
Abstract
Cerebral small vessel diseases of the brain are a major determinant of cognitive impairment in the elderly. In small vessel diseases, the most easily identifiable lesions, both at post-mortem evaluation and magnetic resonance imaging, lie in subcortical areas. However, recent results obtained post-mortem, particularly in severe cases, have highlighted the burden of cortex lesions such as microinfarcts and diffuse neuronal loss. The recent development of image post-processing methods allows now assessing in vivo multiple aspects of the cerebral cortex. This systematic review aimed to analyze in vivo magnetic resonance imaging studies evaluating cortex alterations at different stages of small vessel diseases. Studies assessing the relationships between small vessel disease magnetic resonance imaging markers obtained at the subcortical level and cortex estimates were reviewed both in community-dwelling elderly and in patients with symptomatic small vessel diseases. Thereafter, studies analyzing cortex estimates in small vessel disease patients compared with healthy subjects were evaluated. The results support that important cortex alterations develop along the course of small vessel diseases independently of concomitant neurodegenerative processes. Easy detection and quantification of cortex changes in small vessel diseases as well as understanding their underlying mechanisms are challenging tasks for better understanding cognitive decline in small vessel diseases.
Keywords
Introduction
Age- and hypertension-related cerebral small vessel diseases (SVD) are a major determinant of cognitive decline and disability in the elderly. 1 The clinical and imaging spectra of SVD are wide. More than 80% of elderly subjects present magnetic resonance imaging (MRI) markers of SVD such as white matter hyperintensities (WMH), lacunes of presumed vascular origin, microbleeds, or dilated perivascular spaces.1,2 In the general population, these markers were found associated with gait disturbances and cognitive performances and with a higher risk of stroke and dementia.1,2 Besides, SVD are actually responsible for one fifth of ischemic strokes and represent a major cause of dementia after Alzheimer’s Disease (AD). 2 Thus, SVD are now considered a major public health issue. 2 Recently, an international collaborative effort refined the terminology used in MRI examination in the setting of SVD to facilitate and promote the generalization of research results in this field. 3
In SVD, lesions most easily identified both at neuropathological evaluation and on conventional MRI lie in deep subcortical brain areas. This explains why the term ‘subcortical ischemic vascular dementia’ is often used to describe the severe cognitive decline presumably related to SVD, 4 in line with a classification proposed in the 1970s to differentiate various subtypes of neurodegenerative diseases and separating cortical from subcortical dementias. 5
There is now accumulating evidence in the literature supporting that the cortex is actually involved in SVD. Microinfarcts are commonly found in the cortex of elderly subjects at autopsy. They are associated with other markers of SVD and may represent a major determinant of cognitive impairment.6–9 Cortical atrophy, of comparable severity to that of AD, has been also demonstrated in neuropathological studies of a small number of SVD cases with dementia. 10 Although in vivo imaging is not yet capable of identifying the smallest lesions within the cortical mantle, recent results obtained using ultra-high field MRI showed that the largest intracortical infarcts become now identifiable. 9 Although these data support that the cerebral cortex may play a key role in SVD, the natural history of cortical changes in SVD and their underlying mechanisms remain undetermined.
The purpose of this review was to analyze data estimating in vivo the extent of cortex alterations associated with the wide spectrum of SVD lesions. To do so, we searched for articles that evaluated the cortical alterations observed at different stages of SVD using validated quantitative MRI parameters. In contrast to severe cases for which the diagnosis of SVD can be made according to different sets of validated criteria, there is little agreement regarding the diagnosis of SVD in the absence of stroke, disability, or severe cognitive alterations. Thus, we organized our review into three main parts: (a) studies evaluating the relationships between cortex alterations and MRI markers of SVD at the subcortical level in community-dwelling subjects; (b) identical studies in patients with symptomatic SVD or high vascular risk profile; and (c) studies that compared patients with SVD to age- and sex-matched controls. Given that concomitant AD may promote cortex alterations before the apparition of clinical symptoms, a specific attention was paid to this aspect.
Material and methods
This systematic review follows the PRISMA statements (http://www.prisma-statement.org). Studies were identified by searching PubMed and through systematic scanning of reference lists. Articles from our personal databases were added to the search strategy. Only articles published in English were considered. The last search was run on June 23, 2015. We used the following search terms: white matter lesions, white matter hyperintensity, white matter disease, white matter damage, lacunes, lacunar infarcts, microbleeds, small vessel disease, cerebral microangiopathy, leukoaraiosis, leukopathy, vascular cognitive impairment, subcortical ischemic vascular disease, voxel-based morphometry, cortical thickness, gray matter, grey matter, cortical atrophy, sulcal morphology, cortical morphology, cortical gyri, cortical sulci, cortical gyrification, cortex morphology, and cortical folding. By contrast, multiple sclerosis, progressive multifocal leukoencephalopathy and AIDS were exclusion search terms. The exact search algorithm is provided as supplementary material.
Given the complex architecture of the cerebral cortex, with such a highly folded structure and its small thickness relatively to its surface area, specific MRI protocols are needed to accurately segment the cortex and capture its variability. Thus, only studies based on recognized post-processing methodology relying on high-resolution T1 MRI sequences (i.e. study of cortical thickness, of cortical gray matter using either voxel-based methods or direct quantification, or of sulcal morphology—see Figure 1) were considered. Studies based on high-resolution MRI but evaluating gray matter globally (with inclusion of basal ganglia and cortex without distinction in analyses) and those based on computed tomography were not included. Only studies comparing a SVD group to a control group or studies investigating relationships between a validated subcortical MRI marker of SVD and cortical alterations were considered. Studies including mostly AD patients were excluded since the pathophysiology of WMH in this subgroup remains controversial.
11
We also chose not to evaluate cortical alterations reported in the hippocampus given the very limited local gray-white matter contrast that prevents studying reliably the alterations of cortex in this structure. Studies performed in the CADASIL model were also not included in the present analyses but related results were confronted to those obtained in sporadic SVD when necessary.
