
Abstract
The brain’s vasculature is essential for brain health and its dysfunction contributes to the onset and development of many dementias and neurological disorders. While numerous in vivo imaging techniques exist to investigate cerebral haemodynamics in humans, phase-contrast magnetic resonance imaging (MRI) has emerged as a reliable, non-invasive method of quantifying blood flow within intracranial vessels. In recent years, an advanced form of this method, known as 4D flow, has been developed and utilised in patient studies, where its ability to capture complex blood flow dynamics within any major vessel across the acquired volume has proved effective in collecting large amounts of information in a single scan. While extremely promising as a method of examining the vascular system’s role in brain-related diseases, the collection of 4D data can be time-consuming, meaning data quality has to be traded off against the acquisition time. Here, we review the available literature to examine 4D flow’s capabilities in assessing physiological and pathological features of the cerebrovascular system. Emerging techniques such as dynamic velocity-encoding and advanced undersampling methods, combined with increasingly high-field MRI scanners, are likely to bring 4D flow to the forefront of cerebrovascular imaging studies in the years to come.
Introduction
Blood supply to the brain tissue is a crucial factor in brain health. 1 Impairment of the brain’s blood vessels can lead to ischaemic stroke, haemorrhage and cognitive decline, which contribute to morbidity and mortality. 2 It is important therefore to understand the nature and progression of vascular changes associated with ageing, vascular-based pathologies and neurodegeneration in order to diagnose, treat and prevent these conditions.
Current techniques
Intracranial blood flow is a tightly regulated system, as the brain requires a constant supply of blood for normal function and structural integrity 3 due to its lack of energy storage. In a clinical setting, catheter angiography is often used to examine blood vessels to identify abnormalities such as aneurysms and stenosis – a technique that combines invasive catheter insertion, contrast injection and X-ray exposure. Alternatively, computed tomography angiography can be used alongside injected contrast agents to visualise vessels in the head and neck in high detail for evidence of damage and vascular dysfunction. The use of CT in this technique carries a significant radiation dose, however, and therefore neither method is suitable for volunteers or many large research studies.
To measure intravascular blood flow velocities directly and non-invasively, major cerebral vessels are examined using specialised imaging methods; namely, ultrasonography (US) and phase contrast magnetic resonance imaging (PC-MRI). The former technique measures blood flow velocity in real-time, usually at the neck or through windows in the skull. PC-MRI can measure fluid velocity in any major blood vessel or cerebrospinal fluid (CSF) space of interest and allows for the quantification of lumen area and thus blood or CSF flow. PC-MRI is typically acquired with two spatial dimensions and one temporal dimension representing the cardiac phase (often triggered using an ECG signal or finger pulse oximeter). For quantitative measurements, the slice is placed perpendicular to the vessel of interest.
4D flow
Recently, an advanced form of PC-MRI has been developed that collects more information per unit time and requires less precise placement of the imaging volume. 4D PC-MRI (or 4D flow as it is commonly known) extends the methodology of 2D PC-MRI to cover a three-dimensional slab of data measured over time, with velocities in the three cardinal directions captured (Figure 1). The advantage of this method is that the 4D data can be processed post-hoc at any time to analyse vessels captured and resolved within the slab, and the three-dimensional Fourier encoding results in higher signal-to-noise ratio (SNR) compared to the sequential acquisition of multiple slices. Which blood vessels can be assessed following a 4D flow acquisition depends heavily on spatial resolution and the range of velocities encoded in the image. Major arteries such as the carotids, as well as the first (and potentially second) segments of the cerebral arteries, and major veins are all capable of being analysed using this method. It is important to emphasise that 4D flow is capable of non-invasively quantifying volumetric blood flow within the arteries and veins that supply the brain, and therefore is fundamentally different to available angiography methods both invasive and non-invasive.
