
Abstract
Disruption of the blood–brain barrier (BBB) might play a role in the pathophysiology of cerebral small vessel disease-related ICH. The aim of this study was to assess presence and extent of contrast agent leakage distant from the hematoma as a marker of BBB disruption in patients with spontaneous ICH. We prospectively performed 7 tesla MRI in adult patients with spontaneous ICH and assessed contrast leakage distant from the hematoma on 3D FLAIR images. Thirty-one patients were included (mean age 60 years, 29% women). Median time between ICH and MRI was 20 days (IQR 9–67 days). Seventeen patients (54%; seven lobar, nine deep, one infratentorial ICH) had contrast leakage, located cortical in 16 and cortical and deep in one patient. Patients with contrast leakage more often had lobar cerebral microbleeds (CMBs; 77%) than those without (36%; RR 2.5, 95% CI 1.1–5.7) and a higher number of lobar CMBs (patients with contrast leakage: median 2, IQR 1–8 versus those without: median 0, IQR 0–2; p = 0.02). This study shows that contrast leakage distant from the hematoma is common in days to weeks after spontaneous ICH. It is located predominantly cortical and related to lobar CMBs and therefore possibly to cerebral amyloid angiopathy.
Keywords
Introduction
Intracerebral hemorrhage (ICH) related to cerebral small vessel disease (cSVD) is a detrimental disease resulting in high case-morbidity and -fatality.1,2 Despite ongoing advances in imaging and supportive treatment, incidence has not declined and outcome after ICH has at most marginally improved.2–4 An important contributing factor may be that the underlying pathophysiology is incompletely understood. cSVD-related ICH is mostly attributed to hypertensive vasculopathy or cerebral amyloid angiopathy (CAA), 5 but the exact sequence of events and mechanisms that lead to vessel rupture remains unknown. Accumulating evidence suggests that disruption of the blood–brain barrier (BBB) plays a role in cSVD-related ICH.6–8
Contrast agent leakage (further referred to as contrast leakage) on dynamic contrast enhanced (DCE) MRI as a biomarker of BBB disruption has been demonstrated in patients with (lacunar) stroke,9–11 mild cognitive impairment and Alzheimer's disease.12,13 Using dedicated fluid-attenuated inversion recovery (FLAIR) sequences after gadolinium contrast agent injection, hyperintense foci can be found in the normal appearing brain parenchyma or cerebrospinal fluid (CSF) space: the so-called Hyperintense Acute Reperfusion Marker (HARM).14–17 In the acute phase after ICH (median interval between ICH and MRI 11 h), HARM was found in 85% of patients. 18 We hypothesized that contrast leakage as a marker of BBB disruption is a marker of the underlying cSVD in patients with ICH. Therefore, we assessed the presence and extent of contrast leakage in normal-appearing brain and CSF distant from the hematoma in patients with spontaneous ICH on 7 tesla (T) MRI in the subacute phase after ICH. Additionally, we related the presence and extent of contrast leakage to classical markers of cSVD.
Materials and methods
Study population
Patients were enrolled from an ongoing multicenter prospective observational cohort study in the Netherlands, the Finding the ETiology in spontaneous Cerebral Hemorrhage (FETCH) study. In this study, we included 31 consecutive adult patients who presented to the University Medical Centers of Utrecht, Leiden or Nijmegen, since 1 October 2013, with spontaneous ICH confirmed by computed tomography (CT) and were able to undergo 3 T and/or 7 T MR imaging. Patients with a known cause of ICH, such as a vascular malformation, tumor or trauma, are excluded. For this study, we included all patients who underwent 7 T MRI with a gadolinium-containing contrast agent within three months of the ICH.
The FETCH study was approved by the Medical Ethics Review Committee of the University Medical Center Utrecht, and by all participating centers. Each patient gave written informed consent for participation in the study. The guidelines according to the Declaration of Helsinki were followed.
We categorized the ICH according to location as lobar, deep or infratentorial. Patients with possible or probable CAA were identified using the modified Boston criteria. 19 Hypertension was defined as use of antihypertensive medication, a systolic blood pressure greater than 140 mm Hg, a diastolic blood pressure greater than 90 mm Hg on two documented independent measurements prior to the ICH or left ventricular hypertrophy on ECG.
