
Abstract
Objective
Seroprevalence surveys of healthcare workers for vaccine-preventable diseases, including measles and varicella, are essential for disease prevention and infection control programmes. The purpose of this study was to compare the complement fixation (CF) assay and an enzyme immunoassay (EIA) to determine the prevalence of immunoglobulin G antibodies directed against measles and varicella viruses in healthcare workers
Methods
Antimeasles and antivaricella antibody titres were measured simultaneously in serum samples from healthcare workers employed at a Japanese university hospital, using the CF assay and an EIA.
Results
Serum samples were obtained from 898 healthcare workers. Seropositivity rates determined using the CF assay and EIA were 67.8% versus 94.0%, respectively, for measles, and 83.2% versus 97.6% for varicella. Compared with EIA, a nine- and 22-fold higher number of seronegative subjects was identified by the CF assay for measles and varicella, respectively.
Conclusion
Differences between the CF assay and EIA in detecting seronegative or seropositive healthcare workers for measles and varicella suggest that undertaking a seroprevalence survey using an EIA, rather than a CF assay, would more accurately determine susceptibility to vaccine-preventable diseases, in healthcare settings.
Keywords
Introduction
Measles, mumps, rubella and varicella are viral infections, which are transmitted from an infected person to a susceptible person. Healthcare workers are often exposed to these infections in the clinical setting and so are especially at risk for acquiring these diseases. Maintenance of immunity is therefore essential for disease prevention and successful infection control programmes for such individuals. 1 Immunity against measles, mumps, rubella and varicella is confirmed by laboratory evidence. The complement fixation (CF) assay, haemagglutination inhibition (HI) assay and enzyme immunoassay (EIA, such as an enzyme-linked immunosorbent assay) are commonly used to detect the presence of antibodies against these viruses, although the specificity and sensitivity, as well as cost effectiveness, differs between methods. For example, an EIA is superior in terms of specificity and sensitivity compared with CF and HI assays,2,3 but it is approximately three-fold more expensive. The choice of diagnostic assay is very important because the correct identification of susceptible healthcare workers who should be offered vaccination depends on laboratory results. Despite this, comparisons between CF or HI assays and an EIA in a large series of healthcare workers are lacking. The aim of the present study was to analyse and compare antibody titres against measles and varicella in serum samples from a large series of healthcare workers employed at a Japanese university hospital, using the CF assay and an EIA.
Subjects and methods
Study Population
Healthcare workers employed in any department at Shimane University Hospital, Izumo, Japan during 2005 were recruited into this seroprevalence study, regardless of history of measles or varicella, or documentation of vaccination against these diseases.
This seroprevalence study was undertaken by the Infection Control Committee of Shimane University Hospital in the form of an audit as part of the hospital’s safety and clinical service development, therefore ethical approval was not required. All study participants who undertook screening provided written consent prior to the collection of serum.
Detection of Antiviral Antibodies
Blood samples (8 ml) were obtained from each study participant and centrifuged at 200
Statistical Analyses
All statistical analyses were performed using the SPSS® statistical package, version 18.0 (SPSS Inc., Chicago, IL, USA) for Windows®. Spearman’s rank correlation coefficient was used to investigate the relationship between EIA and CF, and a correlation coefficient was calculated for measles and varicella. Serological data were analysed using the χ2-test.
Results
A total of 898 healthcare workers were included in the study: 219 physicians; 391 nurses; 102 laboratory technicians; 113 administrative staff; 44 teaching staff; 29 graduate students. The study population comprised 299 males and 599 females with a mean ± SD age of 37.81 ± 10.51 years (range 21–65 years).
Antimeasles and antivaricella IgG antibody titres obtained by the CF assay or EIA for 898 healthcare workers are presented in Figure 1. For antimeasles antibodies, the titres obtained by the CF assay were well correlated with those determined by EIA (Spearman’s rank correlation coefficient 0.773, P < 0.001). There were a number of subjects who were seronegative for measles according to the CF assay antibody titres (i.e. titres < × 4) but who were seropositive according to EIA. All those who had CF assay antibody titres ≥ × 4 were also positive as determined by EIA. Similarly, antivaricella antibody titres determined by the CF assay and EIA demonstrated a relatively good correlation (Spearman’s rank correlation coefficient 0.613, P < 0.001), but some subjects identified as being seronegative by the CF assay were seropositive by EIA. All subjects determined to be seropositive according to the CF assay were also seropositive according to EIA results.
