
Abstract
The fractional pressure ratio is introduced to quantitatively assess the hemodynamic significance of severe intracranial stenosis. A computational fluid dynamics-based method is proposed to non-invasively compute the FPRCFD and compared against fractional pressure ratio measured by an invasive technique. Eleven patients with severe intracranial stenosis considered for endovascular intervention were recruited and an invasive procedure was performed to measure the distal and the aortic pressure (Pd and Pa). The fractional pressure ratio was calculated as
Introduction
Arterial luminal stenosis in coronary or cerebral artery can result in insufficient blood perfusion in the heart or brain, causing ischemia and eventually heart attacks or strokes. However, the severity of stenosis does not necessarily reflect the underlying hemodynamic alteration caused by the vessel narrowness, 1 due to complex anatomic and physiologic variations. Therefore, a parameter gauging the hemodynamic significance of the stenosis is desirable to quantify its functional severity.
Fractional flow reserve (FFR) was first introduced by Pijls et al. 2 and has become a ‘gold standard’ in assessing the hemodynamic function of coronary artery stenosis and guiding the decision of revascularization.3–6 FFR is empirically defined as the ratio of the maximal myocardial flow in the stenotic territory and the maximal myocardial flow in the same territory with the stenosis hypothetically absent, indicating the extent of flow alteration caused by the stenosis. 1 When the ratio is close to one, the stenosis is assumed to be well tolerated with almost no hemodynamic alteration, whereas when the ratio is close to zero, the hemodynamic function of the stenotic artery is completely abolished. A ratio of 0.8 has been clinically accepted as a critical threshold for FFR-guided revascularization according to large randomized clinical trials. 4 Since the measurement of the flow reserve is not straightforward, it was shown by Pijls et al. 2 that FFR can be derived from the ratio of two pressures distal and proximal to the stenosis, respectively. The measurements have to be obtained by a pressure wire, during the procedure of percutaneous coronary angiography, which is invasive and may cause periprocedural complications.
In addition to the invasive procedure, recent studies have shown that CFD can be applied to the anatomic models extracted from images of computed tomography angiography (CTA) and FFR may then be estimated non-invasively. 7 Taylor and his group had studied and proposed a framework of this non-invasive method using 3D CFD models coupled with zero dimensional (0D) lumped parameter models for inflow and outflow boundary conditions.7–10 Their method has been successfully translated and was recently approved for clinical use by United States Food and Drug Administration. These techniques have substantially advanced clinical assessment and interventional management of coronary artery stenosis.
Nevertheless, studies in assessing the functional severity of cerebral artery stenosis remain scarce. Neurologists, Liebeskind and Feldmann, recently urged the introduction of a cerebral hemodynamic parameter as a new guidepost for cerebrovascular diseases and proposed the concept of fractional flow (FF) for cerebral hemodynamics. 11 Leng et al. applied a relatively simple CFD method to calculate the pressure ratio distal and proximal to a cerebral stenosis based on CTA data from patients with the symptomatic intracranial atherosclerosis (ICAS) and concluded that the CFD-derived hemodynamic parameter may be potentially useful in predicting subsequent stroke recurrence in patients with symptomatic ICAS.12,13
In comparison with the CFD methods applied in the assessment of coronary artery stenosis, we believe that these preliminary attempts of using numerical methods for cerebrovascular diseases can be greatly improved.12,14 In this study, we intended to achieve the goal by (1) considering anatomic models of full anterior or posterior circulation with primary collaterals included, (2) applying an instantaneous pulsatile inflow, and (3) incorporating a lumped parameter model to mimic the downstream effects from the distal vessels on the outlet boundaries. Instead of inducing cerebral hyperemia in patients and measuring FFR (the risk of hyperemic stimuli in cerebral artery is unclear), we measured the invasive and non-invasive fractional pressure ratios (FPR and FPRCFD) using pressure wires and the improved CFD model, respectively. A statistical comparison was given to show the feasibility as well as the issues of the CFD method.