Imaging protocol and analysis
On admission CT, we assessed hematoma volume using an in-house developed tool, 20 and ICH location. Lobar ICH was defined as ICH isolated to the cortex (with or without involvement of subcortical white matter) and non-lobar ICH as deep (thalamus and basal ganglia) or infratentorial (brainstem and cerebellum) ICH. We used 7 T MRI to assess presence of contrast leakage, CMBs and white matter hyperintensities (WMH). Presence of enlarged perivascular spaces (EPVS) and diffusion weighted imaging (DWI) lesions was assessed on 3 T MRI.
7 T MRI (Philips, Best, The Netherlands) scans were acquired by a standardized protocol; 3D T2-weighted (repetition time (TR)/equivalent echo time (TE) = 3158/60 ms; voxel size = acquired: 0.70 × 0.70 × 0.70 mm3, reconstructed: 0.35 × 0.35 × 0.35 mm3), 3D T1-weighted (TR/TE = 4.8/2.2 ms; voxel size = acquired: 1.00 × 1.01 × 1.00 mm3, reconstructed: 0.66 × 0.66 × 0.50 mm3), dual echo 3D T2*-weighted (TR/first TE/second TE = 20/6.9/15.8 ms; voxel size = acquired: 0.50 × 0.50 × 0.70 mm3, reconstructed: 0.39 × 0.39 × 0.35 mm3) and 3D FLAIR images were acquired (TR/TE/inversion time (TI) = 8000/300/2325 ms; voxel size = acquired: 0.80 × 0.82 × 0.80 mm3, reconstructed: 0.49 × 0.49 × 0.40 mm3). A gadolinium-containing contrast agent was administered in a single intravenous injection of 0.1 mL Gadovist/kg body weight with a maximum of 10 mL Gadovist or 0.2 mL Dotarem/kg body weight with a maximum of 30 mL Dotarem. Postgadolinium FLAIR images were acquired at least 10 min after contrast injection.
3 T unenhanced MRI (Philips, Best, The Netherlands) scans were acquired by a standardized protocol including DWI with apparent diffusion coefficient (ADC) map, an axial T2*, T2-proton density-weighted sequence, inversion recovery and FLAIR, all with 48 contiguous slices and 0.96 × 0.95 × 3.00 mm3 voxels. Also, a 3D T1-weighted sequence was acquired.
Contrast leakage, CMBs, EPVS, WMH and DWI lesions were annotated by two trained readers (WMTJ and AL) independently and blinded for patient information. Discrepancies were resolved in a consensus meeting with an experienced neuroradiologist (JH) and neurologist (CJMK). Contrast leakage was defined as a hyperintense signal in normal-appearing brain or CSF on delayed postgadolinium FLAIR images, while absent on precontrast images. The signal had to be visually distinct and anatomically non-contiguous with the hematoma. We used the 5-point HARM rating scale to rate the extent of the contrast leakage as HARM 0: no contrast leakage, HARM 1: punctate lesions of contrast leakage, HARM 2: multiple punctate lesions of contrast leakage, HARM 3: focal sulcal contrast enhancement, and HARM 4: bilateral and diffuse contrast leakage. 18 CMBs were rated in accordance with the Standards for Reporting Vascular changes on nEuroimaging (STRIVE) definitions and the Microbleed Anatomical Rating Scale,21,22 and WMH by the Fazekas rating scale. 23 DWI lesions were defined as small, hyperintense lesions on DWI with low intensity in the corresponding region on ADC maps remote from ICH and the area of perihematomal edema. 24 EPVS were rated in basal ganglia and centrum semiovale regions on axial T2-weighted sequences using a validated rating scale.25,26
Statistical analysis
We used the Student t-test, χ 2 test, Mann-Whitney U test and logistic regression, as appropriate, to analyze group differences in presence, frequency and distribution of baseline characteristics, CMBs (presence (yes/no) and number of CMBs), DWI lesions (yes/no), categories of EPVS in basal ganglia and centrum semiovale (0: no EPVS, 1: 1–10, 2: 11–20, 3: 21–40, 4: > 40 EPVS) and WMH (Fazekas ≥ 2 vs. < 2) between patients with and without contrast leakage on 7 T MRI.
Results
Baseline characteristics of patients with and without contrast leakage.
