
Abstract
Rapid revascularization is highly effective for acute stroke, but animal studies suggest that reperfusion edema may attenuate its beneficial effects. We investigated the relationship between reperfusion and edema in patients from the Echoplanar Imaging Thrombolysis Evaluation Trial (EPITHET) and Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy (MR RESCUE) cohorts. Reperfusion percentage was measured as the difference in perfusion-weighted imaging lesion volume between baseline and follow-up (day 3–5 for EPITHET; day 6–8 for MR RESCUE). Midline shift (MLS) and swelling volume were quantified on follow-up MRI. We found that reperfusion was associated with less MLS (EPITHET: Spearman ρ = −0.46; P < 0.001, and MR RESCUE: Spearman ρ = −0.49; P < 0.001) and lower swelling volume (EPITHET: Spearman ρ = −0.56; P < 0.001, and MR RESCUE: Spearman ρ = −0.27; P = 0.026). Multivariable analyses performed in EPITHET and MR RESCUE demonstrated that reperfusion independently predicted both less MLS (ß coefficient = −0.056; P = 0.025, and ß coefficient = −0.38; P = 0.028, respectively) and lower swelling volumes (ß coefficient = −4.7; P = 0.007, and ß coefficient = −10.7; P = 0.009, respectively), after adjusting for age, sex, NIHSS, admission glucose and follow-up lesion size. Taken together, our data suggest that even modest improvement in perfusion is associated with less brain edema in EPITHET and MR RESCUE.
Introduction
In acute stroke, early restoration of blood flow to ischemic brain tissue has repeatedly been shown to improve clinical outcomes. Accordingly, revascularization with intravenous tissue plasminogen activator (IV tPA)1,2 or intra-arterial thrombectomy (IAT), 3 and spontaneous revascularization4–7 lead to reduced long-term disability. Such findings support the penumbra hypothesis, which proposes that early revascularization preserves hypoperfused brain tissue at risk of infarction 8 by arresting infarct growth surrounding the core stroke lesion.9–11 However, several studies have also suggested that revascularization may lead to secondary injury.12–14
Post-ischemic reperfusion edema is one potential form of secondary injury, yet studies on the relationship between revascularization and brain edema have yielded conflicting results. Findings from pre-clinical rodent and primate studies suggest that revascularization may result in the development of edema.15–17 In contrast, human studies have shown that persistent proximal occlusion is associated with malignant edema and high mortality.18,19 In this study, we sought to characterize the relationship between reperfusion and edema using serial perfusion-weighted magnetic resonance imaging (PWI) compared with two measures brain edema: midline shift (MLS) and swelling volume. 20
We focused on two cohorts with relatively prolonged periods of ischemia, an IV tPA study [the Echoplanar Imaging Thrombolysis Evaluation Trial (EPITHET)] 21 and an earlier generation IAT study [the Mechanical Retrieval and Recanalization of Stroke Clots Using Embolectomy (MR RESCUE) trial]. 22 Because the interventions tested in both cohorts do not reflect current practice, and because our analysis included patients randomized to each study’s control arm, reperfusion was assessed as a change in perfusion deficit on PWI regardless of treatment modality. Recovery of perfusion deficit, represented quantitatively as reperfusion percentage, was then evaluated for association with morphometric measures of edema. We sought to determine whether improved tissue perfusion after acute stroke was associated with less brain edema.
Subjects and methods
Patient characteristics
Patients enrolled in EPITHET (NCT00238537) and MR RESCUE (NCT00389467) were retrospectively analyzed. Details of the EPITHET 21 and MR RESCUE 22 cohorts have been previously described. Briefly, subjects were enrolled in the EPITHET study from 2001 to 2007 and were randomized to administration of placebo or IV tPA 3–6 h after stroke onset. Subjects were enrolled in the MR RESCUE study from 2004 to 2011, and randomized to IAT or standard medical care within 8 h of stroke onset. Subjects in each cohort received pre-treatment diffusion-weighted imaging (DWI) and perfusion-weighted imaging (PWI), with repeat imaging performed three to five days later in EPITHET, and six to eight days later in MR RESCUE. Due to the baseline differences in the cohorts, analyses were performed in each cohort separately; no pooled analyses were conducted.
Subjects included in the present study had a baseline and at least one follow-up MRI examination with DWI or fluid-attenuated inversion recovery (FLAIR) sequence and PWI. Those with poor quality DWI or PWI (due to motion artifact or technical inadequacy) were excluded if the imaging readers could not delineate a region-of-interest around the DWI lesion or if the concentration curves for PWI sequences could not be generated. All patients enrolled in MR RESCUE had an anterior circulation large-vessel occlusion, while EPITHET included patients without evidence of proximal large-vessel occlusion. This study protocol was reviewed and approved by the Institutional Review Board at Partners Healthcare (protocol 2010P002749) and all subjects or their legally authorized representative originally provided informed consent. This study was carried out according to the guidelines set by the Partners Healthcare Human Research Committee.
Reperfusion measures
Reperfusion has been closely linked to tissue and clinical outcomes.23–25 To investigate the association between reperfusion and brain edema, reperfusion was quantified as the percent change between the baseline and follow-up PWI sequences. The PWI assessments and reperfusion percentage calculations were conducted as part of the original EPITHET and MR RESCUE trials, and the post-acquisition PWI data processing procedures employed have been previously described.21,22 For all patients, reperfusion percentage was calculated as follows: [(PWIbaseline volume – PWIfollow-up volume)/PWIbaseline volume] × 100. In these analyses, an improvement in reperfusion may be due to (1) resolution of the initial occlusion, (2) distal migration of the occlusion, and/or (3) improvements in collateral blood flow in spite of persistent occlusion. We therefore also conducted sensitivity analyses to evaluate whether recanalization status predicted reperfusion percentage, and to assess the correlation of edema metrics with both “successful recanalization” based on serial MR angiography, 24 and separately, “successful reperfusion” dichotomized at >90% reperfusion as originally pre-specified in the EPITHET and MR RESCUE trials21,22 (see Supplementary File).