Material and methods
Clinical protocol
This cross-disciplinary study applied the same data as in the recent feasibility study of functional assessment of intracranial atherosclerosis. 15 The study was approved by the ethics committee of Beijing Tiantan Hospital followed ethical guidelines of the Helsinki Declaration of 1975 (and as revised in 1983) and the International Ethical Guidelines for Biomedical Research Involving Human Subjects, which allowed the off-label use of the pressure guide wire as an auxiliary investigation tool. Written consents were available for all of the patients included. Patients with ischemic stroke (>3 weeks after onset) caused by severe intracranial atherosclerotic stenosis were recruited during February to March 2015 if they were considered for interventional treatment (with or without stenting). A luminal narrowness ≥70% in the intracranial large artery on digital subtraction angiography (DSA) was considered as severe stenosis. For more detailed inclusion criteria and clinical protocols, please refer to the feasibility study. 15
Additionally, we further required the patients to have (1) CTA scans before and (or) after the interventional procedures allowing for a 3D reconstruction of the cerebral artery and (2) single stenosis in the intracranial large artery, more specifically, in the internal carotid artery or the middle cerebral artery or the vertebral artery or the basilar artery. There were eleven patients with all requirements qualified.
Invasive measurement of FPR
The interventional procedure was described in the feasibility study.
15
Two instantaneous pressure waves,
CFD procedure for the non-invasive measurement
Image acquisition and 3D mesh generation
CTA scans were performed for the patients before and (or) after the endovascular procedures and the data were stored in the standard Digital Imaging and Communication in Medicine (DICOM) format. The 3D geometry of vascular surfaces was then reconstructed by a suite of software, Mimics (Materialise NV, Belgium), and then examined and manually refined by two neurologists. Further processing of the vascular surface and generation of the computational domain (volume mesh) was performed using the ANSYS®ICEM CFD meshing software (ANSYS, Inc., USA). Considering the complexity of the geometry, we used the unstructured tetrahedral cell for domain discretization, and the mesh was finer nearby the vessel wall and at the stenosis where the flow field was of greater interest. The total number of elements is above 1 million and the minimum volume of the elements is about
3D model of blood flow
The heat transfer and the compressibility effects of the vascular wall were neglected and the blood flow was assumed to be a viscous and incompressible Newtonian fluid. The blood parameters were defined by constant density

and equation of mass conservation

The initial conditions were set to zero for all the cases, the details of inlet and outlet boundary conditions are discussed in the next section, and the vessel wall was considered as a no-slip boundary condition. The solver of the 3D blood flow is based on a finite volume approach using ANSYS CFX (ANSYS, Inc., USA) version 14.5. The numerical simulations were carried out on an AMAX server which has a dual eight-core Intel SandyBridge E52687W@3.1 GHz processor and 240 GB of memory. A k-way Metis algorithm was applied for the mesh partition and MPI is used for communication among the processors. The total simulation time
Boundary conditions
The boundary conditions of the CFD model include the inlet condition at the internal carotid artery or the vertebral artery and the outlet condition at the distal cerebral artery with an approximate diameter of The proposed settings of the inlet and outlet boundary conditions. For the outlet condition, we incorporated the outlet at distal artery with a Windkessel model (0D model) to mimic the downstream resistance Rd and compliance C to the outlet pressure 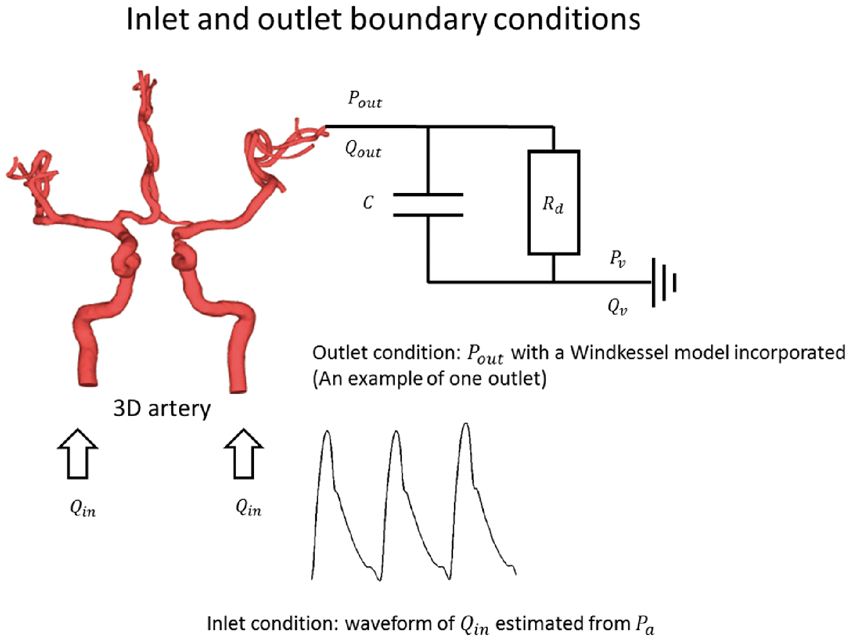
For the inlet boundary conditions, we defined the inflow (

For the outlet condition, we need to define the outlet pressure

Following the assumption in Vignon-Clementel et al.’s recent work, we also assumed the distal venous blood pressure
Statistical analysis
With the non-invasively obtained hemodynamic parameters Pa, Pd, FPR, and the inlet blood flow
Results
Patients’ information and the results of the hemodynamic measures by the invasive (pressure wire) and non-invasive (CFD) methods.