Main methods used to evaluate cortex alterations using in vivo MRI. Schematics of the different methods used to evaluate the cerebral cortex in vivo. Methods with registration involve positioning the MRI of different subjects in a common space to allow between subjects comparisons. This can be done through volume or surface-based registration. Methods without registration consist in extracting brain parameters from MRI in the native space of acquisition.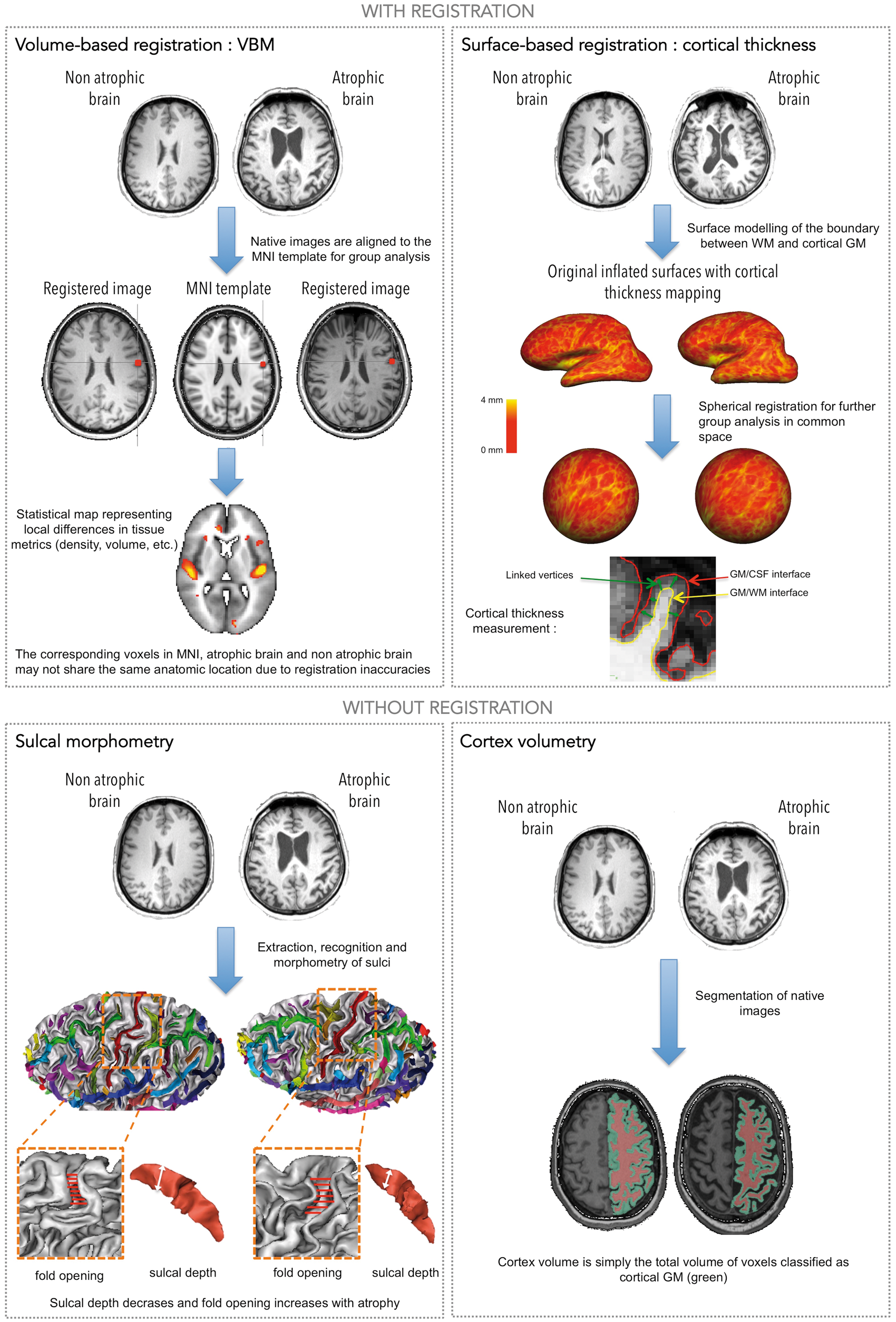
Results
We screened 934 articles, among which 78 full texts were analyzed in details (see Figure 2). Twenty-seven articles fulfilled the inclusion criteria. However, in some articles, data from the same cohort were repeatedly reported; therefore, the final number of distinct studies was 25. Nine were case–control studies, the relationships between the different subcortical MRI markers and cortex measures were evaluated in 16 others, 4 of which were longitudinal studies.
