
Abstract
Headache is one of the most common ailments; migraine is one of the most prevalent and disabling neurological disorders and cluster headache presents as one of the most excruciating pain disorders. Both are complex disorder characterized by recurrent episodes of headache. A key feature is that various triggers can set off an attack providing the opportunity to explore disease mechanisms by experimentally inducing attacks. This review summarizes neuroimaging and hemodynamic studies in human in provoked and spontaneous attacks of migraine and cluster headache. Cerebral hemodynamics during different phases of the migraine attack demonstrate alterations in cerebral blood flow and perfusion, vessel caliber, cortical and sub-cortical function, underscoring that migraine pathophysiology is highly complex. Migraine attacks might begin in diencephalic and brainstem areas, whereas migraine aura is a cortical phenomenon. In cluster headache pathophysiology, the hypothalamus might also play a pivotal role, whereas the pattern of cerebral blood flood differs from migraine. For both disorders, alterations of arterial blood vessel diameter might be more an epiphenomenon of the attack than a causative trigger.
Studying cerebral hemodynamics in provocation models are important in the search for specific biomarkers in the hope to discover future targets for more specific and effective mechanism-based anti-headache treatment.
Introduction
Migraine is a common disabling neurological disorder 1 afflicting 10% of the global adult population. 2 The cost of migraine is substantial 3 and so is the public health burden with migraine being in the top 10 of the most disabling conditions worldwide. 4 Although being less frequent, the impact of the most common trigeminal autonomic cephalalgia, 5 cluster headache (CH), is enormous owing its excruciating severity. A migraine patient can be in interictal, premonitory, headache, or recovery phase 6 of the condition with the headache phase being the most prominent with its key features of moderate to severe headache of pulsating quality, photophobia, phonophobia, nausea as well as worsening with movement. 5 We now assume that its pathophysiology might involve diencephalic and brainstem mechanisms. 7 The relation to the impressive typical migraine aura remains unsolved with cortical spreading depression (CSD) being the most likely pathophysiological mechanism. 8
CH is characterized by (almost) strict unilateral headache with prominent cranio-autonomic features, such as pupillomotor dysfunction, ptosis, lacrimation, conjunctival injection, rhinorrhea, nasal congestion, ear fullness and others. The main dynamic feature of CH is that it occurs in “clusters,” i.e. not equally distributed over time. Typically, in the beginning, patients with CH have periods of recurring, often daily attacks over several weeks (“bouts”) followed by months or years of freedom from attacks (“out of bout”). Moreover, during bouts, patients suffer from recurring attacks, which often occur on a daily basis, and at the same time during the day. From a clinical perspective, thus, an internal clock might be sought turning on single CH attacks and/or switching between in-bout and out of bout.
Our understanding of headache pathophysiology has substantially improved over decades, based on translational research, keeping in mind that only humans can truly explain the very diverse symptoms of migraine or CH. In early research, therapeutic success of vasoconstricting ergotamines 9 and headache during meningeal manipulation in the context of neurosurgical interventions 10 suggested blood vessels as well as meningeal structures being key players during migraine pathophysiology. Therefore, behavior of blood vessels during migraine (but also during CH) attacks as well as brain perfusion has been of interest in studies of migraine mechanism. In this regard, two important aspects need consideration: (i) cerebral arteries can change diameter and thus influence brain perfusion, and (ii) brain activity can result in increased demand of oxygen, energy substrates, such as glucose and metabolite removal with subsequent increase of focal brain perfusion (neurovascular coupling). Both have been studied in detail over the last four decades using different techniques (transcranial Doppler sonography (TCD), SPECT, PET, and MRI) as described in another article of this issue (Schytz et al.: “Methods description, advantages and limitation of each technique”). One of the most recent techniques, resting state functional brain connectivity, also involves neurovascular coupling. Since there is an extra article in this issue (Schwedt et al.), it will not be reviewed here in detail.
Migraine and CH are characterized by recurrent headache attacks of essentially different, but overlapping pathophysiology. To study the individual, in general unpredictable, attack, provocation studies assessing cerebral hemodynamics and neurovascular coupling are necessary and will be reviewed here in detail. Most such studies were on migraine, for which reason migraine will be covered most, but CH will be included as well.
Methods
In March 2017, a literature search in PubMed was performed using the key words “migraine” or “cluster headache” combined with words giving information on cerebral hemodynamics (i.e. “Doppler,” “functional brain imaging,” “MR angiography” or “SPECT”). Further key words were “experimental headache,” “headache trigger,” “human experimental headache model” and “headache provocation.” The reference list of relevant papers was also screened. Articles known to be relevant by the authors were also considered. The search was limited to publications in English, and the final references included were chosen based on the relevance to the scope of this Review.
Migraine
Interictal phase
Recurrent headache is a key clinical feature of migraine according to the International Classification of Headache Disorders. 5 But being migraineur is associated with subtle differences of brain function, that for example might reflect in a general (usually non-obstructive) hypersensitivity to light 11 or a slightly different behavior in electrophysiological tests, e.g. lack of habituation of repetitive visual evoked potentials. 12 Such interictal studies are easier to accomplish than studying the unpredictably occurring attack and address the peculiarity of being migraineur in contrast to not being prone to migraine attacks. In respect to interictal cerebral perfusion, some regional differences to healthy controls can be detected,13–16 but a firm relevance for migraine pathophysiology has yet to be established. Similarly, interictal baseline mean blood flow velocity of intra- and extracranial blood vessels does not differ to controls. 17 The reactivity of arteries to several external stimuli including changes in hyperventilation, breath holding, visual stimulation, glyceryl trinitrate (GTN) points to an increased vasomotor response in migraineurs18–22 although contrary results have to be acknowledged.17,23 In a study involving 20 patients with migraine without aura and 11 control subjects, Dora et al. 20 demonstrated such increased cerebrovascular reactivity to hypercapnia using TCD that interestingly improved after successful prophylactic treatment. This suggests that cerebrovascular reactivity might be a marker for severity of migraine. The “supersensitivity” of the cerebral arteries to GTN was demonstrated in migraineurs 24 establishing a specific interest for the nitric oxide (NO) pathway in migraine research. Furthermore, the demonstration of migraine-like headache being reliably triggered by GTN-infusion 25 helped to overcome an integral and long-standing problem of migraine research – the paroxysmal unpredictability of spontaneous attacks.
Ictal phase
Several methods have been established to trigger migraine attacks in migraineurs including the infusion of vasoactive substances, such as GTN, calcitonin-gene-related peptide (CGRP) and pituitary adenylate cyclase-activating polypeptide (PACAP). 26 A limitation of triggering headache is naturally, that it could be argued that attacks are artificial and thus not valid for studying migraine. However, any migraineur would agree that his or her migraine attacks can be triggered by several events, such as weather change, menstrual period, stress, sleep disturbance and others and would clearly oppose to not calling is migraine. Further, clinical characteristics of GTN-induced delayed headache de facto meet criteria for migraine, 27 and even paraclinical tests, such as brain perfusion measured with [15O]-water PET demonstrate identical areas of hyperperfusion during spontaneous migraine 28 and GTN-induced migraine-like headache 29 such as the dorsal pons.