Perfusion-diffusion mismatch definitions were derived from the original respective studies. Mismatch in EPITHET was defined as [(PWIbaseline volume – DWIbaseline volume)/DWIbaseline volume] × 100.21,22 The penumbral pattern in MR RESCUE was defined as PWIbaseline volume/DWIbaseline volume and dichotomized at 70% or less. 22
Analysis of midline shift
Midline shift was measured in each cohort on the axial view of the follow-up FLAIR or DWI sequence. First, the midline was established by laying a straight line between the anterior and posterior attachment of the falx cerebri. Midline shift was quantified by drawing and measuring a second, perpendicular line at the point of maximal deviation from the midline. In subjects with decompressive craniectomy (DC) for malignant cerebral edema (n = 9 in MR RESCUE), MLS measurements were imputed with the greatest MLS value measured in the corresponding study cohort. All MLS measurements were generated by readers (A-C.O., H.J.I.) blinded to reperfusion status.
Analysis of infarct growth and swelling volume
Midline shift is used as a marker for edema in large hemispheric strokes.26,27 Because EPITHET and MR RESCUE enrolled patients with moderately sized baseline strokes, we also measured brain edema using a second measure, lesional swelling volume. 20 Infarct growth and lesional swelling volumes were measured as previously described20,28 using region-of-interest (ROI) methodology in Analyze 11.0 (Biomedical Imaging Resource, Mayo Clinic, Rochester, MN). In brief, stroke lesion ROIs were outlined on the baseline and the follow-up DWI using a semi-automated seed point method to generate lesion volumes, and change in lesion volume between baseline and follow-up DWI (ΔDWI) was calculated. The component volumes of ΔDWI attributable to infarct growth, swelling, and hemorrhage were distinguished according to our previously described