
Abstract
Background:
The SARS-CoV-2 pandemic is a constant challenge for health care systems, also in Germany. Care of seriously ill and dying people and their relatives is often neglected and suffering increased due to sub-optimal symptom management, visiting restrictions and lonely dying. The project “Palliative Care in Pandemics (PallPan)” intended to develop a national strategy including evidence- and consensus-based recommendations for the care of seriously ill and dying people and their relatives during pandemic times in Germany.
Aim:
To reach consensus on evidence-based recommendations for the care of seriously ill and dying people and their relatives in pandemics.
Methods:
Three-step consensus process comprising two online Delphi rounds and an expert workshop conducted from April to June 2021. One hundred twenty experts from various areas of healthcare, administration, and politics in Germany were included.
Results:
During the consensus-process, pre-formulated evidence-based recommendations were refined step-by-step. This resulted in consensus on 33 recommendations on the topics of “supporting patients and their relatives,” “supporting staff,” and “supporting and maintaining structures and provision of palliative care.” The recommendations address professional carers and various responsibilities on a governmental, federal state and municipal level, and in healthcare facilities.
Conclusion:
We provide evidence and consensus-based recommendations for the care of seriously ill and dying people and their relatives in pandemics in Germany. This is an important step towards a pandemic preparedness and hopefully improves the future palliative care response to pandemics.
Keywords
What is already known about the topic
The SARS-CoV-2 pandemic poses various strains on seriously ill and dying patients and their relatives as well as on health care staff involved in their care.
People receiving palliative care were easily overlooked in policies concerning the German pandemic response.
What this paper adds
Currently, a consistent national strategy for the care of seriously ill and dying people and their relatives during the pandemic is lacking in Germany. PallPan’s national strategy with evidence and consensus-based recommendations fills a gap in the organization of generalist and specialist palliative care in the response to a pandemic.
This paper provides 33 evidence and consensus-based recommendations for the care of seriously ill and dying people and their relatives in pandemic times, addressing the needs of patients and relatives, of staff and care structures for palliative care provision.
Implications for practice, theory, or policy
The national strategy includes recommendations with hands-on advice for generalist and specialist palliative care providers in healthcare facilities.
The national strategy provides clear recommendations and best practice examples for people in charge of hospitals, nursing homes, and other care institutions for generalist and specialist palliative care during the pandemic.
Policy makers on governmental, federal state, and municipal level are given advice on how to support and maintain structures and provision of generalist and specialist palliative care in the response to pandemics.
Introduction
Palliative care aims to prevent and relief physical and psychological suffering as well as social and spiritual distress in seriously ill or dying patients and their relatives. The WHO states that implementing these key elements of palliative care is imperative in responses to humanitarian crises, such as outbreaks of infectious diseases. 1 As the pandemic underpinned, suffering during outbreaks of life threatening infections may result from both the disease and the medical or public health response. 2
The SARS-CoV-2 pandemic demonstrated that the German health care system was not sufficiently prepared for the challenges of providing care for seriously ill and dying people and their relatives in a pandemic—both for infected and non-infected people. The needs of patients dying from their COVID-19 infection and their relatives were often not considered and patients were isolated in hospital and did not have access to sufficient palliative care. Also, patients who are at high risk of a severe course of a Covid-19 infection are cared for in the field of palliative medicine. 3 During the pandemic, not only the possibility of getting an infection poses a threat to seriously ill and dying people, they also feared that they would no longer be able to receive necessary treatment. Patients already carrying a heavy burden due to their illness often found themselves isolated and alone with their fears. Inpatient treatment was discontinued by some to spend the time they had left with their families. Accompaniment and support services for those affected were often limited or even completely discontinued. Relatives were not even allowed to say goodbye to their dying loved ones.4,5
Outbreaks of infectious diseases will occur more frequently in the future and will have more severe consequences. 6 In a pandemic, the need and supply for palliative care support is expected to increase substantially and palliative care services will also need to be available across many different care settings. 7 The strengths of palliative care are symptom management, communication, and support in end-of-life decisions. Therefore, generalist and specialist palliative care principles should be part of national crises management. This poses the urgent need to establish a palliative pandemic preparedness in Germany.
