% CI = 1.599–7.356, p = 0.002) and severe pain (OR = 0.234, 95% CI = 0.081–0.678, p = 0.007) showed significant ORs, as did symptoms that gradually built in intensity (OR = 0.317, 95% CI = 0.171–0.588, p < 0.001), pain lasting more than 20 minutes (OR = 0.268, 95% CI = 0.136–0.529,p < 0.001), and pain triggered by physical exercise (OR = 2.288, 95% CI = 1.212–4.320, p = 0.011). Furthermore, chest pain occurring at rest or with minimal exertion (OR = 0.358, 95% CI = 0.194–0.662, p = 0.001) and pain that subsided with rest or nitroglycerin (OR = 2.583, 95% CI = 1.301–5.131, p = 0.007) were also statistically significant. Chest pain accompanied by diaphoresis (OR = 0.364, 95% CI = 0.174–0.763, p = 0.007) showed a significant OR, indicating a notable relationship between these symptoms.
Multivariate analysis of chest pain assessment
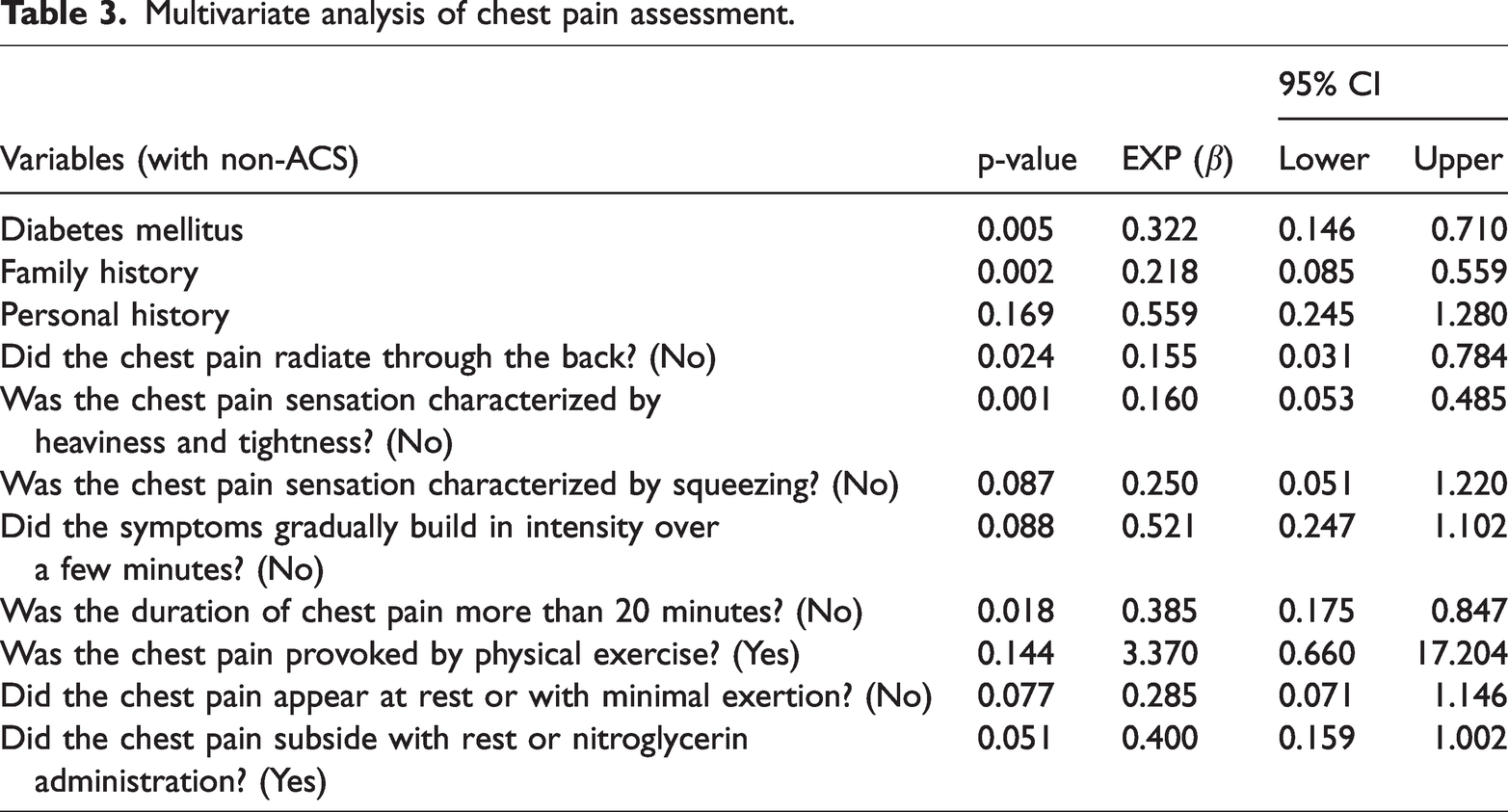
Multivariate logistic regression was used to develop a model for focused questions in chest pain assessment, including only questions with p-values of <0.05 in the analysis. The focused questions for ACS prediction after multivariate logistic regression analysis are shown in Table 3. The model was adjusted for type 2 diabetes mellitus, family history, and personal history risk factors. The focused questions in this model were as follows: Did the chest pain radiate to the back? (No), Was the chest pain sensation characterized by heaviness and tightness? (No), Was the chest pain sensation characterized by squeezing? (No), Did the symptoms gradually build in intensity over a few minutes? (No), Was the duration of chest pain more than 20 minutes? (No), Was the chest pain provoked by physical exercise? (Yes), Did the chest pain occur at rest or with minimal exertion? (Yes), and Did the chest pain subside with rest or nitroglycerin? (Yes). This model achieved a Nagelkerke R-square of 0.422, a Hosmer and Lemeshow test statistic of 0.624, and an Omnibus test statistic of 0.000.
