
Abstract
New oral anticoagulants for the prevention of stroke and systemic embolism in patients with atrial fibrillation have recently been introduced. In this translational study, we explored the risk of long-term anticoagulation on intracerebral hemorrhage under sustained severe arterial hypertension. We initiated anticoagulation with warfarin or apixaban in spontaneously hypertensive rats prone to develop severe hypertension and subsequent intracerebral bleeding complications. A non-anticoagulated group served as control. During an 11-week-study period, blood pressure, anticoagulation parameters, and clinical status were determined regularly. The incidence of histopathologically proven intracerebral hemorrhage was defined as the primary endpoint. Both warfarin and apixaban anticoagulation was fairly stable during the study period, and all rats developed severe hypertension. Intracerebral hemorrhage was determined in 29% (4/14) of warfarin rats and in 10% (1/10) of apixaban rats. Controls did not show cerebral bleeding complications (chi-square not significant). Mortality rate at study termination was 33% (2/6) in controls, 43% (6/14) in the warfarin group, and 60% (6/10) in the apixaban group. Animals died from extracerebral complications in most cases. Our study describes an experimental intracerebral hemorrhage model in the context of sustained hypertension and long-term anticoagulation. Extracerebral bleeding complications occurred more often in warfarin-treated animals compared with apixaban and control rats.
Introduction
Long-term anticoagulation with either vitamin K antagonists or the new oral anticoagulants (NOAC) directly inhibiting thrombin (FII) or activated factor X (FXa) is highly effective in preventing ischemic stroke and systemic embolism in patients with atrial fibrillation. 1 Whereas vitamin K antagonists reveal a substantial risk for intracerebral hemorrhage (ICH; 0.5–1% per year), this most feared complication occurs less often in patients treated with direct thrombin inhibitors or direct factor Xa inhibitors.2–4
Outside the well-controlled clinical trials, many uncertainties regarding the application of the new anticoagulants remain.5,6 A particular concern is whether long-term anticoagulation is safe in patients with arterial hypertension and cerebral small vessel disease. 7 These are frequent comorbidities of elderly individuals with atrial fibrillation. Indeed, analyses point toward an increased risk of ICH in patients anticoagulated with warfarin who have significant cerebral white matter lesions or cerebral microbleeds on magnetic resonance imaging (MRI).7,8 On the other hand, withholding anticoagulation to those patients can hardly been justified in view of its outstanding effectiveness and the high risk of stroke especially in this patient cohort. 9
This translational study compared the effects of long-term anticoagulation with the vitamin K antagonist warfarin and the direct factor Xa inhibitor apixaban on cerebral and extracerebral bleeding complications, mortality, and functional outcome in stroke-prone spontaneously hypertensive rats.10–12
Material and methods
Animals
All experimental procedures were conducted in accordance with the National Institute of Health’s guide for the care and use of laboratory animals. The report of the data in this manuscript is compliant with the ARRIVE (animal research: reporting in vivo experiments) guidelines. 13 The study was approved from the responsible regulatory authorities in Germany (Regierungspräsidium Darmstadt). Male stroke-prone spontaneously hypertensive rats (spSHR; Charles River Laboratories, USA) were used throughout the entire study. This strain serves as a well-established model for malignant arterial hypertension and its cerebral and extracerebral complications. 11 Ischemic strokes and cerebral microbleeds typically occur within 6 to 10 weeks after the beginning of a salt enriched diet.10,12 The rats were delivered to our laboratory at the age of 6 weeks and were caged for an acclimatization period of 1 week (the 7th week of life).
Study planning and sample size calculation
Previous studies in spSHR have shown a high incidence of ICH (70–100%) and a short life span of <20 weeks.10,12 ICH is often multifocal with on average three bleeds per brain. 12 We assumed a detrimental effect of oral anticoagulation on hematoma expansion in severely hypertensive animals. The use of apixaban halved the incidence of ICH in the phase III ARISTOTLE trial of stroke prevention in patients with atrial fibrillation. 3 We have previously shown in the collagenase injection model that hematoma expansion in mice pretreated with warfarin is threefold higher than after pretreatment with the direct thrombin inhibitor dabigatran. 14 Based on the effect size of our previous studies (Cohens D = 1.35),14,15 we needed at least 8 rats per group to detect a significant difference in hematoma volume between the different oral anticoagulation treatment regimens with a power of 80% and a type 1 error of 0.05 with a one-tailed Student's t-test, and 10 rats per group for a two-tailed test. Thus, we randomized 10 rats per group (control, warfarin, apixaban).
Anticoagulation and feeding
From the beginning of their 8th week of life, all rats had free access to salt-enriched pellets (4% saline; SSNIFF Spezialdiäten GmbH, Germany) 12 and free access to salt-enriched drinking water (1% saline). At the same time point, anticoagulant treatment was started in the salt-enriched drinking water in the respective groups. For the warfarin group, a 5 mg coumadin tablet (warfarin sodium; Bristol-Myers Squibb GmbH & Co) was pestled, diluted in 1 l tap water and stirred with 500 rpm for 1 min. This stock solution was then diluted again to the intended concentration according to the current international normalized ratio (INR) values. For the apixaban group, six 5 mg Eliquis tablets (Bristol-Myers Squibb GmbH & Co) were pestled and mixed with 3.6 ml dimethylsulfoxide (DMSO; Sigma-Aldrich Chemie GmbH, Germany). After 1 min, this solution was diluted with tap water to a total volume of 360 ml and stirred with 500 rpm for 2 min. DMSO was required as a co-solvent to achieve the desired apixaban concentrations. To balance for this co-solvent, control- and warfarin-treated animals also received 1% DMSO with their drinking water. The dosing-regimes for warfarin and apixaban anticoagulation in rodents were adapted from previous translational studies of our group.14,16 They were further refined in a pilot trial including eight additional spontaneously hypertensive rats. Here, increasing doses of warfarin and apixaban were tested to achieve stable anticoagulation over time, comparable with the therapeutic range used in humans (target range for warfarin: INR 2 to 3.5; target range for apixaban: anti-Xa-level 1 to 3 IU/ml; 17 see supplemental Figure 1(a) and (b)).
Despite these initial dose-finding procedures, we experienced massive overdosing of warfarin with high attributable mortality in the first week of anticoagulation in our main study. After five animals in the warfarin group had died due to extracerebral hemorrhage as verified by complete autopsy, we decided to cross over four randomly selected rats from the control group to the warfarin group. Following this, group sizes were 6 in the control group, 14 in the warfarin group and still 10 in the apixaban group. Since the cross-over happened in the 8th week of life (the first week of anticoagulation) and ICH typically occurs at later stages of the experiment,10,12 we assumed that this cross-over would not have a relevant impact on the findings of the study.
