
Abstract
Objective
*Liu-Qun Jia and Yong-Chun Shen contributed equally to this work and are joint first authors.
Methods
A comprehensive search of the PubMed and Embase® literature databases identified outcome data from published studies estimating the diagnostic accuracy of neutrophil CD64 expression for neonatal infection. Summary estimates for sensitivity, specificity, diagnostic odds ratios (DOR) and the area under the summary receiver operating characteristic curve (AUC) were calculated using a bivariate random-effects approach.
Results
Twelve studies including 1915 neonates were analysed. Summary estimates (95% confidence intervals) for CD64 expression in the diagnosis of neonatal infection were: sensitivity, 0.78 (0.75, 0.81); specificity, 0.81 (0.78, 0.83); DOR, 21.27 (11.71, 38.65); positive-likelihood ratio, 4.53 (3.22, 6.36); negative-likelihood ratio, 0.23 (0.14, 0.37); AUC, 0.89.
Conclusions
Neutrophil CD64 expression can be used as an additional test in the diagnosis of neonatal infection. Results of a CD64 assay should not be used alone to diagnose such infections, but should be interpreted in combination with other test results and clinical findings.
Introduction
Infection is one of the most important causes of neonatal mortality. 1 Early identification of neonatal infection is, however, a major diagnostic problem, particularly in preterm and very low-birthweight infants, due to the presence of nonspecific clinical signs and the limitations of current diagnostic procedures.1,2 The use of conventional haematological tests in assisting frontline neonatologists to differentiate between infected and noninfected infants is limited since the total white cell count has a wide normal range, and automated laboratory measurements of neutrophil counts are inaccurate in the presence of nucleated red blood cells. 2 Blood culture is considered to be the gold-standard method for the diagnosis of bacteraemia but is fraught with difficulties: bacterial incubation is time-consuming (2–4 days); only small volumes of blood can be taken from infants, which increases the possibility of negative results; bacteraemia in the neonate is often transient or intermittent, especially during the early stages of infection. 2
Neonatal sepsis is a common and severe type of infection: both early and late-onset neonatal sepsis are substantial causes of neonatal morbidity and mortality. 3 Infants with neonatal sepsis often require prolonged hospital admission and have a much higher chance of developing chronic lung disease and neurodevelopmental complications compared with neonateswithout sepsis. 4
Expression of CD64, an antigen present in low concentrations on the surface of nonactivated neutrophils, 5 has been proposed as a diagnostic marker for the evaluation of infection.6,7 CD64 concentration increases five- to 10-fold in response to bacterial infection in preterm and term infants, suggesting that it might be a useful marker of infection in neonates.8,9 Advances in flow cytometric technology have made it possible to identify and quantify CD64 on neutrophils with a rapid turnaround of <4 h using minimal blood volume. 10
The performance of neutrophil CD64 expression in the diagnosis of infection has been investigated in several studies, which have yielded variable results.11–13 The aim of the present study was to perform a meta-analysis to establish the overall diagnostic accuracy of CD64 expression in neonatal infection. In addition, the diagnostic accuracy of CD64 expression, according to time of testing after onset of infection and in cases of neonatal sepsis specifically, was determined. These data should provide important up-to-date information on neutrophil CD64 expression in neonatal infection.
Materials and methods
Data sources and search strategy
Two investigators (L.-Q.J. and Y.-C.S.) independently performed a systematic electronic search of the PubMed and EMBASE® databases up to 1 February 2013, to identify potentially relevant articles. The Cochrane Library database was also searched for relevant reviews and meta-analyses over the same time-period. The following search terms were used: “neonatal” or “newborn” or “infant” and “sepsis” or “septicaemia” or “septicemia” or “pyaemia” or “pyemia” or “infection” and “CD64”. Searches were limited to English and Chinese language publications. The bibliographies of all selected articles were screened to identify potentially relevant additional studies.
