
Abstract
Comorbidities are a hallmark of stroke that both increase the incidence of stroke and worsen outcome. Hypertension is prevalent in the stroke population and the most important modifiable risk factor for stroke. Hypertensive disorders promote stroke through increased shear stress, endothelial dysfunction, and large artery stiffness that transmits pulsatile flow to the cerebral microcirculation. Hypertension also promotes cerebral small vessel disease through several mechanisms, including hypoperfusion, diminished autoregulatory capacity and localized increase in blood–brain barrier permeability. Preeclampsia, a hypertensive disorder of pregnancy, also increases the risk of stroke 4–5-fold compared to normal pregnancy that predisposes women to early-onset cognitive impairment. In this review, we highlight how comorbidities and concomitant disorders are not only risk factors for ischemic stroke, but alter the response to acute ischemia. We focus on hypertension as a comorbidity and its effects on the cerebral circulation that alters the pathophysiology of ischemic stroke and should be considered in guiding future therapeutic strategies.
Introduction
Stroke is a highly heterogeneous condition that occurs in all demographics. Unlike pediatric stroke, ischemic stroke in the adult is predominantly a disorder of comorbidities (e.g. hypertension, diabetes mellitus, hyperlipidemia) and/or altered coagulation states (e.g. pregnancy and preeclampsia). Stroke is the leading cause of long-term disability in the United States and is currently the 5th leading cause of death.1–4 The decline in stroke mortality over the last decade can be partly attributed to the aggressive treatment of hypertension and dyslipidemia that is common in the stroke population.3,5 In fact, hypertension is the most important modifiable risk factor for all types of stroke. The incidence of stroke increases proportionally with both systolic and diastolic pressure, increasing the relative risk 3.1-fold for men and 2.9-fold for women.6,7 Blood pressure also increases in the acute phase of stroke, through unexplained mechanisms, fueling clinical controversy over whether or not and to what extent it should be treated.
Hypertension also worsens stroke outcome. Patients with pre-existing hypertension have small amounts of salvageable tissue (penumbra) and larger infarctions compared to normotensive patients, although lower blood pressure is also detrimental in stroke.8–11 The risk of stroke in the setting of hypertension is also far-reaching. Hypertension is a primary driver of cerebral small vessel disease (CSVD) that leads to cognitive decline and lacunar stroke. In addition, recent studies have shown that in women with prior preeclampsia, a common hypertensive disorder of pregnancy, the long-term risk of stroke is increased 4–5-fold.12–14 The impact of hypertension on the cerebral circulation is therefore of profound importance to the stroke field.
Studies in animal models have demonstrated striking effects of hypertension on the cerebral circulation and have been invaluable in helping to understand the disease process that leads to increased small and large vessel disease risk and worsened outcome from stroke. Inward remodeling of small and large arteries decreases lumen diameters and vasodilatory reserve that if prolonged can cause hypoperfusion and hemodynamic compromise.15,16 Repeated mechanical stress during hypertension and degradation of elastin fibers in the vascular wall stiffens large arteries and transmits the pulsatile load downstream into the brain parenchyma.17,18 Endothelial dysfunction and diminished nitric oxide (NO) are also associated with hypertension that has negative consequences for the brain, including increasing cerebrovascular resistance (CVR) and diminished autoregulatory capacity. 19 In addition, hypertension increases shear stress on the vascular endothelium – the force per unit area created when blood flows over the endothelium. Shear stress is directly related to the velocity of blood flow and viscosity, and inversely proportional to the cube of arterial radius. 20 Under normal conditions, increased shear stress causes an adaptive vasodilatory response through increased NO production that serves to normalize shear stress.20–22 However, under hypertensive conditions that impair NO, the adaptive response to high shear stress is impaired, leading to endothelial damage and upregulation of atherogenic genes.20–22 Thus, increased shear stress on the cerebral endothelium during hypertension causes atheroma formation and subsequent atherosclerosis, an important underlying risk factor for large and small vessel occlusion.23,24 This review highlights basic, clinical and translational studies on the impact of hypertension on the cerebral circulation and how structural and functional alterations of cerebral vessels during hypertension promote stroke and stroke injury. Using hypertension as an example, we underscore how comorbidities or concomitant disorders are not solely risk factors for ischemic stroke, but affect the cerebral circulation that alters the response to acute ischemia. Consideration of these myriad effects on the pathophysiology of ischemic stroke may be instrumental in guiding future therapeutic strategies.
Cerebral blood flow autoregulation
The brain is an organ that regulates cerebral blood flow very effectively in the face of perfusion pressure fluctuations, a response that importantly enables the brain to match its metabolic demand to the blood supply. 25 Autoregulation of cerebral blood flow was first described by Lassen 26 in 1959 after analyzing a number of studies in the human in which cerebral blood flow was measured in response to altering blood pressure using hypotensive medication, tilting head-up, inhalation of carbon dioxide, sympathectomy or adrenalectomy mainly in hypertensive subjects. Lassen found that relatively constant cerebral blood flow could be maintained at systemic blood pressure between approximately 60 to 160 mm Hg. 2 Similar cerebral blood flow autoregulation values have been reported in many other species, including dogs, 27 baboons, 28 monkeys, 29 cats, 30 lambs, 31 pigs, 32 rabbits, 33 rats 34 and mice. 35 Above and below these limits, autoregulation is impaired and cerebral blood flow becomes dependent on arterial pressure in a linear fashion. When blood pressure is not within the limits of autoregulation, or autoregulation is impaired, there is considerable risk of brain injury. For example, when cerebral perfusion pressure falls below the lower limit of autoregulation, cerebral ischemia ensues that can cause permanent injury.36–38
The impact of chronic hypertension on the cerebral blood flow autoregulation was first reported in 1973 by Strandgaard et al.
39
in a group of patients with essential hypertension. This study showed that both the upper and the lower limits of the cerebral blood flow autoregulation curve were shifted to the higher pressures when compared to normotensive humans.
38
In rat models of renal and spontaneous hypertension, similar shift of both limits of the cerebral blood flow autoregulation curves was found.39–42 Harper and Bohlen
41
used hemorrhagic hypotension and phenylephrine infusion to decrease and increase blood pressure, respectively, in spontaneously hypertensive rats (SHRs) and normotensive Wistar-Kyoto rats (WKY) to show the range of cerebral blood flow autoregulation increased from ∼60 to 150 mm Hg in WKY to ∼110 to 200 mm Hg in SHR. Figure 1 shows how the CBF autoregulatory curve is shifted to higher pressures in hypertension. Importantly, the shift in the autoregulatory curve to higher pressures is thought to be protective of the brain during chronic hypertension by limiting the damaging effects of high blood pressure to the downstream microcirculation. However, a shift in the lower threshold to higher pressures can be detrimental during acute hypotension in which the ability to maintain constant cerebral blood flow is diminished and therefore increases the susceptibility of ischemic injury. Interestingly, attempts have been made to normalize cerebral blood flow autoregulation during chronic hypertension, mostly in SHR. Long-term antihypertensive treatment with a vasodilator (budralazine) for nine weeks normalized the upper but not the lower limit of cerebral blood flow autoregulation in SHR.
43
The calcium channel blocker benidipine treatment for eight days normalized both upper and lower limits of cerebral blood flow autoregulation in SHR.
44
Acute angiotensin-converting enzyme (ACE) inhibitor captopril
45
and both acute and longer-term (3–14 days) angiotensin type 1 receptor (AT1R) blocker candesartan45,46 also provided normalization of both the upper and lower thresholds of cerebral blood flow autoregulation in SHR.