Flow diagram.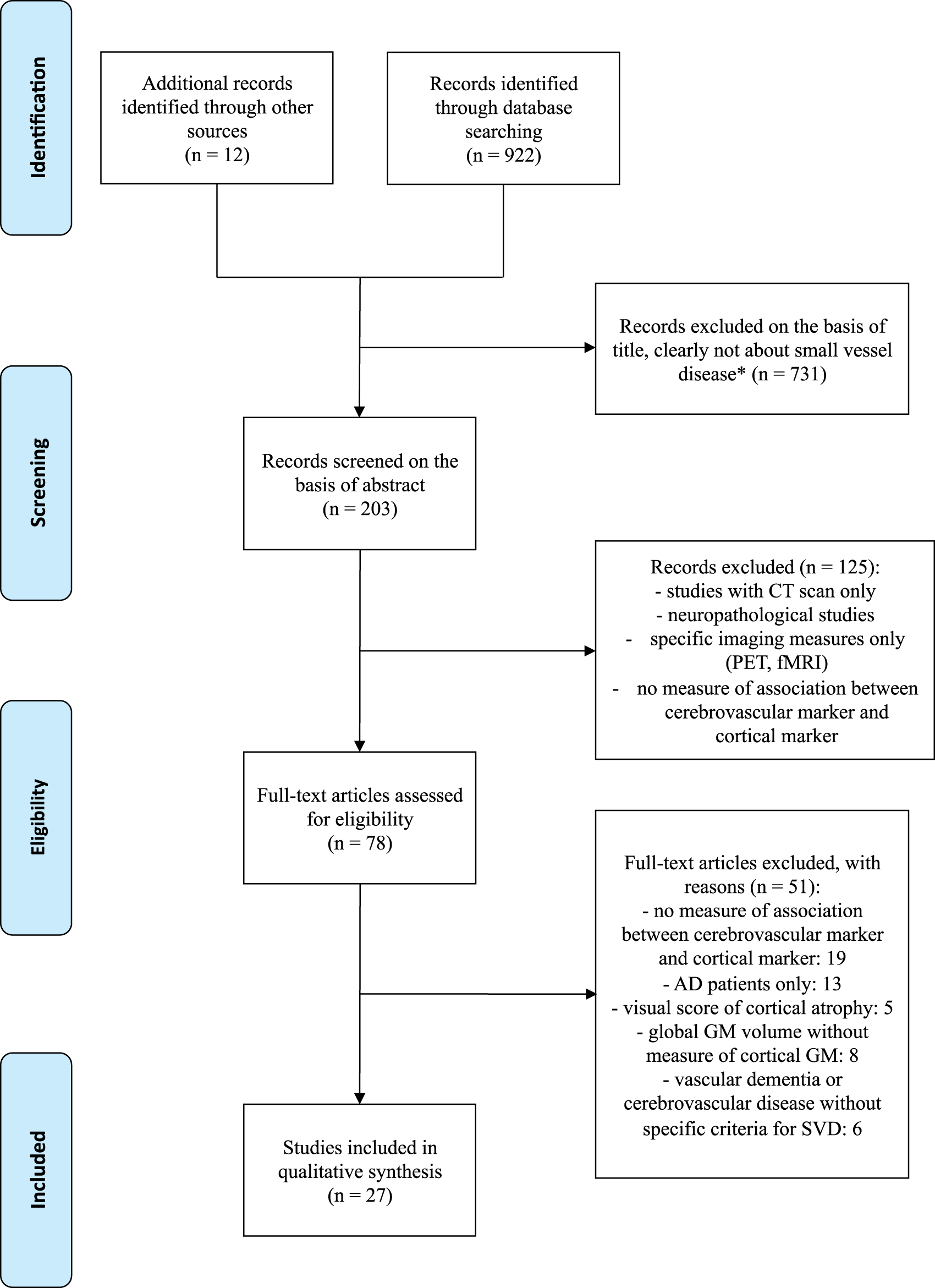
Association between MRI markers of SVD at the subcortical level and estimates of cortex alterations in community-dwelling subjects (see Table 1)
Relationships between subcortical MRI markers and cortical measures in community-dwelling individuals (ordered by sample size N).
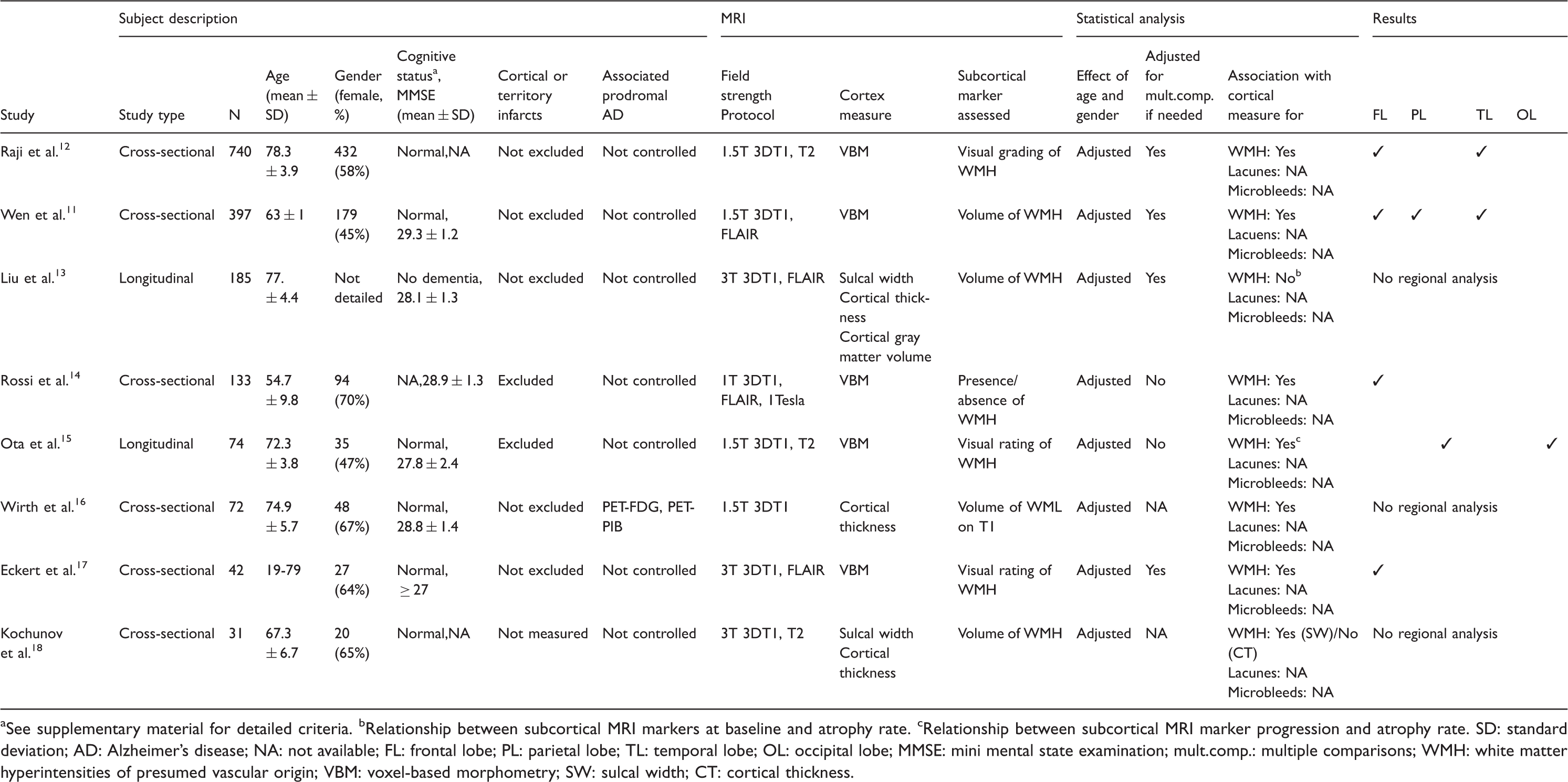
See supplementary material for detailed criteria.