Premonitory phase
The headache phase is most characteristic for patients with migraine and in general most curtailing for quality of life. It, however, does neither arise all of a sudden from good health nor disappear without a trace at its end. Patients rather experience migraine symptoms both before and after the headache phase, see Figure 1. Even though these symptoms do not qualify as a migraine according to IHCD-III beta criteria, they tell the affected individual that there is a headache approaching or still lingering. These phases of the migraine attack are therefore called premonitory and recovery/postdromal.
6
The symptoms and signs during a migraine attack, arbitrarily divided into five distinct phases. In one prospective study, the most common premonitory symptoms are tiredness (72%), followed by difficulty with concentration (51%), neck stiffness (30%) and sensitivity to light (49%).
30
Similar data were found retrospectively by Schoonman et al.
137
with fatigue (46%), phonophobia (36%), yawning (36%) and prospectively by Quintela et al.
128
with anxiety (46%), phonophobia (44%), irritability (42%), yawning (40%) and by Kelman
138
with fatigue (26%), mood change (23%) and gastrointestinal symptoms (22%). Figure adapted from Blau.
6
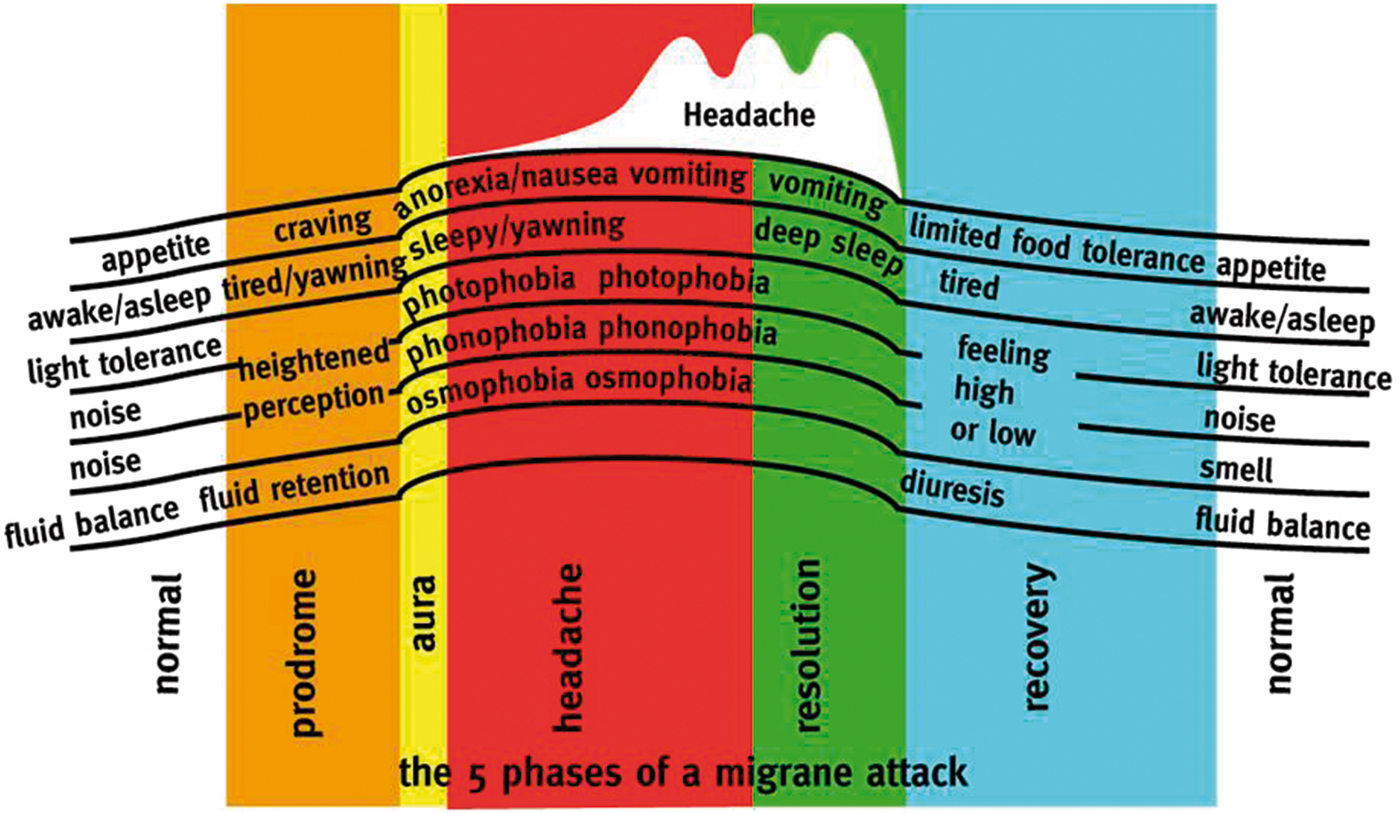
Giffin et al. 30 have studied the premonitory phase prospectively using an electronic diary in 97 patients who experienced premonitory symptoms in the past. Patients were asked for at least one entry per day and for entering in addition symptoms, they rated as premonitory when experienced. Retrospective alterations were not allowed. In the Giffin et al., study 30 the highest predictability ratio, i.e. the ratio of correct to incorrect attribution of a symptom being premonitory was found for yawning (ratio 2.1) and being emotional (2.0). Even higher ratios were found for difficulties with speech (4.9) and written language (3.5), but since migraine with aura has not been excluded in this study, the distinction from dysphasic aura remained unclear.
Premonitory symptoms thus appear to be the first clinical trace of the migraine attack, 6 some of them persisting into the headache or even postdromal phase, others disappearing with the onset of head pain. Understanding the generation of the premonitory phase therefore might offer insights on how and where migraine attacks may begin. Functional brain imaging would be the method of choice, but the unpredictability of the individual attack in episodic migraine in the context of substantial logistic expense would make such approach in particular difficult. At least three different approaches are conceivable and have been followed: triggering of premonitory symptoms (and its subsequent migraine attacks), testing of several patients at random time points with prospective diary-based identification of the time point within the migraine cycle, and sequential examination of individual patients on a regular basis with catching the premonitory phase “by accident.”
In respect of premonitory symptoms, Afridi et al. 31 used the GTN-model in 44 migraineurs. Thirty-three subjects developed typical migraine attacks, and twelve even experienced their typical premonitory symptoms, suggesting that GTN-induced delayed headache (i) is true migraine and (ii) might be a good model for studying the premonitory phase.
Based on this, Maniyar et al.