Graph showing curve of cerebral blood flow autoregulation in hypertensive SHR (closed circle) compared to normotensive WKY (open circle).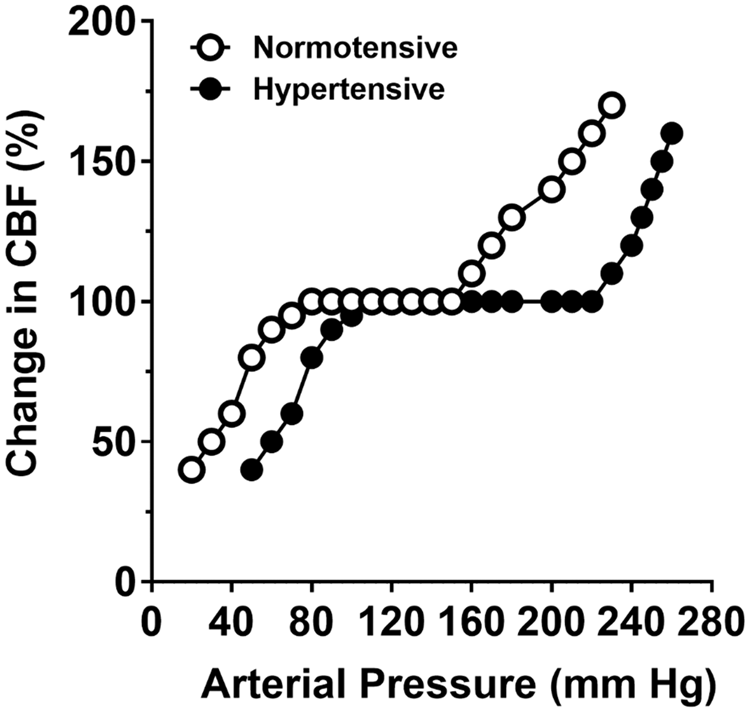
Ischemic stroke can impair cerebral blood flow autoregulation that is associated with worsened outcome. Early studies using radioisotope injection into the carotid artery found that autoregulation was impaired in the ipsilateral hemisphere; however, distinction between core infarction and penumbra was not made.47–49 More recent studies using transcranial Doppler to assess small fluctuations in blood pressure found that in patients with large ischemic strokes, autoregulation was significantly altered.50,51 In addition, patients with impaired autoregulation had worse clinical outcome than those with intact autoregulation.50,51 Other studies have shown little to no effect of stroke on cerebral blood flow autoregulation. Using single-photon emission computed tomography and repeated cerebral blood flow measurements after decreasing blood pressure with nimodipine, there was no change in cerebral blood flow, suggesting intact autoregulation. 52 However, it is worth noting that substantially changing blood pressure in humans is difficult, and potentially dangerous especially in stroke patients. Therefore, defining the upper and lower limits of autoregulation and/or how effective it is in patients with existing brain injury is complex and risky. In addition, despite a plethora of animal studies defining autoregulation of CBF, there are only limited data in ischemic stroke patients for this reason.
Cerebral blood flow autoregulation is facilitated by changes in diameter of resistance blood vessels, leading to changes in vascular resistance and hence cerebral blood flow. Large artery resistance in the brain is high and therefore both large and small vessels participate in the autoregulation of cerebral blood flow. 53 There may be several mechanisms by which ischemic stroke affects autoregulation of cerebral blood flow, including derangements in neuronal activation due to ischemic injury, biproducts of altered metabolism that are vasoactive and/or cause vascular dysfunction in response to ischemia and reperfusion. All brain blood vessels seem to have some degree of myogenic tone, which is tonic basal constriction to intraluminal pressure. Our own studies have shown that myogenic tone of middle cerebral arteries was decreased at post-ischemic reperfusion with the longer duration of ischemia, the greater loss of tone. 54 As the myogenic response is a primary mechanism of autoregulation, 55 the loss of tone in the MCA could contribute to impaired autoregulation during stroke. On the contrary, post-ischemic reperfusion caused an increase in tone in intraparenchymal arterioles, 56 demonstrating the significant heterogeneity in vascular segments in the brain and the response to ischemia and reperfusion.
Structural remodeling during hypertension
One of the most important consequences of chronic hypertension is its effect on cerebral arteries and arterioles that increases CVR and causes hypoperfusion of the brain.15,16 Increased tone and structurally smaller lumens of pial vessels during hypertension are well-documented.57–61 These vascular changes associated with chronic hypertension increase the severity and extent of hypoperfusion and decrease the amount of penumbral tissue during ischemic stroke.62–66 Thus, understanding mechanisms by which chronic hypertension affects vascular function is important for stroke outcome as well as chronic hypoperfusion that can lead to stroke and cognitive decline.
Chronic hypertension causes profound changes in the cerebral circulation that impacts cerebral blood flow, one of them being structural remodeling. Both hypertrophy and inward remodeling of cerebral arteries and arterioles are commonly observed in the cerebral circulation of animal models of hypertension, mostly in SHR and stroke-prone SHR (SHRSP). Hypertrophy of the vessel wall is defined as increased wall thickness, increased wall cross-sectional areas, or increased wall-to-lumen ratio. 67 Inward remodeling, on the other hand, was first defined as smaller external diameter in cerebral arterioles by Baumbach and Heistad in 1989. 68 Later inward remodeling was re-defined and standardized as smaller lumen diameter, which is more important in the context of vascular resistance because lumen diameter is the most important determinant of resistance to flow. 67 Hypertension-induced hypertrophy and inward remodeling are considered protective and also detrimental in cerebral arterioles. Law of LaPlace describes wall tension in a thinned-wall cylindrical vessel by the formula: wall tension = intraluminal pressure × radius and therefore wall stress is wall tension/wall thickness. In this relationship, increased intraluminal pressure, as seen in chronic hypertension, increases wall tension and wall stress. Blood vessels can therefore normalize wall tension and wall stress by decreasing the radius and increasing wall thickness, respectively. In the brain circulation, it has been shown that cerebral arterioles in SHRSP underwent reduced radius (inward remodeling) and increased wall thickness (wall hypertrophy).68,69 Normalized wall tension and wall stress are believed to protect against damaging effect of hypertension on the wall of cerebral vasculature. On the other hand, hypertrophy and inward remodeling of cerebral arteries and arterioles limits vasodilator reserve, i.e. the capacity of the vessel to dilate. In addition, vessel wall hypertrophy of cerebral arteries and arterioles increases the contractile smooth muscle mass and therefore enhances vasoconstrictor responsiveness.70,71 Inward remodeling also reduces maximum diameter of cerebral arterioles during chronic hypertension and therefore reduces the capacity to dilate during acute hypotension. 72
The underlying mechanisms of hypertension-induced hypertrophy and inward remodeling in cerebral arterioles have been extensively studied. Strong evidence now suggests that increased angiotensin II (Ang II) in hypertension, and not hypertension itself, is the main determinant of inward remodeling in cerebral arteries and arterioles, based on a number of observations. First, low-dose use of the ACE-inhibitor perindopril inhibited inward remodeling in SHRSP equally effective when compared to high-dose perindopril although low-dose perindopril was only half as effective as high dose in reducing blood pressure. 73 Second, the beta-adrenergic receptor blocker propranolol did not attenuate inward remodeling although it was as effective as low-dose perindopril in reducing blood pressure in SHRSP. 73 Third, low- and high-dose Ang II infusion for 28 days in mice was equally effective in producing inward remodeling in cerebral arterioles although low-dose Ang II did not significantly increase blood pressure. 74 Fourth, treatment with indapamide, a thiazide-like diuretic, reduced blood pressure in SHR but failed to attenuate inward remodeling in cerebral arterioles. 75 Further mechanistic studies using a high-dose Ang II infusion model in transgenic knockout (KO) mice showed that caveolin-1-mediated activation of matrix metalloproteinase-9 was responsible for inward remodeling of cerebral arterioles. 76
Vasoconstrictor stimuli during hypertension
In addition to structural remodeling that limits the vasodilatory capacity of cerebral arteries and arterioles, reactivity to a number of vasoactive agents is different in SHRSP compared to WKY. For example, cerebral arterioles dilate to serotonin in WKY but constrict in SHRSP. 77 In addition, constriction of cerebral arterioles to norepinephrine is significantly greater in SHR compared to WKY. 70 These results suggest that increased constriction in cerebral arterioles during chronic hypertension may be partly related to increased sympathetic nerve density and/or catecholamine outflow. 78 On the other hand, dilation of cerebral arterioles to vasodilators is impaired in SHRSP versus WKY, including adenosine diphosphate, 77 acetylcholine, 79 bradykinin and calcium ionophore A23187. 80 These results are indicative of endothelial dysfunction in cerebral arteries and arterioles in chronic hypertension that may be related to reduced NO, 81 increased oxidative stress81,82 and/or reduced prostaglandins productions. 83
Ang II