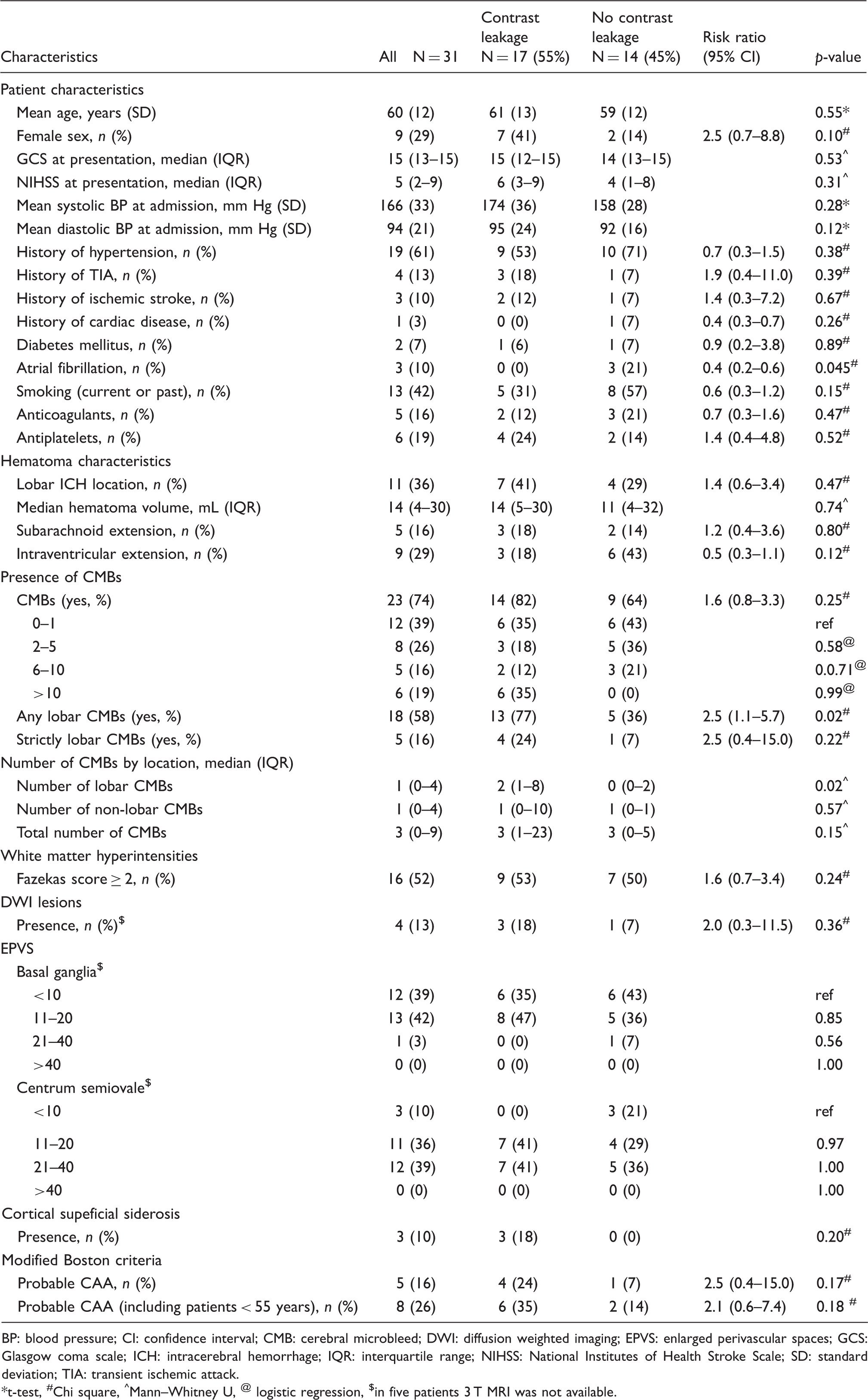
BP: blood pressure; CI: confidence interval; CMB: cerebral microbleed; DWI: diffusion weighted imaging; EPVS: enlarged perivascular spaces; GCS: Glasgow coma scale; ICH: intracerebral hemorrhage; IQR: interquartile range; NIHSS: National Institutes of Health Stroke Scale; SD: standard deviation; TIA: transient ischemic attack.
*t-test, #Chi square, ^Mann–Whitney U, @ logistic regression, $in five patients 3 T MRI was not available.
In 17 patients (54%; seven with lobar, nine with deep, and one with infratentorial ICH), postgadolinium FLAIR images showed contrast leakage distant from the hematoma. Contrast leakage most frequently occurred in a cortical location (16 patients, 94%), rarely deep (1 patient had both cortical and deep contrast leakage, 6%), and never infratentorial. Nine patients (53%) had contrast enhancement in both hemispheres, two (12%) in the symptomatic hemisphere only, and six (35%) in the contralateral hemisphere only. One patient with a cerebellar ICH had supratentorial contrast enhancement in both hemispheres. Four patients (24%) had a punctate lesion of contrast leakage (HARM 1), five patients (29%) multiple punctate lesions of contrast leakage (HARM 2), three patients (18%) showed focal sulcal contrast enhancement (HARM 3) and five patients (29%) bilateral and diffuse contrast leakage (HARM 4). Illustrative examples of patients with different HARM scale scores are provided in Figure 1.
