
Abstract
Objective
To evaluate the relationship between plasma N-terminal prohormone B-type natriuretic peptide (NT-proBNP) and weaning outcomes, and the ability of NT-proBNP level to predict weaning success, in cancer patients with pulmonary complications undergoing noncardiac major surgeries.
Methods
Patients who were mechanically ventilated following postoperative respiratory failure were enrolled. NT-proBNP levels at the end of a 2-h spontaneous breathing trial were measured. Weaning was considered a success in patients who completed the trial and maintained spontaneous breathing following extubation for >48 h.
Results
Out of 29 patients, 22 patients weaned successfully but weaning failed in 7 patients. Plasma NT-proBNP was significantly higher in the weaning failure group than in the weaning success group. For predicting weaning success, the optimal NT-proBNP threshold value at the end of the spontaneous breathing trial was <448 ng/l (receiver operating characteristic analysis; sensitivity 68.18%, specificity 85.71%, positive predictive value 93.7% and negative predictive value 46.2%).
Conclusion
Measuring NT-proBNP at the end of a spontaneous breathing trial may assist in predicting weaning success, as a noninvasive, quantitative and repeatable indicator of cardiac stress in patients with postsurgical respiratory failure.
Keywords
Introduction
Postoperative pulmonary complications following major surgery remain a challenge to surgeons.1,2 In patients requiring prolonged mechanical ventilation, there is an associated increase in costs, risks and mortality rates.3,4 Intubated patients should, therefore, be weaned from mechanical ventilation as soon as possible after assessing readiness for spontaneous breathing.
The pathophysiology of weaning failure is complex: respiratory failure is traditionally regarded as the major cause, while cardiac stress may also play a role in patients who are difficult to wean.5–7 Thus, establishing a simple and noninvasive method to detect cardiac dysfunction in patients who are difficult to wean from mechanical ventilation is important.
Both B-type natriuretic peptide (BNP) and N-terminal prohormone (NT-pro)BNP are sensitive and specific biomarkers used for screening and diagnosis of heart failure.8–10 BNP is co-secreted with biologically inactive NT-proBNP, and both are produced by the ventricles of the heart in response to myocardial stretch.11,12 Either BNP or NT-proBNP values may be used to detect cardiac dysfunction during weaning from mechanical ventilation, and may differentiate weaning success from failure.13–16 There is a single published study focusing on difficult-to-wean patients with chronic obstructive pulmonary disease, 14 but little is known about the association between plasma NT-proBNP concentration and weaning outcomes in postoperative patients.
The present study evaluated the relationship between NT-proBNP plasma levels and weaning outcomes, and whether NT-proBNP concentration could be used to predict weaning success in patients with pulmonary complications undergoing noncardiac surgeries.
Patients and methods
Patients
This study was conducted at the Department of Intensive Care Medicine, Cancer Center, Sun Yat-sen University, Guangzhou, China, between December 2010 and August 2011. Adult patients with cancer, and postsurgical pulmonary complications, requiring invasive mechanical ventilation for more than 24 h were prospectively, sequentially enrolled. Exclusion criteria comprised: (I) patients with tracheostomy; (II) patients with a history of chronic congestive heart failure; (III) patients with moderately to severely impaired renal function whose estimated glomerular filtration rate was <60 ml/min per 1.73 m2. The study was approved by the Institutional Ethics Committee of the Cancer Center, Sun Yat-sen University and written informed consent was obtained from all patients or their legal proxies.
Protocol
All patients receiving mechanical ventilation (Evita® 4 edition ventilator; Dräger Medical AG and Co. KG, Lübeck, Germany) underwent formal daily assessment the potential for discontinuation to assess whether the following criteria were satisfied, in accordance with a previously published study: 17 (I) resolution of acute phase of the disease; (II) adequate oxygenation as indicated by partial pressure of oxygen in arterial blood ≥60 mmHg at fraction of inspired oxygen ≤40% and positive end-expiratory pressure ≤5 cmH2O; (III) stable cardiovascular system; (IV) temperature <38℃; (V) no significant respiratory acidosis; (VI) haemoglobin ≥8 g/dl; (VII) no further need for continuous sedative agents; (VIII) stable metabolic status. If the criteria were met, a 2-h spontaneous breathing trial was performed through a T-tube using oxygen (flow rate 2–4 l/min), with the patient in a semirecumbent position. The trial was directed by intensive care unit (ICU) physicians and nurses (W.L., J.Q., Q.S. and B.G.).