Multivariate analysis of chest pain assessment.
Differences in ACS-related chest pain characteristics between sexes
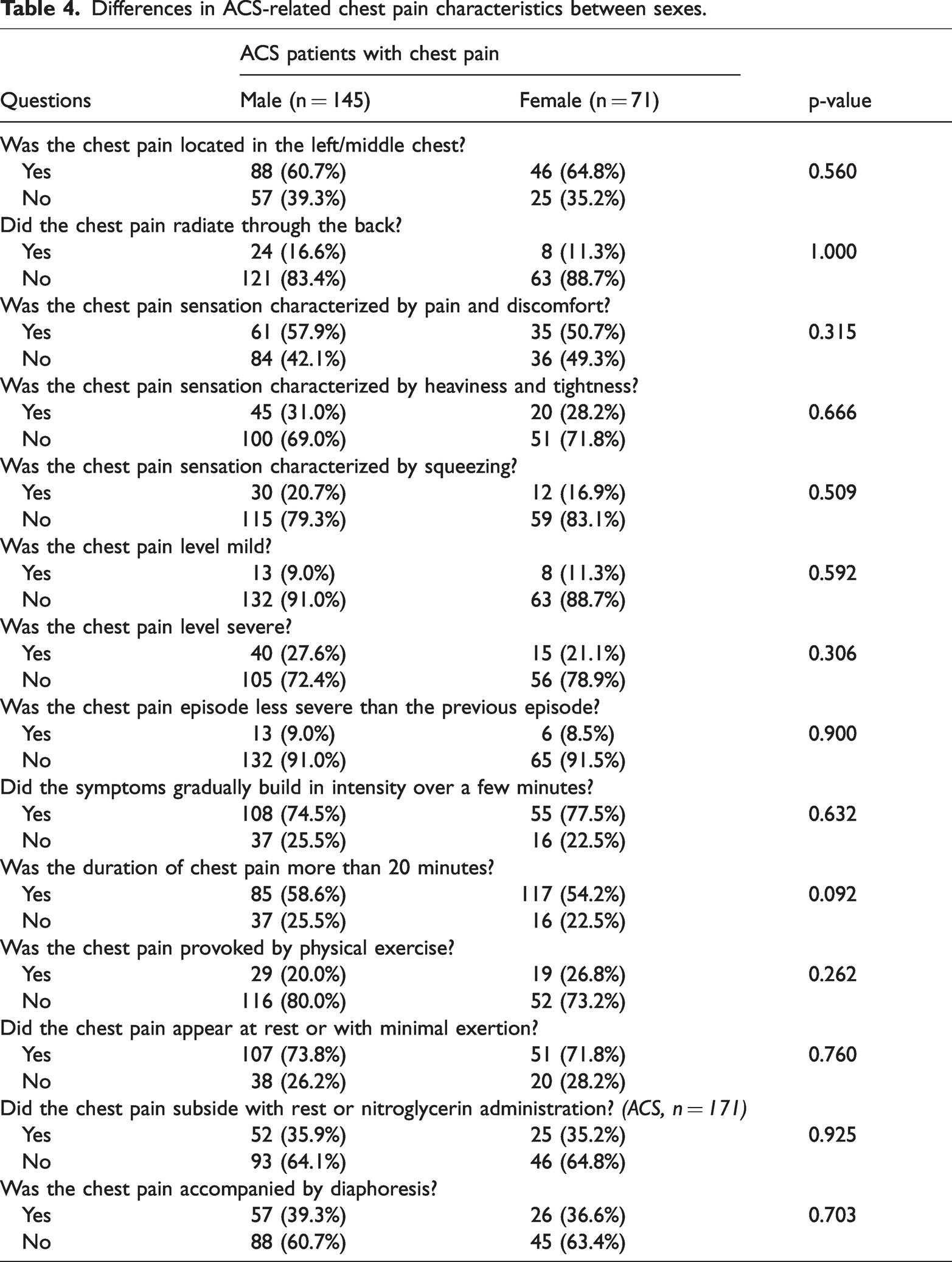
Table 4 presents data on sex-related differences in ACS-related chest pain characteristics. No significant differences were observed between the sexes.