Relationship between subcortical MRI markers at baseline and atrophy rate.
Relationship between subcortical MRI marker progression and atrophy rate.
SD: standard deviation; AD: Alzheimer’s disease; NA: not available; FL: frontal lobe; PL: parietal lobe; TL: temporal lobe; OL: occipital lobe; MMSE: mini mental state examination; mult.comp.: multiple comparisons; WMH: white matter hyperintensities of presumed vascular origin; VBM: voxel-based morphometry; SW: sulcal width; CT: cortical thickness.
Sample sizes were highly heterogeneous, ranging from 31 to 740 subjects.11–18 Mean age was around 75 years in four studies,12,13,15,16 lower in three others (55 in one and 65 in two),11,14,18 while age ranged from 19 to 79 years in one. 17
In all studies, subjects were scanned using 3DT1 1-mm isotropic sequences. Cortex measures were obtained using different techniques, with or without registration, as illustrated in Figure 1. Different methodologies were used to evaluate the burden of WMH: quantitative measures of WMH obtained by automated segmentation,11,13,16,18 semi-quantitative scales,12,15,17 or visual categorization according to WMH location. 14 Lacunes or microbleeds were not evaluated in any of the studies.
The relationships between voxel-based morphometry (VBM) estimates of total cortical gray matter and the burden of WMH were evaluated in four cross-sectional studies that always showed significant inverse associations, independent of age.11,12,14,17 This association was found independent of ApoE genotype in one study. 12 Results were not corrected for multiple comparisons in another one. 14 Finally, in a longitudinal study of 74 subjects, a significant inverse association was also detected between VBM estimates of total cortical gray matter changes and the progression of WMH during a mean follow-up of 3.8 years. 15
The relationships between cortical thickness and the volume of WMH were tested in three cross-sectional studies.13,16,18 A significant inverse relationship was reported in one. 16 In this study, subjects were divided between “abnormal” and “normal” cortical thickness. 16 The threshold between “normal” and “abnormal” cortical thickness was pre-determined according to previous results obtained by contrasting a population of cognitively normal elderly subjects defined clinically and biologically (CDR 0 and normal memory function together with negative Florbetapir-PET imaging or biomarkers obtained through lumbar puncture) to a population of mild AD defined clinically (NINCDS ADRDA criteria, MMSE score between 20 and 26 and CDR of 0.5 or 1). A significantly higher volume of WMH was observed in subjects with “abnormal” cortical thickness compared with subjects with “normal” cortical thickness, independent of age, 16 a finding that could not be explained by associated prodromal AD in the “abnormal” group as Aβ deposition on 11C-PIB-PET imaging did not differ between the two groups. By contrast, there was no significant association between cortical thickness and the volume of WMH in two other studies.13,18
The relationships between sulcal width and the volume of WMH were evaluated in two different studies and revealed a significant association independent of age in one, 18 but not in the other. 13 However, the interpretation of these non-significant results is difficult as these analyses were not the primary aim of those studies and detailed results were not provided.13,18
In summary, significant relationships between cortical gray matter volume and WMH are consistently observed with VBM approaches in community-dwelling elderly but links between WMH and other cortical parameters are inconsistently detected. The cortical impact of lacunes and/or microbleeds is not evaluated yet in these populations and only few data are available to determine whether the cortical alterations are actually secondary to effects of SVD rather than to concomitant prodromal AD.
Association between MRI markers of SVD at the subcortical level and estimates of cortex alterations in patients with symptomatic SVD or with high cardio- or neuro-vascular risk profile (see Table 2)
Relationships between subcortical MRI markers and cortical measures in populations at high cardio-neurovascular risk (ordered by sample sizes N).
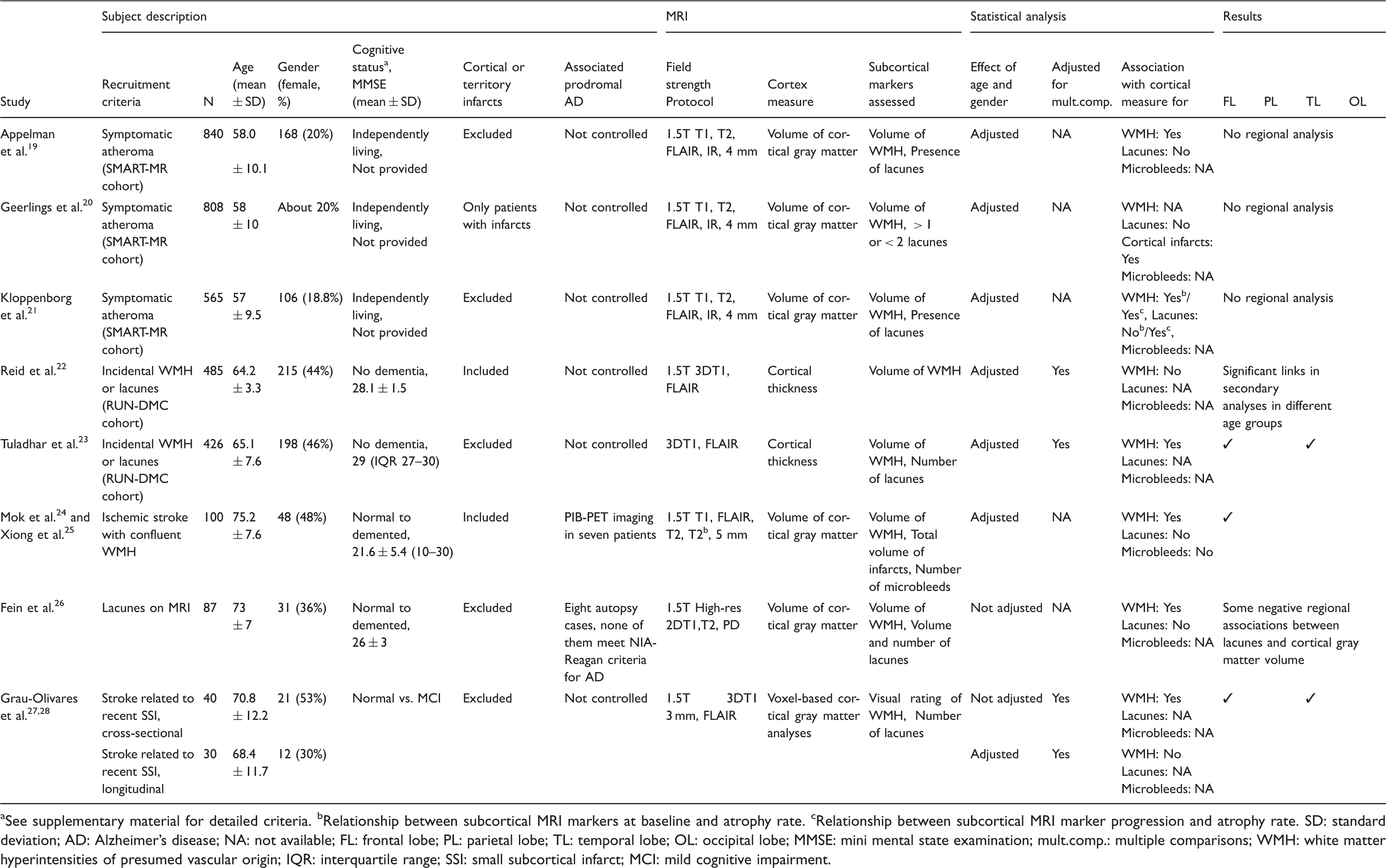
See supplementary material for detailed criteria.