From the 8th week of life onward, a blood sample of 310 µl was taken once a week from all rats by puncturing the retrobulbar plexus. Blood was mixed with 40 µl citrate, leading to a 1:9 dilution. Both INR values and low molecular weight heparin-calibrated anti-Xa-level were determined (ACL Top II, Instrumentation Laboratory). Based on the results of the coagulation analysis, doses of warfarin and apixaban were carefully adjusted, respectively.
Arterial hypertension and hypertension-induced end organ damage
Systolic and diastolic blood pressure was measured once a week non-invasively in all rats by an automated system based on the tail-cuff-method (BP 2000, blood pressure system for rats, Biomedical Instruments, Zöllnitz). This method has previously been validated in spontaneously hypertensive rats. 18 Rats were placed in a restrainer on a heating plate with a temperature of 36℃. A cuff was attached to the tail and gently tightened until detection of the pulse signal was possible. For the next 10 min, the animals had time to acclimatize on the plate. The blood pressure system performed 10 pre-measurements during this time period that were discarded. The next 10 measurements were used to generate a mean value for systolic and diastolic blood pressure.
To confirm the occurrence of hypertension-induced end organ damage, we randomly selected four rats for post-mortem kidney evaluation. Kidneys were cut longitudinally followed by fixation in 4% PFA for 3 days prior to paraffin embedding. Sections of 3 µm were prepared and stained with hematoxylin-eosin (HE) and Van Gieson. The slices were assessed from a blinded evaluator (PP). The glomerular changes were rated by a glomerular damage index (GDI) described elsewhere in detail. 19 Sections also underwent periodic acid-Schiff reaction staining as well as specific proximal tubular staining using anti-CD13 (rat anti-mouse; AbD Serotec, Germany) immunostaining to detect necrotic changes of the proximal tubules as described previously.20,21
ICH
The incidence of ICH at the end of the study period (in the 17th week of life, i.e. 10 weeks after the induction of malignant hypertension by the salt-enriched diet10,12) was predefined as the primary endpoint of the study. If animals died earlier of whatever reason, or if animals had to be euthanized because a pre-defined safety endpoint was reached, the time point of death was considered to be the end of the individual study period. These animals were also included in the primary endpoint analysis.
At study termination, animals were deeply anesthetized (ketamine (100 mg/kg body weight), xylazine (1 mg/kg body weight)) and then perfused with 4% paraformaldehyde (PFA). Animals found dead during the study period were not perfused. Brains were then carefully removed and immersed in 4% formalin. Later on, brains were cut in slices of 1-mm thickness. The rhinencephalon and the cerebellum were discarded. Fixation was conducted in 4% PFA for 1 day prior to paraffin embedding. Sections of 3 µm were prepared (Mikrotom CM 1900, Leica Microsystems Nussloch GmbH, Nussloch) and placed on slides (SuperFrost Plus, Thermo Scientific, Dreieich). Afterward, the slices were kept for 30 min at 40℃ on a heating platform (HI1220, Leica Microsystems Nussloch GmbH, Nussloch) and incubated at 37℃ (Heraeus, Thermo Scientific, Dreieich). Finally, the slices were stained with HE and assessed from a blinded evaluator (PZ, MM).
The occurrence of ICH was recorded, including information on location, size, and structure. The size was measured using Olympus Imaging Analysis software in one representative image section. ICH was considered as fresh (<24 h) if erythrocytes stained bright red in HE staining and no signs of erythrophagocytosis were present. Subacute hemorrhages were assumed if erythrocytes appeared pale in HE staining and signs of erythrophagocytosis were visible. Ischemic infarcts were characterized by the presence of neuronal microvacuoles, eosinophilic cytoplasm with pyknotic nuclei (indicative of apoptosis), and leukocyte infiltration into the ischemic area. Infiltration of blood-derived macrophages characterized a subacute stroke lesion. 22 Furthermore, in every rat, we performed a detailed post-mortal autopsy to detect bleeding complications throughout the body.
Body weight and functional outcome
All weighting and behavioral testing was performed from a blinded evaluator (FB). Body weight was measured once a week in all animals using a standard scale.
From the 8th week of life onward, the modified Bederson Score was determined (once a day between the 8th and 12th week of life and twice a day between the 13th and 17th week of life). 23 In the 8th week of life as well as in the 12th and 17th week of life, a cylinder test, an open field test and an adhesive removal test were performed. 23 In the cylinder test (cylinder height: 250 mm, internal diameter: 172 mm), the animals were videotaped for 80 s, and both the relative activity and the asymmetry index of the use of the front paws were observed. 24 In the open field test, the animals were videotaped for 80 s while exploring a new cage (length: 56 cm, wide: 38 cm, height: 21 cm), and migration distance and relative migration time were determined. In the adhesive removal test, the rats had to remove a sticker from each of their front paws. Three trials were performed, and the mean time to removal of both stickers was documented.
Evaluation of non-lethal extracerebral bleeding complications
At all time-points, the behavior and shape of the animals were carefully observed and any clinical signs of bleeding (such as epistaxis, dark feces, hematuria, hematoma formation, wound bleeding, bleeding after puncture of the retrobulbar plexus) were recorded. From the 8th week of life onward, a hemoccult test (modified Guajak-Test of Greegor; Beckman Coulter) was performed every week in three randomly selected animals per group to screen for occult blood in the feces. Hemoccult testing was also performed whenever suspiciously dark looking feces were observed.
Statistical analysis
Data are given as mean ± SD. Parametric data were compared between groups using univariate ANOVA. Non-parametric (binary) data were compared using the Chi-square test (including post-hoc testing). A significance level of alpha = 0.05 was chosen for all tests. Statistical evaluation was performed using SPSS Version 21 (Statistical Package for the Social Sciences, Armonk, NY, USA).