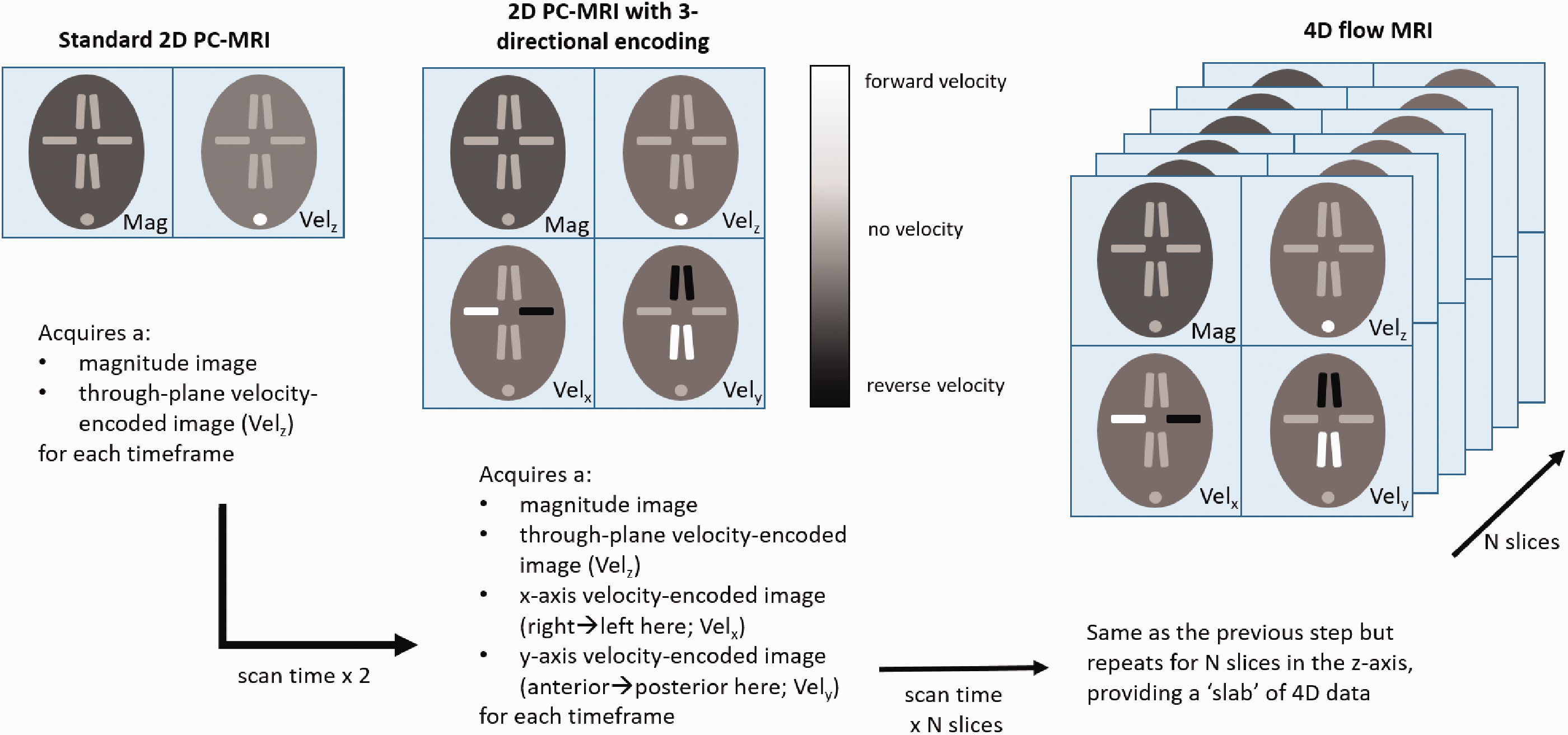
2D phase-contrast to 4D flow MRI. On the left, a diagrammatic representation of the data collected by standard 2D PC-MRI is shown. Each image depicts an axial slice through the brain showing several cerebral blood vessels. A magnitude image of the slice is obtained at each timeframe, as well as a single-direction velocity-encoded image (through-plane velocity, Vz). For three-directional encoding in a single slice, magnitude and through-plane velocity images are retrieved, as well as velocity images in the remaining in-plane directions (Vx and Vy) – this halves the temporal resolution of single-direction velocity encoding. For 4D flow MRI, magnitude, Vz, Vx and Vy data are collected for a multi-slice volume, increasing the scan time by the number of slices required. If the voxels are isotropic, the resulting 4D dataset can be examined at any orientation. As the dataset becomes increasingly complex, we can gain more flow information but require acceleration methods to offset scan times.
As shown in Figure 1, each slice within the 4D ‘slab’ leads to four datasets: one magnitude (structural) image and velocity images for each of the three directions, with one image per timeframe. Across all slices, the amount of data collected can be substantial, meaning acquisition times can be unfeasibly long in a clinical setting.
This systematic review examines the current state of brain 4D flow methodology for clinical research, and aims to showcase its effectiveness in acquiring haemodynamic information from anatomically-defined cerebral blood vessels in a non-invasive, reproducible manner. In doing so, this review will also highlight the promising results being obtained at present as well as the areas of potential improvement. This new tool has reached a certain level of technical maturity and, though not widely available yet, is approaching the point where it may become standard on clinical scanners with clinically relevant scan times. It is important, therefore, to assess its capabilities in addressing significant biological questions as it becomes more useful for research (and potentially clinically) in the future.
The physics behind measuring blood flow in vivo, and the many examples of 2D phase-contrast imaging and Doppler US in clinical brain studies, are beyond the scope of the review. The reader is encouraged to look elsewhere for extensive literature on these topics (for example: Shi et al. 5 and Bryant et al. 6 ).
Methods
In September 2019, we used PubMed to conduct a literature search for studies that include the terms: ‘4D flow’, ‘4D PC MRI’ or ‘3D blood flow phase-contrast’ and ‘brain’, ‘cerebral’ or ‘dementia’. Only English literatures were sought. The search was updated in January 2020. Papers were initially excluded based on their titles and abstracts. The remaining papers were collected for full-text screening to assess their eligibility, and subsequent data extraction if eligible. Title, abstract and full-text screening was carried out by one researcher (AGM).
Eligibility criteria
Papers describing the use of 4D flow MRI to examine human neurological and cerebrovascular diseases, as well as those examining the feasibility of using the technique to examine cerebral vessels, were included in the review. Any studies that used 4D flow on organs other than the brain (usually the heart), on animal models, 3D-printed models or other MRI phantoms were not included. MR angiography studies were also excluded as that method is focused on visualising vessels rather than quantifying their blood flow.
It should also be noted that, due to this being a relatively new technique, case studies with very few subjects were included in the review since they could hold valuable methodological information on 4D flow.
Results
Our search of PubMed returned 251 papers, with no duplicates. We identified 61 papers that met inclusion criteria for this review (2665 subjects, range 1–399, median = 18), spanning 16 years of publication (including 2005) from 2005 to 2020 (Figure 2).