Patients were regarded as having a spontaneous breathing trial failure and were reconnected to mechanical ventilation if they displayed any of the following signs: 17 (I) respiratory rate >35 breaths/min; (II) arterial oxygen saturation <90%; (III) heart rate >140 beats/min; (IV) systolic blood pressure >180 mmHg or diastolic blood pressure <90 mmHg; (V) increased accessory respiratory muscle use; (VI) change in mental status; (VII) diaphoresis and a worsening of discomfort signs. Patients with successful completion of the spontaneous breathing trial were extubated at the end of the trial. Extubation failure was defined as the patient requiring reintubation within 48 h following the spontaneous breathing trial. Weaning failure was defined as either spontaneous breathing trial failure or extubation failure. Weaning success was defined as patients who completed the 2-h spontaneous breathing trial and were successfully extubated.
Data collection and NT-proBNP assay
Demographic data, preoperative cardiopulmonary assessment, surgical procedure, pulmonary complications, and Acute Physiology and Chronic Health Evaluation II (APACHE II) 18 severity score were documented immediately at ICU admission. Heart rate, mean arterial blood pressure, pulse oximetry and continuous central venous pressure were monitored for the duration of ICU stay. During assisted mechanical ventilation, each patient’s daily fluid balance, arterial blood gas and ventilation parameters including duration of mechanical ventilation prior to weaning, respiratory rate, tidal volume, pressure support, fraction of inspired oxygen and positive end-expiratory pressure were recorded until immediately prior to the spontaneous breathing trial.
Venous blood samples (3 ml) were collected from enrolled patients on two occasions: (I) within 0.5 h prior to intubation (baseline NT-proBNP value); (II) at the end of the 2-h spontaneous breathing trial (end-SBT NT-proBNP value). Following blood collection into tubes containing 2 mg/ml ethylenediaminetetra-acetic acid (EDTA), blood samples were centrifuged at 2390 g for 5 min to obtain plasma, which was stored at −20℃ prior to analysis. NT-proBNP was measured using a commercially available immunoassay kit (Elecsys®proBNP; Roche Diagnostics, Basel, Switzerland), according to the manufacturer’s instructions. ICU staff were blinded to the results of NT-proBNP analysis.
Statistical analyses