Results
Oral anticoagulation
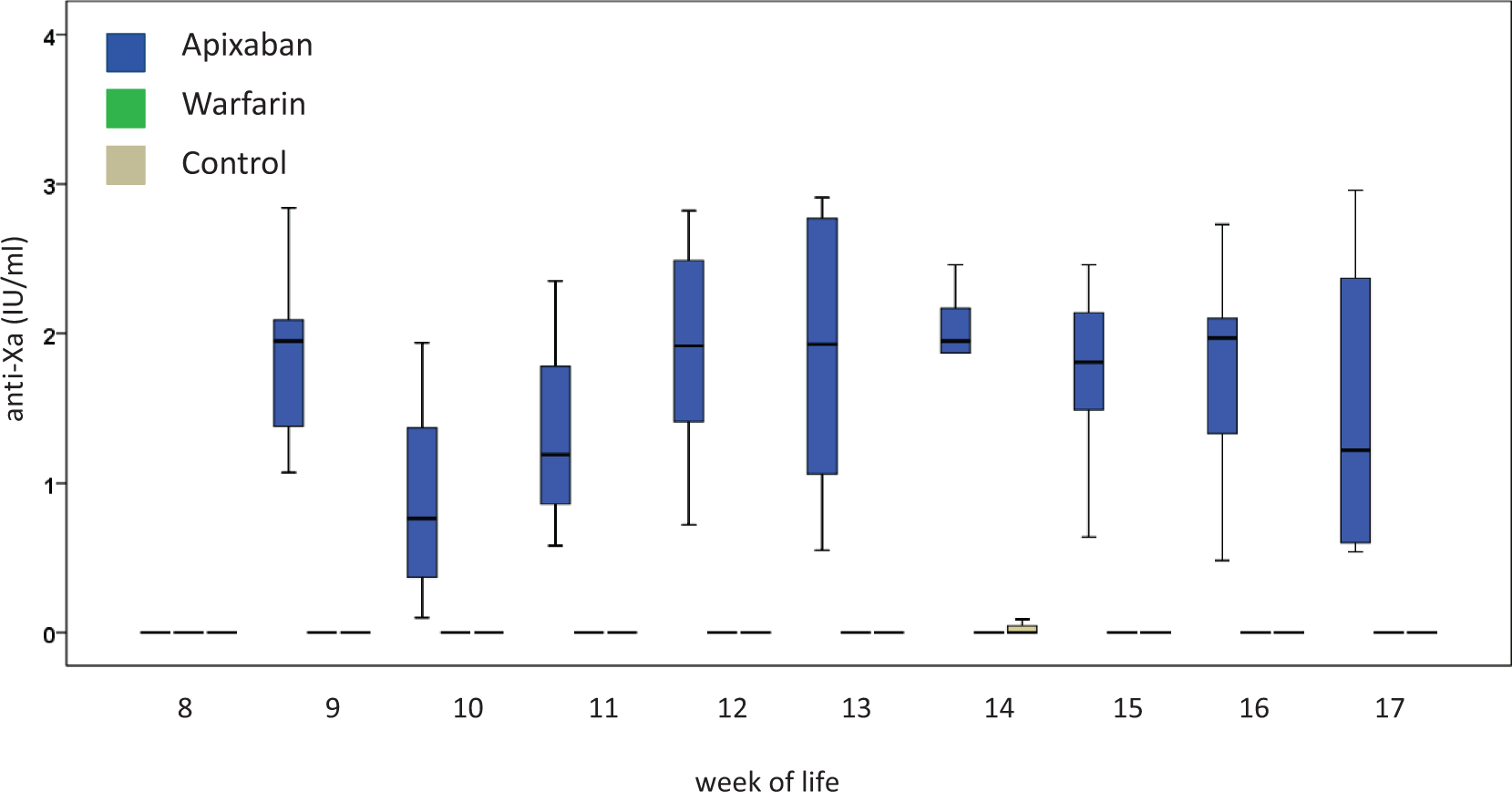
In the control group, INR values remained around 1.0 throughout the entire study period, and anti-factor Xa levels were found below the detection threshold at all time-points. In the warfarin group, mean INR values ranged from minimum values of 1.6 ± 0.6 (16th week of life) to maximum values of 6.6 ± 3.3 (17th week of life), while there was no measurable anti-factor Xa activity. In the apixaban group, mean anti-factor Xa levels ranged from minimum values of 1.0 ± 1.4 IU/ml (10th week of life) to maximum values of 1.9 ± 0.8 (12th week of life), and INR values were found marginally increased in a few animals only (see Figures 1 and 2). Despite a careful dose-finding pilot trial, we faced massive warfarin overdosing leading to the death of five rats of the warfarin group due to extracerebral bleeding complications in the first week of anticoagulation. As detailed above, four randomly selected rats from the control group crossed over to the warfarin group in the 8th week of life.
International normalized ratio (INR) values over time as determined in rats anticoagulated with apixaban (blue) or warfarin (green) as well as in control animals (beige). Distribution of INR values is presented by means of boxplots. The box demonstrates the 25th, 50th (median), and 75th percentile, and the whiskers the 10th and 90th percentile, respectively. In the apixaban group and in the control group, INR values remained close to 1 at almost all time