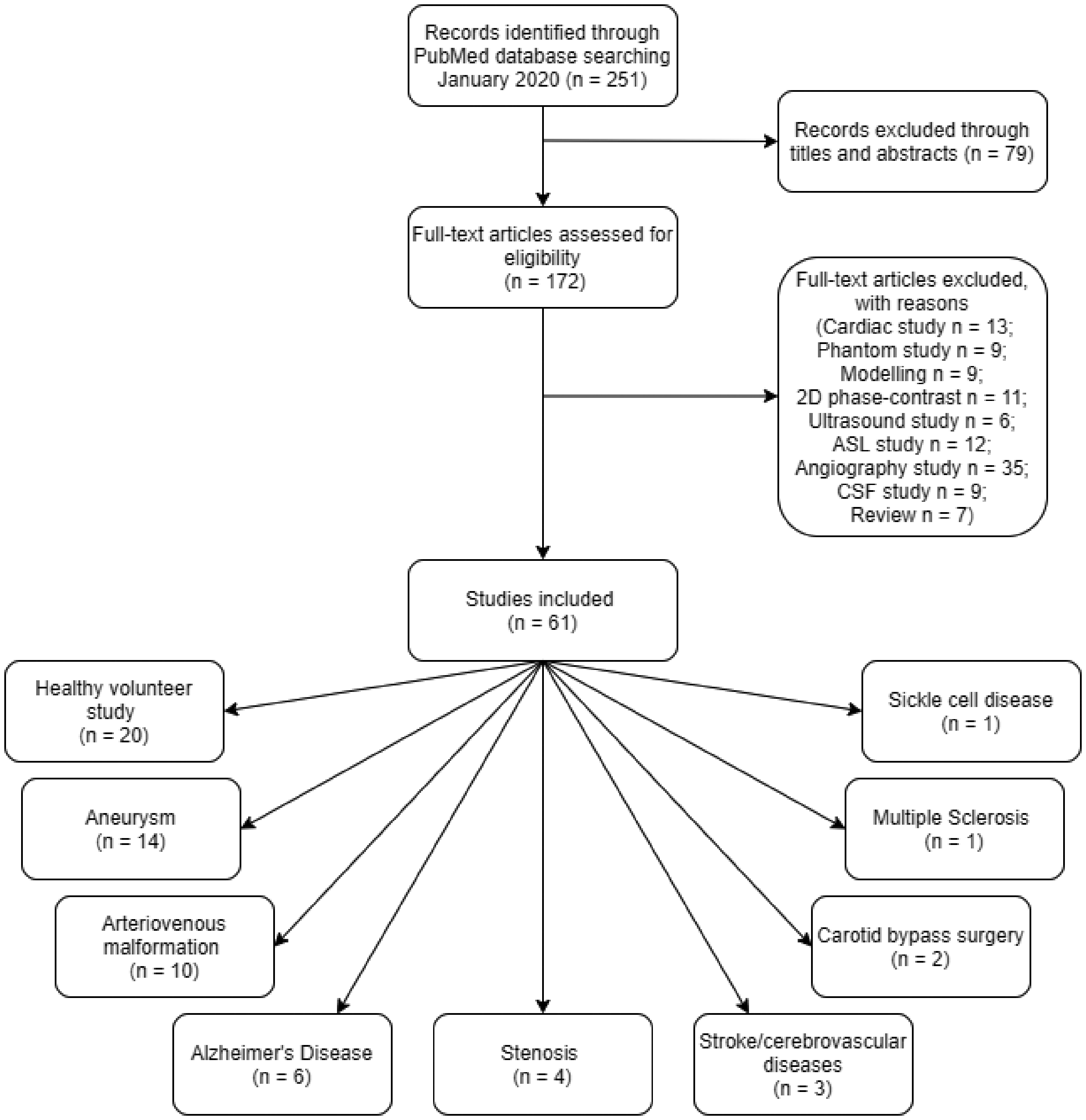
Flow diagram of literature search and its results.
Disease characteristics
We found that aneurysms (n papers = 14), arteriovenous malformation (n = 10), Alzheimer’s disease (AD) (n = 6), stenosis (n = 4), cerebrovascular disease (n = 2), stroke (n = 1), multiple sclerosis (MS; n = 1) and sickle cell disease (SCD) (n = 1) have all been researched using 4D flow on the human brain. Moreover, a large proportion of brain 4D flow studies (32%, n = 20) were technically-focused and examined healthy volunteers, and some were used to examine the aftereffects of carotid bypass surgery (n = 2). A summary of recent, clinical studies using cerebral 4D flow is shown in Table 1.
Summary of clinical 4D flow papers examining cerebral blood vessels.
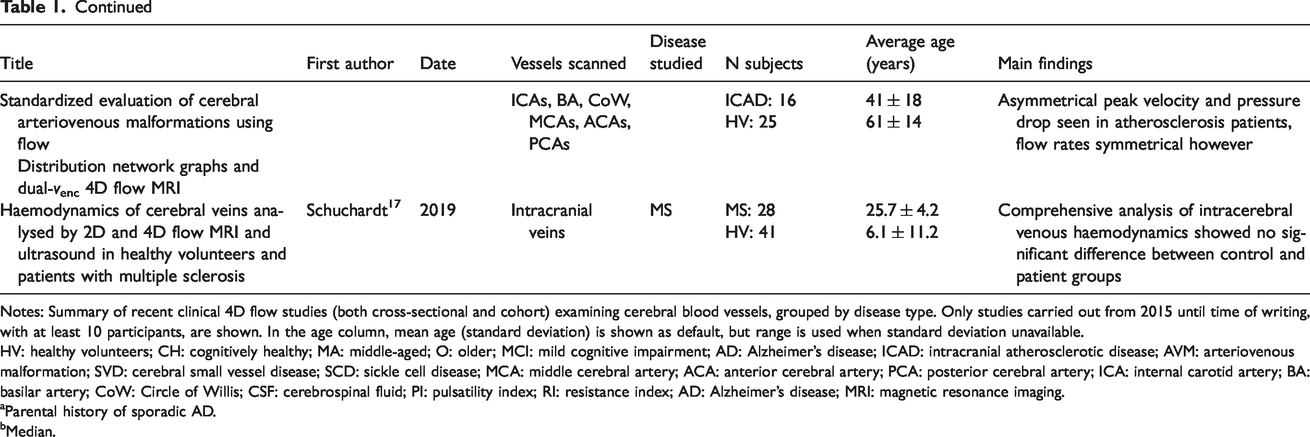
Notes: Summary of recent clinical 4D flow studies (both cross-sectional and cohort) examining cerebral blood vessels, grouped by disease type. Only studies carried out from 2015 until time of writing, with at least 10 participants, are shown. In the age column, mean age (standard deviation) is shown as default, but range is used when standard deviation unavailable.
HV: healthy volunteers; CH: cognitively healthy; MA: middle-aged; O: older; MCI: mild cognitive impairment; AD: Alzheimer’s disease; ICAD: intracranial atherosclerotic disease; AVM: arteriovenous malformation; SVD: cerebral small vessel disease; SCD: sickle cell disease; MCA: middle cerebral artery; ACA: anterior cerebral artery; PCA: posterior cerebral artery; ICA: internal carotid artery; BA: basilar artery; CoW: Circle of Willis; CSF: cerebrospinal fluid; PI: pulsatility index; RI: resistance index; AD: Alzheimer’s disease; MRI: magnetic resonance imaging.
aParental history of sporadic AD.
bMedian.
