
Abstract
Objective:
The use of transthoracic echocardiography (TTE) to identify right-sided infective endocarditis (RSIE) vegetation is controversial. Data are scarce for patients with no history of intravenous drug abuse (IVDA) or cardiac device insertion. This study analysed the consistency of presurgical echocardiographic results with surgical findings for vegetation identification, and the factors that influence accuracy of echocardiography.
Methods:
This retrospective trial divided infective endocarditis (IE) patients into three subgroups according to the results of their presurgical TTE: left-sided native IE (LSNIE), left-sided prosthetic valve IE (LSPIE) and RSIE. The accuracy of TTE was tested by comparing vegetation (number and location), detected presurgery by TTE, with actual findings during surgery.
Results:
In total, 416 patients were analysed, 322 with LSNIE, 31 with LSPIE and 63 with RSIE. Consistency between TTE findings and surgical results was lower in the RSIE group compared with the LSPIE and LSNIE groups. Consistency was lowered by the presence of vegetation in multiple locations and atypical distribution – both of which were increased in the RSIE group. The chance of vegetation in both sides of the heart rose with increased numbers of vegetation locations in RSIE patients. A high proportion of RSIE patients had congenital heart defects, mostly ventricular septal defects.
Conclusions:
TTE may be unsuitable for RSIE patients with no history of IVDA or cardiac device insertion, because multifocal and atypically distributed vegetation may influence detection accuracy.
Keywords
Introduction
Infective endocarditis (IE) is a life-threatening disease associated with a high mortality rate.1–3 Anatomically, IE is characterized by a combination of vegetative, destructive lesions and abscess formation. 4 Vegetative lesions are the hallmark lesions of IE, and transthoracic echocardiography (TTE) is the best technique for noninvasive visualization of such lesions, although the results of this technique are not always accurate. 4 The diagnostic value of TTE in detecting vegetation is influenced by factors including image quality, echogenicity, vegetation size, vegetation location, previous valvular disease or valvular prosthesis, experience and skill of the examiner, and pretest probability of endocarditis. 5 Typically, vegetation presents as an oscillating mass attached to a valvular structure, which moves independently to the valve. The sensitivity of TTE may be reduced for very small vegetative lesions and there may be difficulties in identifying vegetation in the presence of pre-existent severe lesions (such as mitral valve prolapse, degenerative lesions and prosthetic valves). 6 The identification of vegetation may also be difficult when the lesions are nonoscillating and/or atypically distributed. 4 Conversely, false diagnosis of IE may occur due to difficulty differentiating between vegetation and thrombi, prolapsed cusps, cardiac tumours, myxomatous changes, Lambl’s excrescences, strands or noninfective vegetations (marantic endocarditis).4,7
Compared with left-sided IE (LSIE), the incidence of right-sided IE (RSIE) is much lower, accounting for 5–10% of cases of IE.8,9 RSIE is most frequently observed in those with a history of intravenous drug abuse (IVDA).10–12 The value of TTE as a method for discovering vegetation is controversial,8,13–15 although TTE allows satisfactory assessment of large vegetations and of valvular involvement because of the anterior location of the tricuspid valve.8,14 San Roman et al. have shown that even the use of transoesophageal echocardiography (TEE) did not increase the accuracy of TTE for the detection of vegetation in tricuspid endocarditis. 15 However, most of these data were obtained from patients with a history of IVDA or from those who had received cardiac devices, with little data presented for RSIE patients without either of these histories.
The reported incidence of IE in patients with congenital heart disease (CHD) is many times higher than that in the general population,16–18 and is particularly high for RSIE. 17 With economic and technological developments, survival rates have improved in patients with complicated CHD, but this has resulted in the emergence of complex cases of IE. 19
The present study retrospectively analysed patients who received surgery to treat IE (and any concomitant structural abnormality, if present), and compared the consistency of echocardiographic findings with surgical findings of vegetation (and abscesses). This study also compared the consistency rates between LSIE and RSIE patients, and analysed factors that influenced the accuracy of TTE judgements for vegetation in RSIE patients with no history of IVDA or cardiac device insertion. The aims of the study were to provide meaningful information on the diagnosis of RSIE for echocardiographic experts and clinicians, and to promote the accuracy of identification by highlighting important issues that are frequently ignored or misunderstood in clinical work. Such issues are particularly relevant in the treatment of patients with CHD.