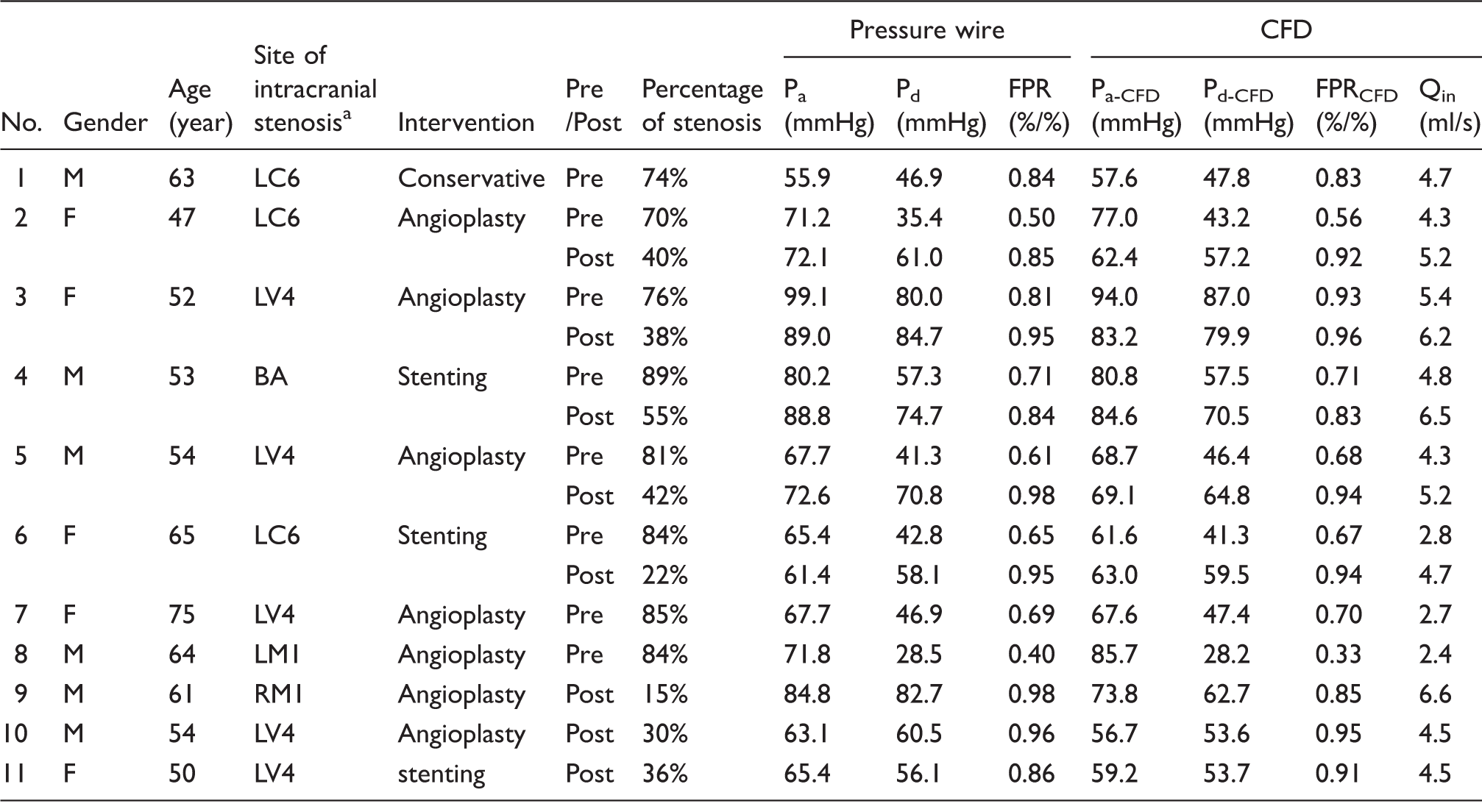
Abbreviation of the types of the stenosis by R-right, L-left, C-carotid, M-middle, V-vertebral, BA-basilar and the number of arterial segment.