32
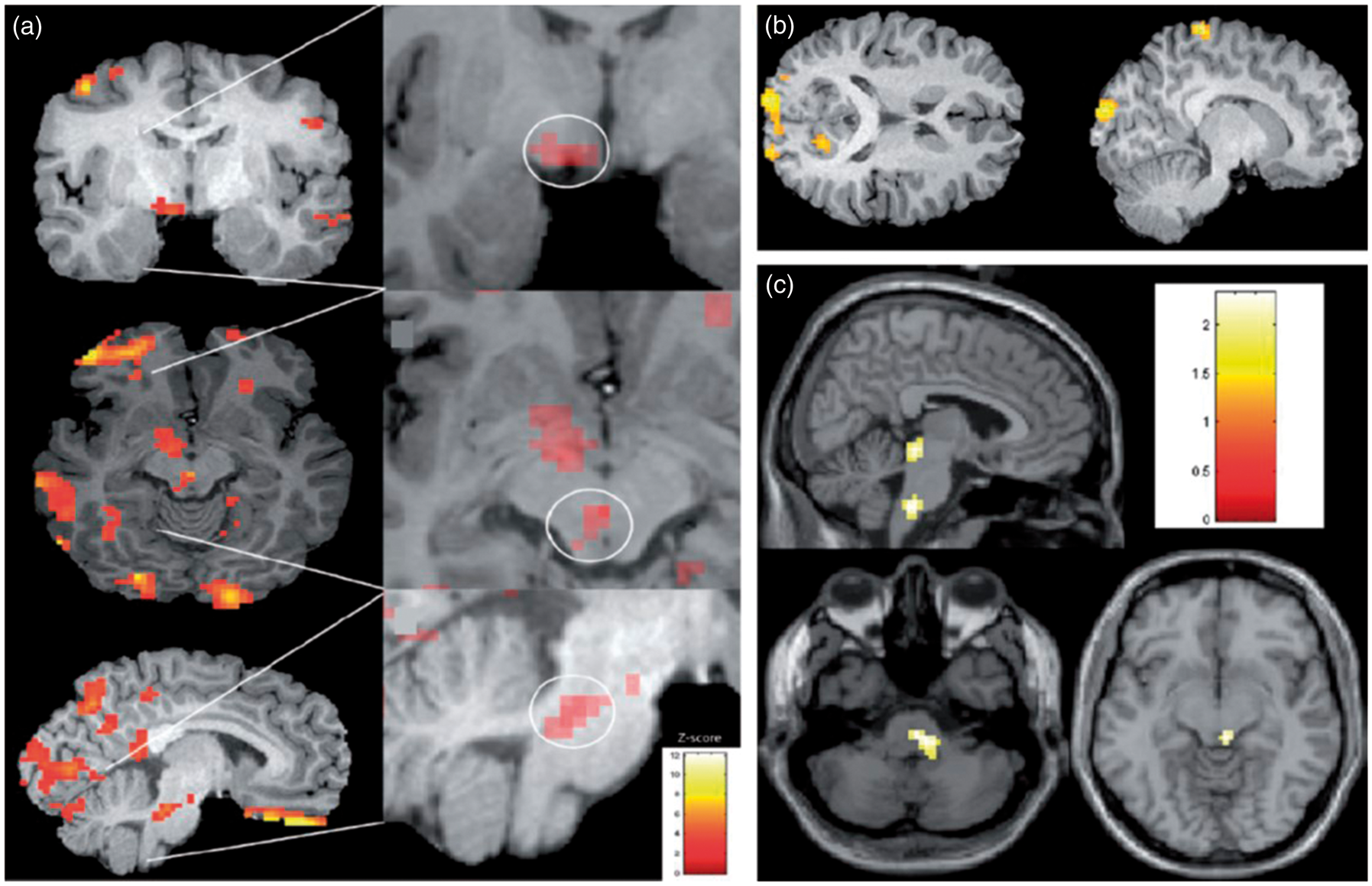
triggered premonitory symptoms in eight migraineurs and compared cerebral blood flow (CBF) using [15O]-water PET between the premonitory phase and interictal baseline. Most common premonitory symptoms were tiredness, thirst, yawning, neck stiffness, photophobia and nausea. They found hyperperfusion as a surrogate parameter for increased brain activity in the hypothalamus, the midbrain, in particular the periaqueductal grey, the dorsal pons and several cortical areas (Figure 2(a)). This is remarkable since the structures identified correspond well with the anatomic location expected to be mediating these symptoms. In a subgroup analysis, Maniyar et al. compared five patients with premonitory photophobia with five migraineurs without and identified increased CBF in the extrastriate visual cortex (Brodmann area 18) during photophobia (Figure 2(b)).
33
Similarly, nausea during the premonitory phase was associated with increased activity in the rostral dorsal medulla and periaqueductal grey (Figure 2(c)).
34
Areas of hyperperfusion during the premonitory phase of the migraine attack. In this earliest phase, patients realize symptoms prior to headache suggesting a dysfunction of the hypothalamus, periaqueductal grey as well as the dorsal pons in congruence with the symptoms reported (a).
32
Patients with photophobia in the premonitory phase similary show hyperperfusion in the occipital lobe (b),
33
patients with nausea in the dorsal medulla as well as the periaqueductal grey (c).
34
In summary, these studies demonstrate that during the GTN-induced premonitory phase, there is brain activation in areas mediating these symptoms. The study investigated a subgroup of migraineurs (i.e. patients with habitual and GTN-induced premonitory symptoms) and did not include control groups (i.e. migraineurs or healthy control subjects without GTN-induced premonitory symptoms). Keeping this in mind, the studies reinforce brain activation prior to any head pain. Since the pathophysiological correlate of head pain is activation of the trigeminal system, it could be hypothesized that migraine attacks start without primary activation of the trigeminal system as previously suggested. 35 Migraine may start in the brain, probably in areas modulating pain, such as the periaqueductal grey or the dorsal rostral pons, and/or in areas being involved in maintaining body homeostasis and circadian or circa-monthly rhythmicity, such as the hypothalamus.