Methods
Patients
Sequential patients with IE, admitted to Beijing Anzhen Hospital between January 2002 and May 2012, were enrolled. All patients included in the study underwent surgery for at least one of the following: removing vegetation and/or abscesses; repairing or replacing valves; correcting CHDs. The patients had received TTE on one of the 0–30 days before the operation. For those who underwent more than one operation during the study period, only the results from the first operation were used in the present analyses. Patients who were not treated with surgery, or who were treated with a procedure that did not require the heart to be opened (for example coronary artery bypass graft or pericardial surgery) were not included in the study. Also excluded were those who did not receive TTE in the Anzhen Hospital, or those in whom TTE was not completed 30 days prior to surgery. Patients with RSIE who received a cardiac device during their surgery were also excluded from the study. All patients were interviewed about their medical history and were evaluated carefully on admission and before surgery. The characteristics of all patients conformed to the Duke criteria for IE. 20
This study was approved by the Institutional Review Board of Beijing Anzhen Hospital. All patients (or parents of patients) provided written informed consent for participation in the study.
Ultrasound assessment
The TTE was performed by highly experienced cardiologists to evaluate the presence, location and size of vegetations, to provide systematic evaluation of all the valves in multiple acquisition angles, and to calculate cardiac chamber size and ejection fraction. During TTE, possible vegetations that were hardly differentiated from a pre-existing lesion with thickened or calcified leaflets were regarded as vegetation during analysis. Interval points were calculated as the time between the last echocardiography and the day of surgery, and were then classified into five groups: 1, 0–3 days; 2, 4–6 days; 3, 7–10 days; 4 , 11–20 days; 5, < 20 days. The regurgitation point of affected valves had four degrees of classification: 0, no regurgitation; 1, mild; 2, moderate; 3, severe. If patients had an echocardiographic examination more than once with different results, the final one prior to surgery was used for this study. According to TTE, patients were classified into three subgroups: left-sided native IE (LSNIE); left-sided prosthetic valve IE (LSPIE); RSIE. Patients with concomitant left- and right-sided IE and CHD were regarded as RSIE during statistical analysis.
Transoesophageal echocardiography was performed on patients at the discretion of the treating clinician and when results of the TTE were questionable.
Surgical assessment
Standard blood cultures were taken for every patient. All patients received antibiotics for 4–8 weeks, dosed according to body weight and creatinine clearance values. The following regimens were used: penicillin alone; penicillin in combination with other antibiotics; cephalosporin in combination with other antibiotics; vancomycin in combination with other antibiotics. Antifungals were prescribed for those whose symptoms were suggestive of a fungal infection.
Duration point refers to the time between symptom onset and day of surgery, and was classified into three subgroups for statistical purposes: 1, 1–30 days; 2, 31–60 days; 3, < 60 days. According to surgical findings, lesions on the mitral and aortic valves of the left heart and the tricuspid and pulmonary valves of the right heart were defined as typically distributed anatomical vegetation. Atypical anatomical vegetation included lesions in the ventricle, atrium, aorta, pulmonary artery, ductus arteriosus, etc. If no vegetation was found in the right hearts of LSNIE and LSPIE patients without structural heart disease by ultrasound, patients were not explored surgically and were classified as having negative findings. If vegetation was not found during surgery, the TEE result was considered to be a false positive. Some patients, therefore, failed to meet the major and minor Duke criteria for IE diagnosis, but were still regarded as IE patients for this study because of their clinical characteristics, which included fever and severely damaged valves.