methodology.20,28 Specifically, the baseline and follow-up DWI sequences were co-registered and were examined in the coronal, sagittal and axial planes. New neuroanatomic areas with restricted diffusion were defined as infarct growth and outlined using Analyze 11.0. Swelling volume was calculated based on the following relationship: swelling volume = ΔDWI – infarct growth volume – parenchymal hemorrhage volume. All swelling volume measurements were performed by independent readers (A-C.O., T.W.K.B.) blinded to reperfusion status.
Statistical analysis
Patients included in the present study were compared using Wilcoxon rank sum or the Student’s t test for continuous variables, and the Fisher’s exact test for binary variables. Spearman’s rank-order correlation was performed to evaluate the association between reperfusion percentage and infarct growth volume, MLS, and swelling volume. Wilcoxon rank sum and the Student’s t test were employed to investigate the association of successful reperfusion with infarct growth volume, MLS, and swelling volume, as appropriate. To evaluate the correlations between recanalization status and reperfusion percentage, MLS, and swelling volume, Kruskal–Wallis or analysis of variance tests were used, as appropriate. Multivariable linear regression models were developed to assess the independent effect of reperfusion on MLS and swelling volume. To account for skewed distributions of covariates in these models, the following variables were log transformed: baseline blood glucose, follow-up DWI volume, baseline DWI volume, MLS, and reperfusion percentage. Variance inflation factor (VIF) values were generated for all multivariable models in order to evaluate for multicollinearity, and all VIF were <1.8. A LOESS local regression line was fit for the relationships between reperfusion percentage and midline shift, swelling volume and infarct