
Abstract
A recent publication in JCBFM, “Static autoregulation in humans” gives rise to critical comments. Autoregulation of cerebral blood flow implies that flow is rather constant within a certain blood pressure (BP) range with a lower and an upper pressure limit. The physiology at the two limits is very different, making comparison of the brain’s vulnerability at the limits questionable. The recent publication in JCBFM claims a narrow autoregulatory range based on pooling of data from several studies. However, we argue that such pooling blurs the autoregulatory limits. We summarize the classical literature, therefrom we argue for a broad autoregulatory range.
Keywords
Introduction
The article by Wang and Payne raises important yet questionable issues, worth considering further. 1 Autoregulation denotes that cerebral blood flow (CBF) remains essentially constant independent of fluctuations of mean arterial blood pressure (MABP) within a certain range of BP. There are limits of the autoregulatory range: when pressure falls below the lower limit flow decreases, and above the upper limit it increases.
The slope at the limits of autoregulation
Wang and Payne found that the slope of CBF/MABP was steeper at the lower range of autoregulation as compared to the upper range, and considered this as an indication of a more effective autoregulation and protection of the brain at the upper range. But the physiology at the upper and lower limits are very different.
Below the lower limit physiology is rather simple. When BP falls moderately below the lower limit an increased extraction of oxygen from the blood keeps brain function intact. If BP falls further then the oxygen supply to the brain becomes insufficient, and fainting can occur. Simple fainting is rather harmless as BP is rapidly restored and normal brain function recovered. When resistance vessels are maximally dilated, flow becomes passively proportional to pressure. In this situation it seems biologically advantageous to have a low lower limit of the autoregulation corresponding to a steep CBF/MABP relation (Figure 1). The hazard for the brain below the lower limit of autoregulation is if BP remains critically low for a critical time period, potentially resulting in irreversible brain damage.
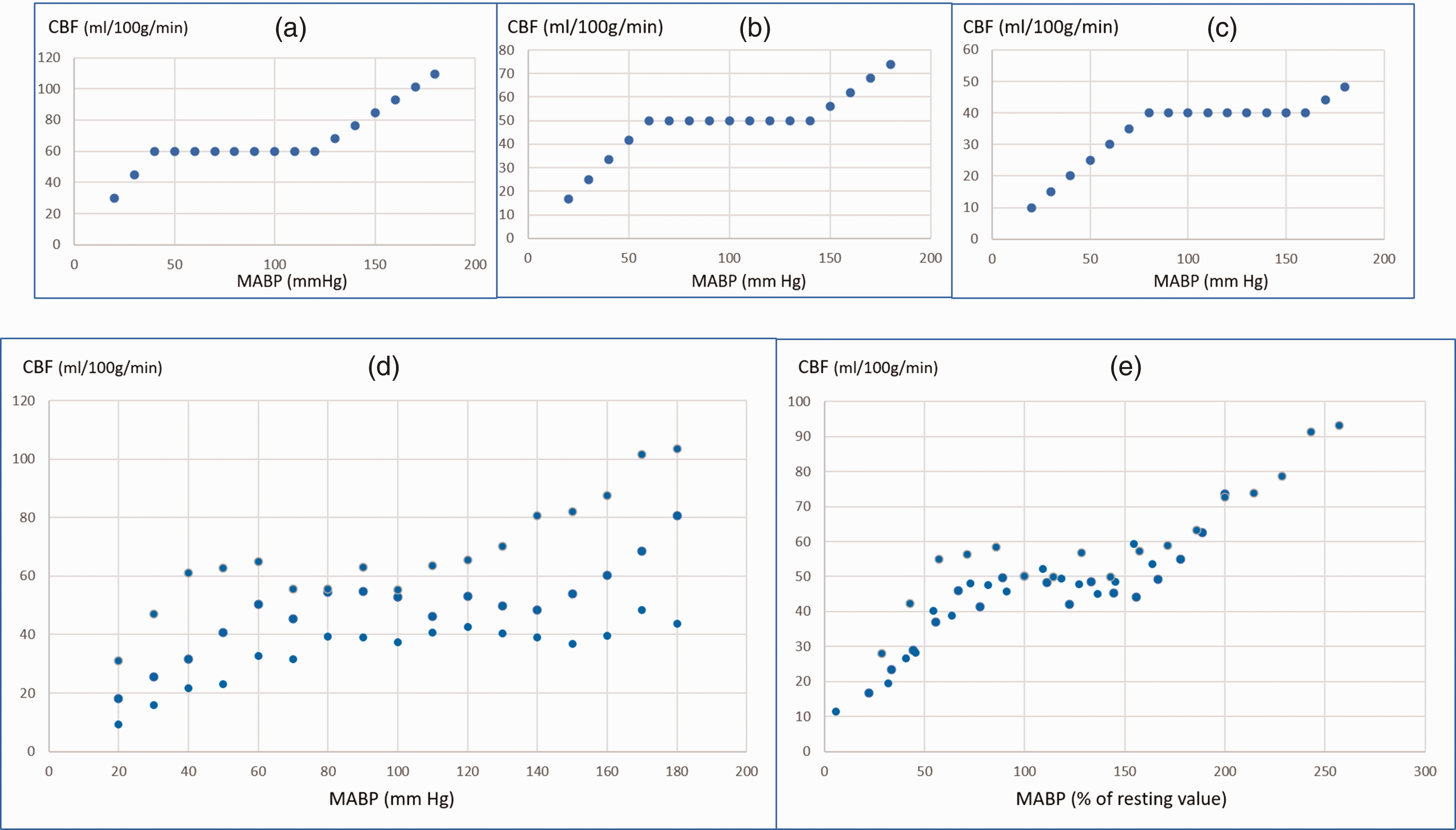
The slope of the CBF/blood pressure relation below the lower limit of autoregulation. (a) Low blood pressure, (b) normal blood pressure and (c) higher lower limit of CBF autoregulation. The low limit corresponds to a steeper CBF/blood pressure slope. Normalised to resting CBF 100%: A-slope: 2,50, B-slope: 1,67 and C-slope: 1,25%CBF/MABP.