Study selection and data extraction
Two independent reviewers (L.-Q.J. and Y.-C.S.) screened the titles and abstracts of all selected studies for relevance. Disagreements were resolved by a third reviewer (F.-Q.W.). The strength of individual studies was weighted for relevance, based on the following criteria: (i) clinical domains should include patients with suspected sepsis or infection and the patients should be neonatal; (ii) reference diagnostic standards were clearly described and all specimens were diagnosed using these standards; (iii) completeness of data (numbers of true-positive [TP], false-positive [FP], true-negative [TN] and false-negative [FN] results) were reported to allow reconstruction of the diagnostic two-by-two table. The following data were extracted from the selected studies: first author; year of publication; number of patients infected/not infected; standard of infection diagnosis (clinical, infection suspected on a clinical basis; proven, culture-proven infection with an identified micro-organism); method of CD64 analysis; analysis cut-off values; numbers of TP, FP, TN and FN specimens; sensitivity and specificity; Quality Assessment for Studies of Diagnostic Accuracy score.
Methods appraisal
The methodological quality of included studies was evaluated using the QUADAS Tool. 14 This provides an evidence-based approach to quality assessment intended for use in systematic reviews of diagnostic accuracy studies. A quality index is generated, with a maximum value of 14.
Statistical analyses
Standard methods recommended for meta-analyses of diagnostic test evaluations were used. 15 Analyses were performed using Meta-DiSc, version 1.4 (ftp://ftp.hrc.es/pub/programas/metadisc/Metadisc_update.htm 16 ) and Stata®, version 12.0 (StataCorp LP, College Station, TX, USA) software. Sensitivity, specificity, positive-likelihood ratio (PLR), negative-likelihood ratio (NLR) and diagnostic odds ratio (DOR) were computed for each study. Statistical heterogeneity among studies was assessed by Q-test and I2 statistics. A P-value of <0.05 indicated a statistically significant level of heterogeneity. According to the result of heterogeneity analysis, the appropriate statistical model for meta-analysis was chosen: in the event of heterogeneity, a random model was chosen; if there was no heterogeneity, a fixed model was used.17,18
The numbers of patients with TP, FP, TN or FN test results were obtained from the selected studies directly or through recalculation, based on the reported measures of accuracy and the incidence and specimen size of the study. Sensitivity, specificity and DOR with 95% confidence intervals (CI) were calculated for each study based on the reconstructive two-by-two table. The results from included studies were plotted on a receiver operating characteristic (ROC) plot of sensitivity against specificity with the specificity axis reversed. In addition, area under the summary ROC curve (AUC) values was determined to demonstrate any trade-offs between sensitivity and specificity since it represents a global summary of test performance. The Q-value (the intersection point of the summary ROC curve with a diagonal line from the left upper corner to the right lower corner of the ROC space) was used as a global measure of diagnostic test efficacy, and corresponds to the highest common value of sensitivity and specificity for the test. This point does not indicate the only, or even the best, combination of sensitivity and specificity for a particular clinical setting, but represents an overall measure of the discriminatory power of a test.
Subgroup analyses were performed on the diagnostic accuracy of CD64 tests according to the onset of infection and accuracy in the diagnosis of neonatal sepsis specifically. Publication bias of included studies was assessed by Deeks’ funnel plot asymmetry test using Stata®, version 12.0 software. 19
Results
Summary of the major characteristics of the 12 studies selected for a meta-analysis to establish the accuracy of neutrophil CD64 expression for the diagnosis of neonatal infection.

Clinical infection defined as infection suspected on a clinical basis; proven infection defined as culture-proven infection with an identified micro-organism.
QUADAS has a maximum score of 14 indicating the highest quality.
Antibody-phycoerythrin molecules bound per cell.
Arithmetic mean + 3 SD of the percentage of CD64 + cells found in normal neonates.
CD64 index.
Neutrophil CD64 mean fluorescence intensities.
Median monocyte/neutrophil CD64 ratio.
QUADAS, Quality Assessment for Studies of Diagnostic Accuracy; TP, true-positive; FP, false-positive; FN, false-negative; TN, true-negative; FCM, flow cytometric technology.
Forest plots of the sensitivity and specificity of CD64 in diagnosing neonatal infection are shown in Figure 1 and Figure 2, respectively. Significant heterogeneity between studies was demonstrated for sensitivity and specificity (I2 = 82.6% and 83.1%, respectively). Given the heterogeneity, the random-effects model approach was selected for further analysis. The pooled PLR was 4.53 (95% CI 3.22, 6.36), NLR was 0.23 (0.14, 0.37) and DOR was 21.27 (11.71, 38.65). The sensitivity, specificity and 95% CI (precision of estimation of pooled sensitivity and specificity) of the 12 studies are shown in Figure 3. The maximum joint sensitivity and specificity (Q-value) was 0.82 and the AUC was 0.89, indicating a moderate level of overall accuracy.