The renin-angiotensin system (RAS) has an important role in the pathophysiology of hypertension. Ang II is the primary hormone of the RAS that is elevated in the circulation and brain in most forms of hypertension and has been implicated as the major cause of oxidative stress, endothelial dysfunction and increased tone in cerebral arteries mainly through the actions of AT1R activation.84–89 AT1R activation increases oxidative stress through increased nicotinamide adenine dinucleotide phosphate (NADPH) oxidase activity, a major producer of superoxide (O2−) that causes vasoconstriction and endothelial dysfunction.88,89 The effect of Ang II on the cerebral circulation has been reviewed in detail by De Silva and Faraci. 90 Importantly, O2− production in response to Ang II was shown to be decreased by AT1R blockers.91–93 Interestingly, there appear to be sex differences in the response to AngII. Ang II-treated male mice deficient in manganese superoxide dismutase (MnSOD) had significant endothelial dysfunction in cerebral arteries, whereas female mice were unaffected, suggesting females are protected from the detrimental effects of Ang II. 94
AT1R blockade has also been shown to improve stroke outcome in hypertensive animals and reduce ischemic stroke severity in humans.95–100 The detrimental effect of AT1R activation in stroke was also demonstrated by studies showing reduced infarction in mice genetically deficient in the AT1R (AT1aR−/−) and increased in mice with Ang II infusion.97–99 The beneficial effects of AT1R blockade on ischemic stroke are not necessarily due to its antihypertensive effects as the same effect was not seen in which blood pressure was lowered through other means (hydralazine or nimodipine), or was not decreased by treatment.100–102 In fact, the mechanism by which AT1R blockade is beneficial to stroke outcome is likely multifactorial. AT1R inhibition was shown to decrease stroke-induced upregulation of brain Ang II and matrix metalloproteinase activation in normotensive rats, suggesting one means by which AT1R inhibition improves outcome may be by preventing edema formation and hemorrhagic transformation. 100 In hypertensive animals, AT1R blockade administered 3 h and 24 h after ischemia reduced infarct size and was associated with decreased Rho-kinase activation that was shown to be increased in cerebral microvessels.102,103 In a head-to-head comparison of AT1R blockade with telmisartan vs. ACE inhibition with Ramipril or the combination of the two given to spontaneously hypertensive stroke-prone rats (SHRSP), both had beneficial effects on stroke incidence and survival, but only telmisartan or the combination of telmisartan and Ramipril improved neurological outcome after acute middle cerebral artery occlusion (MCAO). 104 These results demonstrate that decreasing blood pressure can lower stroke incidence and enhance survival, but that AT1R blockade is most beneficial for stroke outcome, likely through its effect on preventing NADPH oxidase-induced O2− production.
Endothelin
Endothelin-1 (ET-1) is a potent vasoconstrictor peptide synthesized and released mostly by endothelial cells in the cerebral vasculature. 105 ET-1 regulates vascular tone through the activation of two specific receptor subtypes, ETA and ETB receptors. 106 Under physiological conditions, there is a balance between the vasoconstrictor effect induced by ETA receptors on vascular smooth muscle and the vasodilator mechanism mediated by activation of ETB receptors on endothelium to produce NO. 107 ET-1 has been implicated in the pathophysiology of hypertension, including in the brain and cerebral circulation through the actions of Ang II. In SHRSP, ET-1 levels in plasma are increased as are expression of ET-1 and ETA receptors in the brain.108,109 In addition, chronic ET-1 receptor inhibition partially prevents Ang II-induced hypertension. 110 Importantly, Ang II increases expression of ET-1 in several tissues including smooth muscle that is prevented by AT1R antagonism.110,111 Under normal physiological conditions, NO inhibits the release of ET-1. 112 However, conditions that decrease NO, such as hypertension, may enhance ET-1 release and its vasoconstrictor actions in an autocrine feed-forward mechanism.113,114 The effect of Ang II and ET-1 is also altered after stroke. Ang II potentiates vasoconstriction to ET-1 in cerebral arteries after ischemia and reperfusion but not under non-ischemic control conditions. 115
Activation of ET-1 receptors during ischemia and reperfusion has been shown to produce reactive oxygen (ROS) and nitrogen (RONS) species in an endothelium-dependent manner, that may be enhanced during hypertension in which ET-1 is elevated. 116 A previous study found that brain parenchymal arterioles (PAs) constricted to sarafotoxin, a selective ETB receptor agonist, only after tMCAO that was prevented by FeTMPyP to scavenge ONOO−, suggesting that ET-1 activation of ETB receptors on endothelium produces ONOO− to cause vasoconstriction. 117 The constriction to ETB activation was not due to de novo expression of ETB receptors on the smooth muscle, as has been shown in MCA at longer time periods of ischemia and reperfusion. 118 In vivo, ETB receptor antagonism has been shown to decrease infarction 24 h after permanent MCAO if given as a pretreatment.119,120 When ETB receptors were blocked 2 h post-occlusion, there was significant protection at seven days that was associated with upregulation of ETB, but not ETA receptors. 121
Ion channel activation in endothelium and smooth muscle
The cerebral endothelium also has a prominent role in regulation of vascular tone, mainly through the actions of NO and endothelium-derived hyperpolarization (EDH), or release of an EDH factor. Under resting conditions, basal NO production by the cerebral endothelium inhibits resting tone and thus affects cerebral blood flow.122,123 The mechanism of EDH-mediated vasodilation occurs via increased endothelial cell calcium that activates small- and intermediate-conductance calcium-activated potassium (SKCa and IKCa) channels, expressed in endothelium, causing K+ efflux and membrane hyperpolarization that is transferred to smooth muscle via myoendothelial gap junctions.124–127 While EDH does not appear to contribute to resting tone in cerebral arteries, we and others found that inhibition of SKCa/IKCa channels caused constriction of brain PAs, suggesting that unlike MCA, basal EDH is present in PAs that inhibits resting tone and contributes to CBF regulation.128,129 In addition, inhibition of SKCa/IKCa channels in vivo results in decreased CBF, 129 consistent with the concept that SKCa/IKCa channels are active in PAs under basal conditions and have a prominent influence on CBF through EDH. Several studies have shown that brain arterioles are less sensitive to NS309, a potent activator of SKCa/IKCa channels in SHR and SHRSP.130,131 Because SKCa/IKCa activity appears to be basally active and inhibit tone in PAs, their impairment during hypertension could contribute to increased tone and CVR that leads to hypoperfusion chronically and also incomplete reperfusion in the acute phase of stroke.
Other ion channels may be affected by hypertension and ischemic stroke to promote vascular dysregulation as well. Kir2.x channels are heterogeneously expressed in smooth muscle and endothelium depending on the vessel type.132,133 In cerebrovascular smooth muscle, Kir2.1 is expressed and opens with modest increases in extracellular potassium [K+]o (≤ 20 mM), causing outward movement of K+ and hyperpolarization that closes L-type Ca+2 channels to cause potent vasodilation.132,134 Kir2.1 channels have a key role in the vascular response to neuronal activation and in response to ischemia, as [K+]o in the brain increases from resting levels of 3–5 mM to 10–12 mM or greater that causes potent vasodilation of PAs through the activation of Kir channels.131,132 Kir channels may also have an important role in limiting infarct expansion through their vasodilating effect. Several studies have investigated Kir channel function in MCAs after ischemia and reperfusion.135,136 Marrelli et al. found impaired dilation to [K+]o in MCA after 2 h ischemia with 24 h reperfusion. 137 Subsequent patch clamp studies of isolated smooth muscle from MCAs found decreased Kir currents that positively correlated with infarction, suggesting a protective role of Kir channel activity during stroke. 138 Kir channels appear to be affected by hypertension as well and may contribute to impaired neurovascular coupling. 139 In addition, Bastide et al. 140 found a progressive decrease in Kir current density in myocytes from SHRSP, suggesting a role for Kir channels in development of stroke as well.