Statistical analyses
Numeric values were reported as mean ± SD; age, left ventricular ejection fraction (LVEF), heart function, regurgitation point and duration point were compared by analysis of variance. Categorical variables were compared with χ2-test. Statistical calculations were performed using SPSS® version 16.0 (SPSS Inc, Chicago, IL, USA) and a P-value < 0.05 was considered statistically significant. A sensitivity analysis of patients with or without CHD was also undertaken.
Results
This study analysed 416 IE patients (290 male; 126 female), age range 1–78 years (median 39.0 years), who conformed to the Duke criteria for IE. 20 Fifteen patients with concomitant left and right IE and CHD were regarded as RSIE during statistical analysis. TEE was performed on 23 (5.5%) patients, and only 163 (39.2%) had a meaningful positive blood-culture report. Penicillin alone was prescribed for 25 (6.0%) patients, penicillin in combination with any other antibiotics for 189 (45.4%), cephalosporin in combination with any other antibiotics for 151 (36.3%) and vancomycin in combination with any other antibiotics for 50 (12.0%); 78 (18.8%) patients received antifungal agents, with some patients receiving antifungal therapy concomitantly with antibiotics.
Vegetation was not found during surgery in 93 patients; the presurgery TTE result was therefore considered a false positive in 66 patients.
Clinical characteristics of 416 patients with infective endocarditis examined for heart vegetation by transthoracic echocardiography prior to surgery, subdivided based on disease location.

Regurgitation point of affected valve: 0, no regurgitation; 1, mild regurgitation; 2, moderate regurgitation; 3, severe regurgitation.
Calculated from the onset of symptoms to the day of surgery: 1, 1–30 days; 2, 31– 60 days; 3, > 60 days.
New York Heart Association (NYHA) degrees I, II, III and IV were converted to 1, 2, 3 and 4. 36
Time between the last echocardiography and subsequent surgery: 1, 0–3 days; 2, 4–6 days; 3, 7–10 days; 4, 11–20 days; 5, < 20 days.
Consistency between echocardiography and subsequent surgical results.
Numerical values were compared using analysis of variance; categorical variables were compared with χ2-test.
LSNIE, left-sided native infective endocarditis; LSPIE, left-sided prosthetic valve infective endocarditis; RSIE, right-sided infective endocarditis; LVEF, left ventricular ejection fraction; NS not significantly different.
Consistency of vegetation identification between transthoracic echocardiography (TTE) and surgical findings in 416 patients with infective endocarditis.

A, true positive; B, false positive; C, false negative; D, true negative.
Sensitivity, A/(A + C); specificity, D/(B + D); π, (A + D)/(A + B + C + D).
LSNIE, left-sided native infective endocarditis; LSPIE, left-sided prosthetic valve infective endocarditis; RSIE, right-sided infective endocarditis.
The consistency of TTE with surgical findings for patients with surgically-confirmed vegetation is shown in Figure 1A. Patients with multifocal vegetation (at least two locations) had significantly lower consistency between TTE results and surgical findings than patients with vegetation in no or one location (P = 0.003; χ2 = 13.7). After removing all patients found during surgery to be free of vegetation (n = 93), patients with surgically-confirmed atypically distributed (multifocal) vegetation (n = 32) had much lower rates of consistency between TTE and surgical findings than those with typically distributed vegetation (n = 291; 37.5% versus 63.0%, P = 0.002) (Figure 1B).