Forest plot showing the sensitivity of CD64 expression in the diagnosis of neonatal infection overall and in 12 individual studies selected as part of a meta-analysis. Forest plot showing the specificity of CD64 expression in the diagnosis of neonatal infection overall and in 12 individual studies selected as part of a meta-analysis. Summary receiver operating characteristic (ROC) curves for the sensitivity and specificity of CD64 expression in the diagnosis of neonatal infection in 12 studies selected as part of a meta-analysis. AUC, area under the curve.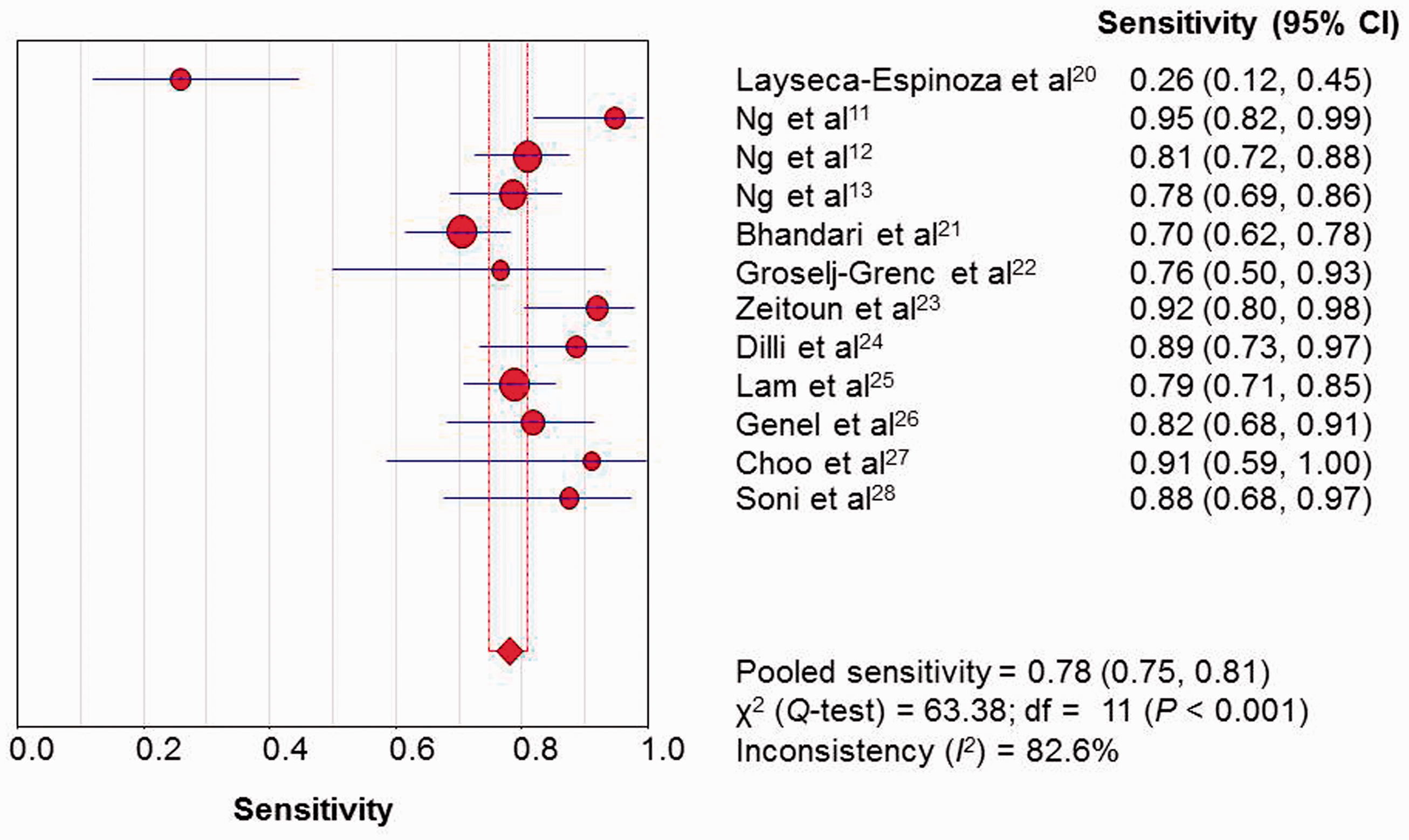


Pooled estimates (and 95% confidence intervals) of the sensitivity, specificity and accuracy of CD64 expression tests according to the time after onset of infection or the specific diagnosis of neonatal sepsis, in selected studies included in a meta-analysis.