Relationship between subcortical MRI markers at baseline and atrophy rate.
Relationship between subcortical MRI marker progression and atrophy rate.
SD: standard deviation; AD: Alzheimer’s disease; NA: not available; FL: frontal lobe; PL: parietal lobe; TL: temporal lobe; OL: occipital lobe; MMSE: mini mental state examination; mult.comp.: multiple comparisons; WMH: white matter hyperintensities of presumed vascular origin; IQR: interquartile range; SSI: small subcortical infarct; MCI: mild cognitive impairment.
In five studies based on three different cohorts, patients were recruited if they had at least one cerebral infarct, most often attributable to SVD. Two reports were based on the same small cohort, in which patients were recruited after a first small subcortical ischemic stroke with separate reports of cross-sectional, 27 and longitudinal analyses. 28 Another cohort comprised 100 patients with any type of ischemic stroke and confluent WMH (60 from these 100 patients had a small subcortical ischemic stroke) and was the basis of two different reports.24,25 In the fifth study, patients were included if they had a history of small subcortical ischemic stroke or a radiologic report of lacune. 26 The sample size of these cohorts ranged from 40 to 100 subjects, mean age was 72 years and mean MMSE score around 25.
Two larger studies (426 and 503 subjects) based on the RUN-DMC cohort, included patients if they had WMH or lacunes on MRI performed for any acute or subacute symptom attributable to SVD.22,23 Those patients were clinically healthier and younger than those recruited in the five above-mentioned studies, with a mean age of 65 years and a mean MMSE score of 28. They also had a relatively low burden of MRI markers of SVD (mean volume of WMH = 12.96 ml; presence of lacunes in 21% of cases) compared with the three first cohorts (mean volume of WMH = 25.06 ml; presence of lacunes in 60 to 100% of patients).
Finally, three studies were based on the SMART-MR cohort that included independently living individuals with symptomatic atherosclerosis (coronary artery disease, stroke or TIA, peripheral arterial disease or abdominal aortic aneurysm).19–21 Their sample size was large (565 to 840 subjects) and the mean age of patients was 58 years.
The presence of cortical infarcts was an exclusion criterion in 6 of 10 studies.19,21,23,26–28 The burden of WMH was evaluated quantitatively in eight studies19–26 and using a semi-quantitative visual score in two.27,28 In seven studies, lacunes were defined as lesions appearing hyperintense on T2 sequence and hypointense on T1 sequence and Flair sequences, and rated either by splitting the population according to the presence and absence of lacunes19,21 or by assessing the number and/or volume of lacunes.20,26–28 Lacunes were not assessed in one study 22 or assessed globally with other infarct types in two others.24,25 The number of microbleeds was only assessed in two studies based on the same cohort.24,25 Attempt to rule out AD diagnosis was made in three studies.24–26 In one, eight brain autopsies were performed, blind to clinical and MRI data and none of them met the NIA-Reagan Institute criteria supporting a high likelihood of AD. 26 In the two others based on the same cohort, 11C-PIB-PET imaging was performed in 7 out of the 100 recruited patients and showed no significant PIB retention.24,25
The relationships between the total volume of cortical gray matter and WMH was tested in four cross-sectional studies based on three different cohorts.19,24–26 All showed significant negative associations independent of age. The results obtained in one longitudinal study showed that both the baseline volume and the increase of periventricular WMH were significantly associated with a larger decrease of the total cortical gray matter volume after a mean follow-up of 3.9 years. 21 A possible bias in some of these studies originating from the same SMART-MR cohort, including the longitudinal study,19,21 was the use of 4-mm thick MR slices that may impact estimates for a highly folded structure such as the cerebral cortex. 29
The relationships between the total volume of cortical gray matter and lacunes were tested in five cross-sectional studies and in one longitudinal study. By contrast to the consistent associations observed between cortex alterations and the burden of WMH, no association was observed between the total volume of cortical gray matter and the presence, 19 number, 20 or volume 26 of lacunes in cross-sectional studies. There was no association either between the volume of cortical gray matter and the total volume of infarcts, including lacunes, in 100 patients with confluent WMH included after any type of ischemic stroke.24,25 By contrast, a significant association between a reduction of the total volume of cortical gray matter and the progression of lacunes, independent of age, gender, baseline brain volume, and follow-up time, was reported in a single study. 21 Finally, no significant association was found between cortical gray matter volume and microbleeds in two studies investigating this aspect.24,25
The relationships between cortical thickness and WMH were tested in two studies originating from the RUN-DMC cohort. The results were inconsistent showing a lower cortical thickness related to the volume of WMH in one study 23 and no significant association in another one, except in secondary subgroup analyses. 22 A possible explanation might be that about 50 patients with cortical infarcts were not excluded from analyses in this latter study although such lesions are another prominent source of cortical atrophy. We found no study that evaluated the relationships between cortical thickness and lacunes or microbleeds.