Examples of patients with different HARM scale scores.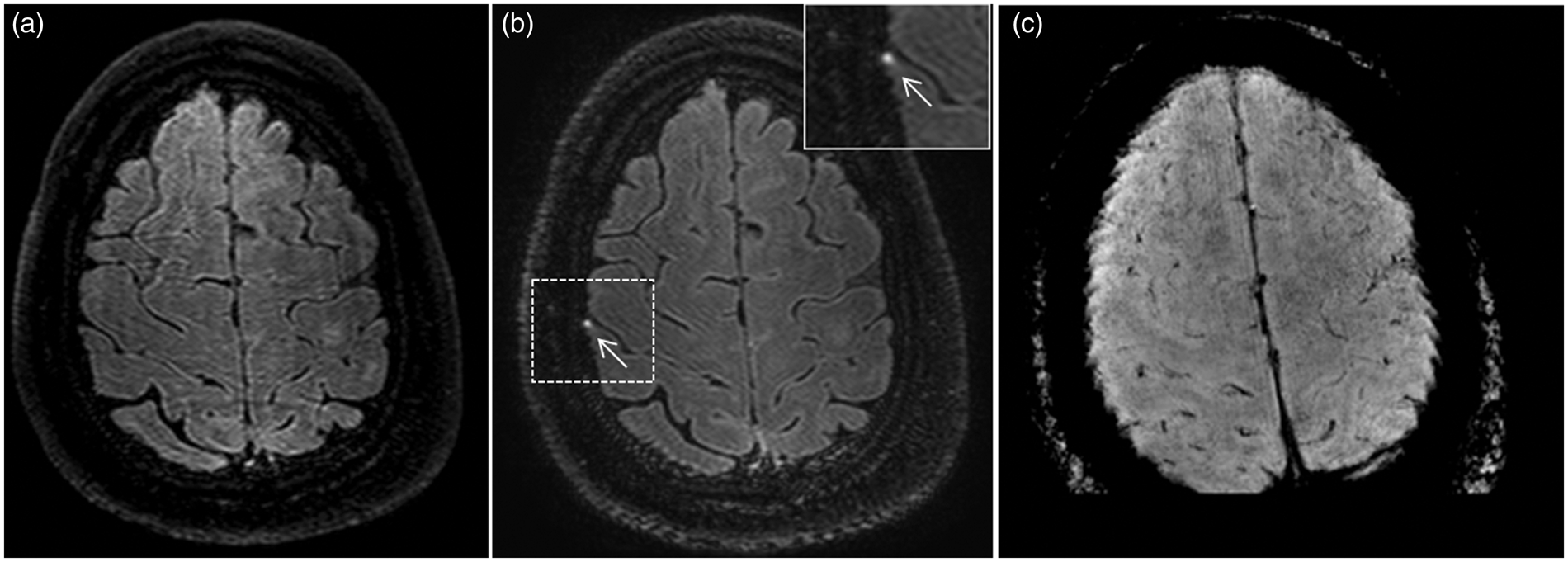
Among the patients with contrast leakage, there was a relatively high proportion of women (0.41; risk ratio (RR) 2.5 (95% confidence interval (CI) 0.7–8.8)), a low proportion of patients with a history of atrial fibrillation (0; RR 0.4 (95% CI 0.2–0.6)) and a high mean diastolic blood pressure at admission (95 mm Hg; p = 0.12), although these differences were not all statistically significant. All other patient characteristics were comparable in patients with and without contrast leakage (Table 1). There was no difference in time interval between ICH and 7 T MRI in patients with (median 20 days; IQR 11–70 days) and without (median 22 days; IQR 5–67 days) contrast leakage (p = 0.55).
