
Abstract
The ischemic penumbra is sensitive to alterations in cerebral perfusion. A myriad of drugs are used in acute ischemic stroke (AIS) management, yet their impact on cerebral hemodynamics is poorly understood. As part of the Cerebral Autoregulation Network led INFOMATAS project (Identifying New Targets for Management and Therapy in Acute Stroke), this paper reviews some of the most common drugs a patient with AIS will come across and their potential influence on cerebral hemodynamics with a particular focus being on cerebral autoregulation (CA). We first discuss how compounds that promote clot lysis and prevent clot formation could potentially impact cerebral hemodynamics, before focusing on how the different classes of antihypertensive drugs can influence cerebral hemodynamics. We discuss the different properties of each drug and their potential impact on cerebral perfusion and CA. With emerging interest in CA status of AIS patients, either during or soon after treatment when timely reperfusion and salvageable tissue is at its most critical, the properties of these pharmacological agents may be relevant for modelling cerebral perfusion accuracy and for setting individualised treatment strategies.
Introduction
A broad spectrum of highly selective pharmacological agents are used in acute ischemic stroke (AIS) treatment and management, where restoring and maintaining adequate cerebral blood flow (CBF) are paramount for a successful intervention. However, the specific effects of the applied drugs on the cerebral hemodynamics in the acute stroke condition are largely overlooked in both research and clinical settings. It also remains unclear which cerebral hemodynamic parameters are related to stroke patient outcome due to the lack of data from large clinical trials and the effects of these pharmacological agents on CBF are rarely reviewed, making future individualised treatment strategy in patients who suffer an AIS difficult.
Despite the technical difficulty in measuring CBF, considerable developments were made early last century in understanding the efficacy and metabolic effects of a variety of compounds on the cerebral vasculature. 1 It was apparent that regardless of the vasoactive compounds that were administered, CBF is relatively conserved through the combination of pressoreceptor reflexes that regulate BP and changes in local cerebrovascular resistance. 1 Cerebral autoregulation (CA) is the ability of the cerebral circulation to maintain constant CBF over a wide range of blood pressures (BP) through intrinsic humoral, neurogenic and myogenic control. 2 , 3 Currently, there has been more of a focus on the dynamic beat-to-beat components of the BP-CBF relationship (i.e., changes that occur 4–5 s to 5 min), termed dynamic CA (dCA). In a recent study, Hecht et al. 4 assessed cortical perfusion in patients with large hemispheric infarctions undergoing hemicraniectomy and found ipsilateral dCA was impaired. They found the severity of dCA impairment was inversely linked to the degree of cortical perfusion, with the greatest dCA impairment observed in the hypoperfused but potentially viable brain regions (i.e., penumbra). Petersen et al. 5 also recently highlighted the importance of managing BP during the acute stages of stroke treatment, as they demonstrated the feasibility of monitoring the autoregulation status for up to 48 hours after endovascular thrombectomy. This study showed that the time patients spent outside their personalized limits of autoregulation were associated with 90-day outcomes and that haemorrhagic transformation was associated with the time above the upper limit of autoregulation, rather than systolic BP thresholds. Thus, considerations have to be made when vasoactive drugs and BP management are used to maintain a stable perfusion in the ischemic penumbra or in avoiding excessive hyperperfusion to achieve an improved clinical outcome.
The Cerebral Autoregulation Network (CARNET, www.car-net.org) was initiated in 2011 to foster collaboration between clinicians and researchers to prioritise dCA research. INFOMATAS was launched in 2016 with the overarching goal to enhance our understanding of basic stroke pathophysiology and to identify new targets and strategies for improving BP management in AIS patients. 6 It needs to be established how and if drug treatment can improve or deteriorate the cerebral autoregulatory response and whether such treatment strategies are of clinical relevance7–9 and can be used in clinical practice to prevent progression of chronic damage to the brain. This review provides a critical reappraisal on the effects of pharmacological interventions on CBF and its regulation in the context of ischemic stroke, drawing upon some research on healthy and on those with vascular risk factors. With there being few studies available within each section both acute and chronic treatment strategies are discussed, where due to inter-species differences, we also focus on human studies and when possible systematic reviews as primary source of information.
Studies in CA with pharmacological interventions in patients with ischemic stroke
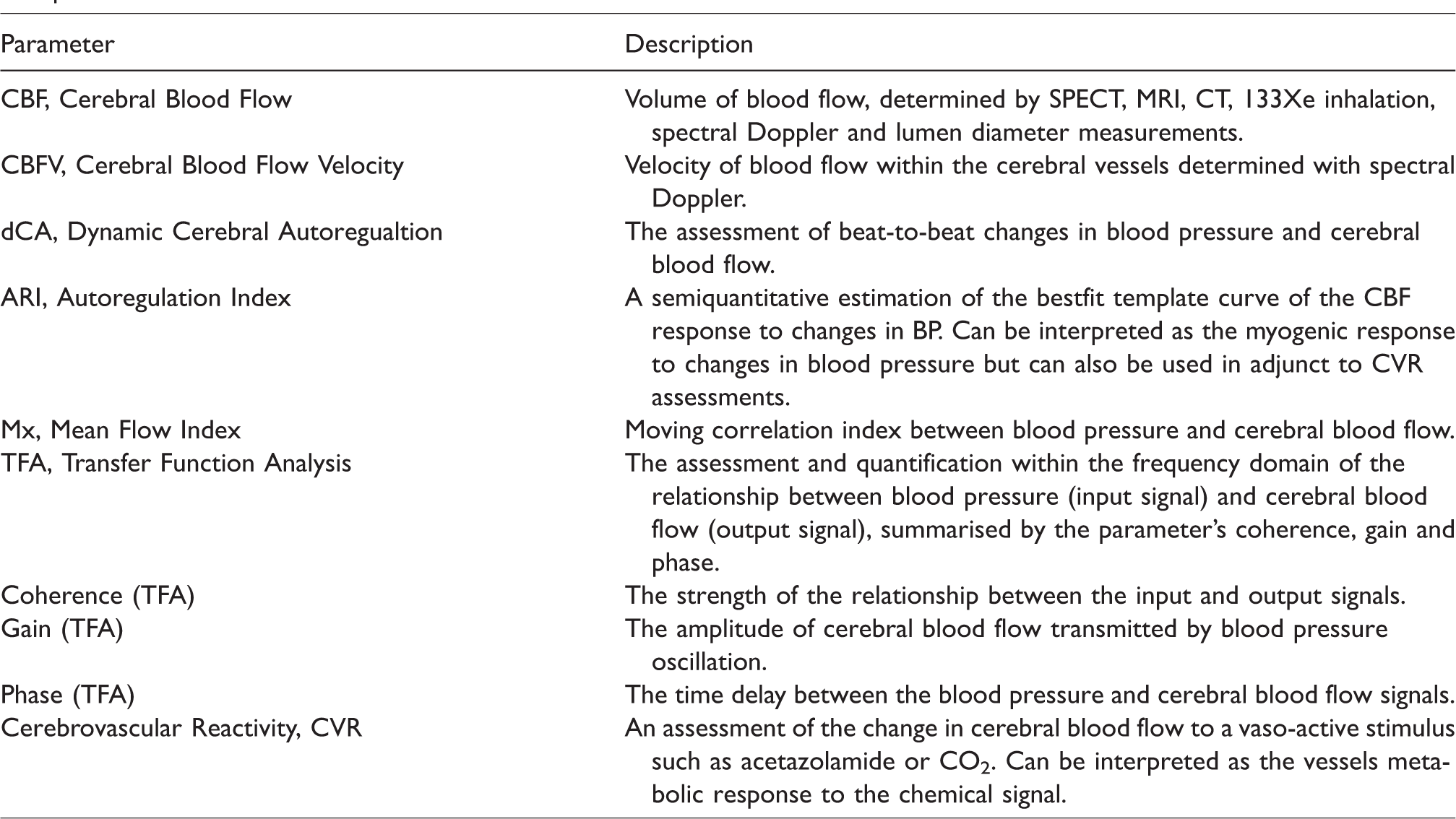
Restoring CBF is paramount for successful intervention in acute stroke and a range of pharmacological agents are used to maintain haemostatic balance and improve blood flow to distal vascular beds. As the post-ischemic pathophysiology and its acute treatment and management are complex, defining and quantifying the contribution that each pharmacological intervention might have on cerebral hemodynamics has proven difficult. Due to the nature of the research and the methodologies needed to assess each physiological parameter (see Table 1), clinical studies that have focused on CA are inherently small in numbers, observational or non-randomized data (see Tables 2 and 3). Thus, studies in healthy individuals and patients with risk factors for cardiovascular disease have been included to provide a better overview and understanding of each pharmacological agent and treatment strategy. Over the years dCA has been quantified and described by several parameters 10 such as the use of transfer function analysis to determine the different frequencies and amplitudes between the BP and CBF oscillations (phase, gain, coherence), autoregulation