Collateral perfusion and hypertension
It is well-established in models of chronic hypertension that the brain is more susceptible to ischemic injury than aged-matched normotensive counterparts. Numerous studies have shown that infarction is larger in genetic models of hypertension (SHR and SHRSP) and in renal hypertension.62,63,130,141–143 One of the primary mechanisms by which infarction is larger in hypertension is the relative lack of salvageable tissue in hypertensive states, i.e. poor collateral status. Although several collateral systems exists within the brain vasculature, the pial collaterals or leptomeningeal anastomoses (LMAs) appear to be the most important for stroke outcome.144–146 Pial collaterals are distal connections between major arterial territories that can promote flow from one region to the other during an occlusion. During MCAO, pial collaterals between the ACA and MCA territories can sustain flow to the penumbra, a region of constrained blood supply that is salvageable if reperfusion occurs promptly or neuroprotective agents are given to prevent neuronal cell death.144–148 Pial collaterals sustain flow to the penumbra, and are therefore a strong predictor of recanalization, reperfusion and favorable clinical outcome.149–151
In addition to having small amounts of salvageable tissue during MCAO, SHR and SHRSP have been shown to have rapid evolution of infarction that encompasses the penumbra. McCabe et al.
63
used magnetic resonance imaging (MRI) to measure relative cerebral blood flow and quantitative apparent diffusion coefficient (ADC) maps to show that SHRSP had larger ADC lesion areas than normotensive WKY rats after just 1 h MCAO (Figure 2). In addition, SHRSP had a significantly larger perfusion deficit and perfusion-diffusion mismatch at 1 h after MCAO that was considerably less in WKY, demonstrating less salvageable tissue in SHRSP.
63
The small amount of mismatch in SHRSP as early as 1 h after MCAO indicates the ischemic injury occurs rapidly in this strain. Other studies have also shown that the ischemic lesion is maximal at 1 h after distal MCAO in SHR that correlated with final infarct at 24 h.152,153
Representative thresholded CBF map with ADC abnormality (black) overlaid highlighting the DWI-PWI mismatch (shown in white) at 1 and 6 h after stroke in a WKY (top) and SHRSP (bottom). Used with permission from McCabe et al. Stroke 2009; 40: 3864–3868.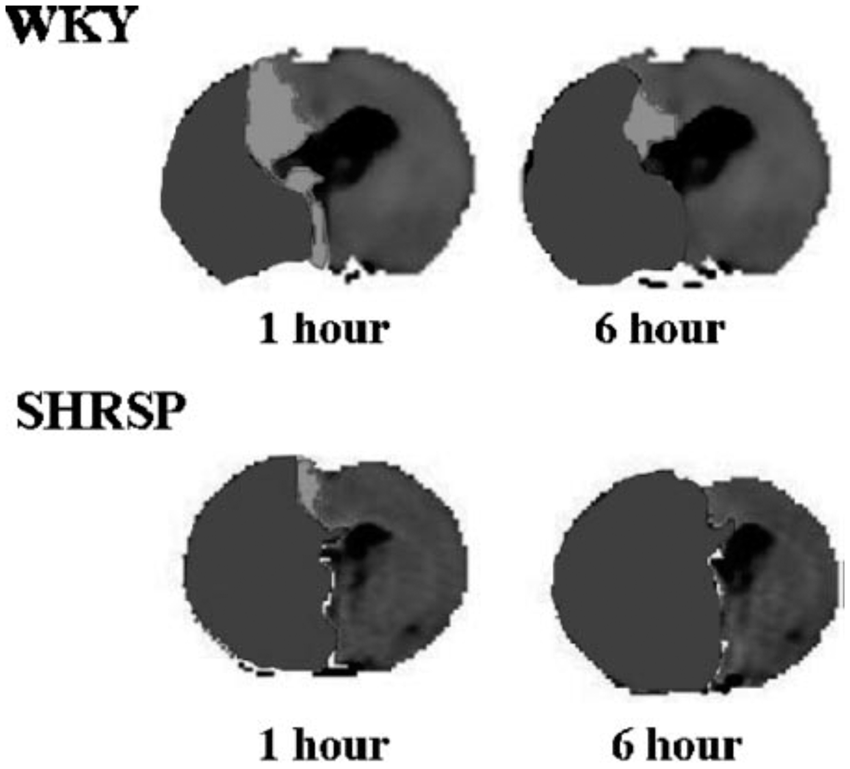
Other studies have shown that SHR and SHRSP have greater depth of ischemia during MCAO and poorer reperfusion that also likely contribute to larger infarction in these models.130,142 Our laboratory used hydrogen clearance to measure absolute levels of cerebral blood flow in the peri-infarct region of normotensive Wistar rats and SHRSP during transient MCAO and reperfusion. During filament occlusion, the perfusion deficit was significantly greater in SHRSP (Figure 3(a)). In addition, when cerebral blood flow was restored by filament withdrawal, reperfusion was incomplete in both strains for the 2 h that it was measured. The increase in perfusion deficit and impaired reperfusion was also shown by Kang et al.
142