Scattergrams showing antimeasles (A) and antivaricella (B) immunoglobulin G antibody titres measured by the complement fixation (CF) assay and an enzyme immunoassay (EIA), using serum samples from healthcare workers (n = 898) employed at a Japanese university hospital. Spearman’s rank correlation coefficients for antimeasles or antivaricella antibody titres were 0.773 and 0.613, respectively (P < 0.001 for both comparisons).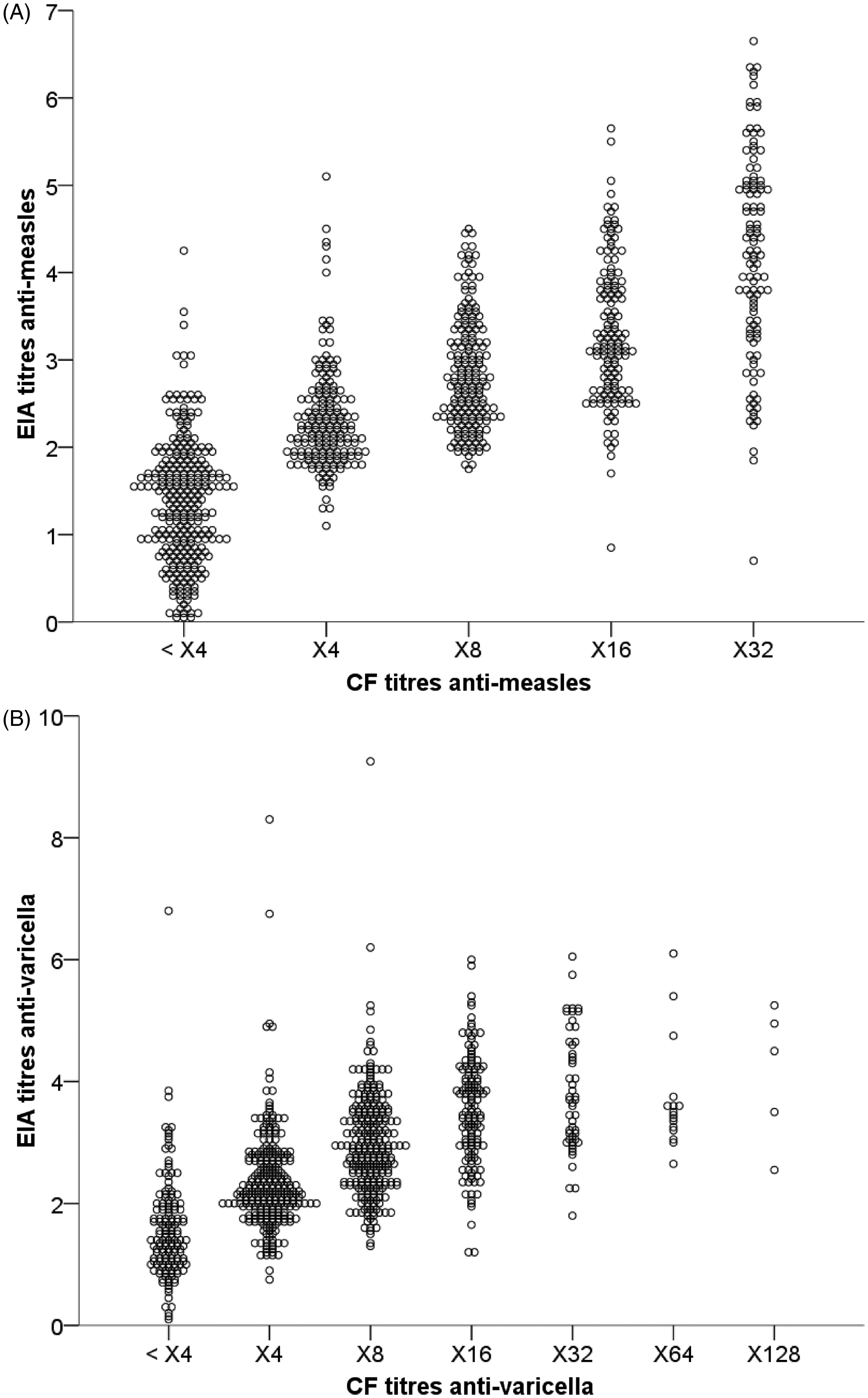
Serological results for antimeasles and antivaricella immunoglobulin G antibody titres, measured by the complement fixation (CF) assay and an enzyme immunoassay (EIA), using serum samples from healthcare workers (n = 898) employed at a Japanese university hospital.