Patients with contrast leakage more often had lobar CMBs (77%) than those without contrast leakage (36%; RR 2.5 (95% CI 1.1–5.7, Table 1)) as well as a higher number of lobar CMBs (patients with contrast leakage: median 2, IQR 1–8 versus those without contrast leakage: median 0, IQR 0–2; p = 0.02, Table 1). Seven out of 17 patients with contrast leakage had a lobar ICH of which five fulfilled the modified Boston criteria for probable (n = 4) or possible CAA (n = 1). The other two patients (44 and 51 years old) with lobar ICH had lobar CMBs or superficial siderosis but did not fulfill the modified Boston criteria for probable CAA, because they were younger than 55 years. We found no differences between patients with and without contrast leakage in the proportion of patients with Fazekas score ≥2, categories of EPVS or the proportion of patients with DWI lesions (Table 1). We found no spatial relationship between the location of the DWI lesions and the location of the contrast leakage.
Discussion
This study shows that over 50% of the patients with spontaneous ICH have contrast leakage distant from the hematoma as evidenced by high field 7 T MRI in the subacute phase, up to 70 days after ICH. It occurs both in patients with lobar and in those with deep and infratentorial ICH, with a predominantly cortical location. In half of the patients, contrast leakage is moderate or severe (HARM 3 and 4) and presence of contrast leakage is associated with presence and number of lobar CMBs.
The proportion of patients with contrast leakage in our cohort (54%) is higher than that in a recent study using 3 T MRI delayed postgadolinium FLAIR images in healthy elderly subjects (mean age 73 years; 19% with contrast leakage), in patients with mild cognitive impairment (mean age 69 years; 30%) and in patients with Alzheimer's disease (mean age 72 years; 40%). 14 In a retrospective cohort study of 46 spontaneous ICH patients, contrast leakage was found distant from the hematoma in 85% of patients with conventional 1.5 T and 3 T MRI performed in the acute phase (median 11 hours) after hemorrhage onset. 18 In that study, a possible but not significant association was found with a higher National Institutes of Health Stroke Scale score (NIHSS) at baseline and shorter time to MRI. Location of the hematoma, however, was not reported in that study. Our patients were scanned in the subacute phase (median 20 days), which may explain the smaller proportion of patients with contrast enhancement, despite higher field MRI. The smaller proportion in our study might also be explained by another potential mechanism of the BBB disruption. In the acute study, the BBB disruption may be due to direct injury of the hematoma. 18 The persisting contrast leakage that we found might still be related to the direct effect of the hematoma but could also be an indicator of BBB disruption as a result of cSVD. 27 A previous study described contrast leakage in 2 of 19 patients with probable CAA, presenting with either atypical or multiple hemorrhages or superficial siderosis, on postgadolinium T1-weighted sequences on 1.5 T MRI. 28 That study did not report the time interval between symptom onset and MRI. In 51 patients with lacunar stroke who underwent MRI in the subacute phase (mean 64 days, SD±12), BBB permeability was present more generalized in most of the sulci and EPVS, in contrast to the areas of focal enhancement in our study of ICH patients. In that study, BBB permeability was visualized using pre- and postgadolinium T1-weighted MR sequences and two image processing methods. 9
We found no association of contrast leakage with DWI lesions on 3 T MRI. A possible explanation might be the variable time interval between 3 T and 7 T MRI with a median time interval of 7 days (IQR 1–56 days), and DWI lesions may start to disappear after approximately 7 to 10 days. 29
The results of our study suggest that increased permeability of the BBB might play a role in cSVD-related ICH, in particular in the presence of lobar CMBs. A potential mechanism explaining contrast leakage is the cascade of events that follow the direct injury and mass effect of ICH, consisting of a release of clot-derived factors, cortical spreading depression and an inflammatory response, including leukocyte infiltration, microglia activation, cytokine and chemokine elevation and glutamate neurotoxicity. These lead to additional brain injury and BBB disruption, supporting the hypothesis that contrast leakage may be a consequence of ICH.1,30–36 This might also explain why contrast leakage can be found in a different lobe than the hematoma or the contralateral hemisphere.