index (ARI) or mean flow index (Mx). For ease of reference, all parameters used to assess CA capacity are referred to in the text as dCA and are defined further within brackets and in Tables 1 to 3. The tables also highlight the methods used to measure CBF, or if cerebrovascular reactivity (CVR), where changes to cerebral blood flow are monitored in response to a stimulus such as CO2, has been used. Before reviewing antihypertensive drugs, we first briefly review fibrinolytics, antithrombotics and lipid-lowering agents that are given to AIS patients.
A list of some the cerebral blood flow and cerebrovascular function abbreviations used within the text and their interpretation.
Summary of clinical studies in ischemic stroke investigating the effect of fibrinolytics, antithrombotics and statins on systemic and cerebral hemodynamics.
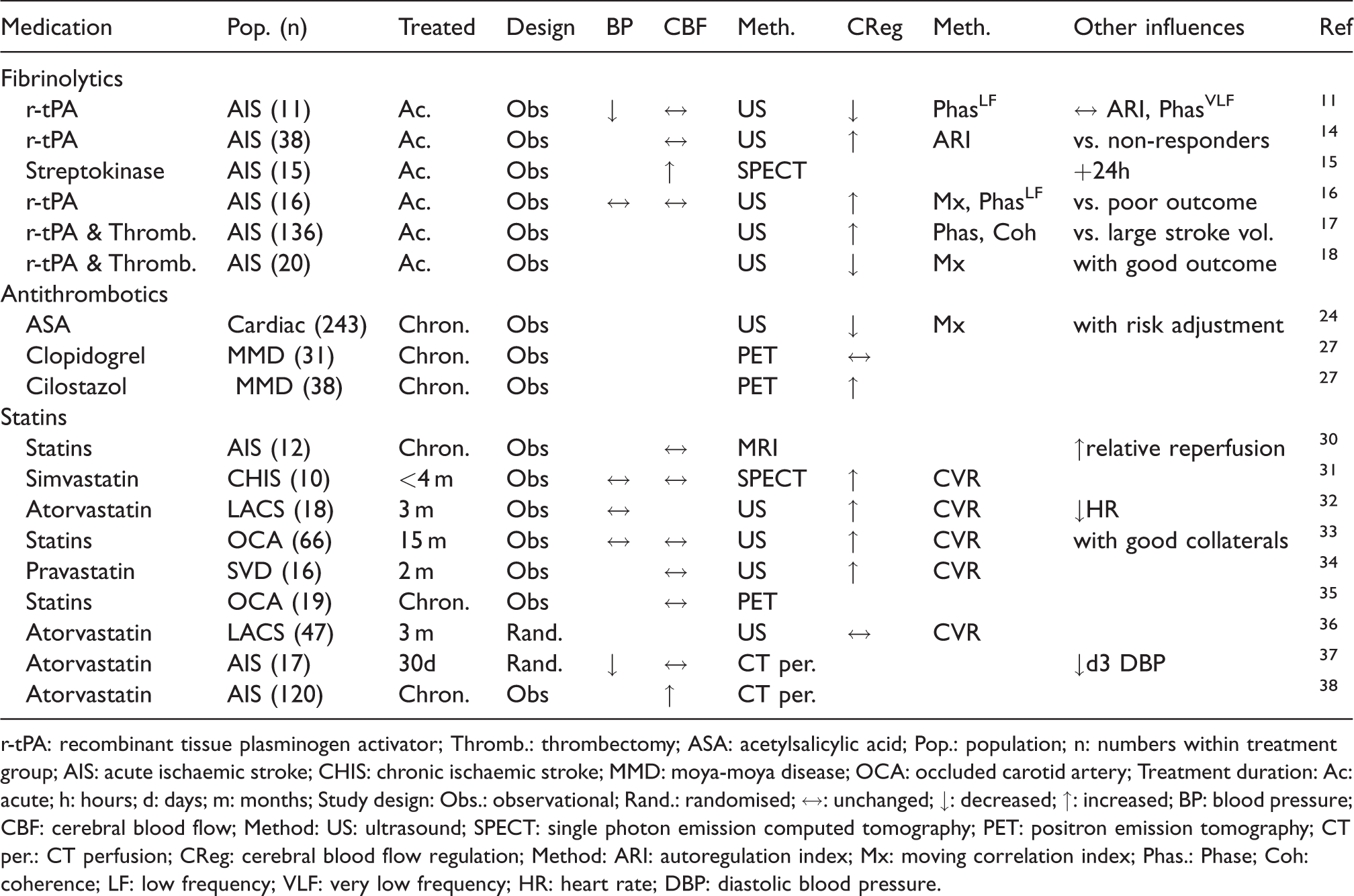
r-tPA: recombinant tissue plasminogen activator; Thromb.: thrombectomy; ASA: acetylsalicylic acid; Pop.: population; n: numbers within treatment group; AIS: acute ischemic stroke; CHIS: chronic ischemic stroke; MMD: moya-moya disease; OCA: occluded carotid artery; Treatment duration: Ac: acute; h: hours; d: days; m: months; Study design: Obs.: observational; Rand.: randomised; ↔: unchanged; ↓: decreased; ↑: increased; BP: blood pressure; CBF: cerebral blood flow; Method: US: ultrasound; SPECT: single photon emission computed tomography; PET: positron emission tomography; CT per.: CT perfusion; CReg: cerebral blood flow regulation; Method: ARI: autoregulation index; Mx: moving correlation index; Phas.: Phase; Coh: coherence; LF: low frequency; VLF: very low frequency; HR: heart rate; DBP: diastolic blood pressure.
Summary of clinical studies in ischemic stroke investigating the effect of antihypertensive drugs on systemic and cerebral hemodynamics.
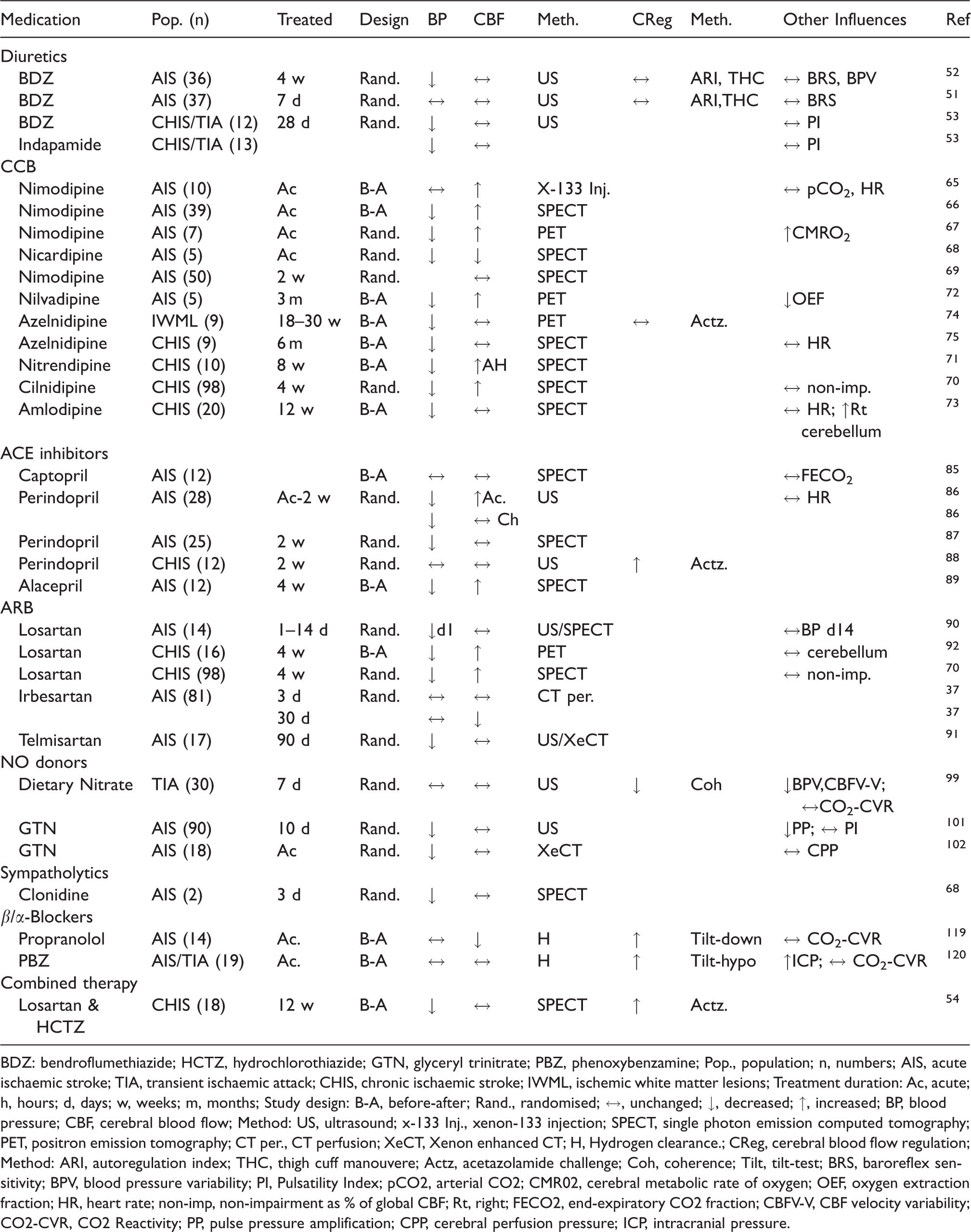
BDZ: bendroflumethiazide; HCTZ, hydrochlorothiazide; GTN, glyceryl trinitrate; PBZ, phenoxybenzamine; Pop., population; n, numbers; AIS, acute ischemic stroke; TIA, transient ischemic attack; CHIS, chronic ischemic stroke; IWML, ischemic white matter lesions; Treatment duration: Ac, acute; h, hours; d, days; w, weeks; m, months; Study design: B-A, before-after; Rand., randomised; ↔, unchanged; ↓, decreased; ↑, increased; BP, blood pressure; CBF, cerebral blood flow; Method: US, ultrasound; x-133 Inj., xenon-133 injection; SPECT, single photon emission computed tomography; PET, positron emission tomography; CT per., CT perfusion; XeCT, Xenon enhanced CT; H, Hydrogen clearance.; CReg, cerebral blood flow regulation; Method: ARI, autoregulation index; THC, thigh cuff manouvere; Actz, acetazolamide challenge; Coh, coherence; Tilt, tilt-test; BRS, baroreflex sensitivity; BPV, blood pressure variability; PI, Pulsatility Index; pCO2, arterial CO2; CMR02, cerebral metabolic rate of oxygen; OEF, oxygen extraction fraction; HR, heart rate; non-imp, non-impairment as % of global CBF; Rt, right; FECO2, end-expiratory CO2 fraction; CBFV-V, CBF velocity variability; CO2-CVR, CO2 Reactivity; PP, pulse pressure amplification; CPP, cerebral perfusion pressure; ICP, intracranial pressure.