Technical characteristics
4D flow scans were carried out on both 1.5 and 3 T MRI scanners (with one use of 7 T), using 8, 12, 20 and 32 channel head or head-and-neck receive coils. Scan times ranged between approximately 5 and 30 min. A total of 20 studies mention the use of an accelerated 4D flow technique known as phase-contrast with vastly undersampled isotropic voxel radial projection imaging (PC-VIPR)7,8; five studies used k-t undersampling of both spatial and temporal data. A summary of technically-focused cerebral 4D flow papers is shown in Table 2.
Summary of technical 4D flow papers examining cerebral blood vessels.
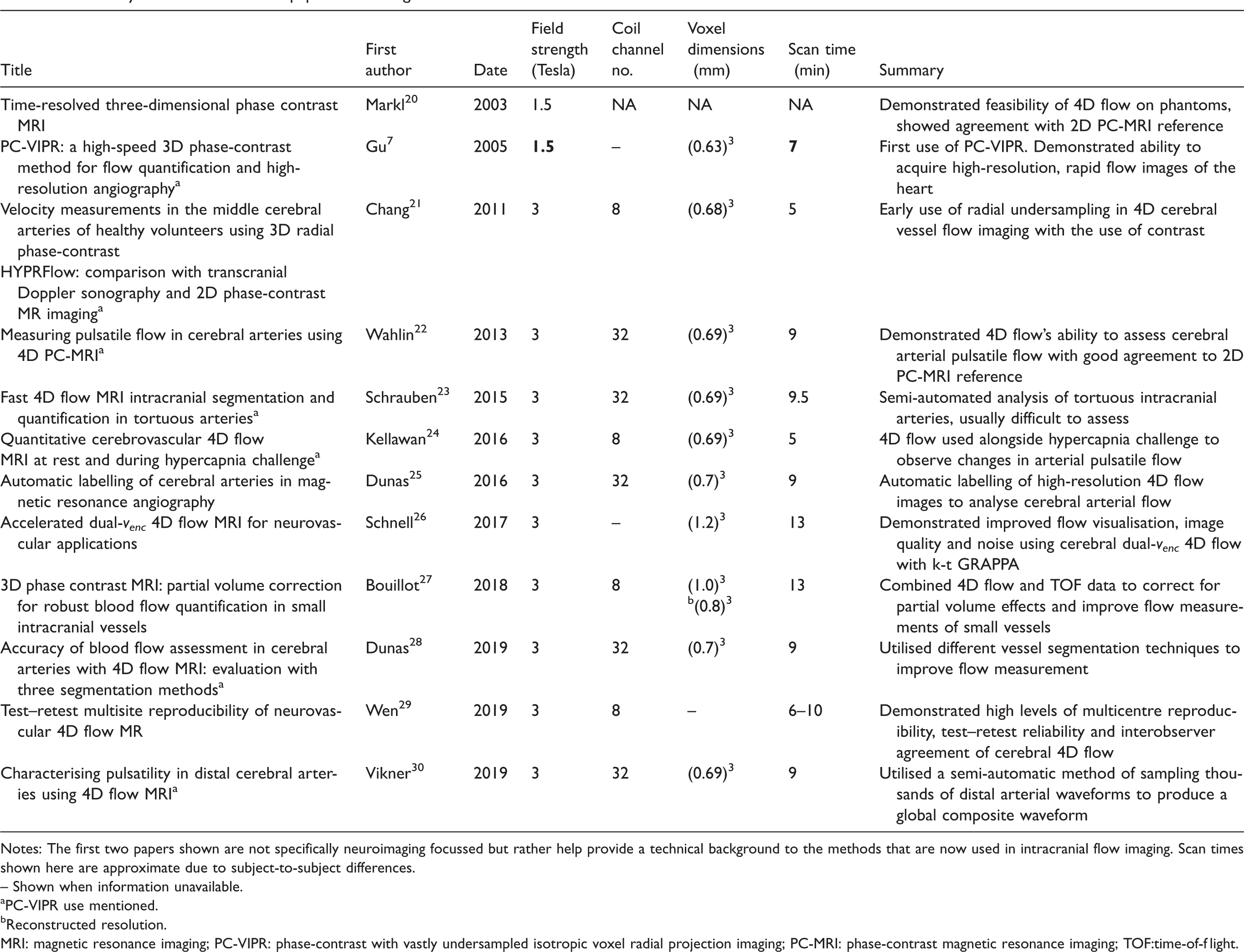
Notes: The first two papers shown are not specifically neuroimaging focussed but rather help provide a technical background to the methods that are now used in intracranial flow imaging. Scan times shown here are approximate due to subject-to-subject differences.
– Shown when information unavailable.
aPC-VIPR use mentioned.
bReconstructed resolution.
MRI: magnetic resonance imaging; PC-VIPR: phase-contrast with vastly undersampled isotropic voxel radial projection imaging; PC-MRI: phase-contrast magnetic resonance imaging; TOF:time-of-f light.
4D flow is used in many contexts, with select arterial and venous examples depicted in Figure 3. Grouped according to disease and research contexts, relevant results from the literature search will now be summarised.