points. Anticoagulation was initiated during the 8th week of life. Anti-factor Xa levels (IU/ml) over time as determined in rats anticoagulated with apixaban (blue) or warfarin (green) as well as in control animals (beige). In the warfarin group and in the control group, anti-factor Xa levels remained close to 0 at almost all time points. Anticoagulation was initiated during the 8th week of life.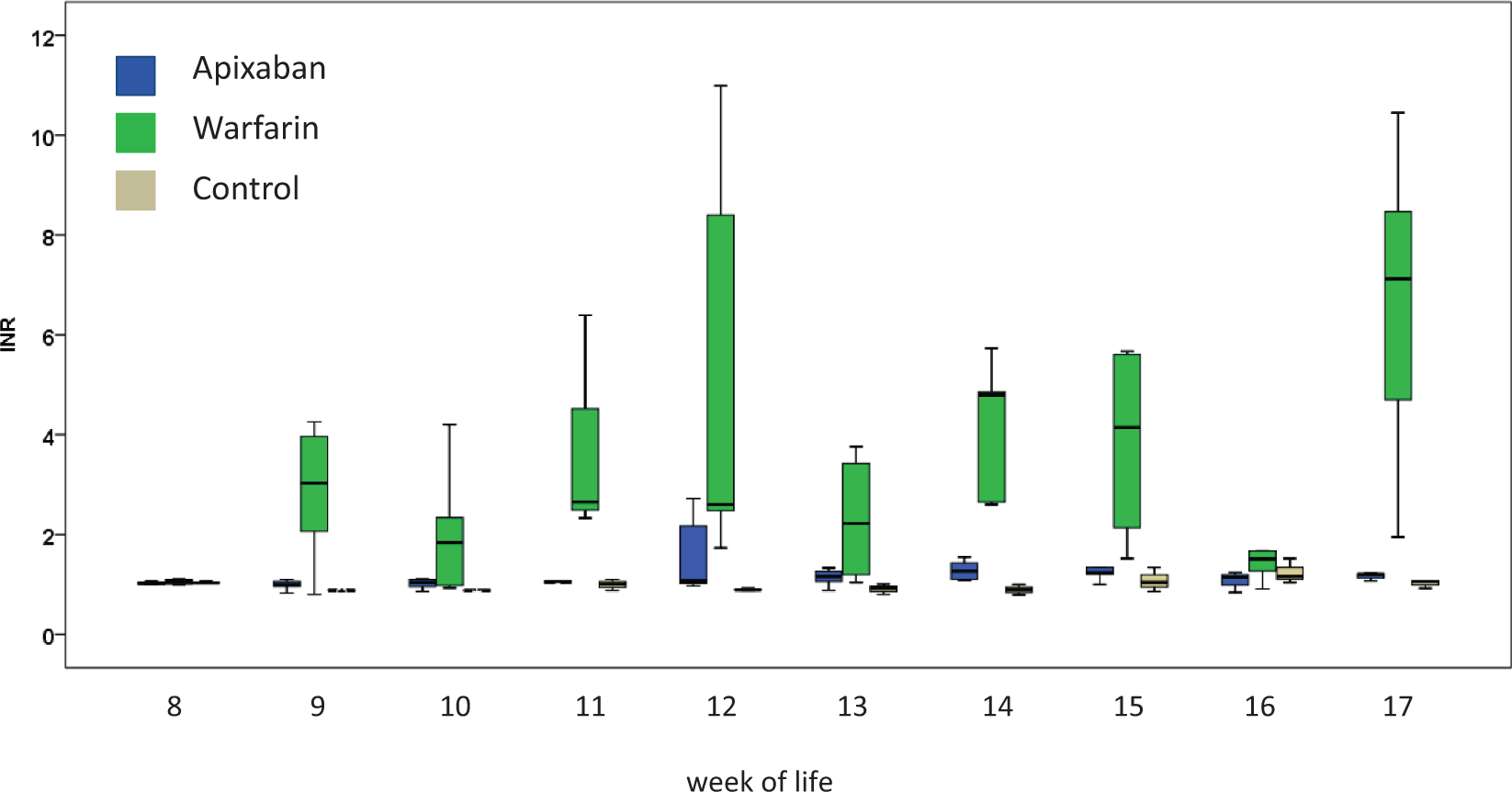
Sustained arterial hypertension
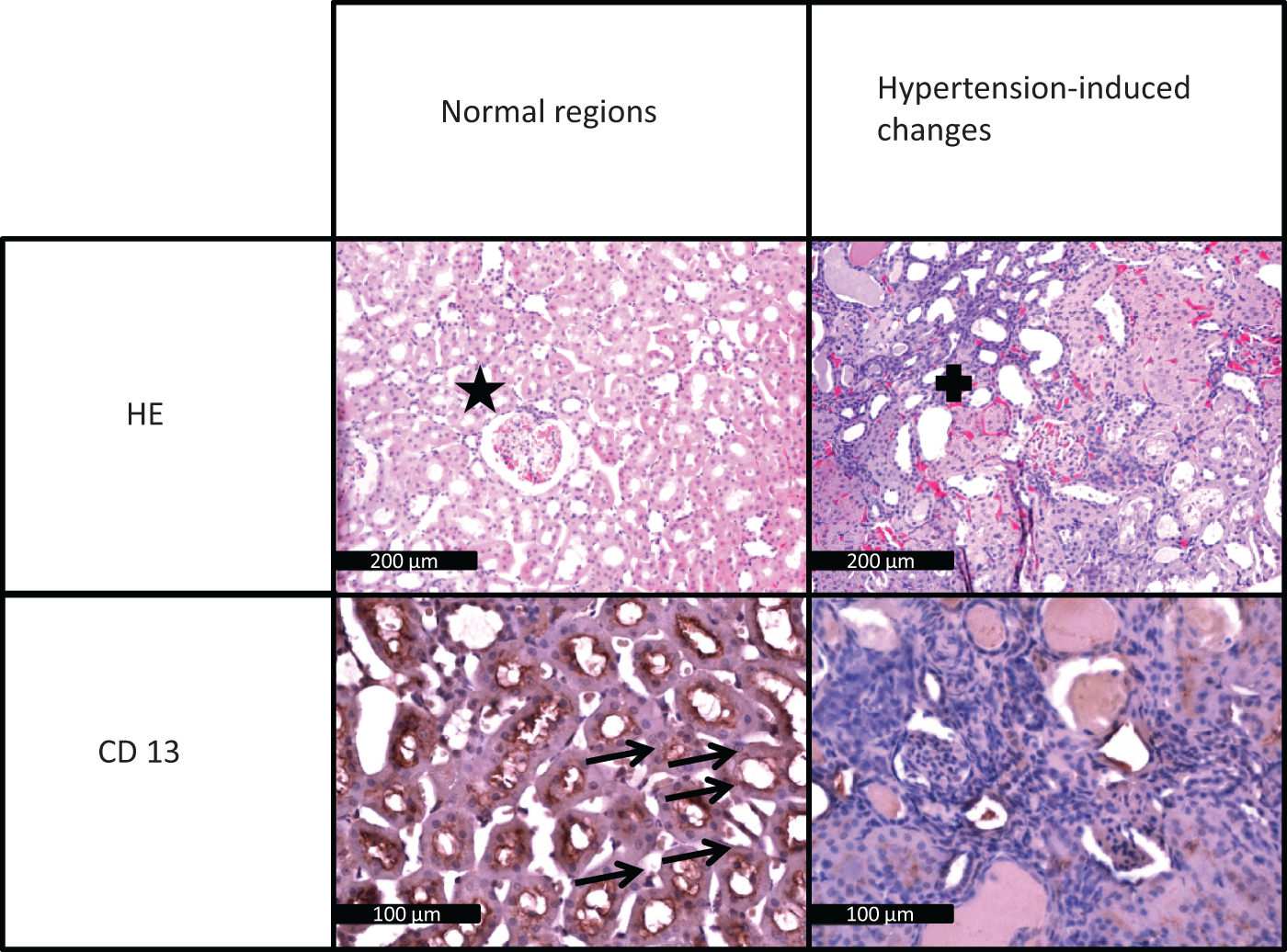
Mean systolic blood pressure in the three groups increased from approx. 150 mmHg (8th week of life) to a maximum of approx. 200 mmHg (13th week of life) and decreased slightly afterward (see Figure 3). Diastolic blood pressure increased in a comparable way (see supplemental Figure 2). There was no difference in blood pressure development between the three groups. Histopathological evaluation of the four randomly selected kidneys confirmed hypertension-induced end organ damage in all investigated animals. Two rats showed severe glomerular damage (fibrinoid necrosis of the arteriolar wall and hemorrhagic necrosis of the glomerular tuft), and two had moderate glomerular damage (medial thickening, narrowed capillary lumina and media necrosis of afferent arterioles). Mean glomerular damage index of the four kidneys was 76. The analysis of the CD13- and PAS-staining also confirmed tubular damage. One animal showed severe tubular changes, one displayed moderate changes and two had mild changes (see Figure 4).
