
Abstract
The role of circumcision and its benefits has received increased attention across several disciplines in recent years; however, there is increasing concern that some uncommon complications such as severe infections are being related to post-circumcision. We describe the clinical course of a 14-day-old boy who had Methicillin-resistant Staphylococcus aureus urosepsis after circumcision.
Introduction
Circumcision is the removal of the foreskin from the penis. 1 During the surgery, usually, the foreskin is opened, adhesions are removed, and the foreskin is separated from the glans. Following that, a device may be fixed, and then the foreskin is cut off. Male circumcision is usually an elective procedure that is practiced for religious, cultural, and medical reasons. The procedure is almost universal in the majority of the Middle East and Gulf countries, Africa, and Central Asia. 2 Methicillin-resistant Staphylococcus aureus (MRSA) is a kind of staphylococcus bacteria that has become resistant to many of the antimicrobials used to treat staphylococcal infections.
Local and systemic infections consider uncommon complications of circumcision; however, these infections have a significant clinical problem. MRSA infections are in-creasingly reported as post-circumcision infections. Most reported cases, including MRSA infections, involve the skin and soft tissues in the form of cellulitis, impetigo, pyoderma, necrotizing fasciitis, and Staphylococcal scalded skin syndrome, while invasive MRSA complications such as bacteremia, urinary tract infections (UTIs), arthritis, pneumonia, and osteomyelitis have been rarely reported. We reported a case of MRSA urosepsis in a male neonate after circumcision.
Case presentation
A 2 weeks old term boy neonate 37 weeks, a product of elective C/S due to the previous scar, with birth weight 3.2 kg, with no neonatal intensive care unit (NICU) admission, presented at the age of 14 days to the emergency department with a history of 1 day fever and hypoactivity. He had no respiratory symptoms, no vomiting, no diarrhea, and no jaundice; he had his circumcision 2 days before presentation at a private clinic which was an unremarkable Plastibell procedure. Upon examination, his febrile temperature was 39.1°C, tachycardia heart rate (HR) 170, and was lethargic; there was mild erythema around the circumcision site, no laceration, and no evidence of soft tissue infection. He was given one push of normal saline of 10 mL/kg. Full septic workup was done and started on IV ampicillin and cefotaxime as per local guidelines. The initial laboratory results are shown in Table 1. Others, including ammonia, coagulation profile, and cerebrospinal fluid (CSF) studies, all were normal. The baby was continued on ampicillin and cefotaxime till the second day, where both blood and urine culture results were positive for MRSA organism, so antibiotics were upgraded to vancomycin, and his clinical status and fever pattern improved from the second day onwards. He stayed at the hospital for a total of 14 days, the repeated set of blood and urine cultures were negative, and his MRSA screening was positive upon admission, so MRSA decolonization was completed for two cycles as he was still positive after the first cycle (chlorhexidine body wash and mupirocin nasal topical). Ultrasound kidney was done as a part of atypical UTI workup, which revealed slight fullness of the renal pericalyceal system bilaterally and incidental finding of a cyst within the splenic parenchyma needed follow-up sonography. Echocardiography was done as a part of MRSA bacteremia protocol which was a normal study with no vegetation and only tiny patent foramen ovale.
Laboratory investigations upon admission.
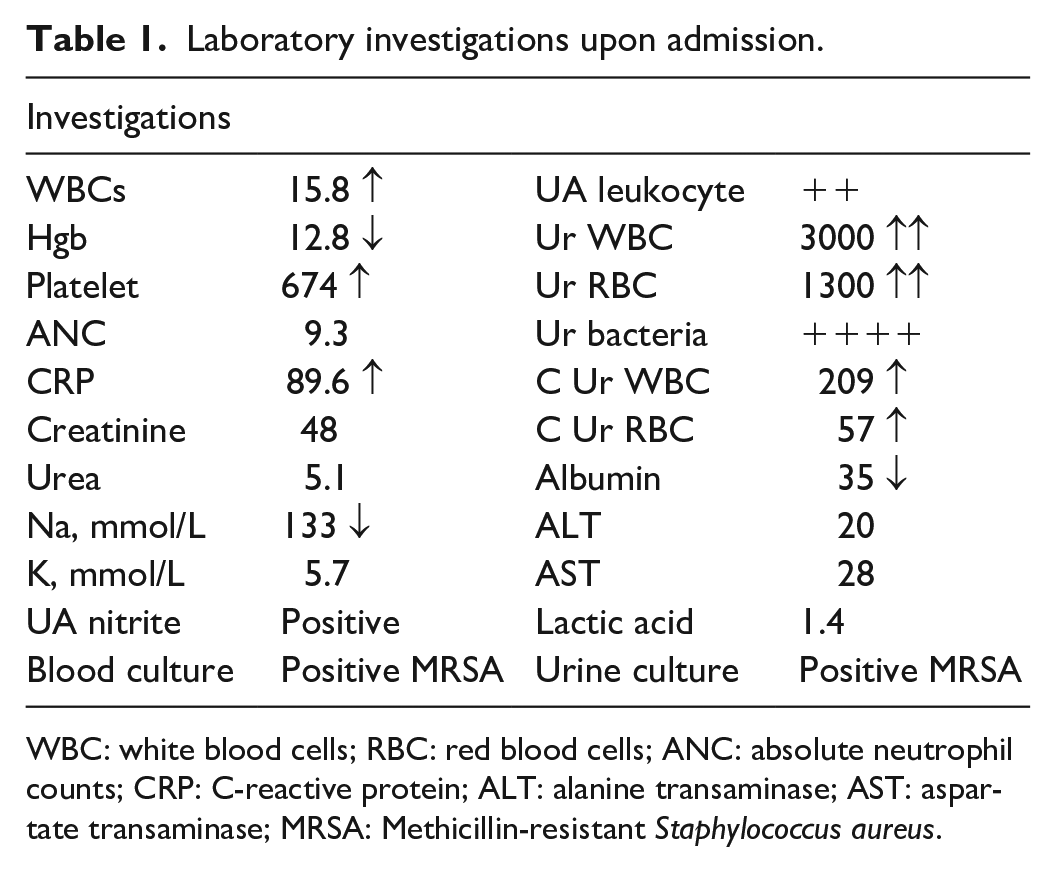