Differences in ACS-related chest pain characteristics between sexes.
Discussion
Patients who smoke, have a history of heart attack, or have a family history of cardiovascular events are at higher risk of experiencing ACS-related chest pain. By contrast, patients without ACS often experience left-sided or mid-chest pain of mild intensity, typically triggered by physical activity and relieved by rest or nitroglycerin. Patients with ACS, however, commonly report chest pain radiating to the back, with sensations of tightness and severe intensity, gradual escalation, and pain at rest or with minimal exertion, often accompanied by diaphoresis.
The adjusted chest pain assessment model in this study included the following questions: Did the chest pain radiate to the back? Was the chest pain sensation characterized by heaviness and tightness? Was the chest pain sensation characterized by squeezing? Did the symptoms gradually build in intensity over a few minutes? Was the duration of chest pain more than 20 minutes? Was the chest pain triggered by physical exercise? Did the chest pain occur at rest or with minimal exertion? Did the chest pain subside with rest or nitroglycerin? This model had a Nagelkerke R-square of 0.422, indicating that it explained 42.2% of non-ACS detection.
Our study showed no significant differences in the ACS-related chest pain location, severity, or duration between the two sexes. Additionally, diabetes mellitus, smoking, and personal or family history of coronary artery disease were associated with an increased risk of ACS-related chest pain, consistent with previous findings.28,29 Due to multiple pathophysiological disturbances, patients with diabetes are predisposed to a proinflammatory, prothrombotic state, which may lead to plaque rupture. 30 Smoking is another established risk factor for ACS because it can elevate levels of matrix metalloproteinases, contributing to unstable coronary artery plaque formation. 30 A family history of coronary artery disease is also an independent risk factor, suggesting a genetic predisposition. 29
In contrast to the findings of Lukitasari et al., 13 our study showed that chest pain located in the left or middle chest was associated with non-ACS chest pain. This discrepancy may be due to differences in participant selection because our study was conducted at a heart institute, while Lukitasari et al.’s 13 study was conducted in an emergency department. This setting difference suggests that our participants had already undergone some level of screening for heart conditions, whereas Lukitasari et al.’s 13 participants likely had a broader range of medical conditions. However, Bösner et al. 31 reported that ACS and non-ACS patients showed similar pain locations. Further research is needed to clarify the relationship between chest pain location and ACS.
Our findings also suggest that pain radiating to the back may indicate ACS, with an OR of 0.221 (95% CI = 0.051–0.954). This observation aligns with the study by Lukitasari et al., 13 where back-radiating chest pain was similarly associated with ACS. However, Malik et al. 16 reported that the most common site for acute myocardial infarction (AMI) pain radiation is the left shoulder and arm.
In terms of chest pain quality, our study showed that patients with non-ACS chest pain were more likely to report mild pain and discomfort, while those with ACS chest pain were more likely to report severe, squeezing pain or sensations of heaviness and tightness. This aligns with the findings of Eslick et al., 32 who reported that patients with cardiac chest pain were twice as likely to report severe to very severe pain than moderate pain, whereas patients with noncardiac chest pain more often reported moderate pain.
Malik et al. 16 suggested that a chest pain duration of more than 20 minutes could serve as a cut-off for AMI, as 90% of patients with AMI reported chest pain lasting more than 20 minutes. Our study found similar results, with a chest pain duration of more than 20 minutes indicating ACS (OR = 0.268, 95% CI = 0.136–0.529). The multivariate analysis also highlighted chest pain duration as an important factor in distinguishing between ACS and non-ACS chest pain.
Our findings indicate that non-ACS chest pain is typically triggered by physical exertion, while ACS chest pain may occur at rest or with minimal exertion. This may be explained by the fact that many patients with non-ACS chest pain experience stable angina, which is often triggered by exercise.13,33,34 Meanwhile, the relationship between exercise and AMI is less clear.