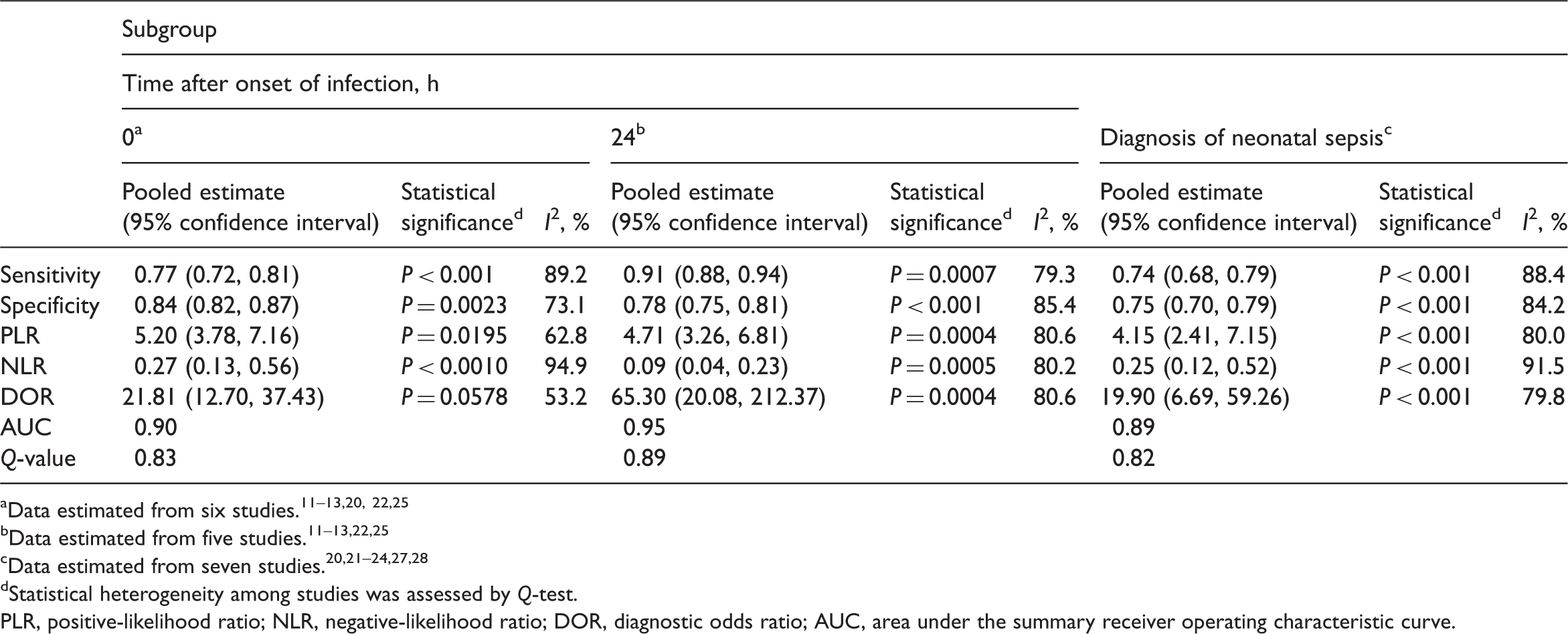
Statistical heterogeneity among studies was assessed by Q-test.
PLR, positive-likelihood ratio; NLR, negative-likelihood ratio; DOR, diagnostic odds ratio; AUC, area under the summary receiver operating characteristic curve.
Deeks’ funnel plot asymmetry test revealed a low likelihood of publication bias with a slope coefficient P-value of 0.94, suggesting symmetry in the data.