WBC: white blood cells; RBC: red blood cells; ANC: absolute neutrophil counts; CRP: C-reactive protein; ALT: alanine transaminase; AST: aspartate transaminase; MRSA: Methicillin-resistant Staphylococcus aureus.
The baby was discharged on amoxicillin prophylaxis, voiding cystourethrography (VCUG) done after 6 weeks revealed Grade III/IV left vesicoureteral reflux (VUR), and was referred for nephrology follow-up.
Discussion
According to the 2018 Task Force on Circumcision of the American Academy of Pediatrics, the incidence of complications after newborn circumcision is unknown. Thirty-two reports of two large series have reported that the complication rate is somewhere between 0.2% and 0.6%. Most of these complications are minor. Bleeding is a more common complication, which happens in 0.1% of circumcisions. 3 Infection followed by bleeding is the second most frequent complication, but most of these infections are minor and involve only some local redness and purulence.
There are also isolated case reports of different complications, such as wound separation, concealed penis, recurrent phimosis, and inadequate cosmesis, due to urinary retention, excess skin, skin bridges, meatitis, inclusion cysts, retained Plastibell devices, and meatal stenosis.
Circumcision is rarely associated with more severe effects, such as necrotizing fasciitis, meningitis, sepsis, and scalded skin syndrome, as well as with major surgical problems such as amputation of a portion of the glans penis and urethral fistula. In US army hospitals, Wiswell and Geschke 4 reported 193 complications (0.19%) among 100,157 circumcised boys, from 1980 to 1985. These involved 62 cases of balanitis and local infections, 20 cases of UTIs, and 8 cases of bacteremia. Most reported post-circumcision invasive infections were related to the local infection site; however, in our case, the baby did not have any signs of local reaction.
Scurlock and Pemberton 5 documented fulminating neonatal sepsis with meningitis following circumcision in four newborn cases. In each case, there was evidence of an infected circumcision wound. Two of the neonates had Escherichia coli, and two had group A beta-hemolytic streptococci recovered from their CSF.
Similarly, Kirkpatrick and Eitzman 6 published life-threatening infections in two premature newborns after circumcision. One baby had UTI caused by a Proteus species, which led to bacteremia, and the other one was infected with a Staphylococcus species.
Even in the reported cases of UTI and septicemia, the most common organisms were Gram-negative organisms, as was the case with Schwartz et al., 7 who found severe bacterial infection in 87 (19.4%) of 449 febrile neonates, 69 (79%) of whom were male. A total of 13 neonates had bacteremia, 10 UTI, and 2 meningitis. The predominant isolates were E. coli and other Enterobacteriaceae, whereas in our reported case, the isolated micro-organism was Gram-positive MRSA, which is uncommonly isolated with circumcision-related infections.
These reports proposed that the high frequency of severe bacterial infection in male infants was due to circumcision in the early days of life. This procedure may have induced a UTI to grow during the following 1–12 days. 8
Conclusion
Our case highlights one of the possible serious complications post circumcision. However, in specific populations, the benefits of the circumcision procedure outweigh the risks, especially if done by trained health care providers with the proper surgical technique. We encourage the providers to recognize the potential risks and advocate for safe surgical techniques.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This case report received ethical approval from the Medical Research Committee at Hamad Medical Corporation (No. MRC-04-20-080).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article.