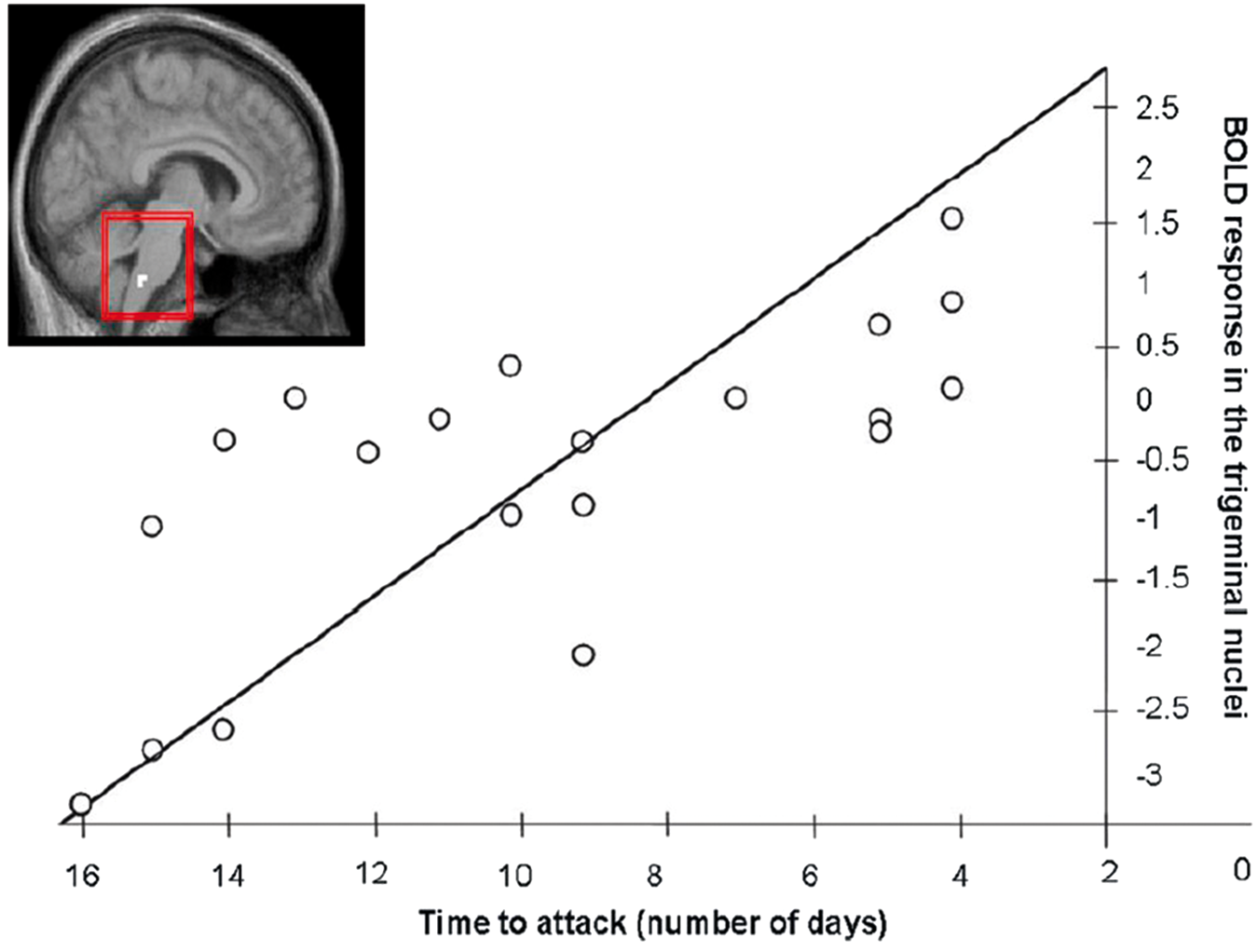
An alternative approach examined patients randomly during the migraine cycle and – quasi retrospectively – identified the premonitory phase or the proximity to the migraine attack using a diary. The study was based on a paradigm using noxious stimulation of the trigeminally innervated nasal mucosa in a randomized order against rose odor or air stimulation. Interictal noxious stimulation in migraineurs led to reduced bilateral activation of the brainstem corresponding to the spinal trigeminal nuclei when compared to controls.
36
Interestingly, this activation of the spinal trigeminal nuclei demonstrated an increase in the days approaching the next migraine attack, almost allowing a prediction of the in general unpredictable headache episodes
37
(Figure 3).
The BOLD response of the trigeminal nucleus to noxious trigeminal stimulation is reduced in interictal migraineurs (insert). In the days prior to the next migraine attack, this response increases substantially suggesting almost a predictability of the so far unpredictable headache attacks, modified from Stankewitz et al.
37
The same group followed a third approach of functionally assessing trigeminal nociception in migraine. Using the same fMRI-paradigm as the Stankewitz study, 36 Schulte et al. 38 studied one subject on a daily basis over 31 days. The subject experienced three migraine attacks during those 30 days, all remained untreated. Comparing pre-ictal, i.e. 24 h prior to the headache phase, with interictal (60 h distance from the headache phase) identified the hypothalamus and the visual cortex responding different to trigeminal nociceptive stimulation. Using a correlation contrast asking for increase of response over three to four days prior to the headache phase with a maximum response during the headache day, the hypothalamus and visual cortex, but also the pons and spinal trigeminal nucleus were identified. Analyzing psychophysiological interaction of ammonia-induced pain in the seed region hypothalamus, the authors found enhanced functional coupling with the spinal trigeminal nuclei during the pre-ictal period suggesting that the driver of the migraine attack might be the hypothalamus modulating the activity of the spinal trigeminal nuclei, i.e. modulating the perception of trigeminal sensory input. The study further demonstrated an influence on pontine areas, which will be discussed in detail below.
In summary, the earliest clinically comprehensible phase of the migraine attack, the premonitory phase, might be a key to our understanding of migraine pathophysiology. Being able to provoke attacks using GTN as well as scanning during various time points of the migraine cycle has proven useful in identifying the hypothalamus as a likely structure driving the individual attack. Further studies investigating what in turn might regulate the hypothalamus, be it hormonal, vascular, more complex events such as CSD, would be a next step to deepen our understanding of migraine pathophysiology.
Aura
In up to a third of migraine patients, 39 attacks are associated with transient focal neurological symptoms called the aura. 5 Most often, these symptoms are visual disturbances 40 but may also include sensory, speech/language and motor symptoms 5 and sometimes also higher cortical functions. 41 Aura typically may begin before the headache, but in a significant number of patients, headache and aura may occur simultaneously 42 and aura may also occur in the absence of headache.
The aura is often perceived as having a “spreading” character (Figure 4), and when more than one aura symptom is reported, they tend to occur in succession
40
suggesting an underlying mechanism that propagates slowly along adjacent brain tissue.
Typical propagation pattern of a visual migraine aura. The figure depicts the right visual hemifield and the travelling visual migraine aura, with the numbers indicating the time passed (in min) since first occurrence (a). Here, the visual disturbance is projected onto a flat model of the primary visual cortex by reversed retinotopic mapping (b). Used with permission and adapted from Dahlem and Hadjikhani.