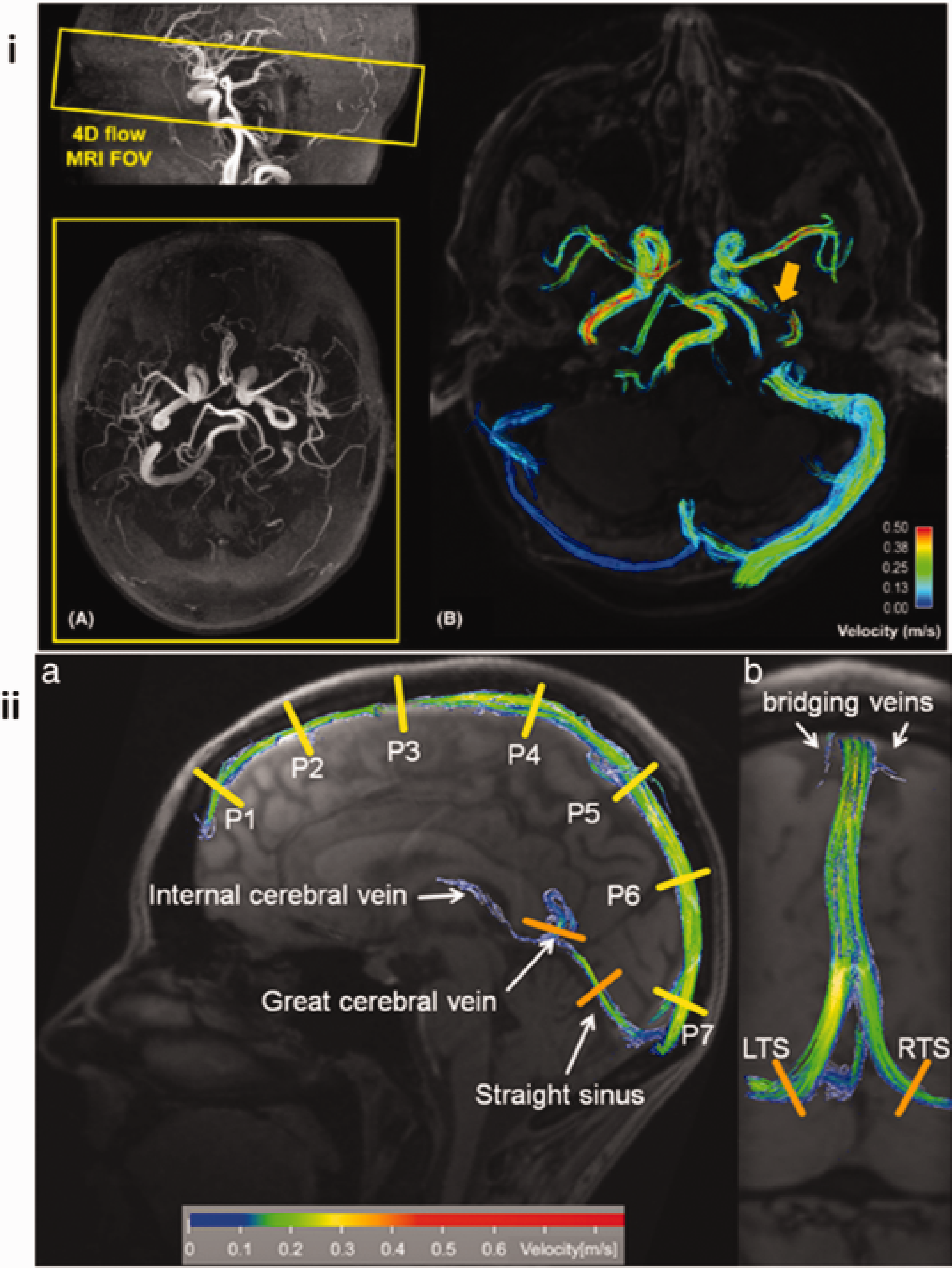
The two images shown here depict 4D flow used in two different research contexts. (a) Vali et al. 15 used 4D flow to measure the pressure drop at the site of intracranial atherosclerotic stenosis, as well as changes in blood flow distribution. This image uses a TOF maximum intensity projection to show the volume coverage of the 4D flow scan, and a velocity map to depict the information acquired. (b) This image was taken from Schuchardt et al.’s 36 paper on analysing cerebral vein haemodynamics. It can be seen that, by utilising a lower venc, detailed velocities can be encoded from a range of cerebral veins in a single 4D flow scan. This information was used to compare MS patients to healthy volunteers.
Alzheimer’s disease
Rivera-Rivera et al. 10 used 4D flow with PC-VIPR to assess intracranial haemodynamics in healthy controls, patients with mild cognitive impairment (MCI) and patients with AD, and found levels of arterial pulsatility throughout the vascular tree were significantly higher in AD compared to MCI and, in turn, to controls. This study acquired substantial cerebral flow information in a relatively short time (seven minutes) with high spatial resolution (0.7 mm isotropic voxels) and shows that it is feasible to carry out a relatively large-scale study (160 subjects) using 4D flow.
The same research group published a study 9 using 4D flow to examine cerebral vessel flow metrics in relation to markers of brain health and AD. They found that lower mean flow of the middle cerebral arteries (MCAs) and internal carotid arteries (ICAs) was associated with greater brain atrophy, as was increased MCA stiffness (represented as Gosling’s Pulsatility Index equation, PI = (flowmax – flowmin)/flowmean); they also found decreased mean flow in the ICAs was associated with lower amyloid beta in the CSF. The same group carried out a similar study two years later, 12 with subjects undergoing a neuropsychiatric battery and lumbar puncture (for CSF assay). They found an association between ICA and MCA mean flow and executive functioning performance, as well as evidence of an association between decreased blood flow and amyloid beta deposition across 38 MCI subjects, correcting for age and sex. The results from these studies suggest that neurovascular health may contribute to the development of AD. Once again, these 4D flow data were obtained using PC-VIPR with an acquisition time of seven minutes and 0.7 mm isotropic voxels, covering substantial vascular territory with a 22 × 22 × 22 cm3 volume across the brain. However, the temporal resolutions used in these studies by Berman et al. and Rivera-Rivera et al. were, like in many 4D flow studies, limited. 4D flow methods use cardiac triggering with prospective or retrospective gating and resolve the data retrospectively into cardiac phases using temporal interpolation. In these two studies, each cardiac cycle was separated into 20 phases.
Rivera-Rivera et al. published a paper in 2017 in which they examined blood flow in the cerebral veins and arteries simultaneously, 11 with similar success to their arterial study. However, they reported problems involving the velocity-encoding parameter, venc, and the large velocity differences between arterial and venous blood. For example, they were unable to analyse 21 straight sinus vessel segments due to their low blood flow velocities, an issue mentioned frequently in the other studies reviewed. The venc parameter adjusts the first moment of the phase-contrast scan’s velocity-encoding bipolar gradient pairs and, prior to the scan, is typically adjusted to encode the highest expected velocity. Any velocities above this result in phase wrap-around, or ‘aliasing’, so the value has to be selected carefully according to the vessel(s) of interest. 31 Conversely, if venc is set too high, precision is lost. The issue faced with 4D flow, therefore, and mentioned frequently in the studies reviewed, is that one venc value is used per acquisition, meaning it cannot be adjusted for separate vessels of differing blood flow velocities and thus the quality of the flow data acquired is vessel-dependent. For example, Dunas et al. report their use of a high venc (110 cm/s) as a limitation of their study, again due to the potentially lost information in slower-flowing vessels.