Data analysis was performed using the SPSS® software package, version 13.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Categorical variables, expressed as percentages, were compared using χ2-test or Fisher's exact test. Continuous variables are presented as mean ± SD and were analysed using Student's t-test or Mann–Whitney U-test as appropriate for the distribution of the data. NT-proBNP values are presented as median (25th–75th percentile) and were compared using Mann–Whitney U-test. A two-tailed P value < 0.05 was considered to be statistically significant. Receiver operating characteristic (ROC) curve statistical analyses were performed using MedCalc software, version 9.2 (MedCalc Software, Mariakerke, Belgium). The ability to use plasma NT-proBNP levels to discriminate between two groups of patients ending in either weaning success or failure was analysed using the method of DeLong et al. 19
Results
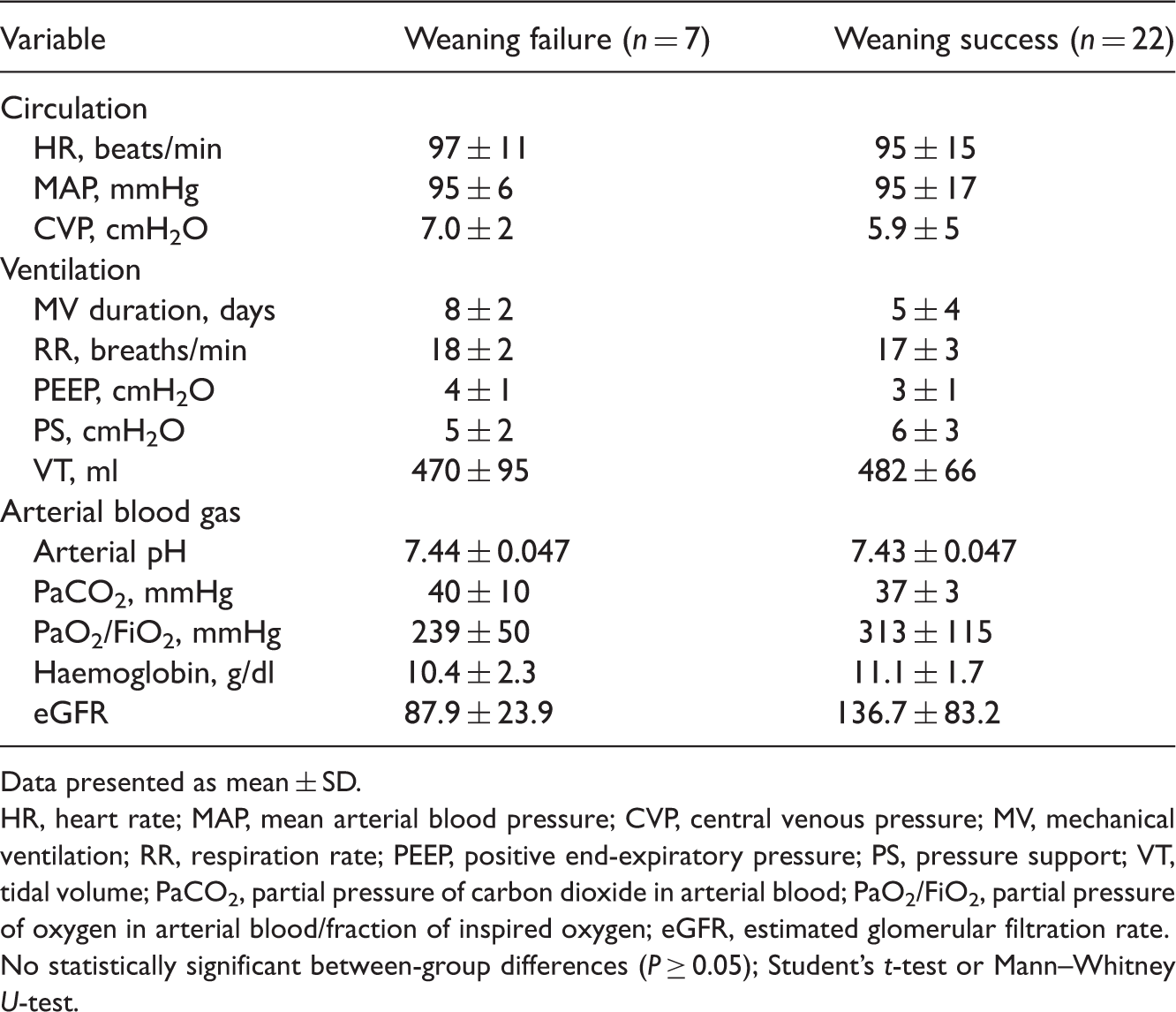
A total of 43 adult patients with cancer and postsurgical pulmonary complications, requiring invasive mechanical ventilation for more than 24 h, were admitted to the department of Intensive Care Medicine between December 2010 and August 2011. Of these, 29 patients were enrolled into the study and 14 patients were excluded (five patients with tracheostomy, two patients with a history of chronic congestive heart failure, and seven patients with moderate to severely impaired renal function whose estimated glomerular filtration rate was <60 ml/min per 1.73 m2). Overall, 22 patients succeeded in the weaning process and seven patients failed. Among those who failed weaning, two patients could not tolerate the 2-h spontaneous breathing trial while the other five patients required reintubation within 48 h (Figure 1). Most of the patients enrolled had undergone thoracic surgery (5/7 [71.4%] in the weaning failure group and 19/22 [86.4%] in the weaning success group). Pneumonia and acute lung injury or acute respiratory distress syndrome accounted for the two most common causes of postoperative mechanical ventilation. There were no significant between-group differences regarding age, sex, body mass index, APACHE II score, preoperative echocardiography (left ventricular ejection fraction; left ventricular fractional shortening; left ventricle diameter; left atrial diameter; right ventricle diameter; right atrial diameter) and preoperative pulmonary function (forced expiratory volume in 1 s; forced vital capacity; maximal voluntary ventilation; diffusing capacity for carbon monoxide) (Table 1). In addition, there were no significant between-group differences in circulatory variables, ventilatory conditions or arterial blood parameters at the end of the 2-h spontaneous breathing trial (Table 2).