139
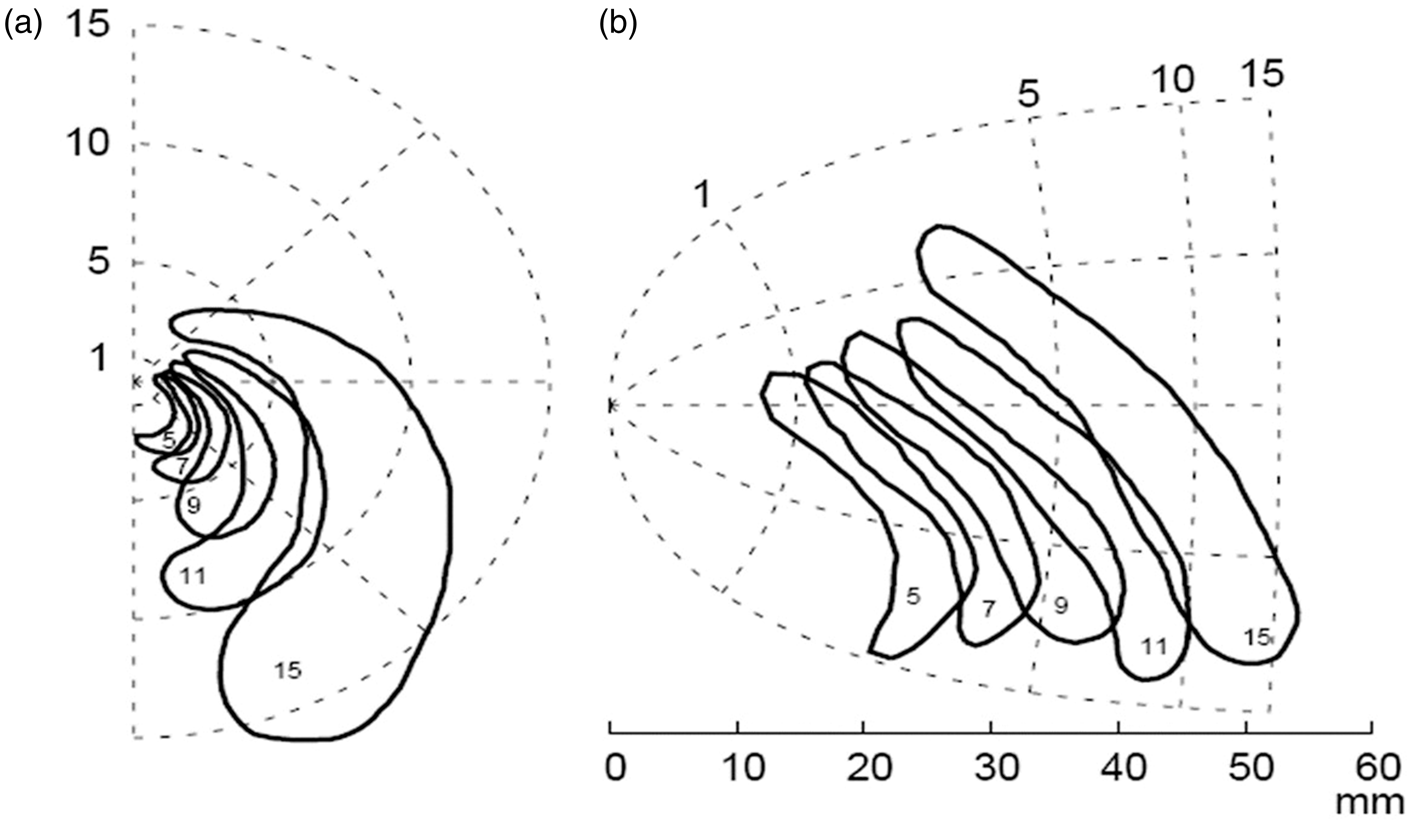
One possible mechanism for the aura is the CSD as described by Leão. 8 CSD is a wave of depolarization of neuronal and glial membranes that propagates in brain tissue at a rate of approximately 3 mm/min. 43 Several animal studies have found increased cortical blood flow during the CSD wave, followed by a long-lasting oligemia.44–46
Direct evidence for the occurrence of CSD in human brain in situ has been obtained using subdural electrophysiological recordings. 47 Most often the aura resolves spontaneously within 15–30 min, and migraine aura is notoriously difficult to provoke experimentally, 48 which hampers imaging studies of this elusive phenomenon.
Still, brain hemodynamics has been measured during aura by single photon emission-computed tomography (SPECT), CT (computed tomography), magnetic resonance imaging (MRI) and positron emission tomography (PET).
The first systematic recordings of migraine aura came from a large series of patients undergoing carotid arteriography. In some patients, migraine aura could be elicited and blood flow measured using intra-arterial [133Xe] SPECT. In a landmark paper from 1981, Olesen et al. 49 reported blood flow changes in eight patients, of whom six had migraine with aura. CBF dropped in the posterior part of the hemisphere, simultaneously with neurological symptoms, headache, or both. The oligemia then spread anteriorly over 15–45 min, without any regard for vascular territories of the large cerebral arteries. In most patients with migraine without aura, migraine attacks caused no changes in CBF.50,51 In some cases, however, oligemia has been reported in MO patients in attacks without reported aura symptoms. 52 In two separate PET studies, posterior hypoperfusion, with an adjusted rCBF decrease around 10% was found in attacks without aura.53,54
In patients with hemiplegic migraine, a rare subtype of migraine with aura with paresis during the aura, 5 rCBF was recorded by the intracarotid [133Xe] SPECT method. In one case series, focal hypoperfusion originated in the frontal lobe, spreading posteriorly to involve the precentral and postcentral regions. 55 In parallel with the changes in rCBF, the patients developed transient motor and/or sensory deficits and subsequently severe headache. In another case series of patients with hemiplegic migraine, 9 out of 13 patients developed aura after the arteriography and were examined by a series of regional CBF measurements. 56 In eight of the nine patients, changes in the rCBF were seen as a spreading oligemia, originating in the posterior part of the brain and progressing anteriorly through the parietal and temporal lobes. There was not a perfect match between neurological symptoms and regional oligemia, because in some patients, the oligemia spread to other regions without giving rise to new focal symptoms. Interestingly, in seven patients, oligemia also appeared in the frontal lobe, apparently independently of the posterior oligemia, indicating that the spreading wave could have several points of origin – a finding not reported in migraine with typical aura.
Two studies of spontaneously occurring attacks of migraine with aura (including hemiplegic migraine) used SPECT to measure rCBF. In 8/11 patients with aura, marked rCBF abnormalities were found, most often as unilateral posterior hypoperfusion (seven of eight cases) in areas corresponding to the focal neurological symptoms. 57 Twelve patients with migraine without aura showed a normal rCBF pattern during an attack. The authors calculated the velocity of the spreading oligemia to be 2.2 ± 0.3 mm/min, which is similar to what Lashley 58 (based on observations on his own visual auras) and Leão 8 reported.