using MRI in SHR. Figure 3(b) shows infarction, measured as early as 2 h after reperfusion was significantly larger in SHRSP. While more extensive perfusion deficits and poor collateral status are important contributors to increased infarction volume in SHR and SHRSP, other factors may also have a role in increasing the sensitivity of the brain to ischemia during hypertension, independent of collateral status, including increased release of glutamate,
154
production of vasoconstrictor agents such as 20-hydroxyeicosatetraenoic acid (20-HETE),
155
and increased ROS.
156
Effect of hypertension on CBF and infarct volume. (a) Cerebral blood flow at baseline and during ischemia and reperfusion in Wistar and SHRSP using hydrogen clearance. Flow measurements were taken 30 and 60 min after MCAO and 15, 30, 60 and 90 min after reperfusion. SHRSP had greater perfusion deficit than Wistar during MCAO and both groups had incomplete reperfusion; (b) brain infarct volume measured using TTC after 2 h of ischemia and 2 h of reperfusion in the same animals as in (a). Results are mean ± SEM. *p < 0.05 vs. Wistar; ^p < 0.05 vs. baseline, using t-test. Used with permission from Cipolla et al. J Cereb Blood Flow Metab 2017; 37: 1276–1285.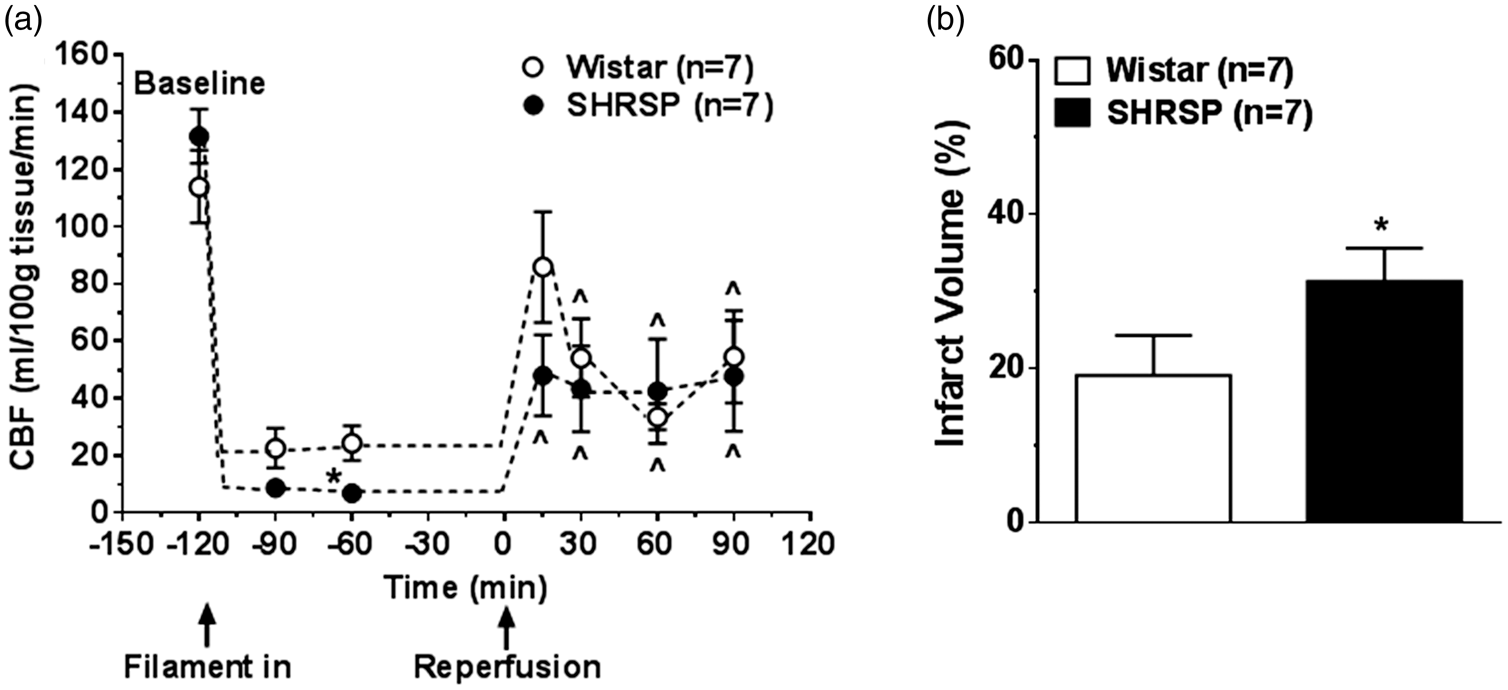
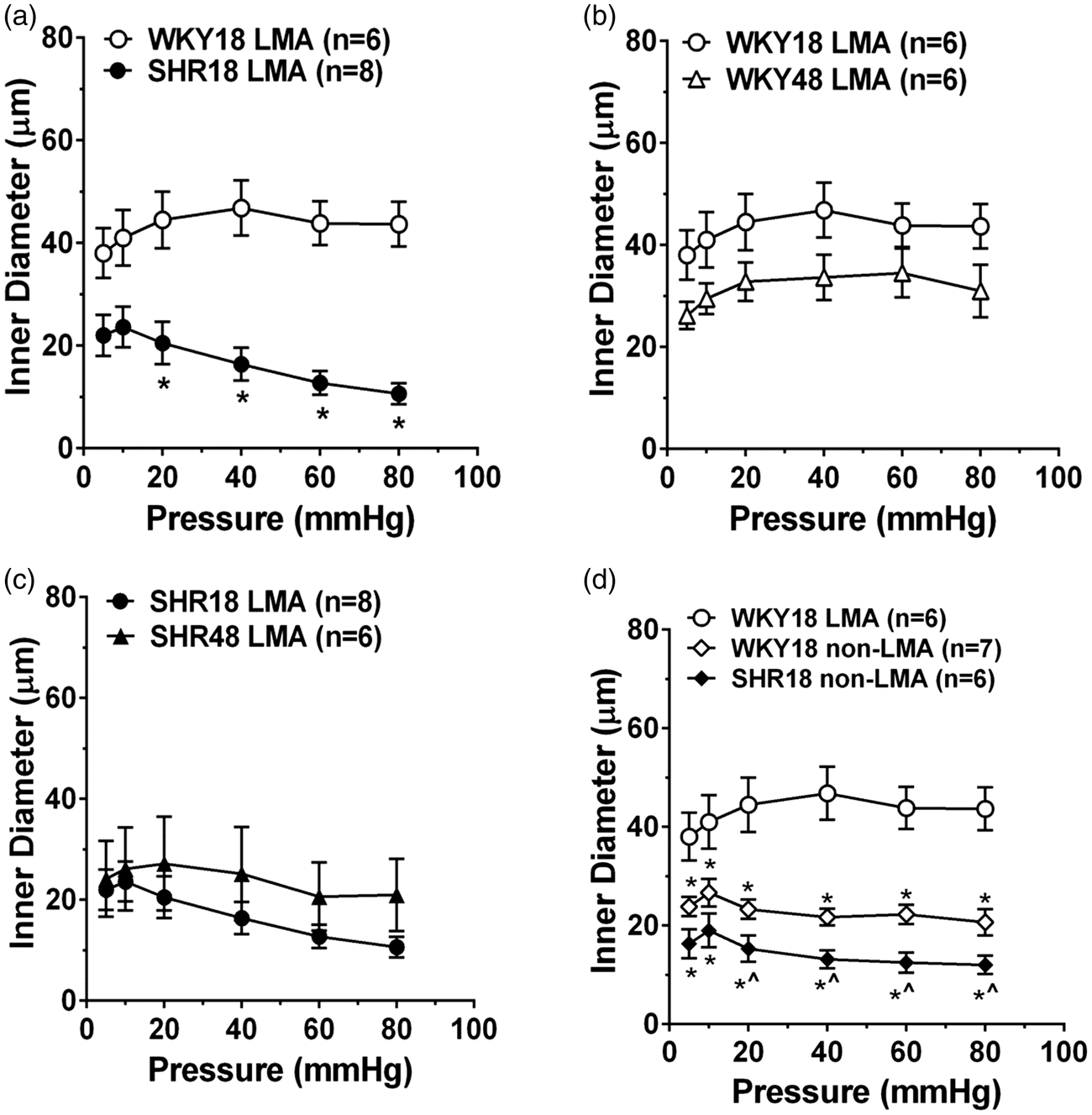
Poor collateral status in models of hypertension has mostly been attributed to structurally smaller lumen diameters of LMAs or fewer pial collateral vessels that limits flow to the penumbra. However, we recently demonstrated the functional capabilities of pial collaterals using an isolated vessel approach. Pial collaterals that connected ACA and MCA vascular territories were dissected and mounted on glass microcannulae and their reactivity to increased intravascular pressure and other vasoactive agents were measured in young (18 week old) and aged (48 week old) male normotensive WKY rats and hypertensive SHR. Figure 4(a) shows a photomicrograph of an LMA – a distal branch of the ACA and MCA arteries – that was dissected and mounted on glass cannulas (Figure 4(b)). When intravascular pressure was increased, LMAs from WKY rats behaved relatively passively and increased diameter as the pressure was increased (Figure 5(a)). The relatively low level of tone and dilatory response of LMAs to increased pressure would be conducive to rapid bidirectional flow and important for facilitating collateral perfusion. Importantly, LMAs from hypertensive SHR were highly vasoactive in response to pressure (Figure 5(a)) and constricted in a myogenic manner. In both strains, aging did not appear to affect the response to increased pressure (Figure 5(b) and (c)). We also compared the response of LMAs to pial arterioles that did not anastomose (non-LMA). Pial arterioles from both WKY and SHR were highly reactive to pressure and were more vasoconstricted than LMAs from WKY rats (Figure 5(d)). These results importantly demonstrate the heterogeneity of vascular function in the cerebral circulation and that LMAs under normotensive conditions are less vasoconstricted than non-LMAs that would be conducive to retrograde flow during an occlusion. However, the highly vasoconstricted nature of LMAs from SHR likely contributes to the increased perfusion deficit and poor collateral status that has been shown in numerous studies. These results also suggest that salvaging penumbral tissue by opening vasoconstricted pial collaterals is indeed, possible. In fact, we recently demonstrated the ability of Sanguinate™, a carboxyhemoglobin gas transfer agent, to increase collateral flow in SHR and decrease early infarction.