Finally, VBM analyses were performed in two studies based on a single small cohort. Cross-sectional analyses showed a significant association between cortical gray matter estimates and the extent of WMH that did not persist in longitudinal analyses.27,28 This discrepancy may be explained by the 25% of loss of follow-up in the longitudinal study and by the lack of adjustment for multiple comparisons in cross-sectional analyses. No association between cortical estimates obtained through VBM analyses and lacunes was reported.27,28
In summary, despite the strong heterogeneity of the samples of patients with SVD or high risk profile, significant inverse relationships between most MRI estimates of cortex structure and the extent of WMH were consistently reported. By contrast, the relationships between cortex alterations and lacunes or microbleeds have been more rarely assessed and showed mostly non-significant associations. Some efforts were made to exclude concomitant AD in these studies, reinforcing the hypothesis of cortex alterations in the context of SVD patients, even in the absence of dementia.
Cortex alterations in patients with SVD by comparison with age- and sex-matched controls
Patients with SVD diagnosed using clinical criteria (see Table 3)
Case–control studies of patients with SVD according to clinical and neuroimaging data (ordered by sample sizes N).
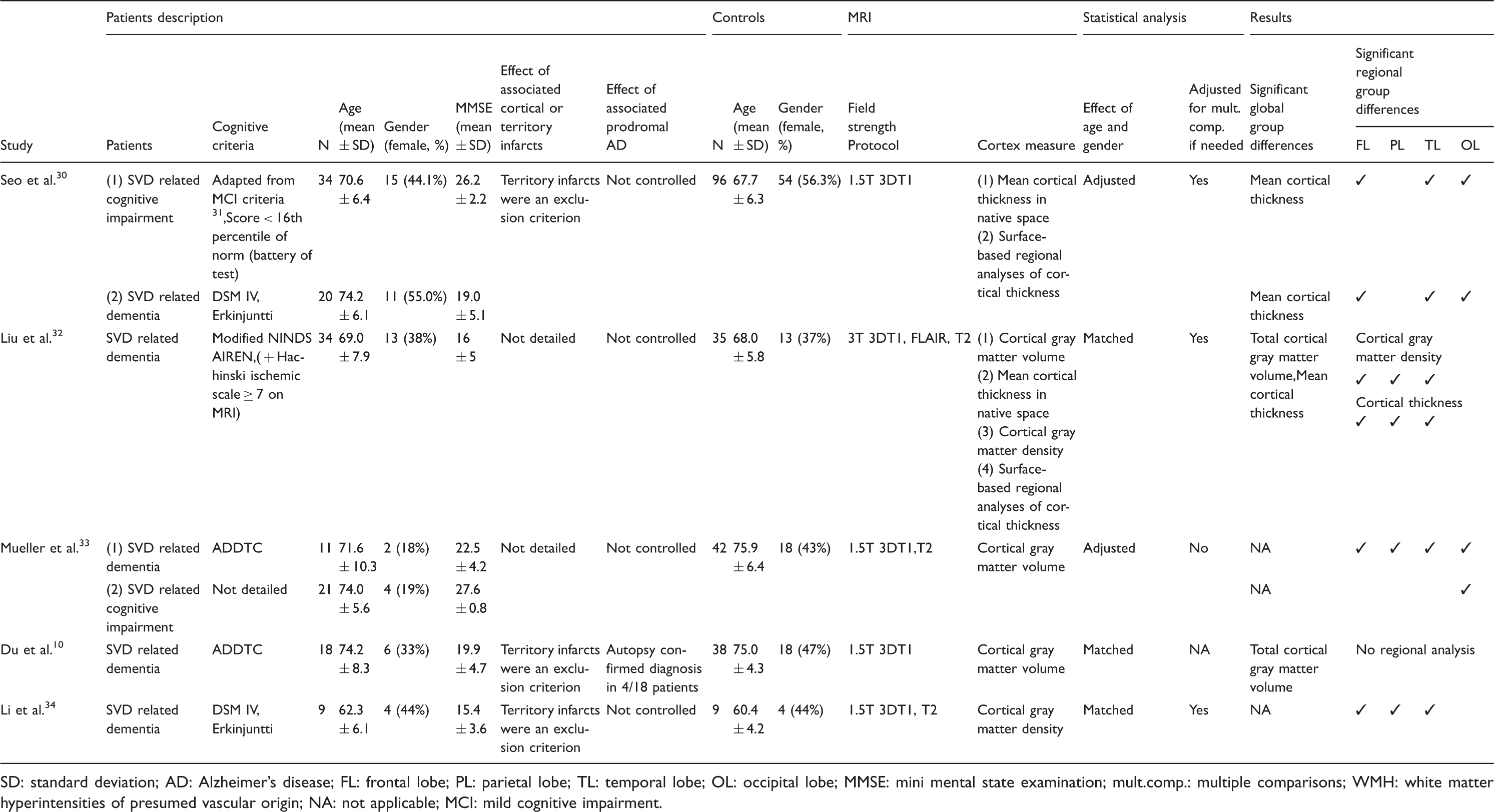
SD: standard deviation; AD: Alzheimer’s disease; FL: frontal lobe; PL: parietal lobe; TL: temporal lobe; OL: occipital lobe; MMSE: mini mental state examination; mult.comp.: multiple comparisons; WMH: white matter hyperintensities of presumed vascular origin; NA: not applicable; MCI: mild cognitive impairment.
Sample sizes in these five studies were small (mean number of patients: 29, mean number of controls: 52). Mean age was about 70 years in four studies10,30,32,33 and close to 60 years in one. 34 Controls were age- and sex-matched in three studies10,32,34 and analyses were adjusted for age and gender in the two others.30,33 Patients and controls were in all cases evaluated using the same scanner, MRI sequence and post-processing method based on 3DT1 millimetric isotropic resolution.