growth volume, given the skewness of the data. All tests were two-sided and performed with the threshold for significance set at P < 0.05. Because this was an exploratory study, no further adjustment for multiple comparisons was made. Statistical analyses were conducted using JMP Pro 12.0 (SAS Institute, Cary, NC).
Results
Study population
Clinical and imaging characteristics of the study cohorts.
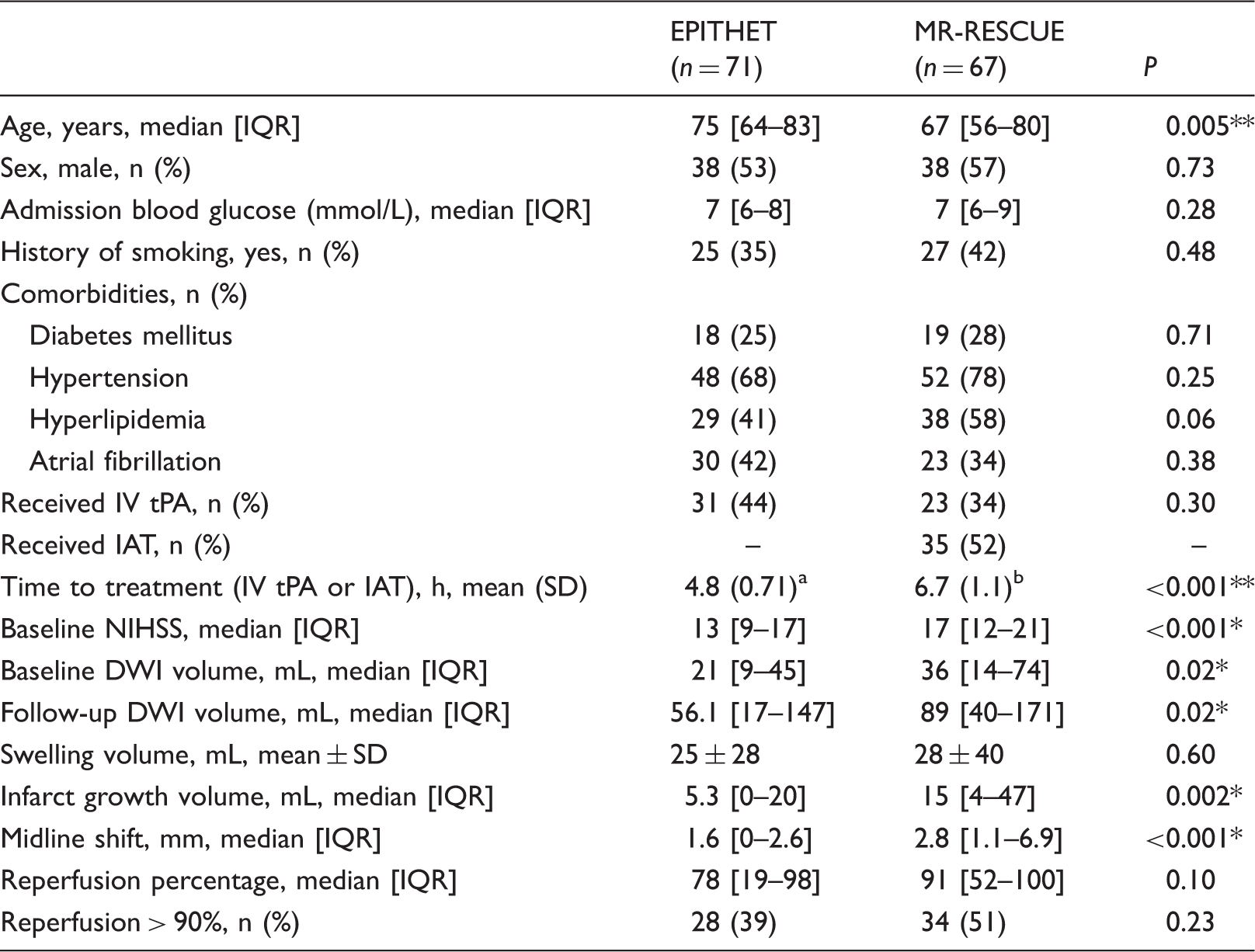
DWI: diffusion-weighted imaging; IAT: intra-arterial thrombectomy; IV tPA: intravenous tissue plasminogen activator; NIHSS: National Institutes of Health Stroke Scale, reperfusion >90%: greater than 90% reduction in perfusion-weighted imaging deficit between baseline and follow-up imaging.
Data are for 31 patients randomized to IV tPA.
Data are for 35 patients randomized to IAT.
t-test, *Wilcoxon rank sum test.
Reperfusion is associated with reduced infarct growth
We next sought to confirm that the degree of reperfusion (i.e., reperfusion percentage) was associated with a smaller volume of infarct growth. As demonstrated in Figure 1(a) and (b), increasing reperfusion percentage was associated with less infarct growth in patients enrolled in both the EPITHET (Spearman ρ = −0.37, P = 0.002) and MR RESCUE (Spearman ρ = −0.42, P < 0.001) cohorts.
Reperfusion is associated with less infarct growth. Increasing percentage of reperfusion is associated with lower infarct growth volume in the EPITHET cohort (n = 71; Spearman ρ = −0.37, P = 0.002) (a), and in the MR RESCUE cohort (n = 67; Spearman ρ = −0.42, P < 0.001) (b). The line corresponds to a smoothing spline fit to the data. In Wilcoxon rank sum testing, successful reperfusion (dichotomized at > 90%) was also associated less infarct growth in EPITHET (n = 71; P = 0.003) (c), and in MR RESCUE (n = 67; P = 0.008) (d).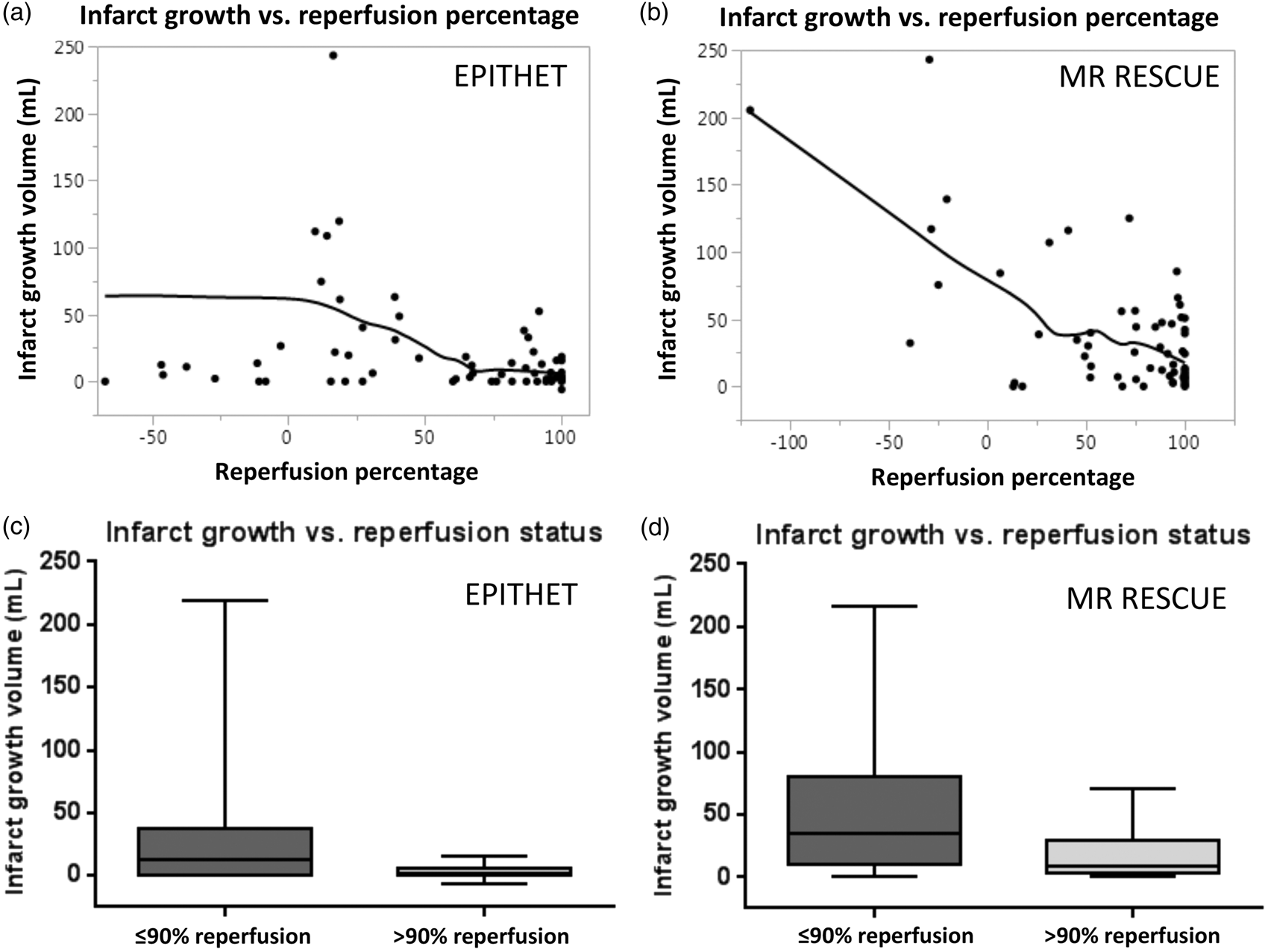