Fibrinolytics
Fibrinolytic agents such as, recombinant tissue plasminogen activator (r-tPA) is one of the first drugs used in acute AIS management. It is a protein involved in the fibrinolysis and the breakdown of blood clots made of polymerized fibrin and platelets. The half-life of fibrinolytic enzymes such as alteplase, tenecteplase and streptokinase last no longer than 5–18 minutes, respectively. While the benefits of early intervention with r-tPA on arterial recanalization is well-established, the acute effects of thrombolysis on cerebral hemodynamics are less well-categorised. In a small cohort of 11 stroke patients, Lam et al. 11 examined the effect of r-tPA infusion on dCA and found during treatment a reduced dCA (phase) within the affected hemisphere in some parameters, while cerebral blood flow velocity (CBFV) remained unchanged. Also noted was a drop in BP immediately before completion of r-tPA infusion, which could have been attributed to factors such as recovery from pain, but does mimic earlier findings in studies investigating streptokinase infusion in patients with myocardial infarction 12 and pulmonary embolism. 13 Similarly, Nogueira et al. 14 observed poorer dCA (ARI) status and CBFV during thrombolysis treatment in non-responder patients to reperfusion treatment compared to responders (based on >4 points improvement in NIH Stroke Scale Score, NIHSS, 24 hours after thrombolysis). Nevertheless, whilst the studies by Lam et al. and Nogueira et al. did not report further differences in CBFV or dCA after 24 hours of treatment, earlier studies had reported cases of hyperperfusion in stroke patients 24 hours after streptokinase treatment. 15 Whilst Reinhard et al. 16 reported unchanged autoregulation status (Mx, phase) 12–24 hours after stroke onset when thrombolysis treatment was successful, a more favourable autoregulation status (phase, coherence) has recently been reported in AIS patients with complete recanalization of large vessel occlusions and who had smaller stroke volume. 17 However, Meyer et al. 18 has demonstrated that dCA (Mx) can still be impaired directly postintervention after successful recanalization of large vessels with intravenous thrombolysis and thrombectomy.
To summarise, with the direct effect of plasminogen activators on vascular tone 19 being limited to animal studies to date, the general profile of the effects of fibrinolytics on cerebral hemodynamics and CA is difficult to characterize without the confounder of stroke, the interaction of risk factors, comorbidities and/or comedication and the difficulty of including suitable controls into the studies. Even data from the contralateral hemisphere provide limited information on the effects of the fibrinolytics due to the collateral circulation. It remains unclear whether reperfusion can be achieved with fibrinolytic agents without compromising autoregulation status.
Antithrombotics
Preventing blood clot formation with antithrombotic therapy is a key treatment strategy for secondary stroke prevention. A variety of drugs is used for this purpose. For cardioembolic stroke, or if the patient is deemed to have a hypercoagulable state, anticoagulants (blood thinners) such as heparin, warfarin or apixaban can be used to limit the body’s coagulation system and blood clotting capability. For all other ischemic strokes, the prostaglandin and thromboxane inhibitor acetylsalicylic acid (ASA), or the adenosine diphosphate receptor P2Y12 inhibitors (clopidogrel, prasugrel, ticagrelor, cilostazol, dipyridamole etc) are used to limit platelet activation and aggregation.
There is insufficient data on whether anticoagulants provide additional benefit to the cerebrovascular system other than maintaining patency of a vessel. Although prostaglandins 20 and thromboxane 21 have been shown to elicit vasodilator and vasoconstrictor effects, oral administration of ASA does not significantly influence the cerebrovasculature. 22 , 23 There is one observational study 24 in patients undergoing cardiopulmonary bypass, in which post-operative stroke and impaired CA (Mx) were independently associated with higher CBFV and preoperative aspirin use, but such an association could be related to a predisposition to vascular disease rather than an altered state of prostaglandin synthesis. In a small cohort of healthy individuals, 25 cilostazol administered orally dilated large cerebral arteries, reduced diastolic BP and CBFV, without affecting total regional CBF. Dipyridamole increases interstitial fluid adenosine and when administered intravenously in healthy individuals it may trigger a decrease in CBF. 26 It was also noted in nonsurgical patients with Moya-Moya disease that two years of treatment with clopidogrel did not affect CBF, whilst cilostazol did promote a significant improvement in CBF. 27 Thus, antithrombotics augment clot lysis and may affect endothelial function, but does not appear to alter cerebrovascular function in neither healthy individuals nor patient cohorts.