At and above the upper limit the physiology is quite different. When BP exceeds the upper limit forceful dilatation of parts of the resistance vessels occurs accompanied by flow increase and vessel wall damage, see review.2,3 Thus, the primary pathology in this situation is brain vessel damage which may lead to oedema and brain damage. Here a preserved or partly preserved autoregulation with a low CBF/MABP slope would be advantageous.
These very different physiology and risks below the lower and above the upper limits of autoregulation make comparison of the extent of brain protection at the two borders essentially impossible.
Plotting the range of autoregulation
Wang and Payne in their article plotted all CBF/MABP values from many studies in a diagram, their figure 6, and used this to estimate the range of intact autoregulation. 1 But one has to take into account that the resting BP varies between individuals and so do the limits of autoregulation. Thus, the limits would be higher if the resting BP is higher and vice versa in individuals with lower resting BP. Furthermore, different individuals have somewhat different resting state CBF. Plotting all individuals high and low resting BP and high and low CBF together would result in scatter blurring the relation between the CBF and the BP and thereby the limits of autoregulation. This drawback could be circumvented by normalising all BP and CBF values to the resting state values, e.g., resting state BP = 100% and resting CBF 50 ml/100 g/min. This would result in a much more precise delineation of the BP-CBF relationship as illustrated in the simulations shown in Figure 1.
Might other factors contribute to the discrepancy between Wang and Payne’s and the classical autoregulatory studies? This point is discussed in the supplementary material.
The classical concept and studies of autoregulation
Classical studies show a broad autoregulatory range both across subjects and in the single individual. Eleven such studies are commented on in the supplementary material. These 11 studies comprise 6 groups of normal subjects, 3 groups of hypertensive patients and 6 groups of patients with minor cerebral diseases. For space limitation only 7 of these studies are mentioned her, but all are in the supplementary material.4 –10 Note that in one of the studies, both lower and upper limits of autoregulation were reached in one normal subject and 3 hypertensive patients and the average autoregulatory range was 65 and 60 mmHg, respectively. 5 Otherwise, each study is detailed in the supplementary material.
It is remarkable that Wang and Payne in their study 1 included only one of these 11 studies, the Jobes and coworkers study, 6 and further that the inclusion was partial and biased. Thus, Jobes and coworkers measured in the single individual CBF in the resting state and subsequently in random order during decreased or increased BP and then increased or decreased BP. The average range of BP was 60 mmHg, and the average CBF was: low BP 44.0, normal BP 38.9 and high BP 49.5 ml/100 g/min. PaCO2 was stable. The low CBF in the resting state remains an unexplained variation. Wang and Payne reported the rest-high BP part, but omitted the low BP-rest part. Further we would like to point out that in their Table 1 Wang and Payne report CBF/BP slopes (%/% and %/mmHg) as numeric values, omitting ± signs.
Concluding remarks
Here we argue against Wang and Payne’s opinion and conclude that: 1) The best protection of the brain below the lower limit of the autoregulatory range seems to be reflected in a low lower limit of autoregulation corresponding to a steep slope of the CBF/BP relation. Above the upper limit a strong vasomotor control corresponding to a low slope of the CBF/BP relation seems advantageous. 2) Merging together the data from several studies of CBF autoregulation carries the risk of blurring the autoregulatory limits, especially if the data are not normalized with regards to the subject’s resting state BP and baseline CBF (Wang and Payne did not normalize); 3) Taking all factors into consideration, the classical studies of CBF autoregulation revealing a wide range of the autoregulatory plateau still remain hard to challenge.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X241258701 - Supplemental material for Static autoregulation in humans
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X241258701 for Static autoregulation in humans by Olaf B Paulson, Svend Strandgaard, Jes Olesen and Jean-Claude Baron: on behalf of INSPIRE study group in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplementary material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.