In Figure 2, we demonstrate three examples of the 3D hemodynamic simulation. Panel A shows a case with 74% stenosis at the C7 segment of the left internal carotid artery (Case 1 in Table 1). In this case, bilateral anterior cerebral arteries were included in the CFD model as we observed the anterior communicating artery on the CTA scan. The result shows that FPRCFD is 0.84 which means the patient had 84% of blood pressure preserved in the (a), (b, c), and (d, e) are three examples referring to the case 1, 5, and 7 in Table 1, respectively. The blood pressure distribution and the corresponding instantaneous pulsation at 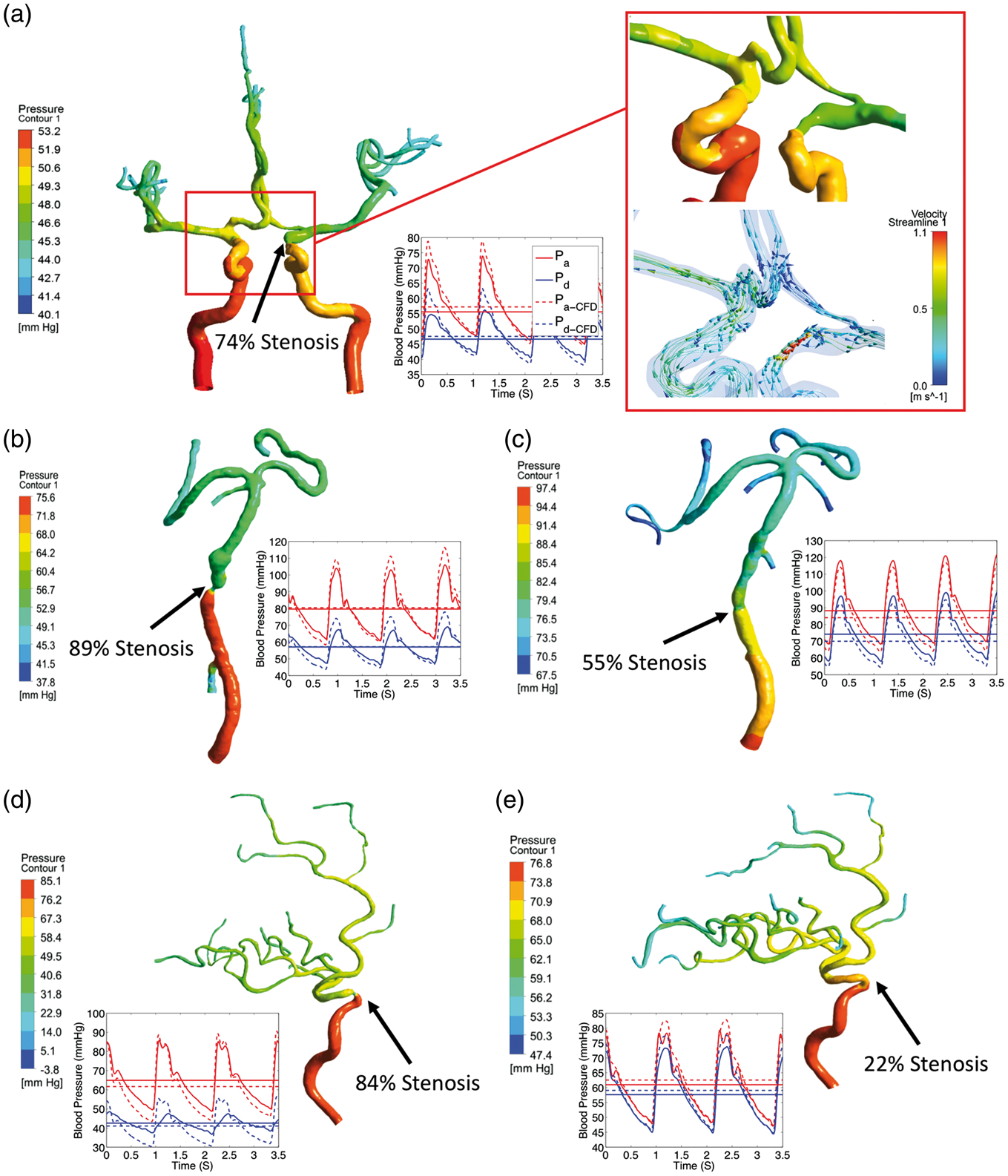
Statistical analysis of the results.
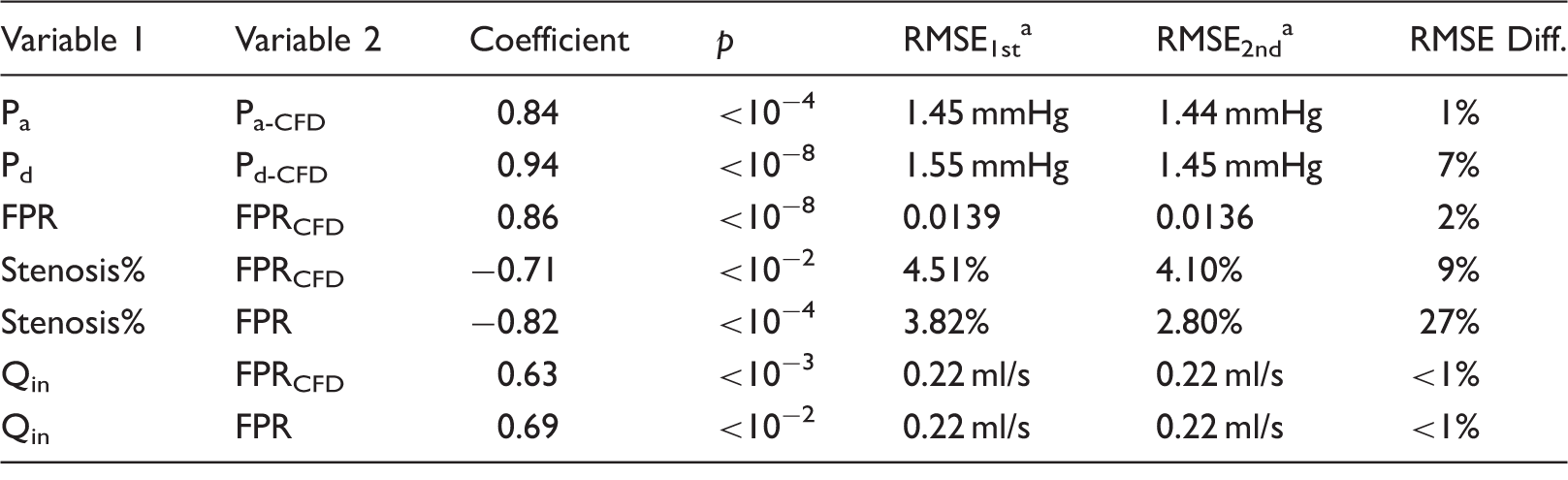
RMSE1st and RMSE2nd are the root-mean-square-error for the first- and second-degree regressions, respectively.