Statins
Statins are a class of β-hydroxy-β-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors that inhibit cholesterol biosynthesis, thereby lowering the blood’s cholesterol levels and slowing atherosclerotic plaque progression. In addition to its cholesterol-lowering effect, statins upregulate endothelial NO synthase (eNOS) expression and activity, stabilise atherosclerotic plaques, decrease oxidative stress and inflammation, and inhibit the thrombogenic response. 28 The effects of statins on cerebral hemodynamics and CA in human studies has previously been reviewed and summarised by Giannopoulos et al. 29 Chronic statin therapy improved cerebrovascular function in eight out of ten clinical studies. For studies in patients with cerebrovascular disease there was one study with improvement in CBF 30 and four studies that demonstrated improvements in CVR,31–34 whilst some did not improve CBF 35 or CVR. 36 Interestingly, the cerebrovascular effects of statin appeared to be greater in patients who likely have impaired vasomotor reactivity. Since eNOS plays a crucial role in mediating the cerebrovascular response to perfusion pressure and CO2, the upregulation of eNOS activity with statins likely account for these improvements in cerebrovascular function. A more recent study by Beer et al. 37 has also found no difference in CBF between AIS patients treated for 30 days with atorvastatin or a placebo. However, Pretnar-Oblak et al. 32 reported a CBFV increase in patients with small vessel disease after 3 months of statin therapy. A recent study that investigated long term statin use in patients with symptomatic intracranial arterial atherosclerotic stenosis, also noted that CBF and cerebral blood volume were elevated with atorvastatin treatment, with the highest dosage also demonstrating less cerebrovascular events such as TIA or cerebral infarct. 38 Consequently, due to their direct effects on eNOS activity, it is difficult to extricate the effect of statins on cerebrovascular function per se. As a result, optiminal statin and thrombolysis treatment strategy remains elusive. 39
Antihypertensive medications
Antihypertensive agents typically lower BP by: 1) reducing heart rate (HR) and/or stroke volume (β-adrenoreceptor blocker, BB); 2) reducing the circulating blood volume (diuretics, mineralocorticoid-antagonist); 3) reducing arterial wall stiffness/tone (Ca2+ channel-blockers, CCB; NO donating drugs); 4) inhibition of the renin-angiotensin-aldosterone system (RAAS) with Angiotensin Receptor blockers (ARB), and angiotensin-converting enzyme inhibitors (ACEI). There are some antihypertensive agents which inhibit central autonomic outflow, such as clonidine, an α2-adrenoreceptor agonist that decreases the release of noradrenaline from the sympathetic nerve terminals. An overview of the action of these antihypertensive medicines on various physiological variables in patients with ischemic stroke is provided in Table 3.
Studies, where treated hypertensive patients were compared with untreated patients, demonstrated that although there is often no difference in CA 40 or CVR, the transmissions of blood pressure oscillations to CBF (gain) is attenuated in hypertensives in comparison to healthy individuals. 7 A systematic review by Sare et al. 41 in 2008 revealed that administration of antihypertensive agents within 7 days of AIS did not alter CBF in randomised controlled trials (RCT), whereas nonrandomized trials did see increases in CBF with CCB. A later Meta-analysis by Webb 42 of controlled trials that compared the effects of vasodilators with non-vasodilating treatments also highlighted the little changes to CBF with the lowering of BP, but that there may be an improvement in CVR and pulsatility index, where the hemodynamics are less pulsatile. These together with some of the studies that investigated the effects of CBF and CA in healthy, diseased and patients with ischemic stroke, concerning their drug classifications, are discussed below.
Diuretics
The precise mechanism for diuretics such as thiazides to lower blood pressure remains elusive (recently reviewed by Rapoport 43 ) but diuretic treatment is an effective antihypertensive strategy that reduces BP via renal excretion of salts and water. The three types of diuretics (thiazide, loop, potassium-sparing) will each target a different site of the kidney to reduce blood volume and reduce blood pressure. Loop diuretics (bumetanide, furosemide, torsemide, ethacrynic acid) are commonly used to treat heart failure, whereas thiazides (bendroflumethiazide, chlorthalidone, hydrochlorothiazide, indapamide, metolazone) that can be combined with other drug treatments are predominantly used for stroke patients, together with potassium-sparing diuretics (amiloride, eplerenone, triamterene).
In healthy cohorts, studies have found a single dose of furosemide to preserve cerebral perfusion (reduced CBFV but increased coherence between BP and CBFV) when challenged with stressors of orthostasis and dehydration 44 or to improve CA (gain, coherence) when there is a mildly induced central hypovolemia. 45 In hypertensive patients, chronic monotherapy with hydrochlorothiazide also prompted no change to CBF or cerebrovascular resistance when no carotid artery stenosis was present; when it was present, cerebrovascular resistance decreased and CBF ipsilateral to the stenosis improved. 46 , 47 However, a study in hypertensive patients with executive mild cognitive impairment 48 demonstrated that hydrochlorothiazide monotherapy impaired CO2 vasomotor range (absolute difference in hypercapnia and hypocapnia CBFV). When hydrochlorothiazide is part of a combination of hypertensive medications CBFV increased and CVR remained unchanged. 49 , 50
Few studies have investigated the effects of diuretics on the cerebral hemodynamics of AIS patients. Monotherapy with bendroflumethiazide or indapamide for up to 28 days did not alter CBF, dCA, or baroreceptor sensitivity (BRS).51–53 When hypertensive patients resistant to losartan (ARB) and who had CVR impairment (due to steno-occlusive disease in either MCA or ICA) were treated with a combination of losartan and HCTZ for 12 weeks, there were improvements in the affected hemisphere in CVR, without any changes to CBF. 54 Collectively, these studies indicate the transient improvement in CA with diuretic monotherapy is not observed in in AIS, and remains absent following 7 days of treatment or more in patients with risk factors. Chronic diuretic treatment does not appear to affect CA, and the possible benefits of diuretics in combination with other hypertensives such as ARB warrant further investigations.