Sickle cell disease
Vaclavu et al. 18 demonstrated the advantages of 4D flow when investigating the pathological characteristics of SCD. The effect of SCD on stroke risk in children is currently evaluated using transcranial Doppler (TCD) US to measure blood flow velocity in the circle of Willis (CoW), where abnormally high velocities are associated with higher risk of overt stroke. 32 However, no TCD-derived biomarker exists in adults to provide a reliable prognosis due to factors such as skull thickness, operator-dependency and poor insonation windows. 4D flow allowed Vaclavu et al. to assess velocity, flow, vessel lumen area and wall shear stress in the CoW and detect significant differences in SCD adults compared to healthy controls. This study achieved a very high spatial resolution with 0.5 mm isotropic voxels, stating that this was the highest resolution that was technically feasible in the six-minute scan time (via the use of PC-VIPR). Temporal resolution was sacrificed for high spatial resolution, a decision made by Vaclavu et al. based on work carried out by Cibis et al. 33 who point out that mean blood flow and shear stress estimates are minimally influenced by temporal resolution and therefore spatial resolution should have priority. This was further accounted for in the Vaclavu et al.’s study by averaging values across the cardiac cycle to obtain time-averaged velocity, flow and shear stress.
Brain ageing and cerebral small vessel disease
Several studies were found to have used 4D flow to assess the role of vessel stiffness (manifest as pulsatility) in cerebrovascular health. Holmgren et al. 34 demonstrated the technique’s ability to measure arterial pulsatility and compliance, and cerebrovascular resistance, across a range of cerebral arteries in a population of elderly subjects (mean 79 ± 5 years). Birnefeld et al. 16 examined the ICAs and MCAs (M1, M3) of 89 patients with acute ischaemic stroke or transient ischaemic attack (divided into two groups based on clinical assessment: those with associated cerebral small vessel disease (SVD) and those without). They found ICA pulsatility to be associated with increased white matter lesion volume and M1 pulsatility with decreased cognitive function. Due to phase-contrast MRI’s ability to measure flow rates (ml/s), Birnefeld et al. were able to use cumulative integration to calculate flow volume pulsatility (FVP) for each vessel of interest. Finding FVP more strongly associated to SVD features compared to the commonly used PI, they argue that this ‘may be a useful biomarker in future studies of cerebral pulsatility’.
Vikner et al. 30 utilised 4D flow in 33 elderly subjects (mean age 79 years, range 70–91) to measure pulsatility of distal, small cerebral arteries. They achieved this by finding and sampling flow waveforms from thousands of small vessels in the brain using automatic positioning of flow planes and spatial interpolation. A global composite flow waveform of these numerous distal arteries could then be estimated and this was shown to increase as a function of age.
Multiple sclerosis
In 2015, Schuchardt et al. 35 conducted a study using 4D flow on 15 healthy volunteers to examine blood flow in the venous sinuses. They found the technique to be effective, highly reliable and accurate by assessing intra- and inter-observer agreement as well as comparing 4D results to 2D blood flow measurements, but state that ‘limited spatial resolution currently precludes flow quantification in small cerebral veins’. In 2019, the same group then used 4D flow to systematically assess the haemodynamics of the brain’s superficial and intracranial venous system with one MRI acquisition 36 (Figure 3(b)). They did this in 28 relapsing–remitting MS patients and 41 controls, finding no relevant differences between the groups. Due to the less pulsatile nature of veins compared to arteries, Schuchardt et al. mention that intracranial venous assessments such as these are less dependent on higher temporal resolutions to capture accurate flow measurements.
Accuracy and reproducibility
As 2D PC-MRI is the current ‘gold-standard’ for assessing blood flow in major cerebral vessels, several studies22,28,37 compared 2D and 4D flow at identical vessel locations for validation purposes, finding significant correlations between results and equal measurement consistency across techniques. Dunas et al. 28 note the low numbers of 4D flow voxels within smaller cerebral vessels – with numerous vessel cross-sections being fewer than 4 voxels (0.7 mm isotropic resolution) in diameter – and defend their use of oversized regions of interest to reduce flow quantification error by capturing all pixels with a flow-signal (albeit while incurring more severe partial volume effects). Wahlin et al. 22 also mention the limitations of lower spatial resolution of 4D compared to 2D PC-MRI, meaning smaller vessels exhibit flow overestimation due to the partial volume effect.
Wen et al. 29 assessed the multicentre reproducibility, test–retest reliability, and interobserver dependence of 4D flow measurements in the intracranial vessels of 10 healthy volunteers, by scanning each subject twice at three different centres. In measurements of blood flow and peak velocity, they found high multicentre reproducibility (intraclass correlation coefficient (ICC) = 0.77-0.96, all P < 0.001) and test–retest reliability (correlation r = 0.75–0.94 and all P < 0.001), as well as strong interobserver agreement (all ICC > 0.9 and all P < 0.001).
Carotid surgery
Sekine et al. 38 utilised 4D flow as a non-invasive means of characterising patients who had undergone extracranial–intracranial carotid bypass surgery (a controversial treatment for ischaemic cerebrovascular disease), extracting flow direction, bypass patency and blood volume data for each artery of interest. They found success in 4D flow’s ability to characterise each bypass, by extracting information from the M1 segment of the MCAs. However, limitations of the study included no comparison to a ‘gold-standard’ technique, uniform venc, long scan times and poor flow extraction of small vessels. A similar study was carried out by the same group in 2019 to assess arterial blood flow before and after carotid bypass surgery, 39 in which undersampling techniques reduced the scan time to just six minutes, yet issues with low spatial resolution continued to limit the evaluation of small arteries.
Discussion
We identified 61 studies that assessed intracranial vessels using 4D flow including 2665 subjects. Across the studies examined in this review, the consensus is undoubtedly that 4D flow MRI provides large amounts of useful data across extensive vascular territories in increasingly short acquisition times. However, the limitations reported in the literature point to recurring themes: scan duration, spatial and temporal resolution, and the negative consequences of the resulting trade-offs. Advanced methods are emerging that will address these issues 40 and will likely bring 4D flow to the forefront of cerebrovascular research, which will now be discussed.