157
(a) Diagram showing LMA (circle) reconnecting distal branches of MCA and ACA. (b) Photomicrograph of isolated and pressurized LMA on glass cannula. Used with permission from Chan et al. Stroke 2016; 47: 1618–1625. Effects of hypertension on myogenic response of LMAs. (a) Myogenic response of LMAs over a range of pressure in young WKY and SHR. LMAs from WKY behaved relatively passively, while LMAs from SHR constricted in response to increase in pressure. Myogenic reactivity of LMAs in young versus aged WKY (b) and SHR (c). Note that myogenic response of LMAs was not changed in aging in either strain. (d) Myogenic reactivity of LMAs comparing LMAs to non-LMAs in WKY and SHR. Non-LMAs were more myogenic than LMAs from WKY, demonstrating the uniqueness of LMAs in facilitating collateral perfusion during cerebral pial artery occlusion. *p < 0.05 vs. WKY18-LMA; ^p < 0.05 vs. WKY18-non-LMA using t-test or one-way ANOVA with post hoc Bonferroni test for multiple comparisons. Used with permission from Chan et al. Stroke 2016; 47: 1618–1625.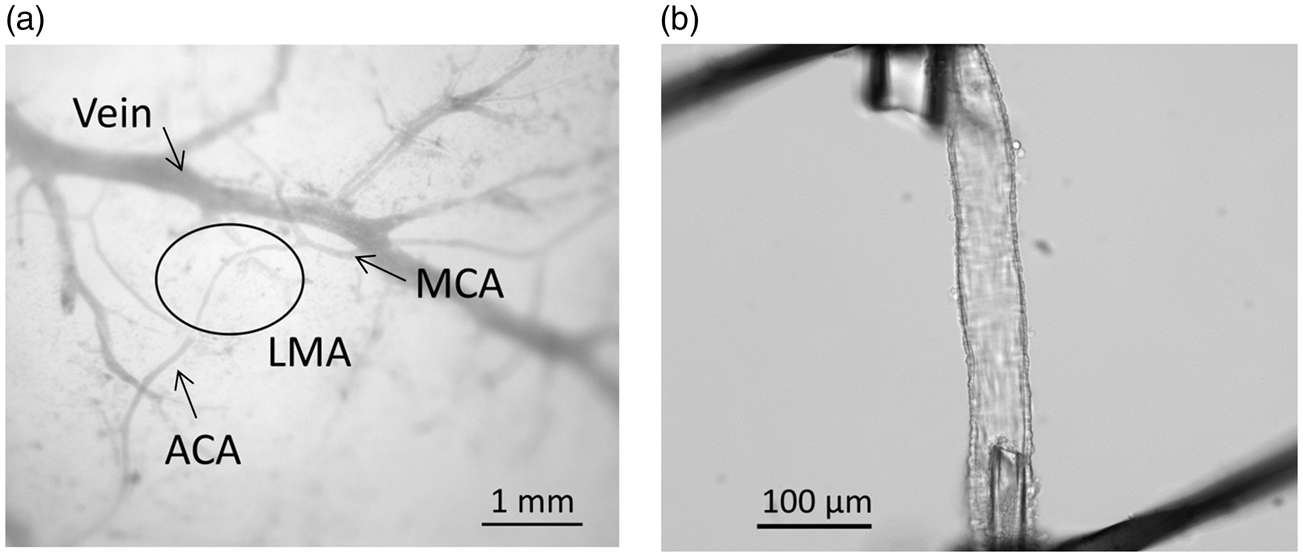
Collateral arteriogenesis and hypertension
The primary collaterals, which include the pial arteries of the Circle of Willis, immediately redirect flow in an event of one or more occlusions within the four extracranial arteries (two carotid and two vertebral arteries) that perfuse the brain. Long-term increases in flow cause structural enlargement in cerebral collaterals, termed arteriogenesis. In a rat model of three-artery occlusion (one carotid and two vertebral), the ipsilateral posterior cerebral artery enlarged by 39% by one week and 72% by three weeks due to a substantial increase in flow from the sole carotid artery. 158 In another model of bilateral common artery occlusion and arteriovenous fistula in rats, arteriogenesis of the posterior cerebral artery occurred due to increased flow from the vertebral arteries. 159 The same study showed that arteriogenesis was due to shear stress-mediated activation of transient receptor potential vanilloid-4 (TRPV4) channels in endothelium. 159
LMAs also undergo arteriogenesis in response to increased flow during chronic occlusions. In normotensive WKY rats, LMAs underwent arteriogenesis (diameter increased by 50%) one month after MCAO. 160 However, LMAs from SHRSP were narrower with less blood flow and larger infarct compared to WKY one month after MCAO. 160 Other studies showed impairment of arteriogenesis in LMAs from SHR subjected to unilateral common artery occlusion that was normalized by antihypertensive treatment.161,162 Impaired arteriogenesis of pial collaterals may be due to decreased TRPV4 expression that has been shown to be decreased in SHRSP compared to WKY. 163
Hypertensive CSVD
CSVD significantly increases the chance of a future stroke,164–166 and is a major cause of lacunar infarction,167–169 vascular dementia and cognitive and motor impairment.169–177 CSVD is caused by a number of factors, including genetics, comorbidities, and diet, yet chronic hypertension is the most common risk factor for CSVD. 178 In fact, many clinical studies reported that the majority, between 70 to 80%, of CSVD patients are hypertensive.167,171,174,177 Due to the cerebral small vessels being too small to visualize in clinical imaging, 179 CSVD is commonly inferred and diagnosed by white matter lesions (WMLs), lacunes, microbleeds, and increased perivascular space seen on MRI.180,181 Studies on CSVD have largely relied on autopsy studies in deceased human brains, which are limited to pathologies of end-stage CSVD and commonly combined with pathologies of other brain diseases. Hypertensive CSVD affects all small vessels in the brain, including arterioles, capillaries, and venules but most data available are in the small perforating arterioles. Classical studies by Fisher showed mostly occlusive lipohyalinosis lesions of small perforating arteries associated with lacunar infarct in 18 autopsy human brains.182,183 Lipohyalinosis is defined by Fisher as occlusion of small perforating arteries by lipid and hyaline materials. Later studies showed that most lipohyalinosis in hypertensive CSVD is characterized by thickening of the vessel wall and narrowing of lumen due to loss of smooth muscle that was replaced by fibrohyaline (fibrin and hyaline) materials.184,185 Other less common features of hypertensive CSVD are atherosclerosis and microaneurysms.184,185 It is believed that occlusive lipohyalinosis lesions of small perforating arteries cause a chronic state of hypoperfusion as evidenced by increased hypoxia-inducing factor-1 in autopsy human brains with WML. 186 More recent studies in hypertensive CSVD patients demonstrated that these patients have impaired vascular reactivity leading to the loss of autoregulation,187–189 impaired neurovascular coupling190,191 and increased blood–brain barrier (BBB) permeability.192–195 Although these studies are important, the pathological changes at earlier stages of hypertensive CSVD and the processes by which hypertension affects small vessels to promote CSVD, deserve further investigation.
The presence of hypertensive CSVD and WML is often asymptomatic and even neglected.196–198 However, the presence of WML is a predictor of CSVD progression and new formation of lacunes. 199 More importantly, severity of WML is not just a predictor of future stroke but also a predictor of stroke outcome including infarct progression and poor cognitive performance.164–166 Increased infarct volume after acute ischemic stroke has also been shown in models of hypertension (SHR and SHRSP).200,201 Lacunar stroke comprises about 25% all first-time ischemic stroke and therefore finding treatment for hypertensive CSVD to reduce stroke burden is of great importance. 202
Peroxisome proliferator-activated receptor gamma and hypertensive CSVD
In addition to antihypertensive treatments, new treatments that specifically normalize the adverse effects of hypertension on target cerebral small vessels at early stages of the disease are important. For example, the transcription factor peroxisome proliferator-activated receptor gamma (PPARγ) may be a therapeutic target for hypertensive CSVD. Dominant negative mutations of PPARγ in humans at P467L or V290M cause insulin resistance and hypertension. 203 Pharmacological activation of PPARγ by thiazolidinediones lowers blood pressure in various animal models of hypertension, including SHR and AngII infusion in rats.204,205 In the cerebral circulation, genetic knock-in mutation of PPARγ at P467L caused endothelial dysfunction, inward remodeling and increased wall thickness in cerebral arterioles. 206 In studies using mice with endothelium-specific interference of PPARγ function, a high-fat diet caused endothelial dysfunction in basilar arteries but not aorta, suggesting PPARγ may be more involved in the protection of the cerebral circulation. 207 In cerebral small vessels, PPARγ activation by rosiglitazone normalized L-NAME-induced increased blood pressure, myogenic tone and hypertrophic inward remodeling in third-order posterior cerebral arteries. 208 Rosiglitazone also normalized L-NAME-induced capillary rarefaction in the brain. 209 Moreover, relaxin, a hormone related to pregnancy, selectively caused outward remodeling of PAs and not the upstream middle cerebral arteries in normotensive female rats through activation of PPARγ. 209 Another study showed that treatment of relaxin increased distensibility of PAs in young female SHR. 210 Collectively, the protective effect of PPARγ activation selectively in cerebral small vessels during hypertension may be a therapeutic target for hypertensive CSVD.