We also analyzed the relationship of infarct growth and reperfusion dichotomized as successful (>90%) or unsuccessful (≤90%) using Wilcoxon rank sum testing. In EPITHET (Figure 1(c)), successful reperfusion was associated with a median infarct growth of 2 mL (IQR 0–7 mL), compared to unsuccessful reperfusion which was associated with a median infarct growth of 12 mL (IQR 0–38 mL; P = 0.003). In the MR RESCUE cohort (Figure 1(d)), successful reperfusion was also associated with less infarct growth (median 8 mL, IQR 3–29 mL) compared to unsuccessful reperfusion (median 35 mL, IQR 10–80 mL; P = 0.008).
Reperfusion is associated with reduced brain edema
Next, we evaluated the association of reperfusion percentage with two separate measures of brain edema: MLS and swelling volume. Increasing reperfusion percentage was associated with less MLS in both EPITHET (Figure 2(a), Spearman ρ = −0.46, P < 0.001) and MR RESCUE (Figure 2(b), Spearman ρ = −0.49, P < 0.001). Higher reperfusion percentage was also associated with lower swelling volume in both EPITHET (Figure 2(c), Spearman ρ = −0.56; P < 0.001) and MR RESCUE (Figure 2(d), Spearman ρ = −0.27, P = 0.026). An example of the measurements of edema in a patient with successful reperfusion is shown in Figure 3, and Figure 4 illustrates an example of unsuccessful reperfusion. We also found similar results when recanalization was used instead of reperfusion (see Supplementary Figure 1) or when reperfusion was dichotomized into successful versus unsuccessful reperfusion (see Supplementary Figure 2). Accordingly, reperfusion percentage was tightly correlated with recanalization status (see Supplementary Figure 3).
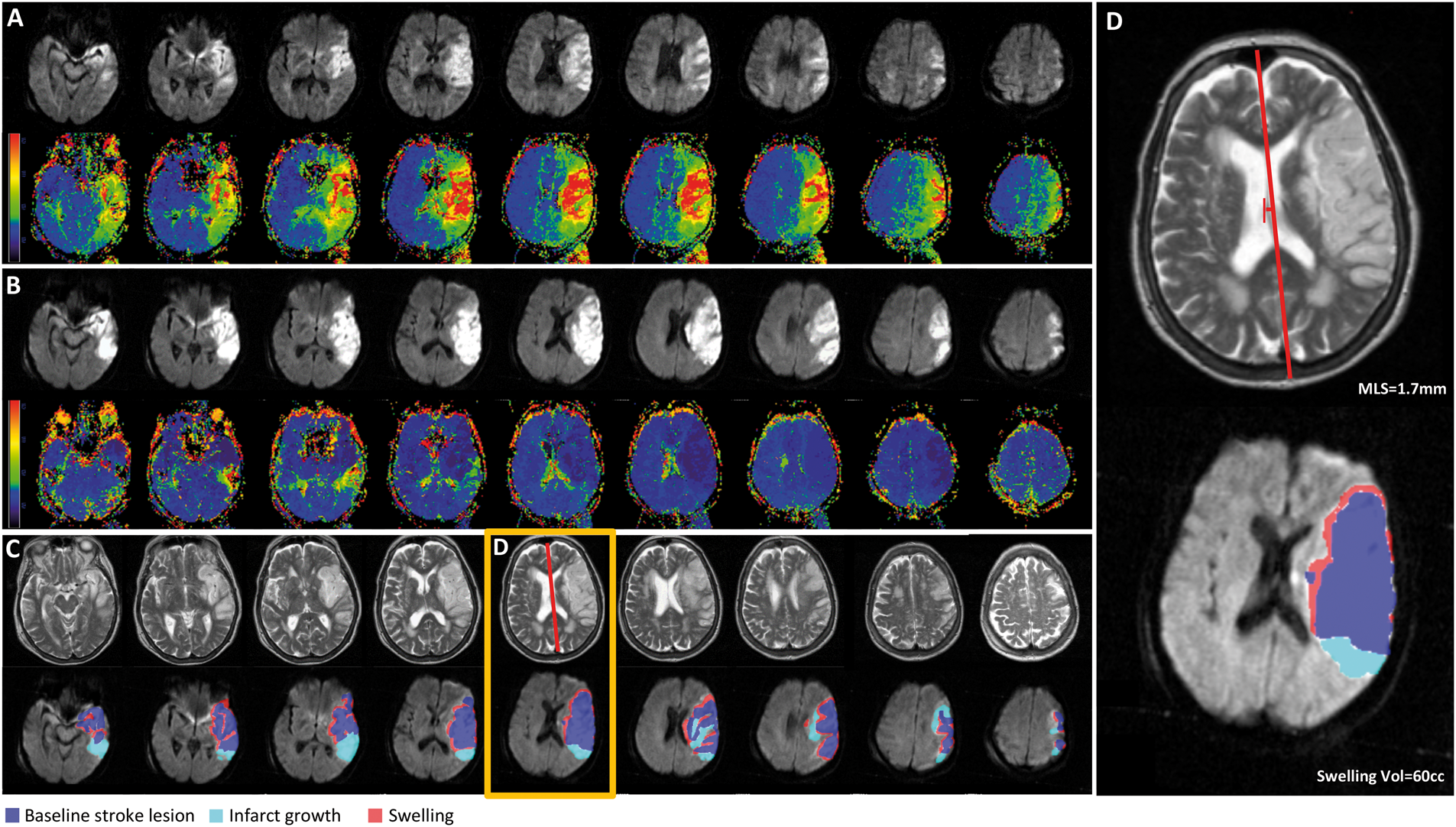
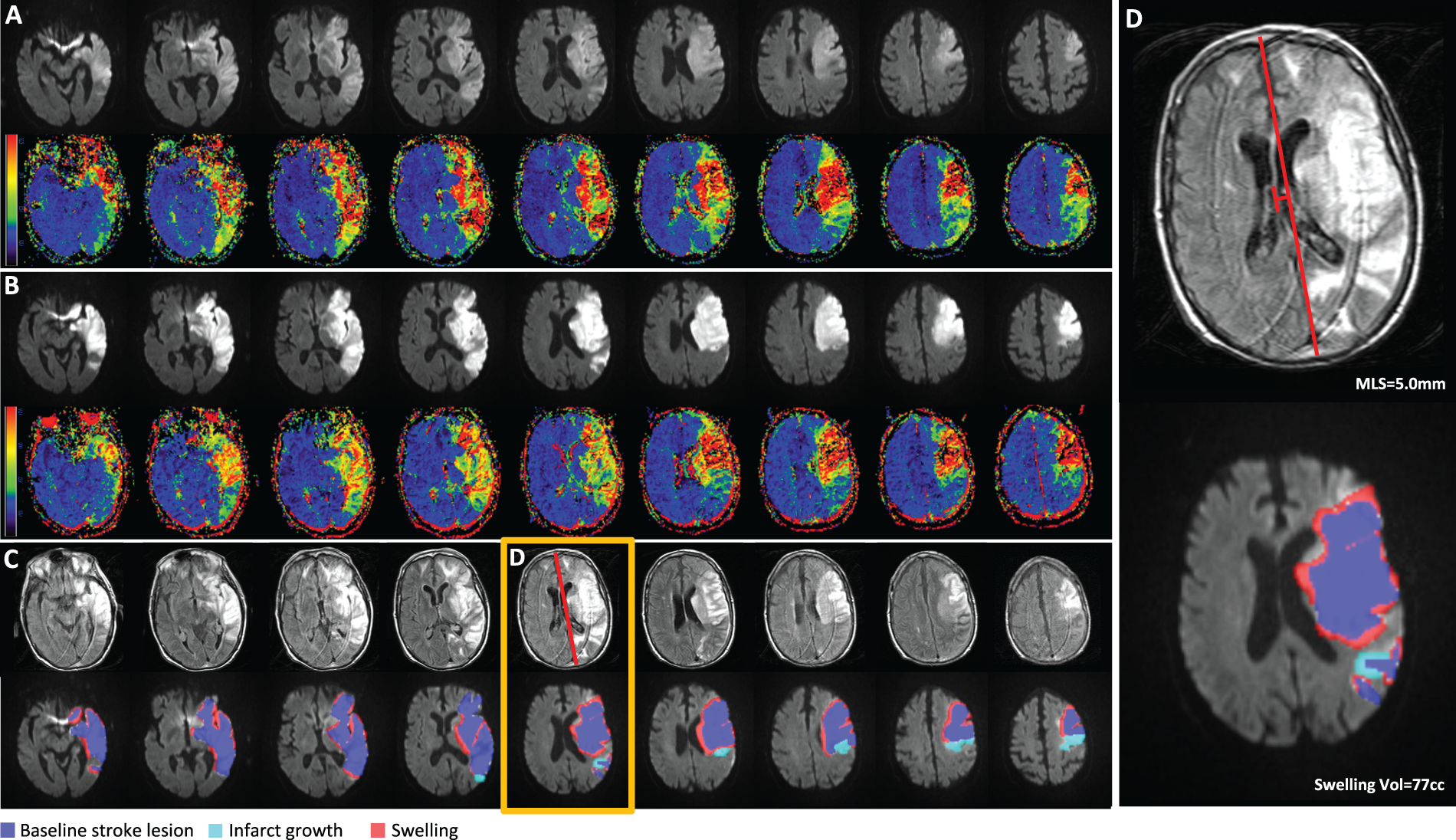