(A) Variation in consistency for vegetation identification between transthoracic echocardiography (TTE) and surgical findings, divided according to the number of locations to which vegetation is attached, in 416 patients with infective endocarditis; (B) Patients with atypically distributed vegetation had significantly lower consistency than those with typically-distributed vegetation (P = 0.002; χ2-test) Patients with zero and one vegetation location had significantly higher consistency compared with patients with > 1 vegetation location (P = 0.003; χ2 = 13.7).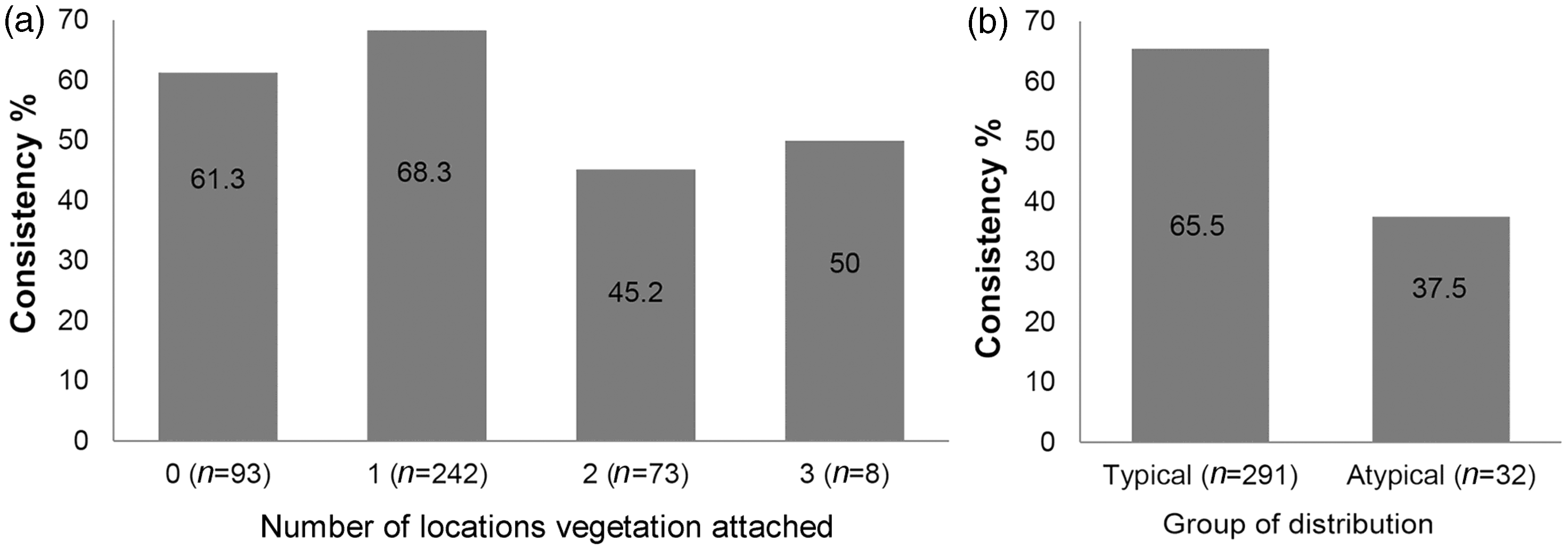
The RSIE group had a significantly higher rate of surgically-confirmed multifocal vegetation than the LSNIE and LSPIE groups (38.1%, 22.4%, 0%, P < 0.001; Figure 2): patients without vegetation findings during surgery were excluded from the calculation. Of the 32 patients with surgically-confirmed atypical vegetation, 68.8%, 31.2% and 0% had RSIE, LSNIE and LSPIE respectively.
Patients with infective endocarditis (n = 416) were divided into those with left-sided prosthetic valve infective endocarditis (LSPIE), left-sided native infective endocarditis (LSNIE) and right-sided infective endocarditis (RSIE). R rates of consistency between transthoracic echocardiography (TTE) and surgical findings, multifocal locations of vegetations and the proportion of patients with atypically distributed vegetation were compared. *Excludes 66 patients positive for vegetation with TTE but negative with surgery. **Includes 66 patients positive for vegetation with TTE but negative with surgery.
Location of vegetation for 63 patients with right-sided infective endocarditis (RSIE).

RSIE, right-sided infective endocarditis; PA, pulmonary artery; RV, right ventricle.
One patient with ventricular septal defect had vegetations in five locations: tricuspid valve, pulmonary valve, outflow of RV, within PA and within the RV.
Denominators for each group.
Although the age range of patients in this study was wide (1–78 years), there was no significant difference in terms of consistency of results between those aged ≤ 39 years (62.0%) and those aged > 39 years (68.1%).