Calcium channel blockers
Calcium channels regulate calcium ions (Ca2+) that enters cells within the heart and the vascular system and play a vital role in maintaining the heart and vessels contractility and myogenic tone. By reducing the amount of Ca2+ entering cells, CCB promotes vasodilation in the systemic and cerebral circulations, and within the heart, promote negative inotropy (myocardial force), negative chronotropy (heart rate) and negative dromotropy (conduction speed). The two different classes of CCB include dihydropyridines (amlodipine, lacidipine, nifedipine, nimodipine) that are used as antihypertensives by reducing systemic vascular resistance and non-dihydropyridines (diltiazem, verapamil etc) that are used in managing cardiac arrhythmias. The new generation of dihydropyridines such as amlodipine, barnidipine, cilnidipine and azelnidipine are better tolerated and do not have the baroreflex activation associated with first (nifedipine, nicardipine) and second-generation (benidipine, nimodipine) CCB. 55
In healthy individuals, CBF has been reported to remain stable 56 or increase 57 after acute nifedipine treatment. There are studies that also demonstrated an increase in cerebral oxygenation 58 whilst CVR was impaired. 56 , 59 Acute treatment with first-generation CCB such as nifedipine can promote a reflex stimulation of cardiac sympathetic activity after quickly lowering BP, which then can increase cardiac output, CBF and pulsatility index. 59 Regarding dCA, studies have indicated a deterioration in CA as there were a reduction in dCA parameters phase, 60 , 61 although the dCA parameter gain was not changed by CCB when changes in etCO2 were accounted for. 62
In hypertensive patients, a transient increase in CBF after acute CCB therapy (nifedipine and verapamil), 57 which returns to baseline values after 4-8 weeks of treatment with nifedipine and amlodipine respectively. 63 However, 3 months of treatment with lacidipine (the third generation CCB), had a greater improvement to local cerebral resistance and focal hypoperfusion than hydrochlorothiazide treatment. 47 Four weeks of nifedipine treatment have been shown to impair dCA (phase) in hypertensive patients compared to age-matched controls. 64
A systematic review by Sare et al., 41 of controlled studies administering antihypertensive agents within 7 days of AIS, highlighted CCB as the only nonrandomized trial to see increases in CBF. There were no studies on CBFV, and largely, the five (see Table 3) before-after studies65–69 that evaluated the effect of CCB on CBF demonstrated an overall increase in CBF. However, a sensitivity analysis focusing on studies describing the acute effects66–68 of CCB, or the studies that had performed RCT67–69 showed no overall improvement in CBF. A relatively large randomised study by Hong et al. 70 also found no difference in the increase in CBF following the 4 weeks treatment of either cilnidipine or losartan to chronic stroke patients or was there any association with CBF impairment (when compared globally) in the ipsilesional hemisphere or cerebellum. In chronic stroke patients, extended treatment strategies with applying CCBs for 8 weeks or more showed either increased CBF in the affected hemisphere 71 or distal to large artery occlusions, 72 or an unchanged CBF.73–75 Of note, azelnidipine did not affect acetazolamide induced vasomotor reactivity. 74
Thus, the effects of CCB as a vasodilator that decreases smooth muscle contractility within cerebrovasculature both after acute and chronic treatment are being established. This can augment the redistribution of blood flow and the oxygenation of normal and ischemic cerebral tissues, as resistance to flow and vascular compliance is improved. But there is emerging evidence from healthy and at-risk patients to suggest that the reduced capacity for myogenic dependent vasoconstriction and tone will compromise CA, particularly in countering conditions that further augment hyperperfusion rather than decreased perfusion pressure where a dilated lumen is maintained. This also highlights the importance of BP management when on CCB and further work is needed in determining how CCB may impact CA and the outcome of patients following a stroke during the acute and chronic phases.
Renin-Angiotensin-Aldosterone system inhibitors
The two main classes of pharmacological agents that act by inhibiting the RAAS include, ARB (e.g. candesartan, telmisartan, valsartan, olmesartan, losartan) and ACEI (e.g. the short-acting captopril, or the long-acting enalapril, lisinopril, perindopril, ramipril). ARB inhibits the type 1 angiotensin II receptors (AT1) and the Gq-protein couple receptors and inositol triphosphate (IP3) signal transduction pathway that is responsible for maintaining vascular smooth muscle contraction. ACEI inhibit the conversion of Angiotensin I to Angiotensin II, preventing the binding to AT1 receptors and the vasoconstriction of vascular smooth muscle. Direct renin inhibitors are not reviewed because no literature regarding cerebral autoregulation was found.
Numerous animal models 76 , 77 have disclosed ACEI and ARB benefits to the cerebrovascular system and CA, including reversing the remodelling of hypertension by antagonizing the AT1- and AT2-receptors, and shifting the autoregulatory response towards lower blood pressure (to the left). However, the evidence in humans in unclear. In healthy persons, Demolis et al. 78 found within an 8 hour period a single dose of the ACEI lisinopril had reduced BP, that accompanied a dilatation and an increased blood flow at the common carotid artery, whereas the MCA had an increase in resistance index although it's mean CBF had remained unchanged. It was suggested that there was a paradoxical increase in cerebrovascular resistance, possibly to compensate for the dilation of the large cerebral arteries, which also augmented cerebral vasodilatory reserve following an acetazolamide challenge. In hypertensive patients, a single dose application of the ACEIs enalapril or ramipril or a short term (one week) application of captopril did not change CBF in patients with and without significant carotid artery disease,79–81 whilst perindopril treatment for three weeks has been shown to lower cerebrovascular resistance (and lower pulsatility index) and increase CBFV. 82 Regarding CA, one small study demonstrated that a single dose captopril administration decreased the lower limit of CBF regulation in 5 out of 7 hypertensive patients. 83
The effect of ARB on CBF or CA in healthy individuals is unclear and due to their poor bioavailability and later date of approval as hypertensives, few studies have investigated the effects in other populations. Small studies have shown that valsartan 64 and candesartan 48 normalise an impaired vasomotor reactivity in hypertensive patients. A combination of losartan with hydrochlorothiazide treatment for up to 4 months reduced cerebrovascular resistance index (ratio of BP:CBF) without changing CBFV, whilst increasing the dCA parameter gain from a low level that was present before treatment. 84
In AIS patients, short term application of ACEIs between one hour to 2 weeks did not result in reductions of CBF 85 or CBFV 86 , 87 but did increase vasomotor reactivity induced by acetazolamide. 88 Only alacepril was reported to increase CBF in both affected and unaffected hemispheres in hypertensive stroke patients. 89
ARB affect CBF of AIS patients in a less conclusive manner. CBF can remain unchanged after short term 90 and long term 54 , 91 treatment, or be increased 70 , 92 after 4 weeks treatment. Losartan in combination with hydrochlorothiazide may increase vasomotor reactivity. 54 However, irbesartan was reported to lower CBF in chronic AIS patients in both the affected and unaffected hemisphere. 37 Apart from this single report, there is no further evidence that RAAS antagonists impair CBF. In summary, their ability in preventing angiotensin II vasoconstriction might apprehend an ability to constrict during increased BP, but reducing vascular resistance (through promoting NO pathways) provide them with the capacity to dilate (large cerebral arteries) when there is a drop in BP. Although such benefits have made them preferable to other hypertensives, there is a dearth of studies confirming the short- and long-term benefits to the cerebrovascular system in ischemic stroke patients.