Accelerating data acquisition
Parallel imaging techniques such as SENSE and GRAPPA significantly accelerate data acquisition at the cost of SNR, allowing multiple receiver coil channels to work in parallel and reduce the number of phase encoding steps required. However, it is still necessary to fully sample the centre of k-space, limiting the acceleration factor in practice. Newer forms of parallel imaging that use the temporal domain, such as k-t GRAPPA, are emerging which reduce the need to fully sample central k-space and reduce acquisition time even further.41–43
In recent years, compressed sensing 44 (CS) has been used to substantially reduce cardiothoracic 4D flow scan times. CS ‘exploits the inherent compressibility of MRI data’ and can be combined with parallel imaging to accelerate 4D flow scans. 45 Although not related to the brain, spiral k-t undersampling has been used alongside CS to successfully acquire 4D flow data from a subject’s abdomen within a single breath hold. 46 Similarly, MR imaging of the aorta using CS has been shown to produce results of similar accuracy to conventional 4D flow within a two-minute scan 45 – with less than five minutes for inline reconstruction. However, some underestimation of peak flow and velocity values did take place as a consequence of such rapid scanning. When it comes to acquiring 4D flow data, the balance between acceptable acquisition times and temporal resolution has to be considered. Ideal temporal resolution may be obtained at the cost of an unfeasible scan time, while conversely shorter scan times will worsen the resolution yet are important in healthcare due to scanner cost as well patient movement within the scanner. In this context, technical developments such as those discussed are promising for the future of brain 4D flow research.
Almost half of the papers examined (n = 35) report the use of 20 or fewer timeframes across the cardiac cycle. This may be considered low temporal resolution when compared to the higher number of phases typically acquired in 2D PC-MRI (for example, Shi et al. 47 and Wahlin et al. 48 acquired 32 timeframes per cardiac cycle). Reduced temporal resolution means flow waveforms may be more rounded and peak values underestimated. Interpolation and view-sharing 49 methods may be used to increase the resulting temporal resolution of a flow scan, but it is important for researchers to be aware that the effective resolution does not improve using these methods.
Improving spatial resolution and coverage
Scanning the smaller blood vessels of the brain requires high spatial resolution, otherwise fine details are missed and Gibbs artifacts (a ringing effect caused by sharp changes in pixel intensity) and partial volume effects are likely to occur. It is especially important in phase-encoding techniques such as this to avoid or correct for cases in which voxels contain the phases of both blood and stationary tissue 50 ; smaller voxels, therefore, reduce the risk of this occurring. One study suggests an isotropic resolution of 0.5–1.2 mm for a typical 2.5 mm diameter vessel. 26 However, to increase spatial resolution, one must allow for increased scan time, reduced imaging coverage or use of high-field MRI such as 7 T to achieve improved resolution without decreasing the SNR. As spatial resolution improves, so too will our ability to assess the brain’s small perforating blood vessels in vivo and learn more about their breakdown in relation to cerebral SVD.51,52 Smaller pixel size leads to the limiting factor of subject motion becoming more prevalent, meaning motion-compensation techniques will become more important as resolution improves.
To increase coverage and allow the 4D flow acquisition of a wider array of cerebral arteries and veins, radial and spiral undersampling techniques (such as PC-VIPR) are effective. Image techniques with high spatial resolution, such as time-of-flight, may be co-registered with 4D flow magnitude data for better identification and analysis of small vessels. Studies from the past few years have shown that it is possible to acquire high 4D flow isotropic spatial resolutions, for example 0.7 mm in approximately seven minutes 11 and 0.5 mm in only six minutes. 18 This will likely improve over the coming years. Furthermore, the use of advanced, semi-automated flow quantification methods has shown promise in analysing distal arteries. 30
As is the case with temporal resolution, interpolation can increase the spatial resolution of flow images, especially when advanced MR undersampling and reconstruction methods are used. It is important, however, to be aware that the effective spatial resolution is often unchanged in these methods. The need for standardisation, validation and quality assessment is becoming increasingly apparent – ideally utilising phantoms with different vessel sizes, flows and levels of pulsatility so that accuracy, precision and actual temporal and spatial resolutions can be determined.
Extending dynamic velocity range
As previously mentioned, the rigid nature of the velocity-encoding parameter, venc, is a common issue in 4D flow brain imaging – where the problem lies in the considerable differences in blood velocity between vessel types. For example, the relatively high vencs used for arteries can cause venous velocities to appear less conspicuous on an image with reduced SNR due to the large breadth of values between the two. Several studies15,19,26 used a dual-venc technique, allowing the dynamic velocity range within the brain to be represented more accurately. By using two separate venc values in one scan (through the application of an advanced technique known as multipoint velocity encoding), they were able to measure high- and low-flowing vessels effectively – with one study reporting a time reduction of 12.5% compared to two separate 2D PC-MRI scans with individual vencs. 26 Interestingly, one study mentions a desire for using separate high- and low-venc values in their 4D flow research on AD but state that it would have taken too long. 11 An alternative to multiple vencs is to vary the parameter between systole and diastole, for fast and slow flow, respectively. In the future, dual-velocity encoding may allow 4D flow studies to more accurately measure blood flow with less noise.
Several studies demonstrated the use of 4D flow in the context of surgical operations.38,39 These are useful in highlighting and summarising the main concerns in using 4D flow in disease research, and the solutions that will likely address these concerns in the future: including (but not limited to) high-field MRI, advanced acceleration techniques (ideally using correlations in space and time), increased resolution and multi-venc acquisition. A summary of the range of popular imaging parameters used in current, state-of-the-art cerebral 4D flow studies is presented in Figure 4.