PallPan
The project “Palliative Care in Pandemics (PallPan)” intended to develop a “National strategy for the care of seriously ill and dying people and their relatives in pandemics.” Dignified and competent care for seriously ill, dying, and bereaved people should be made possible throughout Germany, even under the challenging circumstances of a pandemic. As the centerpiece of the strategy, recommendations for generalist and specialist palliative care for infected and non-infected patients were developed by the PallPan consortium of thirteen university palliative care institutions from all over Germany. 8 The development process of the recommendations are the focus of this paper. Alongside the recommendations, the strategy includes best practice examples and further information on establishing a palliative pandemic preparedness.
Existing recommendations from national and international pandemic plans and international literature on palliative care during pandemics were searched and served as a basis for the development of the recommendations. 9 The initial recommendations emerged from 16 primary studies conducted by the PallPan consortium, which describe and explore the provision of palliative care during the first and second wave of the pandemic in Germany.8,10–12
In the end of March 2021, a first draft was finalized with 34 recommendations. Each recommendation was composed of one introductory statement with following statements as bullet points. Including the introductory statement, the recommendations comprised a total of 101 different statements. The recommendations address professional carers and various responsibilities on a governmental, federal state and municipal level, and in healthcare facilities. The aim of this Delphi study was to reach consensus on the previously developed evidence-based recommendations for the care of seriously ill and dying people and their relatives in pandemics in Germany.
Methods
In this study, a modified Delphi Method was applied. During the classical Delphi procedure, recommendations are evaluated and commented on by experts from various fields in several questionnaire rounds.13,14 Because of time constraints, we adapted this procedure and conducted two Delphi rounds and an expert workshop between the two rounds from April to June 2021. We followed the Guidance on Conducting and REporting DElphi Studies (CREDES) in palliative care. 15
Participants
The process of identifying and recruiting experts followed a multiple-step iterative approach and comprised the definition of inclusion criteria, naming possible experts, selection of relevant experts, and invitation of experts. 16
Definition of inclusion criteria