CF seropositive, ≥ × 4; CF seronegative, antibody titres of < × 4.
EIA, quantitative cut-off values for seronegative antibody titres, <0.5 for measles and <0.6 for varicella; EIA equivocal, antibody titres of 0.5–0.7 and 0.6–0.9 for measles and varicella, respectively; EIA seropositive cut-off antibody titres, >0.7 for measles and >0.9 for varicella.
For antivaricella IgG antibodies, similar proportions of seropositive subjects were detected by both assays (Table 1). The EIA identified a smaller proportion of subjects who were seronegative for antivaricella IgG antibodies compared with the CF assay (χ2 101.5, P < 0.001), indicating a 22-fold difference between the two methods. Among 151 seronegative subjects for varicella detected by the CF assay, 130 subjects (86.1%) were identified as being seropositive by EIA. None of the seropositive subjects for varicella detected by the CF assay were identified as being seronegative with EIA, and none of the seronegative subjects with EIA were determined to be seropositive by the CF assay.
Discussion
The reporting system for the surveillance of infectious disease in Japan (via approximately 3000 sentinel clinics and hospitals for paediatrics and 450 clinics for adults) showed that measles outbreaks occurred consistently each year during 1999–2003. 4 The largest outbreak occurred in 2001, with most affected patients not being vaccinated; this led to a nationwide vaccination campaign. 4 Despite this campaign, measles outbreaks have continued to occur in Japan.4–7 A considerable number of paediatric varicella cases are also reported annually in Japan; numbers of 200000–300000 per year have been reported from ∼3000 paediatric facilities. 8 Vaccination against varicella is optional in Japan for children >1 year of age and documented vaccination rates are only 21.3%. 9 Given these observations, prevention and infection control programmes for measles and varicella are of importance in Japan, not only in the community but also in healthcare settings.
A large difference between the CF assay and EIA in terms of their ability to identify healthcare workers who were seronegative or seropositive for antimeasles or antivaricella IgG antibodies was demonstrated in the present study. The CF assay identified a nine- and 22-fold larger number of seronegative subjects for measles and varicella, respectively, than EIA. It is recommended that these seronegative healthcare workers should receive vaccination against measles and varicella, in order to limit hospital infection in healthcare settings. These results highlight the importance of accurate determination of seroprevalence. Previously published data indicate that use of an EIA may be more suitable for distinguishing between seronegative and seropositive healthcare workers as it is superior to the CF assay in terms of sensitivity and specificity.2,3 The results of the present study are consistent with these reports, and provide further data that might be useful in the determination of a better assay for measuring the seroprevalence of measles and varicella in healthcare workers.
The antibody threshold, which provides protection from viral infection, remains unclear in EIAs. Despite the standard protective threshold of rubella antibody being known,10,11 those for measles and varicella in EIAs are not well defined. Chen et al. 12 demonstrated that eight of nine college students with antibody titres <1:120 (<120 mIU/ml) immediately preceding a measles outbreak developed the disease, compared with none of 71 students with antibody titres ≥1:120. Another study that examined the protective threshold of measles neutralizing antibody among a retrospective cohort of patients in Taiwan used a neutralization EIA to detect the growth of a wild-type measles virus in Vero cells, and suggested that neutralizing titres >1000 mIU/ml may prevent measles infection. 13 It is not, however, clear from these studies how the previously defined antibody titres correspond to the levels measured by each commercially-available EIA.12,13 The quantitative cut-off value differs with each EIA kit. EIA is used in most healthcare settings and so it is of clinical importance to undertake further evaluations of the antibody thresholds that provide protection from measles and varicella, as well as to standardize EIA thresholds.
Seroprevalence surveys have important implications for the management of vaccine programmes for healthcare workers. A reliable assay for the accurate identification of the immune status of healthcare workers is required, such that those individuals who are seronegative for disease can be offered vaccination. Increased vaccination rates may, in turn, contribute to a reduction in disease transmission in healthcare settings and improved patient safety. Results from the present study suggest that using an EIA for analysis of seroprevalence in surveys of healthcare workers may more accurately determine susceptibility to vaccine-preventable diseases in healthcare settings, compared with using the CF assay.
Footnotes
Declaration of Conflicting Interest
The authors declare that there are no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.