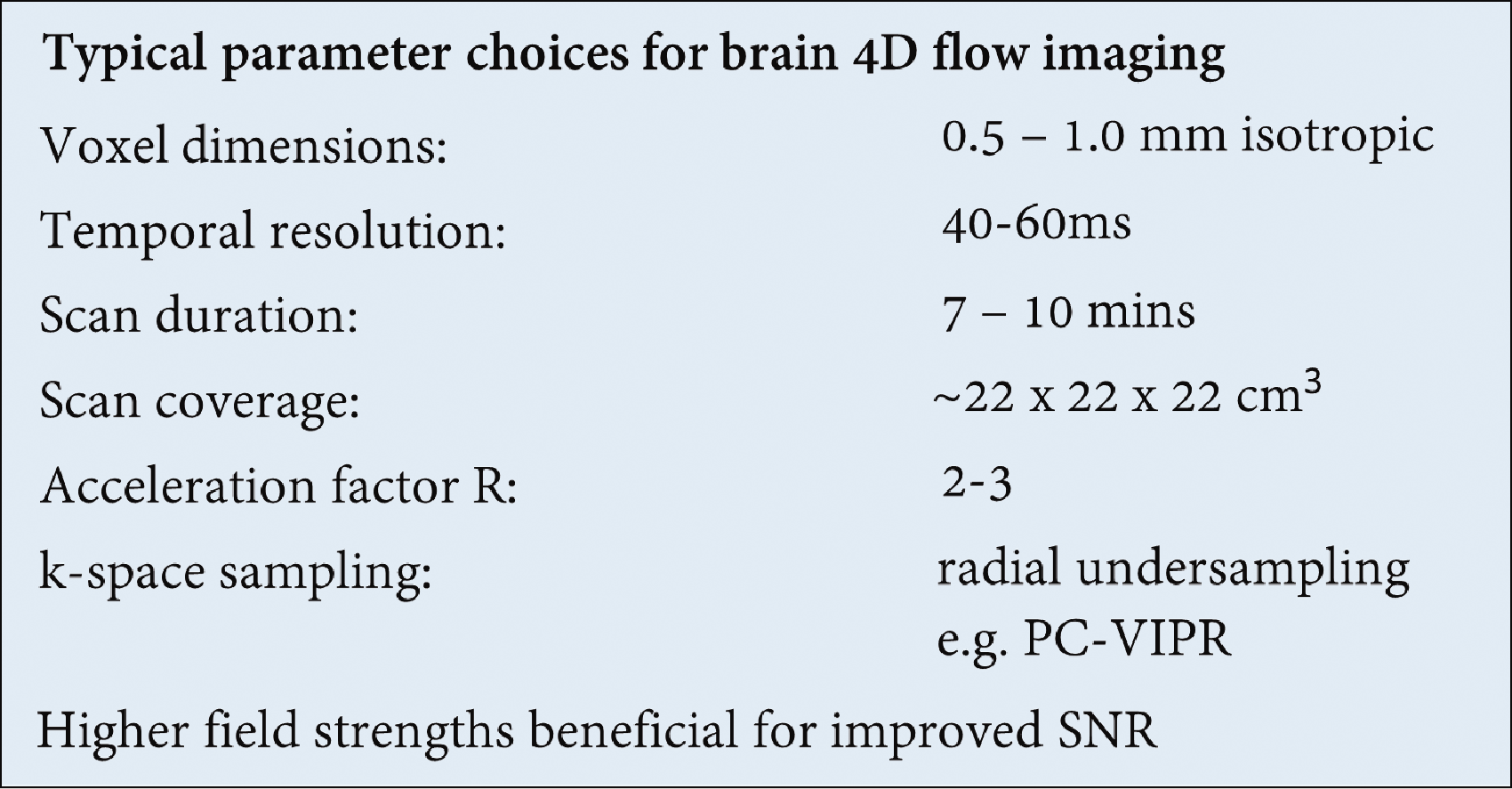
Typical imaging parameters used in recent cerebral 4D flow studies.
Over the past few years, 4D flow brain imaging has been shown to be an effective technique within many contexts. Not only does it possess excellent test–retest multisite reproducibility, 29 but has been used successfully on relatively large samples of elderly, clinically relevant subjects,13,53 and has been used alongside other techniques such as hypoxia-induction to measure cerebrovascular reactivity.54,55 Due to its ability to allow post-hoc quantification of blood flow, pulsatility and pressure changes in anatomically-defined vessels (as distinct from local tissue perfusion) in a non-invasive, low-risk manner, 4D flow arguably aids PC-MRI in filling a niche left by techniques such as arterial spin labelling, catheter angiography and Doppler US.
Conclusion
The studies reviewed here demonstrate the validity of 4D flow when investigating vascular pathologies, as they allow for the visualisation and analysis of 3D blood flow progression through vessels over time, as well as the more complex haemodynamics of disease progression. They also demonstrate the feasibility of scanning relatively large numbers of patients with a neurological disease using this technique, acquiring data that is relatively high resolution with substantial coverage.
The key, and inter-dependent, issues surrounding the technique tend to concern long acquisition times, limited spatial and/or temporal resolution, and limited dynamic velocity range. However, new techniques are rapidly emerging, such as undersampling in both spatial and temporal domains as well as multi-venc acquisition, making 4D flow MRI more feasible for large-scale studies of dementia and neurovascular diseases. The current applications cover a wide range of conditions and subjects, and produce more informative results than the technique’s predecessors. Over the coming years, the trade-off between 4D data quality and acquisition time will likely become less severe and it will earn its place as a relatively fast, yet highly useful, brain imaging technique in more clinical settings as well as research.
Supplemental Material
sj-pdf-1-jcb-10.1177_0271678X20952014 - Supplemental material for 4D flow MRI for non-invasive measurement of blood flow in the brain: A systematic review
Supplemental material, sj-pdf-1-jcb-10.1177_0271678X20952014 for 4D flow MRI for non-invasive measurement of blood flow in the brain: A systematic review by Alasdair G Morgan, Michael J Thrippleton, Joanna M Wardlaw and Ian Marshall in Journal of Cerebral Blood Flow & Metabolism
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: AGM is funded by Medical Research Scotland and Siemens. MJT is funded by NHS Lothian Research and Development Office. We acknowledge support from the Scottish Funding Council and Chief Scientist Office through the Scottish Imaging Network: A Platform for Scientific Excellence (SINAPSE). The work is that of the authors and does not reflect the views of the funders.
Acknowledgements
We gratefully acknowledge Emily Ball for her input and advice on the systematic elements of this review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplementary material for this paper is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.