Mean systolic blood pressure over time as determined in rats anticoagulated with apixaban (blue) or warfarin (green) as well as in control animals (beige). First measurements were performed in the 7th week of life. Salt-enriched diet to induce malignant arterial hypertension was applied in the 8th week of life. Blood pressure increased in all three groups simultaneously. Histopathological evaluation of the selected kidneys (HE-staining (upper part) and CD 13-staining (lower part)). The panels on the right side show hypertension-induced damage, the panels on the left side show normal regions for comparison. The star marks a normal-appearing glomerulus (HE-staining), the cross indicates a destroyed glomerulus. Arrows point to intact proximal tubules (CD 13-staining). Following sustained hypertension, CD 13-staining intensity is reduced, indicating structural damage to the tubules (bottom right panel). The black bar represents 200 µm in the HE-staining and 100 µm in the CD 13-staining.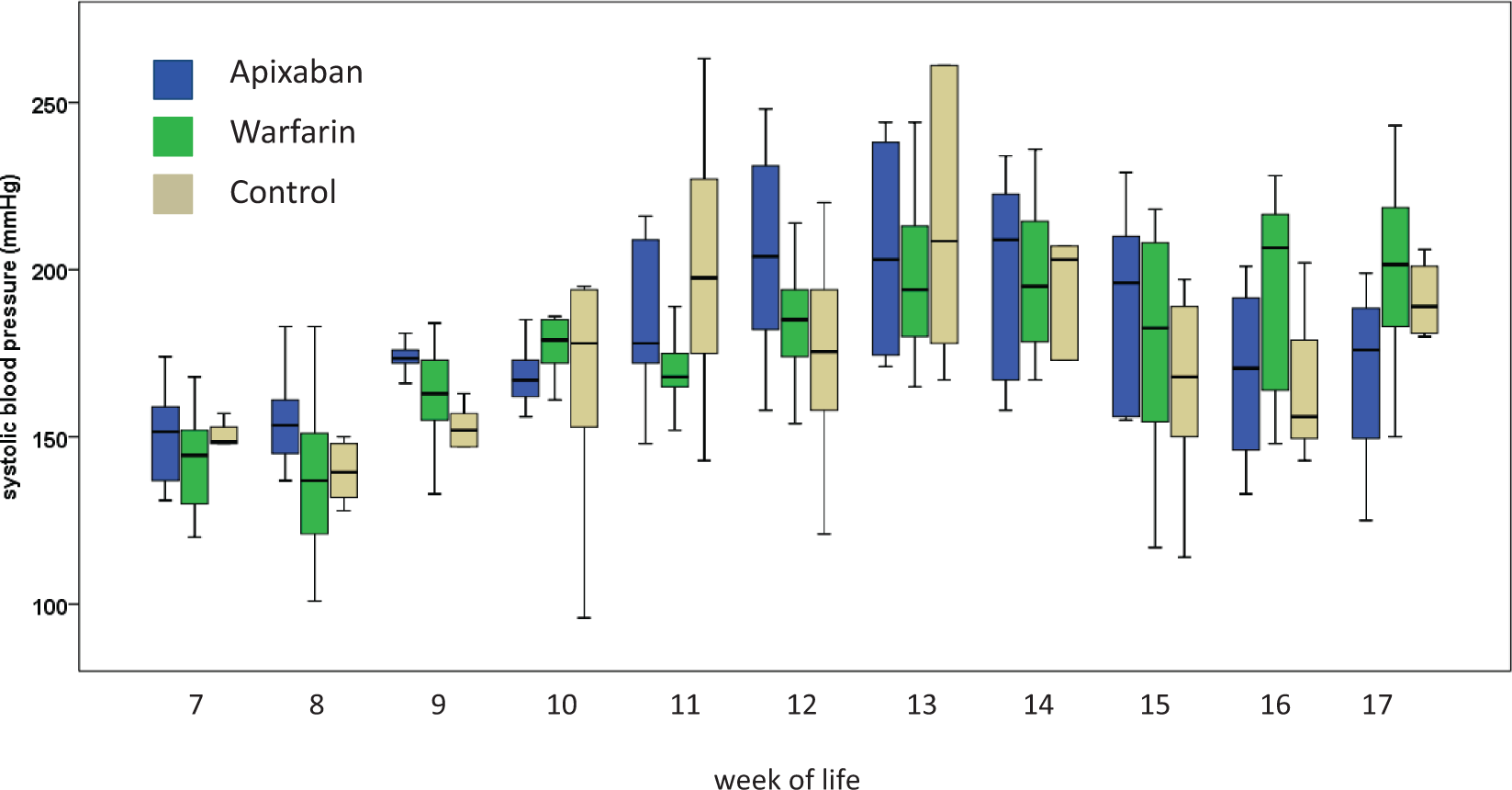
Incidence and characteristics of ICH
Histological analysis at the end of the study period revealed that 29% (4/14) of the warfarin rats showed intracerebral bleedings, in contrast to 10% (1/10) of the apixaban rats. ICH was not apparent in the control group (chi-square for between group differences not significant). Hemorrhages had areas between 0.08 and 1.6 mm2. The bleedings occurred in the majority in the thalamus. In addition, one warfarin animal showed an ischemic infarction with an area of 7.8 mm2, whereas all other animals did not show signs of ischemic strokes (see Figure 5 and supplemental Table 1). Other intracranial bleeding complications (such as subarachnoid hemorrhage) were not apparent.