Flow chart showing weaning outcomes in adult patients with cancer, and postsurgical pulmonary complications, who had received invasive mechanical ventilation for more than 24 h prior to weaning. MV, mechanical ventilation; SBT, spontaneous breathing trial. Demographic and clinical characteristics of adult patients with cancer, and postsurgical pulmonary complications, who had received invasive mechanical ventilation for more than 24 h prior to weaning (n = 29). Data presented as mean ± SD or n (%) of patients. BMI, body mass index; APACHE II, Acute Physiology and Chronic Health Evaluation II; ICU, intensive care unit; LVEF, left ventricular ejection fraction; LVFS, left ventricular fractional shortening; LVD, left ventricle diameter; LAD, left atrial diameter; RVD, right ventricle diameter; RAD, right atrial diameter; FEV1, forced expiratory volume in 1 s; FVC, forced vital capacity; MVV, maximal voluntary ventilation; DLCO, diffusing capacity for carbon monoxide; ALI, acute lung injury; ARDS, acute respiratory distress syndrome. No statistically significant between-group differences (P ≥ 0.05); Student's t-test or Mann–Whitney U-test for continuous variables; χ2-test or Fisher's exact test for categorical variables. Variables measured at end of 2-h spontaneous breathing trial in adult patients with cancer, and postsurgical pulmonary complications, who had received invasive mechanical ventilation for more than 24 h prior to weaning (n = 29). Data presented as mean ± SD. HR, heart rate; MAP, mean arterial blood pressure; CVP, central venous pressure; MV, mechanical ventilation; RR, respiration rate; PEEP, positive end-expiratory pressure; PS, pressure support; VT, tidal volume; PaCO2, partial pressure of carbon dioxide in arterial blood; PaO2/FiO2, partial pressure of oxygen in arterial blood/fraction of inspired oxygen; eGFR, estimated glomerular filtration rate. No statistically significant between-group differences (P ≥ 0.05); Student's t-test or Mann–Whitney U-test.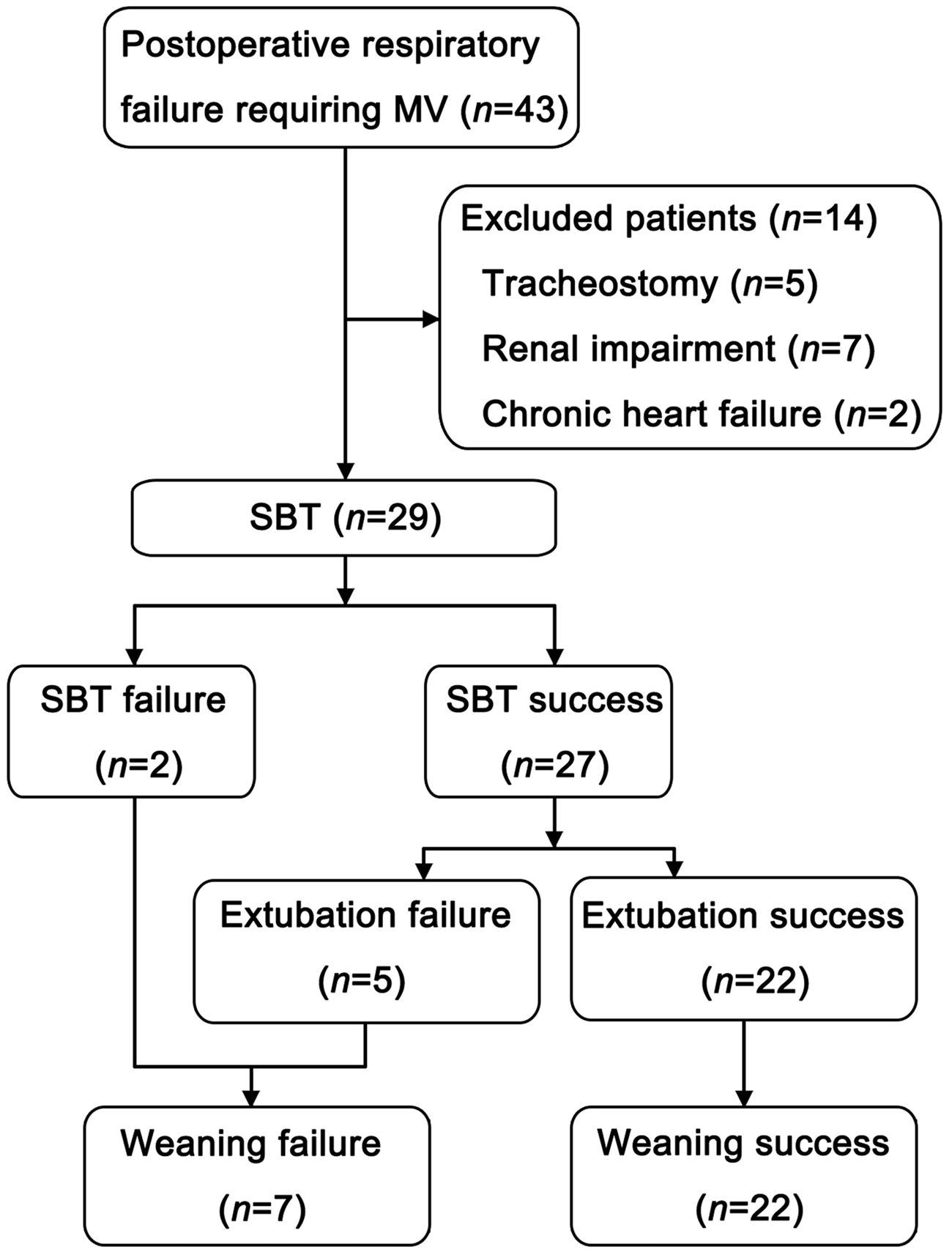