Our study’s statistics revealed no significant differences in the clinical symptoms of ACS-related chest pain between women and men presenting at the Vietnam Heart Institute. To our knowledge, quantifying diagnostic accuracy based on clinical symptoms in ACS-related chest pain, with a direct sex comparison, has not been previously documented. Our findings align with three other studies that examined chest pain characteristics in ACS patients visiting the emergency room.22,35,36 Notably, one of these studies also conducted a multivariable analysis, which showed that only a minority of clinical symptoms retained significance in the model for both sexes.
Prompt recognition and diagnosis of ACS remain challenging in both clinical and community settings. Patients’ delays in seeking prehospital care may stem from unfamiliarity with ACS symptoms, difficulty interpreting them, or confusion between ACS signs and those associated with respiratory or gastrointestinal issues. 37 This study could contribute to the foundational development of a mobile application specifically designed for patients with chest pain. Such an evidence-based tool would enable individuals to assess their symptoms accurately, differentiate between ACS and non-ACS causes, and make informed decisions regarding the need for urgent care. Furthermore, this research can support the creation of culturally and linguistically appropriate health materials and educational sessions tailored for the Vietnamese, especially in remote areas. These targeted interventions aim to raise public awareness of the diverse and often subtle presentations of ACS, as well as its risk factors, thereby reducing misunderstandings and promoting timely healthcare-seeking behavior.
Limitations
Despite the promising implications of this study for reducing pre-hospital delay time, several limitations warrant consideration. First, data were collected exclusively from a single hospital, the Vietnam National Heart Institute in Hanoi, with a relatively small sample size. This may limit the generalizability of our findings to the broader population. Second, the sample was derived from individuals who had undergone initial screening at the Emergency Department of Bachmai Hospital and had been diagnosed with potential cardiac problems before transfer to the Vietnam National Heart Institute. This process reduced the number of non-ACS chest pain cases and limited the variability in chest pain characteristics. Third, the retrospective design introduces the possibility of subjective and inaccurate information. Finally, the questionnaire’s low Nagelkerke R-square of 0.422 suggests limited ability to classify between non-ACS and ACS-related chest pain. We recommend conducting a larger study across emergency departments in central hospitals nationwide to improve the classification of chest pain symptoms.
Conclusion
Considerable overlap exists between non-ACS and ACS-related chest pain. Our study suggests that a set of questions—including Did the chest pain radiate to the back?, Was the sensation characterized by heaviness and tightness?, Was the sensation characterized by squeezing?, Did symptoms gradually build in intensity?, Did the pain last more than 20 minutes?, Was it triggered by physical exercise?, Did it occur at rest or with minimal exertion?, and Did it subside with rest or nitroglycerin?—may help distinguish non-ACS-related chest pain with moderate predictive value. No significant differences were found between the two sexes in ACS-related chest pain symptoms. This research supports the development of digital applications and educational programs for the prevention and management of cardiovascular disease.
Supplemental Material
sj-pdf-1-imr-10.1177_03000605241300009 - Supplemental material for Characterizing chest pain in patients with acute coronary syndrome at Vietnam National Heart Institute: a case-control study
Supplemental material, sj-pdf-1-imr-10.1177_03000605241300009 for Characterizing chest pain in patients with acute coronary syndrome at Vietnam National Heart Institute: a case-control study by Lan Anh Nguyen, Nhat Minh Pham, Manh Hung Pham, Hong Nhung Nguyen Thi, Hoai Nguyen Thi and Tuan Nguyen Huu in Journal of International Medical Research
Supplemental Material
sj-pdf-2-imr-10.1177_03000605241300009 - Supplemental material for Characterizing chest pain in patients with acute coronary syndrome at Vietnam National Heart Institute: a case-control study
Supplemental material, sj-pdf-2-imr-10.1177_03000605241300009 for Characterizing chest pain in patients with acute coronary syndrome at Vietnam National Heart Institute: a case-control study by Lan Anh Nguyen, Nhat Minh Pham, Manh Hung Pham, Hong Nhung Nguyen Thi, Hoai Nguyen Thi and Tuan Nguyen Huu in Journal of International Medical Research
Footnotes
Acknowledgments
The authors greatly appreciate the staff and patients of the Vietnam National Heart Institute for their kind help and support during this study.
Author contributions
N.M.P and L.A.N. conceived and designed the study and had full access to all data. H.N.N.T. and H.N.T. collected the data. L.A.N. and N.M.P. analyzed the data and conducted the statistical analysis. N.M.P. edited, revised, and submitted the manuscript. M.H.P. supervised the project. T.N.H. contributed to the writing, reviewing, and editing of the manuscript. All authors contributed to the writing of the original draft.
Data availability
The data used to support the findings of this study are available from the corresponding author upon request.
Declaration of conflicting interest
The authors declare that they have no competing interests.
Funding
This research did not receive any specific grant from any funding agency in the public, commercial, or not-for-profit sector.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.