Reperfusion is associated with less brain edema. Greater degree of reperfusion is associated with less MLS in EPITHET (n = 71; Spearman ρ = −0.46, P < 0.001) (a), and MR RESCUE (n = 67; Spearman ρ = −0.49, P < 0.001) (b). Increasing reperfusion percentage predicts lower swelling volume in the EPITHET cohort (n = 71; Spearman ρ = −0.56, P < 0.001) (c), and in the MR RESCUE cohort (n = 67; Spearman ρ = −0.27, P = 0.026) (d). Each line corresponds to a smoothing spline fit to the data; the reported P values were generated from non-parametric analysis. Reduced edema in a patient with successful reperfusion. Example images from a patient enrolled in EPITHET. (a) The baseline DWI and perfusion map reveals the infarct and associated region of hypoperfusion. (b) The follow-up DWI and perfusion map shows the infarct volume and restoration of cerebral blood flow in the region of the infarct. (c) Example of midline shift measurement on T2 sequence and the measurement of infarct growth and swelling volume on co-registered follow-up DWI scan. (d) An individual slice highlighted by the orange box in (c) demonstrates a maximum midline shift of 1.7 mm. The total swelling volume was 60 cc. Greater edema in a patient with unsuccessful reperfusion. Example images from a patient enrolled in EPITHET with a similar infarct size as in Figure 3. (a) The baseline DWI and perfusion map reveals the infarct and associated region of hypoperfusion. (b) The follow-up DWI and perfusion map show the infarct volume and persistent perfusion deficit. (c) Example of midline shift measurement on T2 fluid-attenuated inversion recovery sequence and the measurement of infarct growth and swelling volume on co-registered follow-up DWI scan. (d) An individual slice highlighted by the orange box in (c) demonstrates a midline shift of 5.0 mm. The total swelling volume was 77 cc.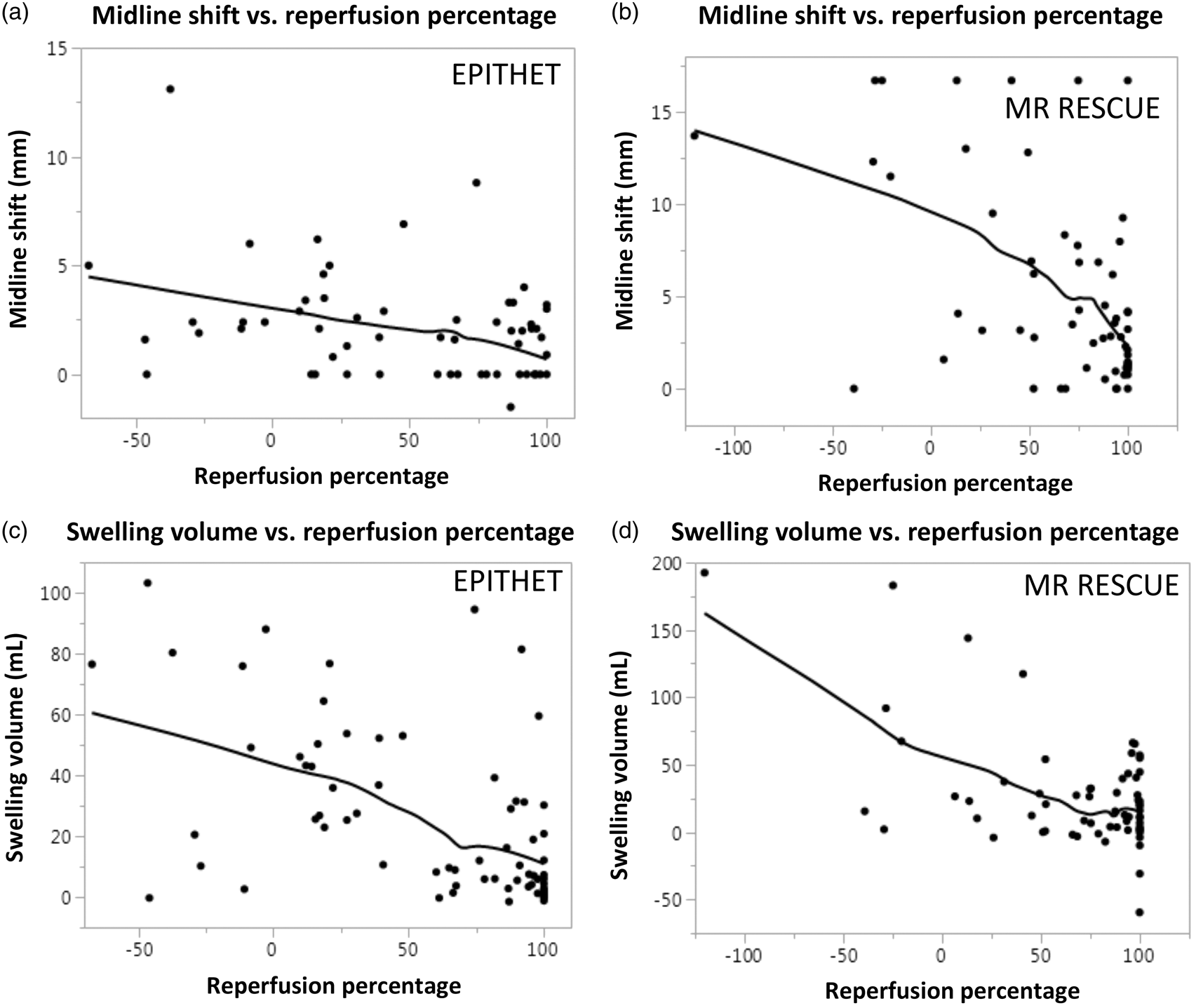
Reperfusion independently predicts reduced brain edema
Univariable and multivariable predictors of midline shift and swelling volume in EPITHET.