In spontaneous attacks of migraine with aura, SPECT-imaging between 0.5 and 2.5 h after onset of the attack demonstrated regional hypoperfusion in the cerebral hemisphere corresponding to the aura symptom, which was followed by hyperemia in the same region. 59 Alterations of CBF were unilateral and involved the posterior part of the brain. However, in patients with motor deficits, flow defects were also found more frontally. In juvenile migraine patients with aura, SPECT scans showed consistently hypoperfusion in areas corresponding to the neurological symptoms.60,61
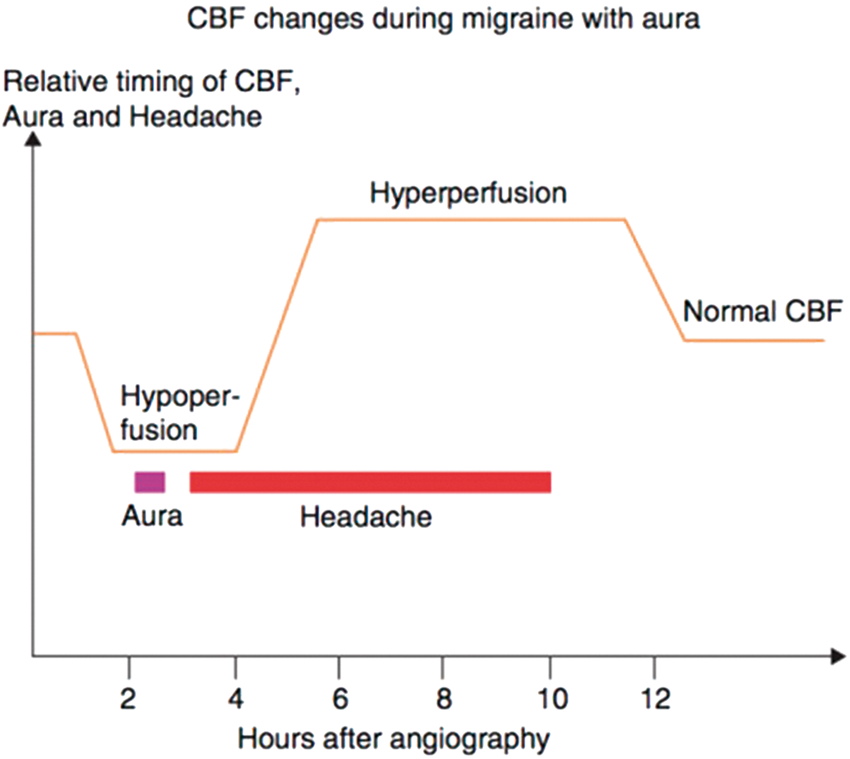
A summary of these studies using SPECT by Olesen et al.
62
concludes an initial reduction of rCBF in the aura phase, followed by headache with a gradual change of rCBF from abnormally low to abnormally high without apparent changes in headache (Figure 5).
Schematic illustration in migraine with aura of the temporal relation between angiography (time 0 h), hypoperfusion, aura, headache, hyperperfusion, disappearance of headache, and disappearance of hyperperfusion. Note the discrepancy between the headache and cerebral blood flow changes, adapted from Olesen et al.
62
In the acute phase of migraine aura, standard structural neuroimaging is unlikely to reveal anything and is rarely indicated. 63 Using dedicated MRI stroke-protocols, cerebral hypoperfusion was reported in migraine with typical aura64,65 and at the onset of aura in familial hemiplegic migraine.66,67
Perfusion- and diffusion-weighted MRI was performed during spontaneous visual auras in four migraineurs. A moderate focal reduction in rCBF and cerebral blood volume was revealed in the occipital lobe during multiple spontaneous migraine visual auras. 68 In an extension to that study, a significant rCBF decrease (27%) was found in the occipital cortex contralateral to the affected hemifield, without significant changes in other brain regions. 69
In a seminal paper by Hadjikhani et al., 70 high-field functional magnetic resonance imaging (fMRI) study, blood oxygenation level-dependent (BOLD) response to checkerboard pattern stimulation was tracked near-continuously during visual aura in three subjects, experiencing five attacks. During symptoms, BOLD-response changed with reduced amplitude and initial increase of mean BOLD followed by a decrease (“depression”) contiguously spreading over the occipital cortex, congruent with the retinotopy of the visual percept. The velocity of the signal change was 3.5 ± 1.1 mm/min, and like CSD, the spreading phenomenon did not cross prominent sulci (e.g. the parieto-occipital sulcus). In visually triggered migraine with aura, 71 fMRI could show changes in cortical perfusion slowly propagating along the occipital cortex with a velocity from 3 to 6 mm/min. This suggests that in human, CSD is the pathophysiological correlate of migraine aura. In animal studies, CSD was associated with an increased permeability of the blood–brain barrier (BBB). 72 In humans, however, the BBB remained intact during the headache phase of spontaneous migraine with aura 73 as well as in GTN-induced migraine attacks. 74
In a [I5O]-water PET study, red wine susceptible migraine patients were provoked with 25 ml of red wine, 75 and seven aura examinations were obtained in six individuals. The authors reported significantly reduced blood flow and metabolism of the primary visual cortex during headache, without any changes during the aura. In a corresponding study in patients with migraine without aura, migraine attacks induced by red wine, did not alter CBF. 76
In summary, the link between migraine aura symptoms and hemodynamics is complicated and encompasses a number of conflicting results. Aura is short-lasting, fully reversible but difficult to provoke experimentally, thus hampering detailed neuroimaging of the cerebral hemodynamics during aura. In many reports, gradual spread of oligemia was not always evident, and does not always correlate to the aura symptoms. In some cases, global oligemia was found, even when patients reported one-sided symptoms, and CBF changes in migraine without clinical aura symptoms also raises the possibility that migraine aura may in some cases be clinically silent. In many cases, stroke-imaging has been able to capture the aura, which may be a feasible way for future aura studies.
Headache
Based on the presumed vascular origin of migraine pain,9,10 a number of studies have examined how dilation of cerebral and meningeal vessels is related to migraine pathophysiology.
Provoked attacks
NO is a highly diffusible, lipophilic molecule released from endothelial cells and stimulates cGMP synthesis 77 causing smooth muscle relaxation and vasodilatation. 78
Sicuteri et al.
79
were the first to study the relationship between NO-donor GTN-induced headache and reported that migraine patients were more sensitive to sublingual GTN than healthy controls, and this lead to the development of a human experimental migraine model
80
that has been extensively reviewed26,81 (Figure 6).
The experimental set-up of a human migraine study, modified from Olesen et al.
140
Headache intensity is recorded on a verbal rating scale from 0 to 10 (0, no headache; 1, a very mild headache (including a feeling of pressing or throbbing); 5, moderate headache; 10, worst imaginable headache).