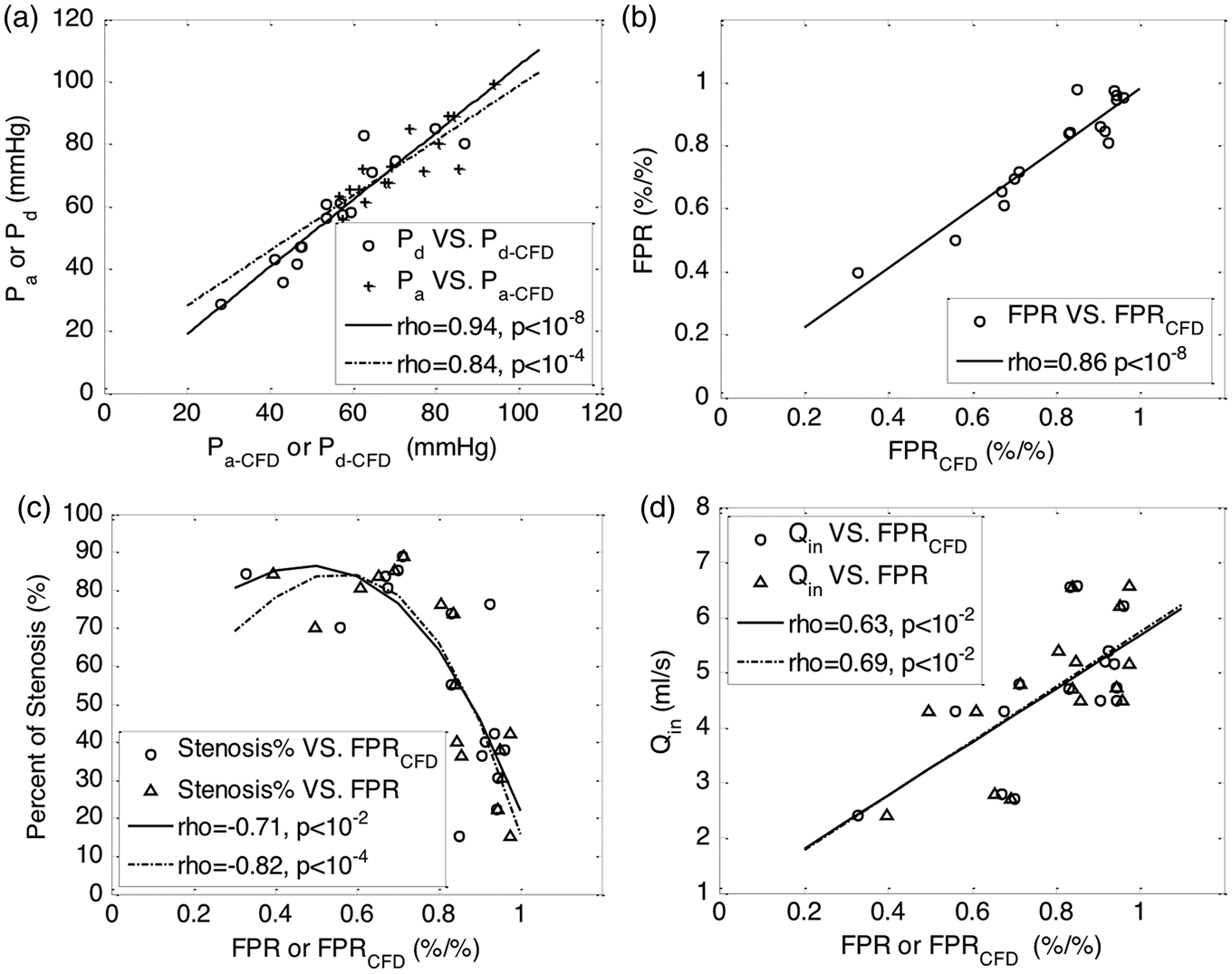
The plots of statistical analysis of the results are given. (a) The invasive blood pressures, Pa and Pd, against the non-invasive pressures,
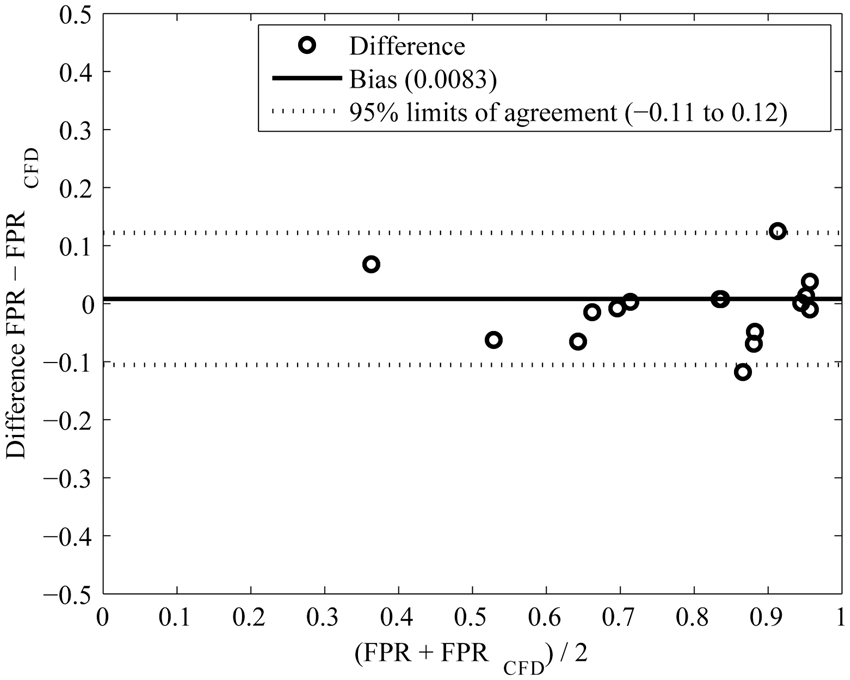
The results of the Bland–Altman analysis are demonstrated. The differences (FPR − FPRCFD) are denoted by circles. The mean difference (bias) between the FPR and FPRCFD is 0.0083 (solid line) and the 95% limits of agreement are −0.11 to 0.12 (dotted line), respectively. Note that two cases at approximately 0.84 (x-axis) are almost overlapped.
Discussion
Main findings
According to our study, the proposed CFD simulation achieved comparable results with the invasive measurements. The computed pressure ratios are highly correlated with the ones measured by the pressure wires (r = 0.88, p < 0.001) and the Bland–Altman analysis shows excellent agreement of the invasive and non-invasive measurements. The numerical simulation results also revealed a significant relationship (r = 0.68, p = 0.0019) between the pressure ratios and the computed carotid artery (inlet) blood flow which is, however, less correlated with the percentage of stenosis (r = −0.59, p = 0.009). This agrees with the findings in coronary arteries 22 where the hemodynamic alteration is only partly determined by the percentage of the luminal stenosis.
Improvement of the CFD model