(a–d) Representative examples of intracerebral hemorrhages that were detected during histopathological evaluation of the rat brains (HE staining); (a) fresh intracerebral hemorrhage (estimated onset < 24 h), original magnification: 20×, warfarin group (No. 8); (b) fresh intracerebral hemorrhage (estimated onset < 24 h), original magnification: 40×, apixaban group (No. 20), (c) intracerebral hemorrhage, red blood cells pale, invasion of white blood cells, no erythrophages (estimated onset 12–24 h), original magnification 100×, warfarin group (No. 7), (d) little spot of red blood cell extravasate (approximately 60 µm in diameter) (estimated onset < 24 h), original magnification: 200×, warfarin group (No. 19)). (a′) displays a macroscopic view on the brain with the intracerebral hemorrhage shown in (a). The hemorrhage can be seen as a bluish parietal spot.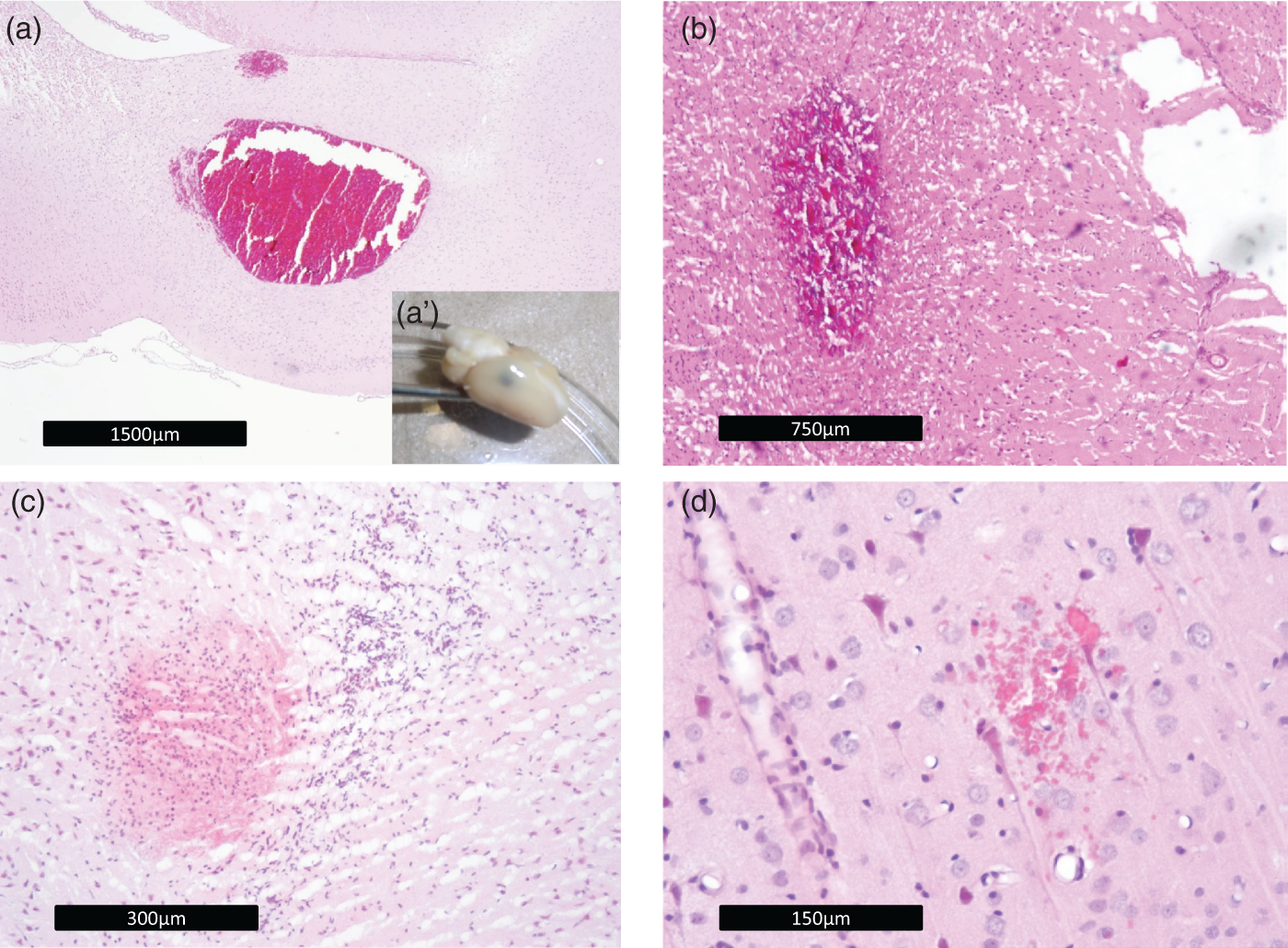
Survival
Mortality rate at study termination (17th week of life) was 33% (2/6) in the control group, 43% (6/14) in the warfarin group, and 60% (6/10) in the apixaban group (see Figure 6 for Kaplan–Meier curves). Warfarin rats died primarily in the first two experimental weeks, in the majority due to extracerebral bleeding complications. This happened although a careful dose adjustment was performed in the pilot experiments (see methods and supplemental Figure 1(a) and (b)). In contrast, the apixaban and control animals died predominantly in the last 3 weeks of the study period, in the majority also due to extracerebral complications (see supplemental Table 2).
Kaplan–Meier curves displaying cumulative survival rates of rats anticoagulated with apixaban (blue) or warfarin (green) as well as in control animals (beige).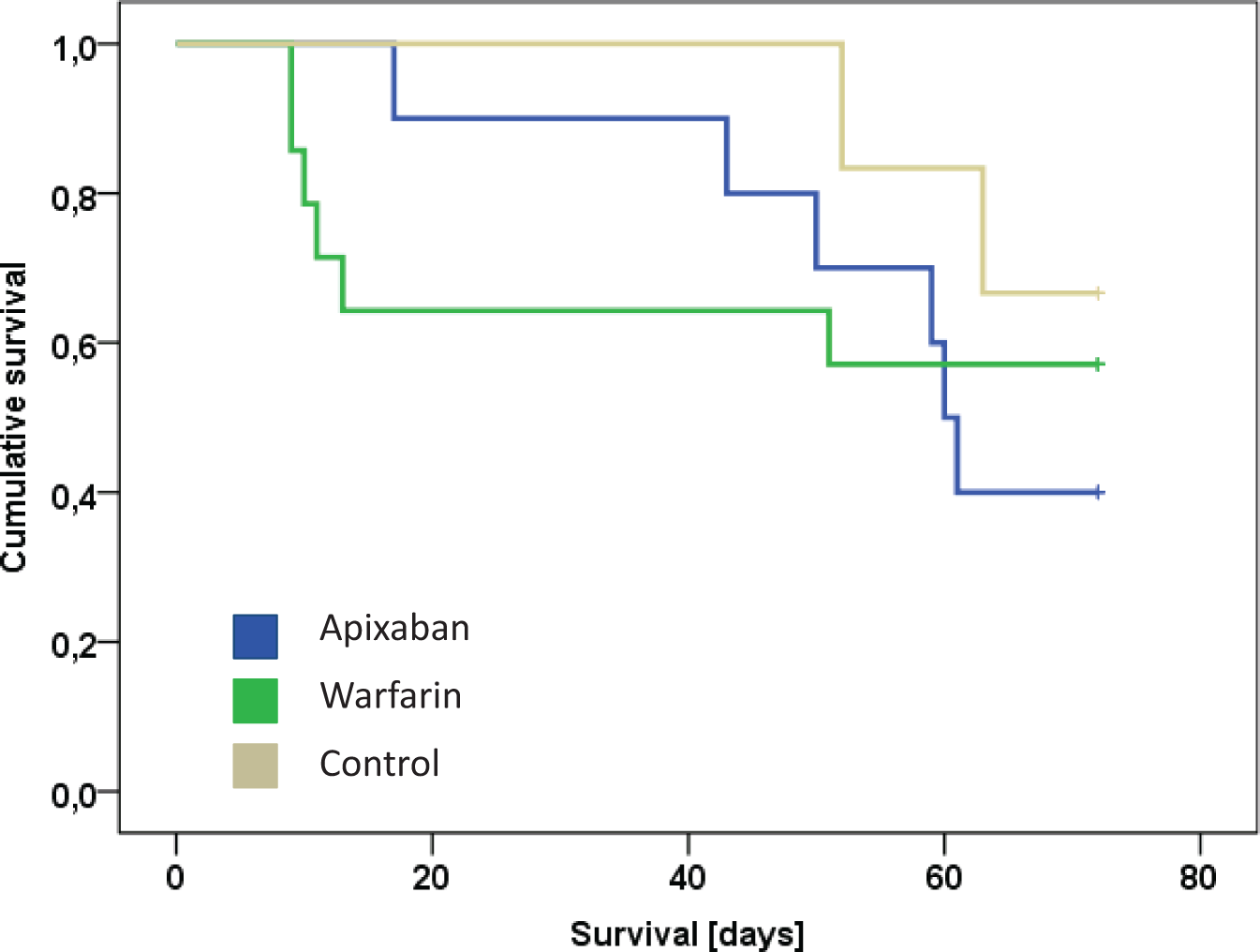
Functional outcome
Mean body weight in the 7th week of life in the three groups was 117 ± 12 g. It increased to a mean of 274 ± 18 g in the 17th week of life without any difference between groups (see Figure 7). In the warfarin group, three animals developed motor deficits as measured by the Bederson score in the first week of anticoagulation. Beginning in the 12th week of life, one warfarin rat, five apixaban rats, and two control rats revealed abnormalities (>0) in Bederson scoring. There was no significant difference between treatment arms. Furthermore, we did not obtain significant differences in functional outcome assessment between the groups (i.e. cylinder test, open field test, adhesive removal test; see supplemental Figure 3(a)–(e)).