The mean cortical thickness measured over the whole cortex was compared between SVDD patients and controls in two studies and between SVDCI patients and controls in one, with significantly lower measures observed in patients in all cases.30,32 In additional regional analyses, group differences were consistently observed in frontal and temporal areas.30,32
The total cortical gray matter volume was compared between SVDD patients and controls in two studies, showing significant lower volumes in patients in both of them.10,32 The volume of cortical gray matter measured in each cerebral lobe (without reporting global measures) was compared between SVDD or SVDCI patients and controls in a single study. 33 Significantly lower cortical gray matter volume were observed in SVDD patients in all cerebral lobes and in SVDCI patients only in the occipital lobe. 33
Finally, local cortical gray matter estimates determined using VBM were compared between SVDD patients and controls in two studies, with significantly lower estimates observed in patients in both studies, in all cortical regions but the occipital lobe.32,34
Additionally, the relationships between the burden of subcortical MRI markers of SVD and cortex alterations in SVDD patients were tested in only one study, showing, using uncorrected additional analyses, that a higher number of lacunes was associated with a lower cortical thickness in frontal, parietal, temporal, and insular lobes. 32 By contrast, the volume of WMH was not related to cortical thickness. 32 These relationships were also tested in one study after pooling SVDD and SVDCI patients, showing a significant linear negative association between the volume of WMH and that of cortical gray matter in all lobes, but this was also observed in controls. 33 The association between lacunes and cortex alterations was not evaluated in this study. 33
In summary, significant and consistent alterations of cortex estimates were reported using various methodologies in patients with cognitive impairment or dementia attributed to SVD by comparison with age- and sex-matched controls. However, with the exception of post-mortem data confirming the diagnosis of SVD in four cases in one study, few data are available to ensure that cortex alterations are actually related to SVD and are not secondary to a degenerative disorder.
Patients with SVD diagnosed according to radiological criteria (see Table 4)
Case–control studies of patients with SVD according to neuroimaging data (ordered by sample sizes N).
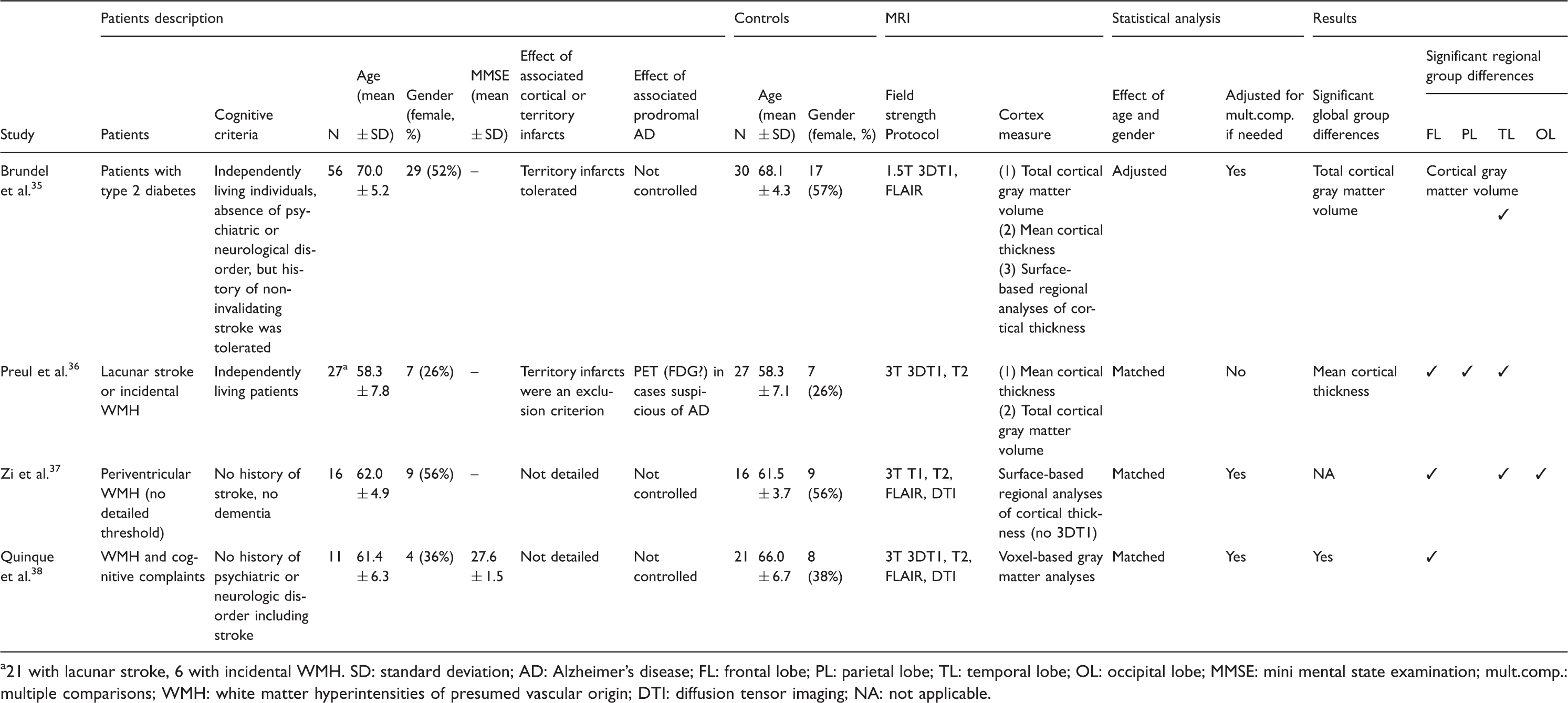
21 with lacunar stroke, 6 with incidental WMH.
SD: standard deviation; AD: Alzheimer’s disease; FL: frontal lobe; PL: parietal lobe; TL: temporal lobe; OL: occipital lobe; MMSE: mini mental state examination; mult.comp.: multiple comparisons; WMH: white matter hyperintensities of presumed vascular origin; DTI: diffusion tensor imaging; NA: not applicable.