Preeclampsia
Preeclampsia is a hypertensive disorder of pregnancy characterized by de novo hypertension after the 20th week of gestation with evidence of organ damage. Preeclampsia complicates up to 10% of pregnancies worldwide and is one of the greatest causes of maternal and fetal morbidity and mortality.211–213 Compared to normal pregnancy, preeclampsia is characterized by increased peripheral vascular resistance and hypertension, endothelial dysfunction, hypercoagulation, and increased vascular stiffness.214–218 Although preeclampsia is defined as a disorder of pregnancy, its consequences are far reaching and can extend decades into the postpartum years. Preeclampsia is a major risk factor for future cardiovascular and cerebrovascular diseases including hypertension, heart failure and stroke.12–14,214–219 Preeclampsia is also associated with brain atrophy and cognitive decline later in life.217,218 The cognitive defects and decline positively correlate with lesions in deep brain structures (i.e. WMLs).220–224 Importantly, formerly preeclamptic women can develop cognitive impairment and WMLs as early as in their 30s, suggesting preeclampsia predisposes the brain to early-onset cognitive impairment and white matter damage.220,221,225–228
Dyslipidemia and vessel stiffness in preeclampsia
There are several mechanisms by which preeclampsia could promote cerebrovascular disease. Preeclampsia is a state of dyslipidemia in which the normally elevated low-density lipoprotein (LDL) cholesterol during pregnancy is exaggerated. 229 Importantly, very low-density LDL (vLDL) is increased in preeclamptic women that is highly susceptible to oxidation to form oxidized LDL (oxLDL). 229 Levels of oxLDL are over 200% increase in serum of women with early-onset preeclampsia (diagnosis prior to 34 weeks’ gestation). 230 oxLDL binds the LOX-1 receptor with high affinity to activate NADPH oxidase to generate superoxide (O2−), a primary mechanism of atherogenesis. 230 Studies in humans have shown that arteries from women with preeclampsia have increased oxLDL and LOX-1 expression, suggesting this is a mechanism of endothelial dysfunction and oxidative stress. 231
Preeclamptic women also have increased large artery stiffness that may precede clinical symptoms. In a prospective study, carotid-femoral and carotid-radial pulse wave velocity were increased at 22 weeks’ gestation in women who subsequently went on to develop preeclampsia. 232 The importance of finding women with preeclampsia have increased large vessel stiffness is that it is an independent predictor of cerebrovascular disease and stroke. 233 Peripheral arterial stiffness occurs with aging, hypertension and dyslipidemia that also promote microvascular damage by transmitting pulsatile pressure to distal microvessels.17,18 The brain is highly susceptible to microvascular damage associated with peripheral arterial stiffening because it is an organ with high flow and low impedance, thus allowing the pulsatile load to be transmitted more deeply into the brain parenchyma.17,18 The propagation of high pulsatile flow to the cerebral microvasculature is thought to promote remodeling and cause microvascular damage that underlies white matter hyperintensities, cerebral microbleeds and lacunar infarcts.17,58,234 In addition, clinical studies have shown strong associations between arterial stiffness and vascular dementia, suggesting cerebral microvascular remodeling secondary to enhanced arterial stiffness may be a causative factor in neurocognitive decline.58,235,236 Importantly, preeclamptic women have increased peripheral arterial stiffness, including enhanced carotid pulse wave velocity and augmentation index as well as increased carotid intima-media thickness237,238 that persists postpartum.214,239,240 Although the mechanism by which arterial stiffness occurs in preeclampsia is not known, oxLDL appears to have a central role in promoting arterial stiffness outside of pregnancy. Elevated oxLDL levels are associated with higher arterial stiffness in aging, independent of cardiovascular disease risk factors, 241 and in patients with peripheral arterial disease. 242 While the presence of high oxLDL is, in and of itself, a marker of high oxidative stress, several studies have demonstrated that arterial stiffness is associated with LOX-1 binding and increase oxidative stress in patients with hypertension, metabolic syndrome and aging.243–247
Our own studies found mild hippocampus-dependent cognitive impairment in a rat model of preeclampsia.
248
Hippocampal arterioles, isolated with the internal transverse hippocampal artery (Figure 6(a) and (b)), were smaller and stiffer than those from normal pregnant or nonpregnant rats (Figure 6(c) and (d)).
249
In addition, while hippocampal blood flow was not different between groups basally, the experimental preeclamptic rats lacked the normal hyperemic response to seizure. The importance of these findings is that women with preeclampsia are more susceptible to seizure (termed eclampsia) and the lack of a hyperemic response during seizure may increase seizure-induced damage to hippocampal neurons through hypoxic ischemic injury. In addition, whether hippocampal arteriolar remodeling and increased stiffness was due to high oxLDL and/or increased large vessel stiffness is not clear, but if this effect is persistent years after pregnancy, it could contribute to early onset cognitive impairment that has been shown to occur in these women.
Effect of experimental preeclampsia (ePE) on passive structural and biomechanical properties of HAs. (a) Diagram showing the arterial blood supply to the hippocampus. (b) Photomicrograph of isolated and pressurized HA branching off the internal transverse hippocampal artery. (c) Passive inner diameters over a range of pressures. (d) Stress–strain curves as a measure of vessel stiffness; a shift to the left demonstrates increased stiffness. *p < 0.05 vs. Nonpreg; ** p < 0.01 vs. Nonpreg; ^^p < 0.01 vs. Nonpreg and Preg by one-way ANOVA with post hoc Bonferroni test for multiple comparisons. Used with permission from Coyle. Exp Neurol 1976; 52: 447–458 and Johnson and Cipolla. J Cerebr Blood Flow Metab 2017; 37: 2857–2869.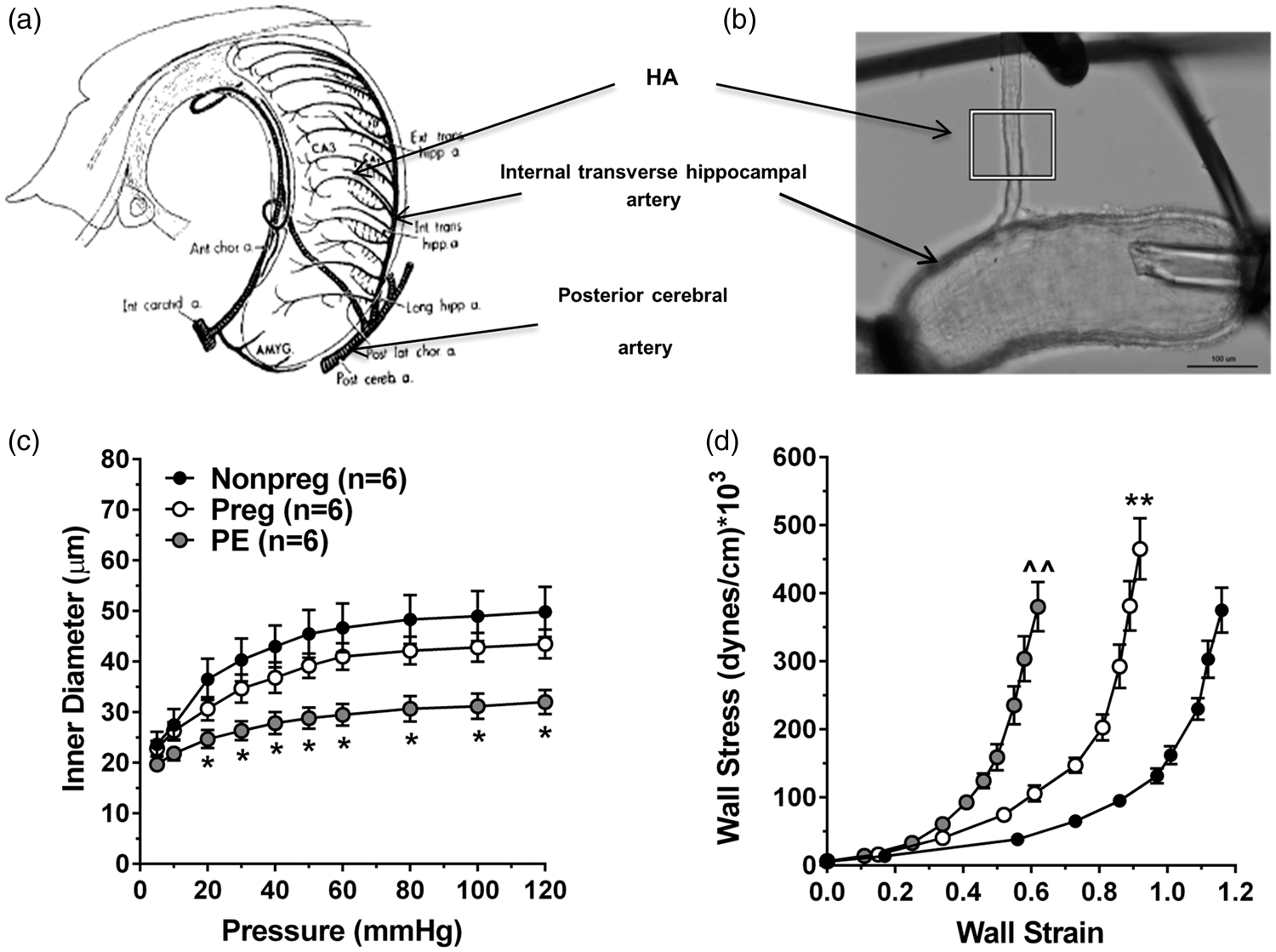
Stroke in preeclampsia
Hypertensive disorders of pregnancy, most notably preeclampsia, is a major cause of stroke in young women, a trend that is increasing.250,251 Different subtypes of stroke occur in preeclamptic women, including ischemic and hemorrhagic, demonstrating the heterogeneity of both stroke and preeclampsia.250,251 Normotensive pregnancy alone is a state associated with increases in coagulation factor levels and decreases in endogenous anti-coagulation, promoting a hypercoagulable state.252–254 The hypercoagulability during pregnancy is thought to ensure control of bleeding during birth and placental separation. In preeclamptic women, this normal prothrombotic state further exaggerated.255–257 Endothelial dysfunction, combined with hemostatic disturbances likely contribute to some of the stroke risk in these women, especially cerebral venous thrombosis and intracerebral hemorrhage. Although pregnancy alone increases stroke risk, other factors associated with preeclampsia further increase this risk, including hypertension, obesity and metabolic syndrome that are common features and comorbidities of preeclamptic women.258–262 In addition, arterial and venous vascular remodeling during pregnancy and the postpartum state, combined with dramatic fluctuations in plasma volume and cardiac output, likely contributes to risk of subarachnoid hemorrhage and aneurysm rupture.