80
At baseline, and then at fixed and predefined intervals, the hemodynamic effects of the infusion are recorded, and may include recordings of the intra- and extracranial arteries. Vital signs such as heart rate and blood pressure are measured continuously throughout the study. The studies can be tailored to assess certain aspects. If the focus is to address imaging or plasma levels of a given substances, scans and blood samples are conducted at baseline, and when the effects are expected as well as after treatment of the attack.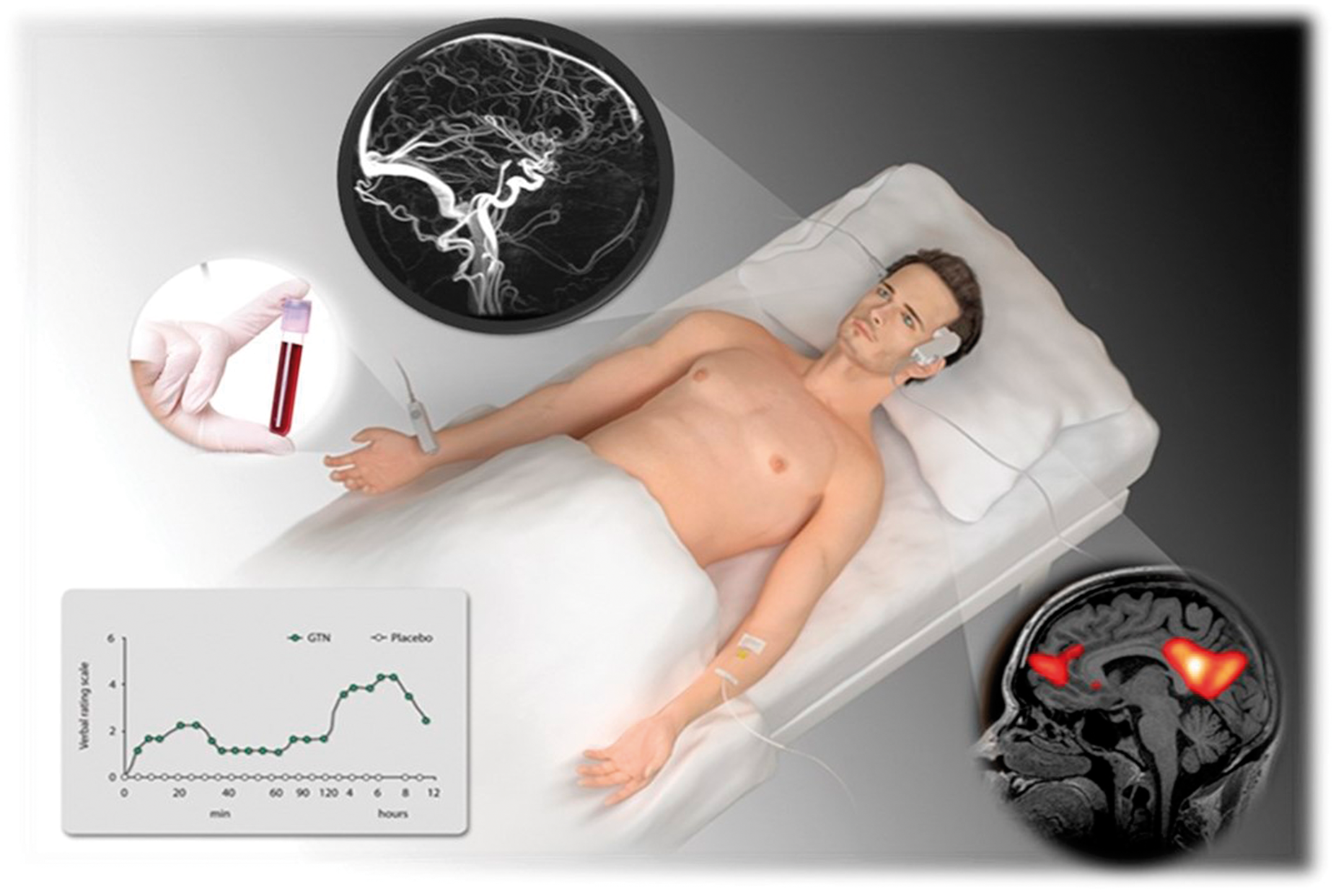
GTN was used in a number of studies in migraine patients, that all suggested vasodilatation during the immediate headache.25,82–85 GTN infusion caused more pronounced dilation of extra- and intracerebral arteries in migraine patients than in controls. The onset of the immediate GTN-induced headache in healthy volunteers is correlated to dilation of the MCA, 86 but vasodilation outlasts the headache.86,87 Cerebrovascular CO2 reactivity is increased in patients with migraine with aura, 88 and a study comparing CO2 reactivity found similar results during GTN-induced and spontaneous migraine attacks, thus supporting the validity of the GTN model. 89 PET-studies have also reported brainstem activation after GTN90,91 exactly as reported during spontaneous migraine attacks.92,93
Other endogenous signaling molecules that could act as migraine triggers are some neuropeptides. 94 Neuropeptides are involved in a wide range of biological functions, including pain and vasodilation, and they act at metabotropic or G-protein-coupled receptors 95 often with cAMP as a major second messenger. 96
Animal models of headache and pain suggest a modulatory role of CGRP in nociceptive transmission.97,98 In migraine patients, CGRP induces migraine99,100 and a reduction of blood flow velocity on ultrasound of the middle cerebral artery (MCA) without change in CBF suggesting vasodilation. 101 In healthy volunteers pretreated with the CGRP receptor antagonist BIBN4096BS, CGRP infusion caused extracranial dilation that could be prevented by BIBN4096BS. 102 In migraine patients, using high-field MRA, it was found that CGRP-induced migraine without aura is associated with dilatation of extra- and intracerebral arteries and that the headache location is associated with the location of the vasodilatation. 103 In addition to such vasodiation, fMRI studies support that CGRP also modulates nociceptive transmission in the trigeminal pain pathways. 104
Vasoactive intestinal peptide (VIP) and PACAP are vasoactive peptides belonging to a family of structurally related peptides. 105 In human provocation studies, systeic administration of VIP induces only a short-lasting and mild headache in healthy volunteers. 106 In a similarly designed, randomized, double-blind crossover study, 12 patients with migraine without aura received VIP or placebo. Despite a marked dilation of cranial arteries, VIP did not trigger migraine attacks. 107 In healthy volunteers, PACAP caused headache in 11 of 12 subjects 108 and induced headache was associated with prolonged dilatation of the middle meningeal artery but not of the MCA. 109 The marked difference in migraine-induction between the two very similar neuropeptides was studied in a head-to-head comparison between VIP and PACAP. 110 PACAP-infusion induced migraine-like attacks in 73% of MO patients compared to 18% after VIP. The vasodilating effect of PACAP also lasted longer than that of VIP. 110
Based on human experiments reporting no linear relationship was found between experimental immediate headache and dilatation of the intra- and extra cerebral arteries. 111
Spontaneous attacks
In one study, 10 patients with unilateral headache were studied both during an attack and after 5 headache-free days. Ultrasound was used to measure blood flow velocity in the MCA. During migraine, the MCA velocity on the headache side was significantly lower than that on the non-headache side, with no change in rCBF suggesting an intracranial large arterial dilatation on the headache side, estimated around 20%. 50 Such reduced MCA velocity suggestive of arterial dilatation during headache was supported by some112,113 and contradicted by other studies leaving the question of a pathophysiological role for vascular dilatation during migraine attacks open.114–116
The different results could be related to the fact the studies used an indirect measure of vascular diameter. Also, timing of imaging varied markedly between studies, between patients within the studies and even between different migraine subtypes, as noted in one study where the interval between headache onset and transcranial Doppler was shorter in case of migraine with aura. 117 In a recent systematic review, it was concluded that spontaneous migraine attacks are not accompanied by blood flow velocity changes in the MCA. 118
Neuroimaging can be used to directly and accurately assess vascular changes during headache under standardized circumstances.119,120 An elaborate study of twenty migraine attacks induced by nitroglycerin reported no significant changes in cerebral artery diameters or CBF during migraine headache. 121 The most definitive study to date included 19 patients who were scanned during migraine. Migraine pain was not accompanied by extracranial arterial dilatation, and by only slight intracranial dilatation. 122
In summary, vasodilation seems to be involved in migraine induction, but migraine can occur without vasodilation, 123 and vasodilation can occur without inducing migraine. 107 It seems that vascular changes, are unlikely to be the primary cause for head pain in migraine. 124 The interplay between vascular changes and pain is not resolved, and further studies are necessary to complete the complex picture of migraine pathophysiology.