Plasma NT-proBNP concentrations were not significantly different between the two groups at baseline: the median level was 917 (270–1934) ng/l in the weaning failure group and 569 (245–2828) ng/l in the weaning success group (P = 0.752) (Figure 2A). At the end of the 2-h spontaneous breathing trial, plasma NT-proBNP concentrations were significantly higher in the weaning failure group than in the weaning success group (P = 0.041; median levels 829 [464–1234] ng/l and 345 [153–770] ng/l, respectively; Figure 2B).
Box-and-whisker plots comparing plasma levels of N-terminal prohormone B-type natriuretic peptide (NT-proBNP) between weaning success (n = 22) and failure (n = 7) groups of adult patients with cancer and postsurgical pulmonary complications who had received invasive mechanical ventilation for more than 24 h prior to weaning. NT-proBNP levels were measured on two occasions: (A) baseline NT-proBNP within 0.5 h prior to mechanical ventilation; (B) NT-proBNP at the end of the 2-h spontaneous breathing trial (End-SBT). The central bands of the box are the medians; the extremities of the box are the 25th and 75th percentiles; error bars represent maximum and minimum outliers; the circle represents an extreme outlier.
The ROC analysis estimated the diagnostic performance of NT-proBNP in detecting weaning success at the end of the spontaneous breathing trial (Figure 3). The area under the ROC curve was 0.760 (95% confidence interval, 0.566, 0.898). A cutoff value of 448 ng/l corresponded with the optimum values for accuracy (69.9%), along with sensitivity (68.18%), specificity (85.71%), positive predictive value (93.7 %) and negative predictive value (46.2 %).
Receiver operating characteristic (ROC) curve showing N-terminal prohormone B-type natriuretic peptide (NT-proBNP) value at the end of a 2-h spontaneous breathing trial, used to predict weaning success. Area under the ROC curve = 0.76 (95% confidence interval 0.566, 0.898, P = 0.0086). The diagonal line dividing the area = 0.5.