Sample sizes were small (mean number of patients: 16, mean number of controls: 24). Mean age was about 60 years in three studies36–38 and 70 years in the other. 35 Controls were age- and sex-matched in three studies36–38 and analyses were adjusted for age and gender in the other. 35 Patients and controls were assessed on the same scanner using the same sequence in all cases and post-processing relied on MRI with 3DT1 1 mm isotropic resolution in all studies but one that used T1 weighted sequence with a slice thickness of 5 mm. 37
The mean cortical thickness measured over the whole cortex was compared between SVD patients and controls in two studies,35,36 reporting in both cases lower cortical thickness in patients, that reached significance in only one study. 36 This was possibly related to the different profiles of patients selected in these studies: the difference was significant in the sample including cases with severe SVD (21 out of 26 patients had lacunar stroke) 36 but not in diabetic patients among which some had a diagnosis of SVD. 35
The total cortical gray matter volume was compared between SVD patients and controls in the same two studies. The total volume of cortical gray matter was lower in patients in these two studies,35,36 but statistical significance was reached only in the diabetic sample. 35 Whether this difference is directly related to the role of diabetes 35 or due to technical issues 36 remains undetermined.
Surface-based regional analyses of cortical thickness was performed in two studies35,37 and showed a significantly lower cortical thickness in patients compared with controls in both. This reduction was detected diffusely except in the parietal lobe in one study 37 but analyses were not corrected for multiple comparisons. It was found only in the temporal lobe in the other study. 35 Whether technical issues explain these differences could not be totally excluded.
Finally, VBM estimates of cortical gray matter were compared in only one study between a very small sample of 11 patients having WMH on MRI performed for cognitive complaints and controls. In this study, significantly lower estimates of cortical gray matter in two clusters located in the frontal lobes bilaterally were detected in SVD patients compared with controls. 38 These results remain difficult to interpret given the small number of patients and the very focal asymmetric clusters detected.
In summary, in patients with SVD defined according to a wide range of MRI criteria, significantly lower cortex estimates were consistently observed by comparison with age- and sex-matched controls. However, these studies included only small sample sizes, were in all cases cross-sectional, and efforts were rarely made to exclude concomitant prodromal AD as a source of the observed cortical alterations.
Discussion
The results of the present systematic review support the hypothesis that the cerebral cortex is diffusely altered in SVD, from the earliest stages in subjects sampled from the general population and having only WMH on their MRI to latest stages, in patients with stroke and/or dementia attributed to SVD, thus challenging the concept of “subcortical ischemic vascular dementia.” Although the results of most articles included in the present review are consistent, important questions remain unanswered.
First, given the fact that AD can promote cortex atrophy before the appearance of clinical symptoms,39,40 it is important to keep in mind that the reported cortex alterations are not necessarily the results of SVD. Only in 5 among the 25 studies identified in the present review, the authors attempted to exclude a possible role of concomitant prodromal AD. 11C-PIB-PET imaging was performed in 72/72 subjects in one study, 16 in 7/100 individuals in the other 24 and ruled out PIB binding consistent with AD diagnosis. FDG-PET imaging was obtained in an additional study for patients with suspected AD who were excluded when cortical hypoperfusion consistent with AD was detected. 36 Finally, AD was excluded according to autopsy data in only two studies (in 4/18 subjects in one study, 10 in 8/87 subjects in the other 26 ). Nonetheless, it is important to note that, given the frequency of mixed cases, even those studies could not formally exclude an effect of associated neurodegenerative illnesses.40–42 In this respect, it is important to emphasize that cortical alterations were also demonstrated in hereditary SVD affecting younger patients.43–46 Anyway, further studies including a larger number of patients with quantification of both SVD and neurodegenerative processes are needed to determine the exact extent of cortex alterations in SVD without associated AD, and the relative impact of AD and of SVD on cortex metrics in patients having both SVD and AD.
Second, the nature of the observed cortex alterations also remains incompletely understood. No study trying to disentangle the effects on cortical gray matter volume or cortical thickness from that on cortical surface area or cortex morphology was done yet. Additionally, as effect sizes were rarely provided in the different studies, it was not possible to compare the results of the different studies by other means than by their significance. Also, technical issues or global brain alterations could lead to the detection of group differences, particularly with the use of VBM estimates, that may not be related to cortex alterations. 47 Additionally, cortical thickness, but not cortex morphology, is strongly dependent on gray to white matter contrast, which is clearly altered in SVD, 48 while cortex morphology is strongly dependent on the underlying white matter structure. 49
The mechanisms linking subcortical markers of SVD with cortical alterations remain to be determined. The inverse links repeatedly observed between the extent of WMH and cortex alterations, independent of age, might be secondary to remote degeneration. 45 Alternatively, WMH in subcortical areas might also be in part secondary to cortical atrophy through retrograde degeneration.11,33,50 Another explanation could be that WMH and cortical alterations share common underlying mechanisms such as chronic hypoperfusion.11,24 By contrast to that of WMH, the association between lacunes or microbleeds with cortex alterations were only rarely and inconsistently observed precluding any conclusion regarding their own impact. The observed impact of lacunes on remotely connected cortex in a genetic model of SVD suggests that lacunes can actually lead to cortex alterations through secondary degeneration, 45 which may even promote amyloid deposition. 42
The relationships between cortical alterations and cognitive status were analyzed in 10 out of the 25 selected studies. While memory and global cognition were associated with alterations of cortex measures in few studies,26,32 the most consistent finding is that executive functions and processing speed12,16,23,37 are significantly related to the cortical alterations detected in SVD. This association was found independent of age, gender, and of level of education. Some results even suggest that cortical alterations in SVD may impact cognition independently of WMH volume and sometimes, even with a stronger effect than that found only with WMH.23,24 Further studies are needed to determine the impact of cortex alterations independently of other MRI markers of SVD, particularly global brain atrophy.
Altogether, despite an important heterogeneity in SVD definition, methodologies, post-processing methods and strategies in data analysis, the results of these studies provide strong evidence that diffuse alterations of the cerebral cortex may occur early during the course of SVD. Available data also support that SVD should no longer be considered as a subcortical disorder. Further studies are needed to better depict the mechanisms and consequences of cortical alterations in SVD.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by grants from the Network of European Funding for Neuroscience Research grant (01EW1207), from Fondation Leducq (Transatlantic Network of Excellence on the Pathogenesis of Small Vessel Disease of the Brain, ![]() ), and from the Ile-de-France regional health agency.
), and from the Ile-de-France regional health agency.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contributions
EJ and HC designed the review. RP and FDG collected and analyzed the literature. RP, FDG, and EJ wrote the initial draft of the review. All authors reviewed the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.