The risk of ischemic stroke in preeclamptic women is not limited to the index pregnancy. Several case-controlled studies have demonstrated that women with a history of preeclampsia were associated with increased risk of stroke remote from pregnancy.263,264 The mechanism by which prior preeclampsia increases stroke risk years after pregnancy is not clear. While it is possible that endothelial dysfunction and hemostatic dysregulation associated with preeclampsia persist later in life, another possibility is that women who develop preeclampsia have a predisposition to cardiovascular disease risk that the physiological stress of pregnancy unmasks, i.e. preeclampsia is a manifestation of overall cardiovascular and cerebrovascular disease risk. Understanding the underlying causes of increased stroke risk in preeclampsia during pregnancy and years later is a challenge. However, it is clear that women with prior preeclampsia, especially early-onset preeclampsia, are at increased risk of cerebrovascular disease and stroke. In fact, the American Heart Association recommends that a history of preeclampsia be considered a major risk factor for heart disease and stroke. 265
Summary and conclusions
Chronic hypertension has a profound impact on the cerebral circulation, summarized in Figure 7. In general, hypertension is associated with high levels of Ang II and AT1R activation in the blood vessels and brain that increases superoxide production and diminishes the normal vasodilatory influence of NO. There is also an increased vasoconstrictor influence (e.g. ET-1) that together with decreased endothelial NO increases CVR and shifts both the low and high limits of the autoregulatory curve to higher pressures. During acute ischemic stroke, the smaller lumen diameters and increased vasoconstriction of cerebral arteries and arterioles can increase perfusion deficit and impair collateral perfusion, leading to increased infarction. In addition, if prolonged, the increased CVR can cause hypoperfusion and contribute to CSVD, a leading contributor to stroke. Hypertension also increases pulse pressure and shear stress on the endothelium that can cause BBB disruption and vascular wall damage, both contributors to CSVD. Preeclampsia, a common hypertensive disorder of pregnancy, is associated with high levels of oxLDL and LOX-1 activation that increases BBB permeability that can promote seizure (eclampsia). In addition, women with prior preeclampsia have an increased risk of stroke and early-onset cognitive impairment, that is not seen in women with gestational hypertension, suggesting preeclampsia is a unique and more devastating form of hypertension. Figure 7 summarizes the major effects of hypertension on the cerebral circulation and some of the molecular and biochemical mechanisms of dysfunction, many of which can be considered targets for therapeutic intervention.
Summary figure showing potential impacts of hypertension on the cerebral circulation that may increase the chance of future stroke and/or worsen stroke outcomes.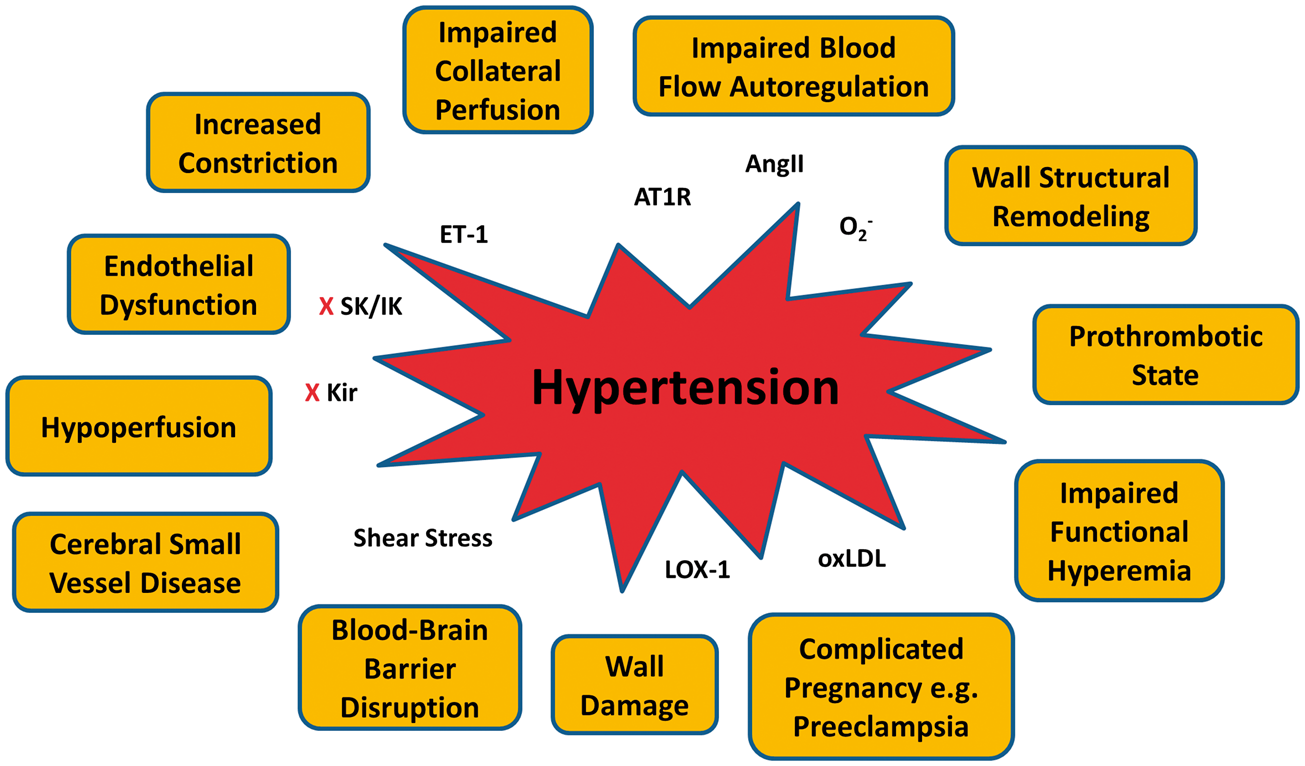
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.