Discussion
The present study demonstrated a significant difference in NT-proBNP levels at the end of a 2-h spontaneous breathing trial between mechanical ventilation weaning success and failure groups, concurring with the results of other studies.14,15 These results suggest that factors leading to weaning failure may also contribute to the secretion of NT-proBNP. It is known that natriuretic peptides, including BNP and NT-proBNP, are synthesized in the heart in response to cardiac wall distension and stretching, and neurohormonal activation. 20 During a spontaneous breathing trial, sedation is withdrawn and cardiopulmonary stresses are produced as the increased ventilatory drive alters intrathoracic pressure, increases venous return, augments left ventricular transmural pressure and increases afterload. 21 These stimuli induce natriuretic peptide secretion within minutes in response to heart volume and pressure overload. 22
The results of the present investigation contradict one published study, 13 in which baseline BNP levels prior to a spontaneous breathing trial, rather than those measured at the end of a spontaneous breathing trial, differed between patients who either failed or succeeded weaning. This discrepancy may be explained by several factors. First, BNP, rather than NT-proBNP, was measured in the published study. It is known that BNP and NT-proBNP have different half-lives 23 and reaction times to stimuli, 24 which may in turn cause variable concentrations. Secondly, the sampling interval for NT-proBNP in the present investigation was longer than that for BNP in the published study, which used a 1-h interval. 13 Optimum sampling intervals for assessing increases in BNP and NT-proBNP levels during spontaneous breathing trials, however, remain unknown. Thirdly, the study population in the present investigation mainly included noncardiac postoperative patients whereas the published study included general ICU patients from all causes. 13
Using ROC analysis, a cutoff NT-proBNP value of 448 ng/l at the end of the 2-h spontaneous breathing trial predicted weaning success with the highest diagnostic accuracy. Measuring the percentage change in BNP level during a spontaneous breathing trial to predict weaning outcome 16 has been shown to have higher diagnostic accuracy than in the present investigation, which measured NT-proBNP levels (91% 16 versus 69.9%). Unlike the present investigation, however, patients with decreased glomerular filtration rate were not excluded in the published study. 16 In ICU patients, the high prevalence of impaired kidney function may lead to higher plasma NT-proBNP concentrations by lowering renal clearance. 25 This factor may contribute to the discrepancy between the two studies, in addition to the fact that the present investigation included a relatively small study population.
The goal of safe weaning is to reach a balance between delayed and premature weaning. Despite a number of prerequisites for assessing the readiness to wean from mechanical ventilation, approximately 20–30% of artificially ventilated patients fail their first weaning trial. 26 Combining BNP measurements with a spontaneous breathing trial has been reported to improve the prediction of extubation success from 80%, based on the spontaneous breathing trial criteria alone, to 97%. 16 Thus, measurement of NT-proBNP levels may be useful in helping to select the time at which patients are ready for weaning.
Measurements of NT-proBNP had a high positive value for predicting weaning success in the present study; however, the ability to predict weaning failure appeared unsatisfactory (negative predictive value 46.2%). These results suggest that in some circumstances, NT-proBNP measurements alone, without clinical interpretation and knowledge, may not be useful in predicting weaning trial failure. The causes of failure in spontaneous breathing trials, or reintubation, are complicated. Respiratory failure and cardiac dysfunction 27 have been reported as being important mechanisms for weaning failure. NT-proBNP values were shown to be higher in patients when heart failure was diagnosed as the cause of weaning failure.14,15 Measurements of plasma BNP levels are useful in the diagnosis of heart failure, with high sensitivity and specificity and strong positive predictive values. 10 In the case of borderline NT-proBNP values, however, it is necessary to confirm or exclude diagnosis by additional means, such as echocardiography. 28 A number of complicating factors commonly related to patients in ICU could potentially affect plasma BNP levels, including sepsis, shock, renal insufficiency, anemia and atrial fibrillation. 29 Thus, future long-term prospective studies with larger sample sizes are required to confirm the findings of the present study.
There are several limitations inherent in the present study. First, a relatively small sample of specifically selected postoperative cancer patients was included. It remains to be determined, therefore, whether NT-proBNP levels could be used as a predictor of weaning outcome in patients with different medical backgrounds and needs, receiving mechanical ventilation. Secondly, the elevated NT-proBNP levels alone were not enough to identify the underlying causes of weaning failure. Although natriuretic peptide levels have been used in the differential diagnosis of respiratory and cardiac dyspnoea, they have been shown to have only low to moderate accuracy. 30 High levels of NT-proBNP might, however, mandate further investigation using echocardiography, measurement of pulmonary artery occlusion pressure and central venous oxygen saturation to diagnose heart failure and apply appropriate intervention. Finally, the present study focused on NT-proBNP and did not compare BNP and NT-proBNP levels in predicting weaning outcome. It may not be concluded, therefore, whether one natriuretic peptide is superior to the other. In the setting of the present study, a combination of NT-proBNP with BNP and other hemodynamic measurement may increase the overall diagnostic accuracy.
In summary, measuring NT-proBNP at the end of a 2-h spontaneous breathing trial may assist in predicting weaning outcome in patients with postsurgical respiratory failure, and could be suggested as a noninvasive, quantitative and repeatable indicator of cardiac stress in patients with postsurgical respiratory failure.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.