Incorporation of a two-element Windkessel model to the outlet boundary of the 3D CFD model is more realistic than using a constant or a fixed pulsation of blood pressure which ignores the downstream effects. Our results showed that, by this means, the non-invasive hemodynamic parameters,
Another realistic consideration was the inclusion of primary collateral arteries that allow for mimicking the hemodynamic function of the communicating artery. This may help in some extent to explain our findings that the pressure drop distal to the stenosis was not entirely determined by the stenosis. In Figure 3(c), we found that it was more appropriate to describe the relationship between the percentage of the stenosis and the FPR by a nonlinear relationship than a linear regression. On contrast, in Figure 3(d), the FPR was linearly correlated with the inlet blood flow of the cerebral artery, indicating that this parameter is more directly related to the hemodynamic changes than the anatomic changes caused by atherosclerosis. One typical example is in Figure 2(a) where the patient had only 17% (FPR = 0.83) blood pressure lost across the stenosis with 74% luminal narrowing at C7 of the left internal carotid artery. The CFD simulation showed that there is a right-to-left blood flow across the anterior communicating artery, resulting in asymmetric inlet blood flow at 6.5 ml/s and 2.2 ml/s on the right and the left carotid arteries, respectively. It is evident that the right anterior circulation compensates the reduced blood flow in the stenotic left ICA, through increased flow in right ICA and the right-to-left flow via the anterior communicating artery.