Resolution phase
Once the headache subsides a large number of patients still experience some symptoms lingering on for hours to days suggesting that the attack is still far from over. 125 This phase of the attack is not well-defined, but the suffering caused by postdrome symptoms can be very real and even impact the ability to work or interact with family or social life. 126 Studies report that the majority of migraine patients experience such postdromal symptoms127,128 including tiredness, mood changes, weakness and cognitive impairment. Some of these symptoms are also described in the premonitory phase. 30 It thus remains a possibility that these symptoms are present all along the attack.
This phase of the attack is under-studied but never the less a significant cause of disability. 129 Imaging studies of the resolution phase are scarce, but from the CBF studies in the 1980 s, it is clear that cerebral hyperperfusion outlasts the headache phase 62 (Figure 5). In the remarkable 30-days fMRI study, only the visual cortex showed stronger activity as a response to pain compared to the ictal phase. 38 This is line with a previous PET-study reporting that pain lead to increased activation in the visual cortex interictally. 130 A number of other PET studies also reported cortical or brainstem perfusion changes that persisted even after succesfull administration of sumatriptan for migraine headache.53,93
From a scientific point of view, postictal studies may in some respects be easier to conduct than studies aiming for the short-lasting aura symptoms or the very inset of headache, because there is time to set up scanners and prepare patient, equipment and study medication. Studies in this phase of the attack may shed light on where in the brain activation persists after headache, clarify endo-phenotypes of postdromal migraine and study treatment effects.
Cluster headache
In respect of functional brain imaging, the unpredictability of spontaneous CH attacks is as obvious as for migraine described above. Therefore, only a few studies have managed to image CH attacks. Similar to migraine, triggering such attacks for the purpose of brain imaging was a way forward. In the seminal work by May et al., 131 attacks in nine CH patients, who were in-bout, were triggered using GTN-inhalation. The authors used [15O]-water PET to assess rCBF during baseline, GTN-inhalation, headache and pain-free by sumatriptan. During GTN-induced headache, there was activation in regions of pain processing, such as the ventroposterior thalamus, the anterior cingulate cortex, and the insula. Importantly, there was further activation of the inferior hypothalamus grey matter, which was specific for the pain state in-bout and absent during out of bout and in controls. With the same method, Bahra et al. 91 triggered headache in a patients who suffered from both, migraine and CH using GTN. Importantly, he solely developed headache of migrainous, but not CH phenotype. The functional neuroimaging revealed consistently alterations of rCBF in areas typical for migraine 93 including the dorsal rostral brainstem, but not in the hypothalamus suggesting that migraine and CH are not only different entities on clinical grounds, but also behave differently in paraclinical studies. When comparing nine CH patients in bout during GTN-triggered with control subjects “out of bout” during mild (non-cluster) GTN-headache, specific activation of the hypothalamus was confirmed. 132 The authors further studied vasodilatation of the internal carotid arteries. They found, as expected, vasodilatation of the internal carotid arteries during GTN application. This activation of blood flow persisted and even increased during the CH attack and further was present in one patient, who experienced a spontaneous, i.e. untriggered, CH attack in the scanner. This suggests that CH is a neurovascular headache disorder with the hypothalamus being of major significance for its pathophysiology. Based on the results of these studies, the hypothalamus was chosen as the target for deep-brain stimulation in patients with chronic CH. 133 In such patients, May et al. 134 compared rCBF using [15O]-water PET during stimulator switched on and switched off to understand the mechanism of deep-brain simulation. The authors identified a complex modulation of the pain network by hypothalamic stimulation including activation of the ipsilateral trigeminal nucleus and thalamus.
The occurrence in “clusters” with the two phases “in bout” opposed by “out of bout” is typical for the condition. The “switch” turning one phase into the other, however, is unknown, but would be crucial for our understanding of this severe headache. Studies comparing both phases are far less difficult from a logistic perspective and are thus numerous. The results, however, are less clear than the hypothalamic activation during CH attacks as described above. Sprenger et al. 135 applied [18F]-FDG PET in 11 CH patients during the cluster period to compare brain metabolism within subjects (i.e. with “out of bout”) and with healthy controls. They identified increased metabolism in several areas of pain processing, such as the cingulum, prefrontal cortex, insula, thalamus and temporal cortex. A decrease of metabolism was found in the cerebellopontine area. Similarly, Yang et al. 136 compared brain structure in 12 CH patients between “in bout” and “out of bout” and identified grey matter volume increase in the left anterior cingulate, insula and the fusiform gyrus. “In bout” (n = 49) compared to age- and gender-matched controls (n = 49) revealed grey matter volume reductions in the bilateral middle frontal, left superior and medial frontal gyri. 136 Both studies show some structural and functional congruence indicating a dysfunction of top-down modulation of nociception being associated with the shift from “out of bout” to “in bout.”
Conclusion & future directions
Studying hemodynamics of neurological disorders allows a conclusion in respect of both, vascular mechanisms and, by studying neurovascular coupling, brain dysfunction. The episodic nature of the two most frequent and debilitating primary headache disorders, migraine and CH, challenges the systematic study of the actual paroxysmal event. In addition to spontaneous events, provocation models have been utilized and dramatically increased our understanding of these conditions.
In migraineurs, hypothalamic activation in the premonitory phase, i.e. before the occurrence of any pain, highlights that the attack starts within the brain. Typical migraine aura has been extremely difficult to trigger with only few studies demonstrating the hemodynamic alterations in the cortex supporting the hypothesis of CSD as the underlying event. Various neurotransmitters have been tested to trigger migraine headache suggesting an important role for NO, CGRP, and PACAP, which all are potent vasodilators. The induction of migraine-like headache by sildenafil without vasodilatation and the induction of vasodilatation without triggering headache by vasoactive intestinal peptide, however, suggested that vasodilatation is more likely an epiphenomenon than the key pathophysiological event.
The identification of hypothalamic activation in CH has demonstrated an objective difference to migraine as already suggested by the differential clinical presentation. In its chronic and most debilitating subtype, such report of a new possible target has led to new treatment possibilities.
The search goes on for biomarkers in the hope that both migraine and CH will show both a vascular and a neuronal fingerprint. In addition to the advances of understanding headache pathophysiology, provocation models might in the future help to study both acute and prophylactic therapy in the different phases of headache under carefully planned circumstances.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.