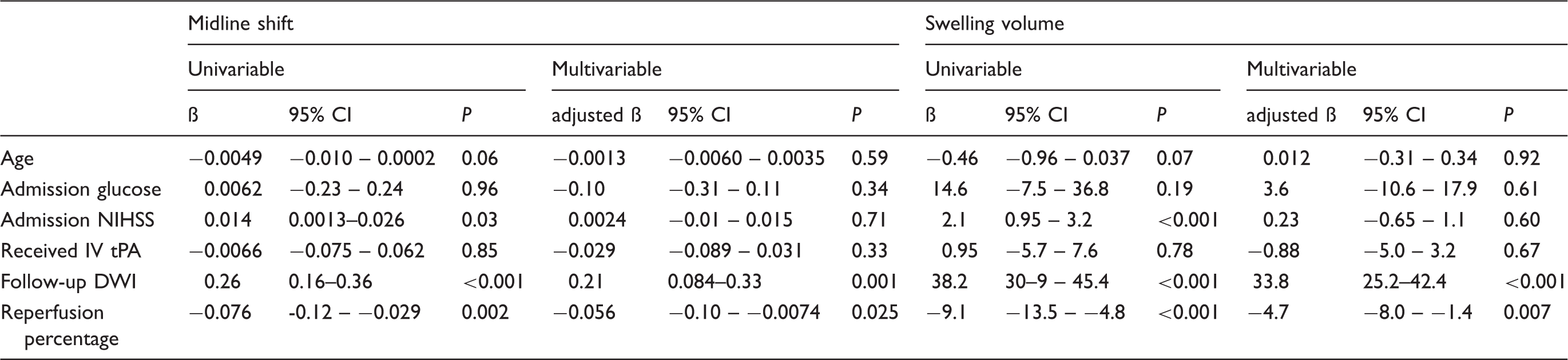
Note: Admission glucose, follow-up DWI volume, reperfusion percentage, and midline shift were log transformed before inclusion in each model. Data are from the Echoplanar Imaging Thrombolysis Evaluation Trial (EPITHET) cohort.
CI: confidence interval; DWI: diffusion-weighted imaging; IV tPA: intravenous tissue plasminogen activator; NIHSS: National Institutes of Health Stroke Scale.
Univariable and multivariable predictors of midline shift and swelling volume in MR RESCUE.
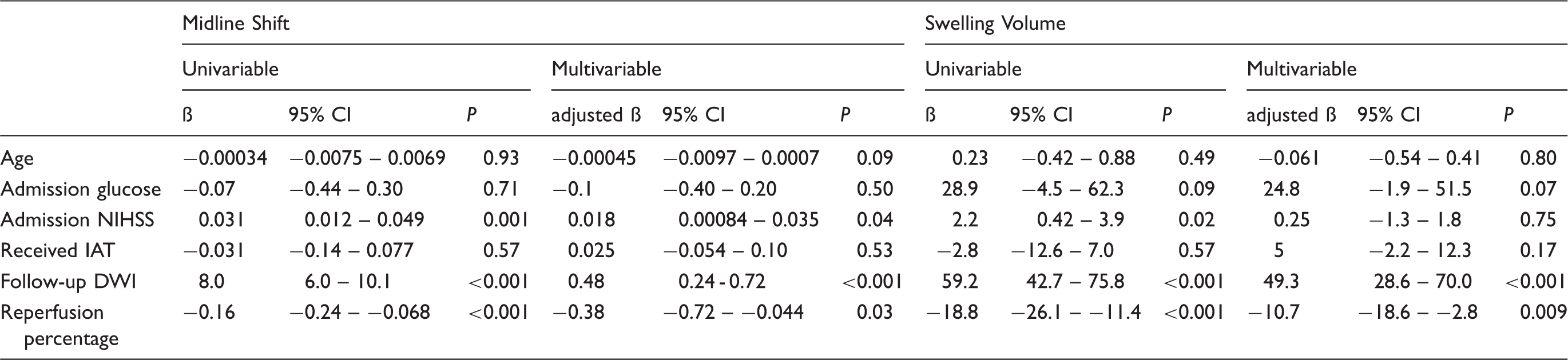
Note: Admission glucose, follow-up DWI volume, reperfusion percentage, and midline shift were log transformed before inclusion in each model. Data are from the Mechanical Retrieval and Recanalization of Stroke Clots Using Thrombectomy Trial (MR RESCUE) cohort.
CI: confidence interval; DWI: diffusion-weighted imaging; IAT: intra-arterial thrombectomy; NIHSS: National Institutes of Health Stroke Scale.
To assess the robustness of these findings, we substituted the follow-up DWI stroke volume with baseline DWI volume and found that reperfusion percentage remained independently associated with reduced MLS and swelling volume (Supplementary Table 1). We also performed additional sensitivity analyses to examine the role of perfusion–diffusion mismatch. Incorporating mismatch percentage in EPITHET did not alter the independent association between reperfusion and reduced brain edema using either MLS or lesional swelling volume (Supplementary Table 2). An analogous model in MR RESCUE did not alter the association between reperfusion and lesional swelling volume, although it did diminish the association with MLS (Supplementary Table 2). Finally, we evaluated whether the relationship between reperfusion percentage and brain edema was time dependent. Although the sample size had limited power, we nevertheless found that reperfusion remained an independent predictor of MLS and swelling volume in each cohort (Supplementary Table 3).
Discussion
In this study, we investigated the relationship between the degree of reperfusion and brain edema in patients enrolled in EPITHET and MR RESCUE. We investigated two quantitative metrics of brain edema (MLS and lesional swelling volume) since MLS may be less sensitive to edema in smaller strokes as compared to large hemispheric infarction. 20 Nonetheless, we found a consistent relationship between reperfusion percentage and each edema metric. In both cohorts, greater reperfusion percentage was associated with decreased infarct growth, MLS, and swelling volume. Multivariable analyses confirmed independent associations, after controlling for other variables, including age, baseline stroke severity, treatment type, and stroke volume.