Mean body weight (g) over time as determined in rats anticoagulated with apixaban (blue) or warfarin (green) as well as in control animals (beige). First measurements were performed in the 7th week of life. Salt-enriched diet to induce malignant arterial hypertension was applied in the 8th week of life. Body weight increased in all three groups simultaneously. Variance increased between week 13 and 15, as some rats developed neurological symptoms. The second increase at the end of the study period results from a positive selection effect.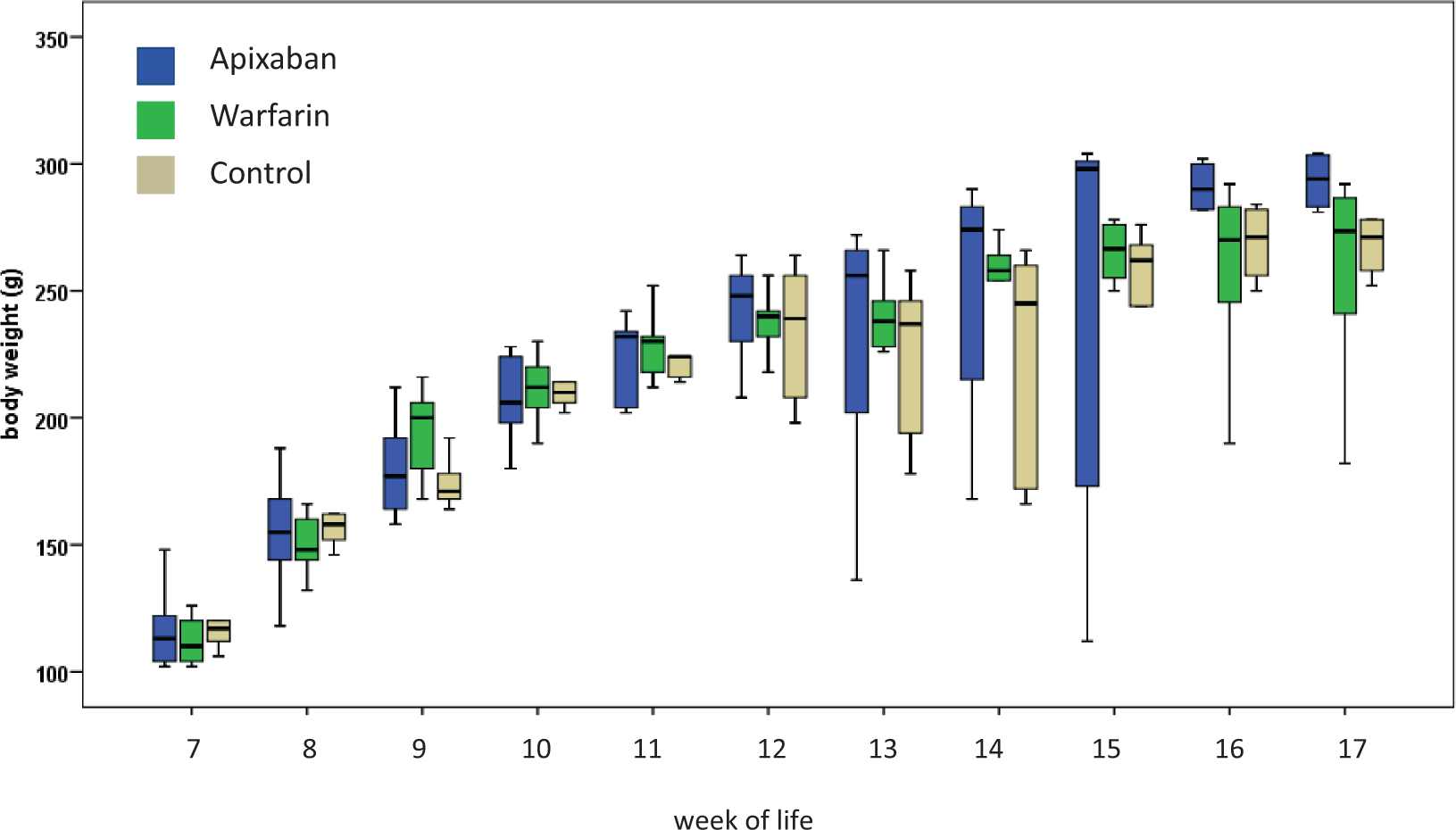
Non-lethal extracerebral bleeding complications
During the study period, we recorded 33 non-lethal extracerebral bleeding events. Hereof, 70% occurred in the warfarin group, 24% in the apixaban group, and 6% in the control group (chi-square p < 0.001; post-hoc warfarin vs. apixaban p < 0.001, warfarin vs. control p < 0.001, apixaban vs. control p = 0.041). We obtained 11 positive hemoccult tests, 8 of those occurred in the warfarin group, 2 in the apixaban group, and 1 in the control group (chi-square p = 0.003; post-hoc warfarin vs. apixaban p = 0.015, warfarin vs. control p = 0.004, apixaban vs. control p = 0.500).