Sensitivity analysis of the 63 patients with RSIE with or without CHD showed that, despite low numbers of patients, the presence of CHD did not influence the consistency of results for RSIE patients (consistency for CHD, 28/52 (53.8%), consistency for those without CHD, four of 11 (36.4%), P = 0.353).
Of 32 patients with surgically-confirmed vegetation, 14 patients were admitted by the end of 2007, and the other 18 were admitted after 2007. Eight-one patients were surgically-confirmed to have multifocal vegetation, while 57 were admitted after 2007.
Discussion
Transthoracic echocardiography is regarded as a useful method for diagnosing RSIE because it allows easy and correct diagnosis of tricuspid vegetations.5,21 This is the commonest affected location in RSIE, and the majority of patients with endocarditis are young people with IVDA, who have large vegetations.8,11 However, in our study, patients were not IVDA and 53 (84.1%) of the RSIE patients had CHD. These RSIE patients were younger, with better heart function and a more complicated intracardiac structure compared with patients with LSPIE or LSNIE, which may have made identification of vegetation more difficult in RSIE patients than in those without structural heart abnormalities. Compared with patients with LSNIE or LSPIE, the consistency of echocardiographic identification of vegetation with actual surgical findings was lower in the RSIE group. Therefore, the identification of RSIE by TTE may not be suitable for patients who have no history of IVDA or cardiac device insertion, but who do have structural abnormalities.
Vegetations are typically attached to the low-pressure side of heart valves including the mitral valve, tricuspid valve, aortic valve, and (less frequently) the pulmonary valve. For these areas, echocardiograpic images are good. Vegetation may be located anywhere on the components of the valvular and subvalvular apparatus, as well as on the mural endocardium of the cardiac chambers or the ascending aorta. 6 In the present study, surgery confirmed that atypically distributed vegetation was present in 32 (7.7%) of all IE patients, including vegetation in the aorta, pulmonary artery, left ventricle, right ventricle and other positions of the left and right heart. Compared with IE patients with typically-distributed vegetation, patients with atypically distributed vegetation had reduced consistency (by 28.0%) between TTE and surgical findings. This phenomenon was even more striking among RSIE patients. RSIE vegetation may not only be entrapped in the tricuspid and chordal apparatus, but also in mural and atrial or ventricular defect areas, and sometimes may present as embolized vegetation floating free in the right ventricle or pulmonary artery.4,22,23 In the present study, VSD was the dominant type of congenital abnormality for RSIE patients, and the chances of atypically distributed vegetation were higher for these patients than for those with LSNIE and LSPIE. In addition, we found a much lower consistency between TTE and surgical identification of vegetation among RSIE patients than among LSIE patients, which differs from a case report confirming TTE validity for diagnosing atypically distributed RSIE vegetation. 24 In our opinion, TTE may not be adequate for diagnosing suspected IE patients with CHD and/or atypically distributed vegetation because of its poor accuracy, especially for RSIE patients. Although the need for routine TEE in RSIE remains questionable, it may be useful in detecting unusual localizations of RSIE, such as infection on the Eustachian valve or on the Chiari network;25,26 in addition, TEE is more sensitive than TTE in the detection of pulmonary vegetation and abscesses (particularly those adjacent to the membranous septum), and associated left-sided involvement. 27 When necessary, X-ray or computed tomography should also be considered, to exclude pulmonary embolism.