The computation of the pulsatile pressure with the high temporal resolution at a sampling rate of 100 Hz provides instantaneous information of cerebral hemodynamics. We can then derive the hemodynamic parameters,
Relation of FF, FPR, and FFR and their clinical implications
Liebeskind and Feldmann first proposed the concept of FF, adapted from the coronary circulation, to indicate the hemodynamic significance of cerebral artery stenosis. 11 It can be interpreted as a parameter without considering the potential blood flow reserve. In this study, we however used FPR which is equal to FFR if the blood flow reserve is taken into account. According to the assumptions of FFR,1,2 we deduced simplified mathematical relations in Supplementary information (available online). It turns out that FF ≥ FPR ≥ FFR without hyperemia induced and FF = FPR = FFR with distal artery maximally dilated, suggesting that FPR is a closer parameter to FFR than FF, though they both converge to FFR when the resistance of the distal artery is reduced to minimum.
Indeed, in this study, both the computational method and the interventional method suggested that the FPR is a functional parameter of cerebral hemodynamic, which is different from the severity of stenosis. In Figure 3(c), the values of FPR from the patients with severe stenosis (>70% luminal stenosis) were scattered transversely, implying that the patients even with high degree of stenosis could have blood pressure preserved sufficiently. This agrees with the findings in the study of FFR in coronary artery diseases (CAD). 1 However, FPR is not equal to FFR unless the distal arteries are maximally dilated. Although hyperemic stimulus is required for FFR in CAD, the potential risks in cerebrovascular diseases have not been sufficiently assessed and it is therefore of great concern. We thus suggest that FPR is used as a functional parameter that shows hemodynamic alteration without considering the potential reserve of the blood flow, and further speculate that FPR might be a good approximation of FFR in patients with symptomatic intracranial artery stenosis as blood flow reserve is likely consumed in this condition. Indirect evidence may be found in autoregulation, as previous study showed significant impairment of cerebral autoregulation in patients with stenosis, suggesting significant dilation of the resistance vessels.26,27
Limitations
Despite the excellent agreement of our computational results and the clinic measurements, we recognize the following limitations in this study. (1) Possible changes of downstream vessel resistance were not considered. There was thus no effect of cerebral autoregulation simulated when stenosis presented. (2) Only limited collateral information was provided by the CTA source images. This might explain the relatively large difference between the invasive and non-invasive measurements in the cases (case 8 and 9 in Table 1) with stenosis in the middle cerebral artery where the downstream flow can be supplied by pial collaterals which are not considered in the proposed CFD model. We note that some recent studies applied the phase-contrast MRI based imaging techniques to measure intracranial hemodynamic information with good temporal resolution.20,28 These techniques need to be considered in the future CFD simulation.
Conclusions
In this paper, we introduce a parameter, the fractional pressure ratio, which can be obtained invasively or non-invasively and we show that the parameter reflects the hemodynamic significance of the stenosis. A CFD-based method is proposed to compute FPR, and the value of the computed FPRCFD is close to the value obtained with the invasive measurement. This CFD-based method is therefore being potentially useful in the non-invasive assessment of the functional alteration caused by cerebral luminal stenosis. The numerical simulation also helps in elucidating that the pressure ratio is more closely related to the hemodynamics than the percentage of stenosis. Further refinement of the CFD-based method, together with clinical studies of the functional assessment of stenosis, is necessary in order to achieve more accurate estimate under more general situations and for the technique to become clinically practical.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Natural Science Foundation of China (grant nos 81471207 and 81501004); and the Shenzhen Science and Technology Innovation Council (grant nos KQCX2015033117354152 and JSGG20150602143414338).
Declaration of conflicting interests
The author(s) declare that there is no conflict of interest with respect to the research, authorship, and/or publication of this paper.
Authors’ contributions
JL and XCC proposed and designed the CFD model for this study. LL designed the clinical experiment. JL, XCC and LL wrote the manuscript. ZY and WSS implemented the CFD method. YP and XLi collected the CTA images. JW and RC reconstructed the 3D artery from the CTA images and transferred the 3D artery into meshes. XLe and HQ performed the statistical analysis. BJ, LS, YW (for Yilong Wang), ZM, and YW designed and implemented the interventional measurement.