To determine inclusion criteria, the German health system’s responsibilities for pandemics were analyzed. Relevant occupational settings of experts were defined on three system-levels (macro, meso, and micro level).17–19 The macro level is characterized by systems operating on a governmental level. These systems are responsible for the maintenance of the health system in case of a pandemic. Systems operating on the meso level reach federal states and municipal levels. The micro level comprises all institutions and professionals concerned with health care and palliative care, both generalist and specialist.17–19 On the micro level we differentiated between (1) responsibility for institutions or services providing generalist and specialist palliative care and (2) service provision (staff).
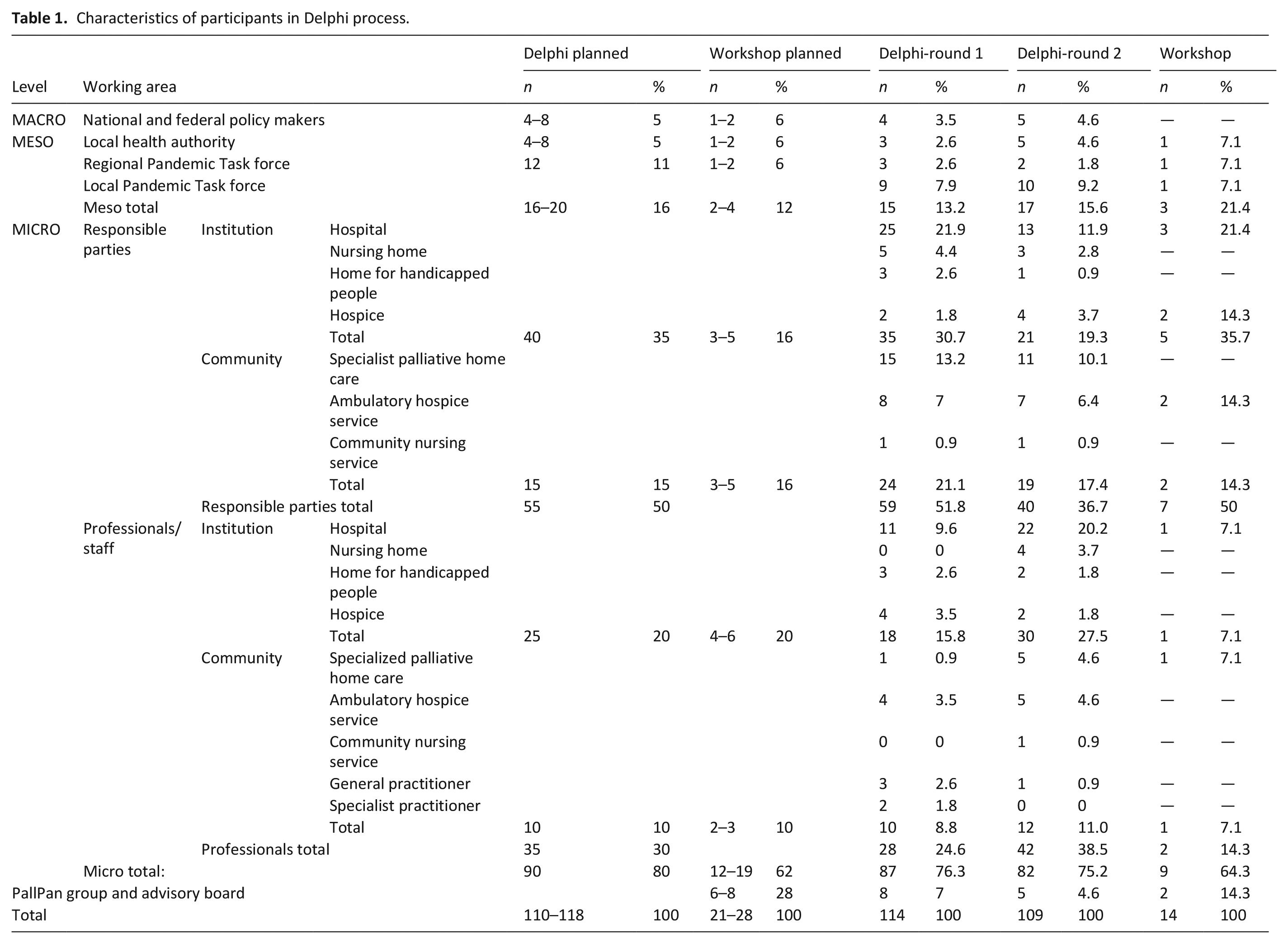
The experts involved in the consensus process should be representatives of the target groups of the recommendations. To assess to which extent each level should be represented in the consensus process, the preliminary draft of the recommendations (beginning of March 2021) was analyzed regarding the composition of target groups. From this analysis we defined a desired composition of professionals and responsibilities in the Delphi rounds and in the expert workshop (see Table 1). Furthermore, relevant criteria for the desired experts were defined. These were “responsibility in the context of the pandemic (policy maker, part of a pandemic response team, organizational task in the pandemic, responsibility in a care setting)” or “care for seriously ill and dying individuals and their relatives.”
Characteristics of participants in Delphi process.
Naming possible experts and selection of relevant experts
The PallPan consortium proposed names of possible experts. Relevant experts were chosen by considering the above defined criteria and relevant occupational settings as well as representation of federal states. One hundred twenty experts were identified for participation in the Delphi process. Of these, 28 were chosen to be invited to the workshop (inclusion criteria as above, desired percentage of professions and responsibilities according to Table 1).
Invitation of experts
All identified relevant experts were contacted via e-mail on 12th April 2021 and were invited to participate in the Delphi process. The e-mail contained a link leading to the online survey of the first Delphi round. Ten days later, a reminder was sent to all participants originally invited to the Delphi process. On 23rd April 2021, the relevant experts were invited to the workshop. The link to the survey for the second Delphi round was sent on 26th May 2021 and experts were reminded to participate 1 week later.