In the present study, the consistency rate of TTE with surgical findings was only 45.7% when multifocal vegetations were verified during surgery. For RSIE patients, 24 (38.1%) had more than two vegetation involved locations, which may be related to the high proportion of structural abnormalities in the hearts of these patients. For RSIE patients with no history of IVDA or cardiac device insertion, attention is needed to identify widely distributed vegetation, especially those lesions that are atypically located. According to some reports, TEE is useful for identifying multifocal IE affecting valves, mural areas within atria and ventricles, and arteries.28–30
In our study the tricuspid was the most commonly affected valve in the right heart, and most patients with multifocal vegetation had CHD. Although some RSIE patients presented with left heart vegetation, only three (4.8%) patients had cyanotic CHD (all tetralogy of Fallot) and very few had trivial right-to-left shunt. In our opinion, this means that patients with CHD may have a higher risk of concomitant RSIE and LSIE even at an early disease stage, before a severe haemodynamic disorder. It seems VSD patients with associated valvular regurgitation have higher incidences of IE, 31 but it remains unclear whether the rectification of a structural abnormality reduces the risk of LSIE for patients who already have tricuspid regurgitation due to VSD or an ASD. Whether or not left-to-right shunts are present for RSIE patients with CHD, especially VSD, we consider that special attention is needed to investigate multifocal as well as concomitant left-sided vegetation, which seems to be more dangerous than isolated RSIE vegetation and should always be treated more aggressively by surgery. TEE is also recommended for CHD patients with suspicions of concomitant RSIE and LSIE.29,30
Several shortcomings with the present study should be mentioned. First, as a retrospective study, data were as good as were available, and were not always perfect. For example, although the complete study consistency (TTE results and surgical findings) was > 80% in our analysis, very few people received TEE (which should be considered in patients with poor image quality with TTE, and in those who have a negative TTE result despite a moderate or high level of clinical suspicion of IE). 32 The decision to operate on patients without a TEE was taken because most of the IE patients in this study had concomitant CHD and surgery was already necessary to correct a congenital abnormality. Secondly, the diagnosis of IE may be difficult at an early disease stage, when vegetative lesions are not yet present or are too small to be identified. 33 In this study, a few patients presenting with complicated pathologies had different TTE findings by the same cardiologist over a period of several days, so the final one (before surgery) was used in order to fulfil the study objective. Thirdly, with rapid development of the hospital facilities over recent decades, the echocardiographic equipment has greatly improved, which was difficult to take into consideration in our study. However, the accuracy of echocardiographic identification appeared to be similar year on year, despite improvements in equipment. Noticeably, 18 (56.6%) of patients with atypically distributed vegetation and 57 (70.4%) with multifocal vegetation were admitted after 2007 rather than in the first half of the study, which made the diagnosis of IE more challenging for doctors in the latter half of the study, even with better apparatus, and can to some extent explain the similar accuracy of TTE over the decade. No literature is available to compare the accuracy between the old and the more advanced echocardiographic apparatus in terms of RSIE, but careful selection of transducers (sometimes higher frequency transducers may improve spatial resolution), the use of the ‘zoom function’, and paying attention to the adjustment of sector width, depth and focus settings are recommended for accurate identification of vegetation in the right heart. 4
The time delay between the last echocardiography and surgery may influence the accuracy of vegetation identification, but was similar between the groups and therefore unlikely to influence the results of this study. Ideally, echocardiography should occur 1–3 days before surgery, considering the instability of vegetative lesions in the heart.
This study recorded a very low rate of positive blood cultures. This is likely due to the fact that Beijing Anzhen Hospital is a tertiary referral centre, receiving patients with IE from around the country, most of whom had received antibiotics in their local hospital prior to transfer.
The experiences of other developed countries in the treatment of patients with IE may not translate well to Chinese society because of different social and health backgrounds. For example, the incidence of chronic obstructive pulmonary disease (COPD) is higher in China than in western nations, partly because of higher rates of smoking and pollution in China. 34 Patients with COPD with barrel chests may have a lower rate of accuracy of vegetation identification in the right heart (where blood velocity is slower than in the left side) with TTE, compared with patients without COPD. 35 Our results are applicable to patients worldwide. Further research to investigate the accuracy of echocardiography for diagnosing IE without IVDA, but with CHD and other diseases, is worthwhile.
In conclusion, the objective findings from surgery in this retrospective study have shown that TTE may not be ideal for investigating vegetation in RSIE patients with no history of IVDA or cardiac device insertion. To promote accurate rates of TTE identification, doctors should be very alert to multifocal and atypically distributed vegetative lesions. For RSIE patients complicated with CHD, special caution is needed to exclude the potential presence of concomitant left-sided vegetation.
Footnotes
Declaration of conflicting interest
The authors had no conflicts of interest to declare in relation to this article.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.