Discussion
This is the first translational study that investigated the effects of long-term anticoagulation on the risk of ICH during sustained malignant hypertension. Mouse models of short-term anticoagulation (1–3 days) with both warfarin and new oral anticoagulants have recently been developed.14,16,25 Here, anticoagulated rodents were subjected to undergo the well-established collagenase model of ICH. These studies have provided interesting insights into the pathophysiology of ICH expansion under warfarin and the new oral anticoagulants.14,16,25
The present study improves and refines these models, (I) by using animals prone to develop brain hemorrhages, thereby avoiding the artificial induction of ICH by the stereotactic application of collagenase, and (II) by establishing a method of long-term anticoagulation in rodents.14,16 According to our protocol, it is now possible to keep animals under “therapeutic” anticoagulation both with warfarin and apixaban for several weeks. Similar to what is observed in humans, INR values revealed certain undulations in our study, likely due to inter-individual variations in water consumption or vitamin K metabolism. Despite a careful adjustment of warfarin dosage in the pilot trial, five rats in the warfarin group died during the first days of the study. This was due to extracerebral bleeding complications that in all likelihood occurred in the context of increased INR values. In contrast, in the apixaban group, anti-factor Xa levels varied to a much lesser extent, and extracerebral bleeding complications were observed less frequently than in the warfarin group. This reflects the known risk of warfarin anticoagulations in our model, and points toward a relative safety of new oral anticoagulations compared with warfarin with regard to dosing issues. 26
Regarding the primary endpoint, we observed relatively few intracerebral bleeding complications, even though all of our animals developed sustained severe arterial hypertension. Indeed, a careful histopathological analysis of kidneys of randomly selected rats revealed moderate to severe hypertensive damage of the glomeruli in all cases, which proves that hypertension has provoked end organ damage. Other groups reported kidney damage to precede cerebral injury in spSHR. 27 In our study, however, severe hypertension and end organ damage did not translate into the development of severe intracerebral bleeding complications on a regular basis, as it is in case of anticoagulated animals subjected to a territorial infarction, e.g. by means of middle cerebral artery occlusion.28,29 Both large parenchymal bleedings and extensive hemorrhagic transformation were not observed in our animals. Rather, a hypertension-induced index event (i.e. a vessel rupture by chance) seems to be a pre-requisite for the bleedings to develop. Even though the animals were anticoagulated, the bleedings did not tend to expand toward large hemispheric bleedings, although this can be observed in case of collagenase-induced ICH occurring under short-term anticoagulation.14,16
On the other hand, all bleeding events occurred in anticoagulated rats, and three out of four took place in the warfarin group. Together with the findings that warfarin animals revealed severe complications in the initial phase and more frequently showed signs of non-lethal extracerebral bleedings (i.e. positive hemoccult testing) as compared with apixaban and control rats, we consider our study to appropriately mirror many of the difficulties associated with warfarin intake in humans. It provides a signal that, under severe hypertension, apixaban anticoagulation leads to less bleeding complications as compared with warfarin.
Regarding functional outcome, we did not obtain significant differences between groups. It is not surprising that the rather small bleedings did not immediately translate into a relevant functional deficit, in contrast to larger and expanding bleedings in the collagenase ICH model.14,16 Furthermore, during the final weeks of the experiment, animals also developed symptoms resulting from extracerebral disorders (e.g. kidney dysfunction). This fact interfered with an unbiased comparison of neurological deficits resulting from ICH. Our study was not powered to identify differences in functional outcome between groups.
Strengths of our study are the first-ever description of long-term anticoagulation in an experimental model of hypertension-associated ICH. Both maintaining the anticoagulation in the “therapeutic” range and the development of the malignant hypertension with end organ damage worked well. We decided to maintain anticoagulation at the upper limit of the therapeutic range used in humans, to maximize the discriminatory power (i.e. to find differences between warfarin and apixaban) in the study. On the other side, a lower therapeutic range may have prevented mice to die in the first week of warfarin intake. Without doubt, a shortcoming of our study is the fact that fewer primary outcome events (i.e. ICH) occurred than assumed during prospective study planning. A priori sample size calculations were based on studies describing cerebral hemorrhagic events in the majority of rats after 10 weeks of malignant hypertension.10,12 However, this was not observed in our study, either due to a genetic drift in the spSHR strain used or because of lethal extracerebral complications that occurred prior to ICH. Potential neuroprotective effects of the solvent DMSO might be another explanation for the low number of outcome events, 30 and DMSO may also protect from hypertension induced cerebral small vessel damage. Regarding the translational relevance, it has to be mentioned that both similarities and differences exist between human and rodent coagulation systems. 31 Unfortunately, due to its long-term design, important pathophysiological measures could not be determined in this study. In particular, brain water content measurements are frequently performed in the context of experimental ICH. Given that thrombin is an important mediator of edema formation, anticoagulation with warfarin or direct oral anticoagulants could differentially influence edema formation after ICH. In long-term ICH experiments, however, the “starting point” after which brain edema formation is determined (e.g. 72 h after ICH formation) is difficult to define. It has also to be mentioned as a limitation that sham animals were not evaluated in this study, and that effects of aging on outcome testing cannot be ruled out.
In summary, our model constitutes a step forward toward a better adjustment of translational models to the human condition. In the future, other anticoagulants may be tested using this paradigm, and other pathological conditions may be investigated in the context of long-term anticoagulation, e.g. diabetes mellitus. The results of our study point to a relative safety of anticoagulation under severe arterial hypertension in terms of ICH development. ICH seems to occur sporadically rather than on a regular basis in this setting. More extracerebral bleeding complications occurred in the warfarin group as compared with the apixaban rats.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: All study drugs were purchased from the pharmacy of our university hospital. We used departmental research funding to conduct the study.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Christian Foerch and Waltraud Pfeilschifter received research funding from Boehringer Ingelheim to perform experimental and clinical studies on new oral anticoagulants. No funding was received from any company to perform the present study.
Authors' contributions
Waltraud Pfeilschifter: designed the study, supervised the experiments, analyzed the data; Thurid Steinstraesser: performed the animal experiments, performed the histopathological analysis of the kidneys, analyzed the data, wrote the manuscript; Patrick Paulus: performed the histopathological analysis of the kidneys; Pia Susan Zeiner: performed the histopathological analysis of the brains; Ferdinand Bohmann: performed the outcome analysis; Alf Theisen: supervised the blood pressure analysis and anticoagulation of the animals; Edelgard Lindhoff-Last: analyzed and interpreted the coagulation data, wrote respective parts of the manuscript; Cornelia Penski: performed the histopathological analysis of the brains; Marlies Wagner: performed the outcome analysis; Michel Mittelbronn: analyzed and interpreted the histopathological analysis of the brains, wrote respective parts of the manuscript; Christian Foerch: designed the study, analyzed the data, wrote the manuscript.