Discussion
Neonates constitute a special group with regard to the diagnosis of infection. Clinical signs and symptoms, if present, are subtle and nonspecific, and current laboratory tests do not perform well. Early identification of neonatal infection is valuable for accurate therapeutic decision-making in order to reduce morbidity and mortality and to limit the unnecessary use of anti-infective treatment in patients with clinical signs but without infection 3 .
To the authors’ knowledge, the present meta-analysis is the first to estimate the diagnostic accuracy of neutrophil CD64 expression for neonatal infection. In addition, the diagnostic accuracy of CD64 expression for neonatal infection at different time-points after the onset of infection, and specifically in neonatal sepsis, were explored.
Twelve studies were included in the present meta-analysis and showed that CD64 plays an important role in diagnosing neonatal infection. Using a bivariate random-effects approach, a summary estimate of 78% for sensitivity and 81% for specificity of CD64 expression testing was determined; the maximum joint sensitivity and specificity (Q-value) was 0.82 while the AUC was 0.89, indicating a moderate level of overall accuracy.
The DOR is a single indicator of test accuracy that combines data from sensitivity and specificity into a single number. 29 It is the ratio of the odds of positive test results in a patient with disease relative to the odds of positive test results in a patient without disease; the value ranges from 0 to infinity, with higher values indicating higher accuracy. In the present meta-analysis, the mean DOR was found to be 21.27, indicating a moderate level of overall accuracy. Likelihood ratios, such as the PLR and NLR, are considered to be more clinically meaningful measures of diagnostic accuracy. Ratios of more than 10 or less than 0.1 generate large and often conclusive shifts from pre-test to post-test probability, indicating high accuracy. 30 The pooled PLR of 4.53 estimated in the present meta-analysis suggested that patients with neonatal infection have an approximately fivefold higher chance of being CD64-positive compared with patients without infection; the pooled NLR of 0.23 suggests that if CD64 expression was negative, the probability of the patient having N infection is 23%, which is not low enough to rule out infection. These data suggest that a negative CD64 result alone should not be used to rule out neonatal infection.
Data from the present meta-analysis demonstrated that the CD64 diagnostic test had the highest sensitivity (91%) at 24 h after infection onset. Increases in CD64 are demonstrable within 4–6 h of neutrophil contact with pro-inflammatory cytokines, with peak expression observed >48 h. 31 This suggests that measurement of CD64 at the onset of infection may increase the chance of a false-negative result. Normalization of increased neutrophil CD64 expression during antibiotic therapy has been reported, 32 indicating the importance of measuring neutrophil CD64 expression at the correct time.
Even if CD64 expression is increased with infection, the degree of expression is always lower than that observed in cases of sepsis. 5 The present meta-analysis, however, failed to demonstrate any differences in diagnostic accuracy between cases of infection and cases of sepsis: seven studies focusing specifically on sepsis were analysed and the overall pooled sensitivity and specificity of CD64 testing were 0.74 and 0.75, respectively.
False-negative and false-positive results may be related to the different cut-off values of the reported CD64 tests. In the 12 studies included in the present meta-analysis, a wide variation in sensitivity and specificity was reported, with a wide range of cut-off values even if the same method for the measurement of CD64 expression had been employed. In one study, the sensitivity and specificity of the CD64 test changed when different cut-off values were used. 12
Some limitations should be considered when interpreting the results of the present meta-analysis. First, the sample sizes of several of the included studies were small meaning that they did not have adequate power to assess diagnostic accuracy. Secondly, the included studies used different cut-off values for CD64 expression and performed the tests at different times after the onset of infection, which may contribute to the heterogeneity between studies. Thirdly, the present meta-analysis was limited to published studies, meaning that it may miss some of the ‘grey’ literature.
In conclusion, the results from the present meta-analysis of 12 published studies demonstrated that neutrophil CD64 expression can play a role in the diagnosis of neonatal infection, and that the diagnostic accuracy of the test is moderate. The results of the CD64 assay should not be used alone to diagnose neonatal infection but should be interpreted in combination with other test results and clinical findings. Further studies to determine the optimal time for CD64 expression testing after the onset of infection and the optimal cut-off values are required.
Footnotes
Declaration of conflicting interest
The authors declare that there are no conflicts of interest.
Funding
This work was supported by grants from the National Natural Science Foundation of China to Dr Fu-Qiang Wen (no. 81230001 and no. 31171103) and Dr Tao Wang (no. 31000513).