Nitric oxide donors
Nitric oxide (NO) is a potent vasodilator produced in the endothelium from oxygen and L-arginine in a reaction catalyzed by the enzyme eNOS. Local production of NO diffuses into surrounding vascular smooth muscle cells, where it activates soluble guanylyl cyclase and subsequent cyclic guanosine monophosphate formation and vasorelaxation. The NO donor’s sodium nitroprusside (SNP) and glyceryl trinitrate (GTN) are used in clinical settings to treat acute hypertension and angina, while L-Arginine and sodium nitrate are used in both pre-clinical and clinical trials.
In healthy individuals, NO donors decrease systolic BP in a dose-dependent manner, 93 , 94 decrease BRS and CBFV.95–97 One week of sodium nitrate supplementation has been shown to increase CVR and decrease arterial stiffness in young healthy individuals, 98 and decreased blood pressure variability (BPV) and improved dCA (decreased coherence) in acute transient ischemic attack patients. 99 In a recent review 100 of the use of GTN in the management of acute stroke (both ischemic and haemorrhagic stroke), GTN was reported to maintain CBF 101 , 102 whilst lowering BP, improve cognition, mood and quality of life, and reduce death and disability. When administered with transdermal patches, a low dose of GTN (5 mg/day) within 4 hours of stroke onset, for 7 days rapidly reduced BP safely. 103 When administered within 3 days 101 or 5 days 102 of stroke onset, reductions in central and peripheral systolic BP did not appear to alter CBF or global cerebral perfusion 1–24 hours following administration. Despite the lack of effects on resting CBF in stroke patients with low-dose of transdermal GTN, there is emerging evidence that NO donors improve cerebrovascular function in both healthy cohorts and transient ischemic attack patients at high risk of stroke, as well as improve patient outcome following AIS. Since the effect of NO donors on vascular tone appears to be dose-dependent, further studies are needed to establish the effects of NO donors on the cerebrovascular function in acute stroke.
Centrally acting sympatholytics
Centrally acting sympatholytics will act within the brain to prevent the release of neurotransmitters from the sympathetic nervous system that is responsible for increasing the heart rate and contractility. To decrease the sympathetic tone, central α2-adrenoreceptor agonists (clonidine, guanabenz, guanfacine, alpha-methyldopa) act via the stimulation of central α2-adrenergic receptors that suppresses (provide negative feedback) the activity of the sympathetic neurons. The sympatholytic drugs that are ganglion blocking (trimethaphan etc) are not in use in AIS patients and have therefore not been reviewed.
In healthy persons, clonidine decreases BP, peripheral vascular resistance and cardiac output and increases BRS, but decreases CBF (about 30%) and CBFV via an increase of cerebral vascular resistance. 104 Additionally, CVR is attenuated. 105
In hypertensive patients, clonidine monotherapy reduces BP, heart rate and increases BRS. 106 Clonidine may have the property to adjust CBF as it was reported that increases or decreases in CBF were dependent on initial CBF, with low CBF prompting an increase and a high initial flow rate prompting a decrease. 107 Clonidine’s sedative properties and its administration during anaesthesia have been described to attenuate CBFV and cerebral CVR during hypercapnia, but not during hypocapnia or normocapnia, or the cerebrovascular CO2 response during sevoflurane anaesthesia. 108 As aforementioned, Lisk et al. 68 conducted a small RCT and found that when compared to nicardipine, there was no additional benefit to using clonidine in hypertensive AIS poststroke.
Thus, with there being a lack of large RCT to determine if there would be any benefits to the use of α-AR agonists as a hypertensive strategy in the acute phase of stroke, 109 there is also a lack of studies in humans that indicate if clonidine may be beneficial to the cerebrovascular system. However, experimental preclinical models have disclosed that clonidine can enhance CVR in the cat cerebrovascular system 110 and that pre-treatment of clonidine can confer neuroprotection during cerebral ischaemia in rats via the NMDA-R. 111 Thus, by targeting the pre-synaptic α2-receptors and modifying the release of adrenaline and noradrenaline it seems possible to reduce the systemic BP, reduce CBF, which subsequently reduces the CO2 response, possibly by the increase in cerebrovascular resistance and relying more on the myogenic control and its intrinsic properties.