Taken together, our analyses reaffirm that reperfusion prevents infarct expansion, and also suggests that reperfusion is associated with less brain edema. These data add another dimension to the well-described penumbra hypothesis, wherein reperfusion prevents infarct growth by rescuing hypoperfused tissue.8–11 Our data also raise the possibility that reperfusion may rescue brain tissue by limiting edema-associated tissue injury, and supports the notion that there may be multiple beneficial effects of reperfusion.
Prior studies on the relationship of revascularization and edema in patients have yielded variable or inconclusive results. For example, in large stroke, persistent proximal vessel occlusion has been linked to clinically significant edema. 19 A more recent study reported that large core lesions were associated with edema, but an association with TICI reperfusion and edema was not evident, perhaps because a qualitative approach to edema measurement was employed. 29 Here we report that in two cohorts with relatively delayed time to treatment (EPITHET treatment was initiated at ∼ 5 and MR RESCUE at ∼7 h), a greater degree of reperfusion was associated with lower brain edema. We hypothesize that our quantitative approach to edema measurement revealed a relationship not captured by prior methods.
Our findings are in apparent contradiction with rodent and primate models, which have shown that revascularization can accentuate brain edema.15–17,30 Several possibilities may explain the discrepancy in these studies. First, our analysis of reperfusion percentage may reflect several physiological phenomena. An increase in reperfusion percentage may derive from several processes, including: (1) resolution of the occlusion, (2) migration of the occlusion to more distal vessels, and/or (3) improvements in collateral blood flow. As such, reperfusion percentage, although highly correlated with recanalization status (Supplementary Figure 3), may not solely represent restored blood flow from revascularization. Second, the rate of ischemia and progression to infarction is likely different in humans as compared to animal models. 31 This may result in differing propensities for reperfusion edema. Third, prior animal studies had measured edema shortly after revascularization,15–17 whereas available patient imaging data correspond to substantially later time points, when edema has reached a plateau. Finally, it is likely that reperfusion injury proceeds differently in rodent compared to human brain due to neuroanatomical differences. For example, rodent lissencephaly or disparate collateral flow patterns may be key mediators of the discordant findings between clinical and preclinical studies.
There also are also several potential explanations for the variable findings in clinical studies. One important possibility is that reperfusion edema may be a substantial risk in only select circumstances, perhaps only after late revascularization or in the setting of severe infarction (conditions that are less commonly treated with IV tPA and/or IAT). It is likely that such patients were excluded from enrollment in both EPITHET and MR RESCUE, and as such, our study results may not be generalizable to severe infarction. It is also possible that our study was underpowered to detect the uncommon, but clinically meaningful event of reperfusion edema in late revascularization and/or severe infarction. Additional identification of clinical risk factors for reperfusion edema may help to further clarify the discrepancies among rodent models and clinical studies.
Our study has limitations. Our results may have limited generalizability because the present analyses were performed in a cohort of patients with moderate-to-severe stroke, in the context of two clinical trials. EPITHET patients were randomized to IV tPA 3–6 h after stroke onset, and MR RESCUE patients were randomized to thrombectomy using early generation clot retrieval devices. While these cohorts do not reflect current clinical practice, analysis of these cohorts would tend to bias towards the null hypothesis, suggesting that there may be a robust association between reperfusion and reduced brain edema. Our study does not answer whether or not thrombolysis or thrombectomy directly attenuates brain edema. However, in sensitivity analysis using reperfusion or recanalization dichotomized into successful or unsuccessful categories, each was associated with a smaller amount of edema. Such findings raise the hypothesis that therapeutic reperfusion may mitigate brain edema. Future studies in contemporary thrombectomy cohorts are needed to address this unresolved issue. Finally, the imaging requirements for our analyses necessitated the exclusion of subjects who lacked follow-up MRI or PWI, potentially introducing bias. These individuals may have had more severe strokes making them unstable during each study’s follow-up period, or they may have expired prior to imaging acquisition. While we anticipate, this may have excluded the most severe strokes that would be prone to reperfusion edema, it does not change our main finding that reperfusion leads to decreased brain swelling in most circumstances.
Summary
Taken together, our findings suggest that a greater degree of reperfusion is associated with less brain edema after ischemic stroke. While our data do not exclude the possibility of worse edema in some circumstances, our findings raise the possibility that favorable outcome with IV tPA and IAT may, in part, be linked to less brain edema.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for EPITHET was from the National Health and Medical Research Council, Australia (S.M.D., G.A.D.) and the funding for the MR RESCUE trial was from the NIH P50NS044378 (C.S.K.). The analysis was funded in part by NIH K23NS076597, NIH R01NS099209, and the Andrew David Heitman Neurovascular Research Foundation (W.T.K.). Dr. Kimberly has received research support from Remedy Pharmaceuticals, NIH grants K23NS076597 and R01NS099209, the Andrew David Heitman Neurovascular Research Foundation and AHA 14GRNT19060044.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
Study concept and design: HJI, ACO, MBB, WTK. Acquisition, analysis or interpretation of data: HJI, ACO, MBB, SD, TWKB, BCVC, SMD, GAD, KNS, RJ, JLS, CSK, WTK. Drafting of the manuscript: HJI, WTK. Critical revision of the manuscript for important intellectual content: HJI, ACO, MBB, SD, TWKB, BCVC, SMD, GAD, KNS, RJ, JLS, CSK, WTK. Study supervision: SMD, GAD, CSK, WTK.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.