Another hypothesis based on animal studies is that BBB disruption may in fact precede ICH.37,38 This hypothesis is supported by our previous observation of a patient with multiple lobar ICHs who showed focal contrast enhancement before appearance of a CMB exactly at the site of that contrast enhancement. 39 As we assessed patients only after they had experienced the ICH, our study cannot draw conclusions on causal inference. MRI contrast leakage indicative of BBB disruption may be another marker of the underlying cSVD pathology next to the ICH and classic MRI markers of cSVD, including WMH, lacunes, EPVS, CMBs, recent small subcortical infarcts and brain atrophy. 21 To date, it remains unclear why in some patients cSVD manifests as ischemia, whereas in others cSVD causes hemorrhage. Even in the cSVD that is related to hypertension and not CAA, some patients appear to be more prone to hemorrhage than others as suggested by the fact that new CMBs are found more frequently in those who already had CMBs before, than in those who did not.40–42
We found contrast leakage predominantly cortical, even in patients with deep ICH. A potential explanation is that hypertensive vasculopathy not only affects the deep penetrating vessels but also the superficial cortical vessels or that it affects deep penetrating vessels in a different way than superficial cortical vessels. 43 Also, it could be that patients with non-lobar ICH have CAA in addition to hypertensive vasculopathy (for example HARM score 4 in Figure 1). 44 Other studies describe that contrast leakage or BBB disruption might be caused by cortical spreading depression.31,45–48 The association of contrast leakage with lobar CMBs and that four of the five patients in our study with probable CAA according to the modified Boston criteria had contrast leakage, tentatively supports a relation with CAA. The predilection of contrast leakage in cortical rather than deep areas was also found by others in cognitive healthy elderly subjects, and in patients with mild cognitive impairment or Alzheimer's disease and ischemic stroke.14–16,18,49,50
We found no association with other cSVD markers than CMBs (i.e. DWI lesions, EPVS and WMH). In a previous cohort of ICH patients, there was also no association of contrast leakage with WMH. 18 In the study in cognitively healthy elderly patients, patients with mild cognitive impairment and Alzheimer's disease, there was also no association of contrast leakage with lacunes or WMH. 14 This might indicate that contrast leakage is a marker independent of other cSVD features, and possibly be particularly associated with CAA.
Strengths of our study are that we were able to prospectively collect patients with spontaneous ICH from multiple centers and assess these patients in the 7 T MRI scanner in the subacute stage of ICH. Another strength is that 7 T MRI has a high signal-to-noise ratio with also better contrast-to-noise in FLAIR images than conventional MRI scanners. This allows the use of voxel sizes less than a millimeter and consequently the possibility of a better yield by being able to detect small punctate lesions of contrast leakage, including in deeper areas. 51 We used FLAIR images instead of T1-weighted images, because this MR sequence has a better sensitivity in detecting low concentrations of Gadolinium.14,52,53 Furthermore, FLAIR images are less sensitive to the effects of gadolinium contrast in the blood vessels, because of a stronger signal decay due to the effects of blood flow in combination with shortening of the T2 relaxation time at higher concentrations of gadolinium.14,54 Postgadolinium FLAIR enhancement on 3 T MRI is a novel technique which has also been used in cranial nerve imaging for identifying both normal and abnormal cranial nerves.55–57
Our study also has limitations. First, the sample size was small. Second, including severely affected ICH patient for 7 T MR imaging is challenging and this may have resulted in a selection bias in that we included less affected patients with smaller hematomas and a relatively lower NIHSS scores. Third, assessing contrast leakage on postgadolinium FLAIR images may be more rater dependent than techniques such as DCE-MRI and cannot be used to quantify the amount of leakage. Fourth, raters were not blinded for ICH location which might have included detection bias. Finally, there was variation in time interval between ICH and MRI between patients. As the median time interval was similar between patients with and without contrast leakage, this will not have affected the analyses of different cSVD markers in these groups.
Our findings need confirmation, preferably in a larger cohort of ICH patients with and without CAA. Furthermore, it would be of interest to study the relation between contrast leakage and outcome. Also, sequential scanning of patients with contrast leakage to follow changes in contrast enhancement over time would be of interest. Further work is needed to determine whether FLAIR contrast enhancement, as a biomarker of BBB disruption, is able to predict recurrent ICH or cognitive deterioration. 21
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Klijn is supported by a clinical established investigator grant of the Dutch Heart Foundation (Grant Number 2012T077) and an ASPASIA grant from The Netherlands Organisation for Health Research and Development, ZonMw (grant number 015008048)
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors' contributions
Wilmar MT Jolink: study concept and design, acquisition of data, rating images, interpretation of the results, drafting the manuscript. Arjen Lindenholz: rating images, interpretation of the results, critical revisions. Ellis S van Etten: acquisition of data, critical revisions. Koen M van Nieuwenhuizen: acquisition of data, critical revisions. Floris HBM Schreuder: acquisition of data, critical revisions. Hugo J Kuijf: imaging analysis, critical revisions, Matthias JP van Osch: acquisition of data, critical revisions. Jeroen Hendrikse: rating images, critical revisions. Gabriel JE Rinkel: interpretation of the results, critical revisions. Marieke JH Wermer: interpretation of the results, critical revisions. Catharina JM Klijn: study concept and design, rating images, interpretation of the results, critical revisions.