Peripheral sympatholytic drugs (β-adrenoreceptor blockers and α-adrenoreceptor blockers)
Blocking β-adrenoreceptors (β-AR) at the heart and vasculature provides competition to an augmented sympathetic system, and the use of BB is a well-established antihypertensive strategy that acts by reducing the HR, depressing cardiac functions (cardiac contractility, conduction), and modifying the cardiac output and the oxygen consumption within the cardiac tissue. As β2-AR are also expressed on smooth muscle within the airways and vasculature and have a minor vasoconstricting role in regulating vascular tone, the more selective β1-antagonists (acebutolol, atenolol, bisoprolol, esmolol, metoprolol, nebivolol) are more specific to the heart. Of note, the selective β1-BB nebivolol also has vasodilation properties (NO-mediated) within the vascular system. 112 The non-selective BB that also acts as β2-antagonists (carteolol, nadolol, penbutolol, pindolol, propranolol, timolol) will prompt some vasoconstriction within peripheral system, whilst carvedilol and labetalol, can also act as α1-AR antagonists, which overcome the dominant vasoconstricting role of α-AR within the vasculature. α1-AR antagonists or α-blockers such as doxazosin, terazosin and prazosin thus prompt a reduction in total peripheral resistance. β2-agonists that act as bronchodilators to treat asthma and COPD (and contradictory to the use of BB) are not reviewed.
In healthy individuals, BB with associated vasodilatory properties (α1-blocker - celiprolol, nebivolol, carvedilol, and labetalol via increased NO bioactivity) did not change CBF, CBFV or CVR. 113 Compared to the naïve condition the more cardio-selective BB (such as metoprolol) does not change BP, CBFV and static CA as well as dCA (rate of CBFV regulation, RoR, to thigh cuff release). 114 The non-selective β1- and β2-blocker propranolol 115 attenuated exercise capacity and the HR, BP and cardiac output increases to exercise, as well as reducing CBFV and frontal lobe oxygenation. Esmolol may reduce cerebral oxygenation when applied together with haemodilution therapy. 116 The α-1 and α-2 receptor antagonist phentolamine (acutely administered intravenously) did not change CBFV but increased the dCA parameter gain and reduced coherence that also decreased etCO22. A single oral dose of prazosin (α-1 blocker) did not affect CBFV at rest and did not decrease the rate of CBFV return after thigh cuff release. 117
In hypertensive patients, selective β-blockers atenolol increased CBFV after four weeks of treatment in comparison to uncontrolled hypertensive group but decreased dCA parameters phase and gain. 64 A single dose of prazosin did not reduce CBF in the hypotensive period associated with the first dose of BB. 118
In AIS patients, the use of BB in managing hypertension is not recommended following stroke unless the patient has a pre-existing condition, usually angina or myocardial infarction (to decrease cardiac work rate and oxygen demand), heart failure or arrhythmias. Meyer et al. 119 investigated the effects of propranolol in patients with cerebral ischaemia and infarction and reported a decrease in CBF and oxygen consumption and increase in cerebrovascular resistance, with no changes to BP and intracranial venous pressure. A tilt-table test disclosed that BB improved CA to tolerate increases to cranial perfusion pressure (CPP) but a tendency to deteriorate CA when CPP was lowered, with CVR not being affected. An earlier study by the same group 120 adopting a similar study design also reported that the α-blocker phenoxybenzamine improved CA when CPP is lowered, but worsened when CPP is raised with the vasoreactivity not significantly altered. To summarise, in stroke patient’s, the limited evidence suggests that BB and α-blockers are thought to have opposing effects on the autoregulation curve. These studies also suggest that cerebrovascualr reactivity is largely controlled by local metabolic mechanisms and not by autonomic innervations of cerebral vessels.
Future outlook
Overall, this review exposes areas of future research that would be of benefit to patients with stroke and the research field in general. Little is currently known about the effects of antithrombotics, thrombolytics and diuretics on dCA, mainly as they are often used in combination with other therapies. The effects of β-blockers and CCB are well described, and there is emerging evidence of the benefits of ACEI/ARB and NO donors. However, it is unknown whether drugs with a vasodilatory effect (statins, CCB, NO donors) can improve or deteriorate CA and whether a global improvement also reflects improved CA within the penumbra. Investigations on dCA are lacking in comparison to other physiological investigations, possibly due to the complex methodologies and inconsistencies that the INFOMATAS working group is currently addressing. Of note, can the conflicting results in the dCA parameter gain, common in hypertensive patients, 7 , 9 , 61 , 84 , 121 be explained by the drug interactions and changes to vascular tone? Or by using mathematical models and individualised treatment strategies, can we derive what antihypertensive therapy is best applied for a specific acute stroke treatment strategy?
Of special interest are those drugs, such as statins, ACEI or ARB (particularly in preclinical models) that have shown promise to have additional effects on the cardiovascular system, including improving CA. Prospective clinical long-term studies evaluating these compounds are essential. Recent and current ongoing studies that have been designed to investigate the effects of different drug treatments during chronic stages of stroke, such as LACI-1 122 and OxHARP 123 that are randomised, cross-over and placebo designed trials that include cerebral hemodynamic and cerebrovascular assessments will provide some future perspectives. However, whether similar designed trials can be used within the acute stages of stroke will be more challenging. All stroke subtypes can impair dCA, where a deterioration will occur within the first days before improving during the chronic period. In this condition carefully performed observational studies with bedside monitoring which observe dCA could help address safety considerations.
Impairment of dCA is associated with poor outcome. A disturbed dCA is associated with cerebral complications of thrombolysis but it is unclear whether this association is an independent variable or the result of dCA impairment due to stroke and its corresponding clinical severity, or the presence of an augmented BP and/or its variability. Despite their positive effects it is not established whether the presence or absence of the aforementioned drugs may play a role in dCA's evolution over time. Some benefits for the patients have been reported 5 if dCA between BP and CBF is used to guide BP management during the first two days after a stroke; this approach is promising and should be evaluated further.
Summary
Despite the importance and complexity of CBF control, the current clinical approach to acute stroke rarely considers the implication of pharmacological interventions on cerebral autoregulation and other determinants of cerebral perfusion. The effects of pharmacological interventions on cerebrovascular function warrant further investigation, with carefully designed studies that maybe use a crossover design or drug titration to guide the dCA parameters that can later be used for multiparametric modelling. Some of these developments and questions have been highlighted in this series of reviews by the CARNET’s working group INFOMATAS in the hope to better predict a stroke patients’ response to therapy and to improve future clinical outcome.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.