Part 1: First Delphi round
Questionnaire
Using the online survey tool LimeSurvey, an online survey was developed. 20 It was based on the structure of the recommendations and was piloted by five independent researchers. The survey comprised a welcome site with explanations about the PallPan Project and the development of the recommendations. The participants were invited to assess the recommendations based on their expertise and professional experience. When assessing the recommendations, the experts were asked to consider relevance, feasibility and comprehensibility of each of the 101 statements of the recommendations. Subject of the vote was their agreement with each statement. Each survey page had three items, item one being the voting of the recommendation, item two comprised space for additional comments, and item three demonstrated best practice examples for the recommendation in question. Voting of the statements was based on a 6-point Likert-scale. 21 The answer options were “I agree completely,” ”I agree”, “I rather agree,” “I rather disagree,” “I disagree” and “I totally disagree.” A seventh option “I can’t judge this issue” was provided to skip the voting for the respective recommendation if participants did not feel competent to judge the recommendation. An exemplary illustration of the survey pages can be found in Supplemental Appendix.
Application
The participation in the survey was voluntary and anonymous. By completing the survey, participants consented to take part in the study. Data protection was guaranteed. IP addresses of participants were not saved. To prevent multiple entries, cookies were saved. The participants were able to save their responses and proceed another time. Participants could navigate forward and backward. Voting of item one was mandatory.
Analysis
Only complete surveys were considered. Voting data was analyzed using the Statistical Package for the Social Sciences (SPSS, Version 27) and free text comments were downloaded in an excel sheet. The proportion of answer options was calculated for each statement of the recommendations. Consensus was defined as agreement ⩾75%. Agreement included the answer options “I agree completely” and “I agree.” If at least one statement of a recommendation did not reach consensus, the whole recommendation did not reach consensus and was discussed in the workshop. Free text comments for all recommendations were analyzed by two independent members of the research group (STS, AP). Each recommendation was revised according to relevant aspects agreed on by both. The revisions related either to the content of the recommendation or were of editorial nature. If the content needed adaptation, the recommendation was discussed in the workshop.
Part 2: Workshop
We conducted a 1-day, face-to-face meeting via Zoom with 14 selected experts. 22 The workshop was coordinated by an independent moderator. The aim of the workshop was to discuss and revise recommendations based on the results of the first Delphi round. In the first part of the workshop, the recommendations that did not reach consensus were discussed and edited in break-out sessions with small groups of experts (4–5 persons). Afterward, changes and still existing problems were discussed in the plenum. After the plenary discussion, the experts voted on the modified recommendations. The second part of the workshop included the plenary discussion, editing and voting of the recommendations that reached consensus in the first Delphi round but were modified in terms of content because of emerging aspects in the free text comments.
For voting during the workshop, “onlineTED,” a live, flexibly adjustable online voting tool was used. 23 The response options included either agreement/disagreement on a 5-point Likert scale (the previously used 6-point Likert scale could not be adhered to because the onlineTED application only allowed five response options), “Yes/No” answers or voting between different possible wordings of the recommendation.
Part 3: Second Delphi round
All recommendations discussed and revised in the expert workshop were put to vote in the second Delphi round. The questionnaire of the second Delphi round was similar to the questionnaire in the first round. In contrast to the first round, participants were asked to rate the whole recommendation, meaning the introductory statement with following statements in bullet points in the second round. Application and analysis of the survey took place similarly to the first round. If a recommendation did not reach consensus in the second round, it was excluded. Free text comments were screened for new emerging aspects according to the first Delphi round.
The study was approved by the Local Research Ethics Committee of the Medical Faculty of the Ludwig-Maximilians-University Munich (No. 21-0324).
Results
Participants in Delphi rounds
Of 120 invited experts in the first Delphi round, five declined participation due to too many other commitments. Thus, the number of experts contacted decreased to 115 in the second round. In each round, 73 experts provided responses and completed the survey (60.8% and 63.5%, following the definition of the “minimum response rate”). 24 Participants represented most of the 16 federal states of Germany (besides Saarland, Bremen, Schleswig-Holstein, and Sachsen-Anhalt). About more than half of the participants were female in the first round (n = 39; 53%) and less than half in the second round (n = 32; 44%). Experts were mostly between 41 and 70 years old. More than half had more than 10 years professional experience (n = 46; 63% and n = 41; 56% respectively). The composition of professional background in the Delphi rounds can be found in Table 1.
Part 1: First Delphi round
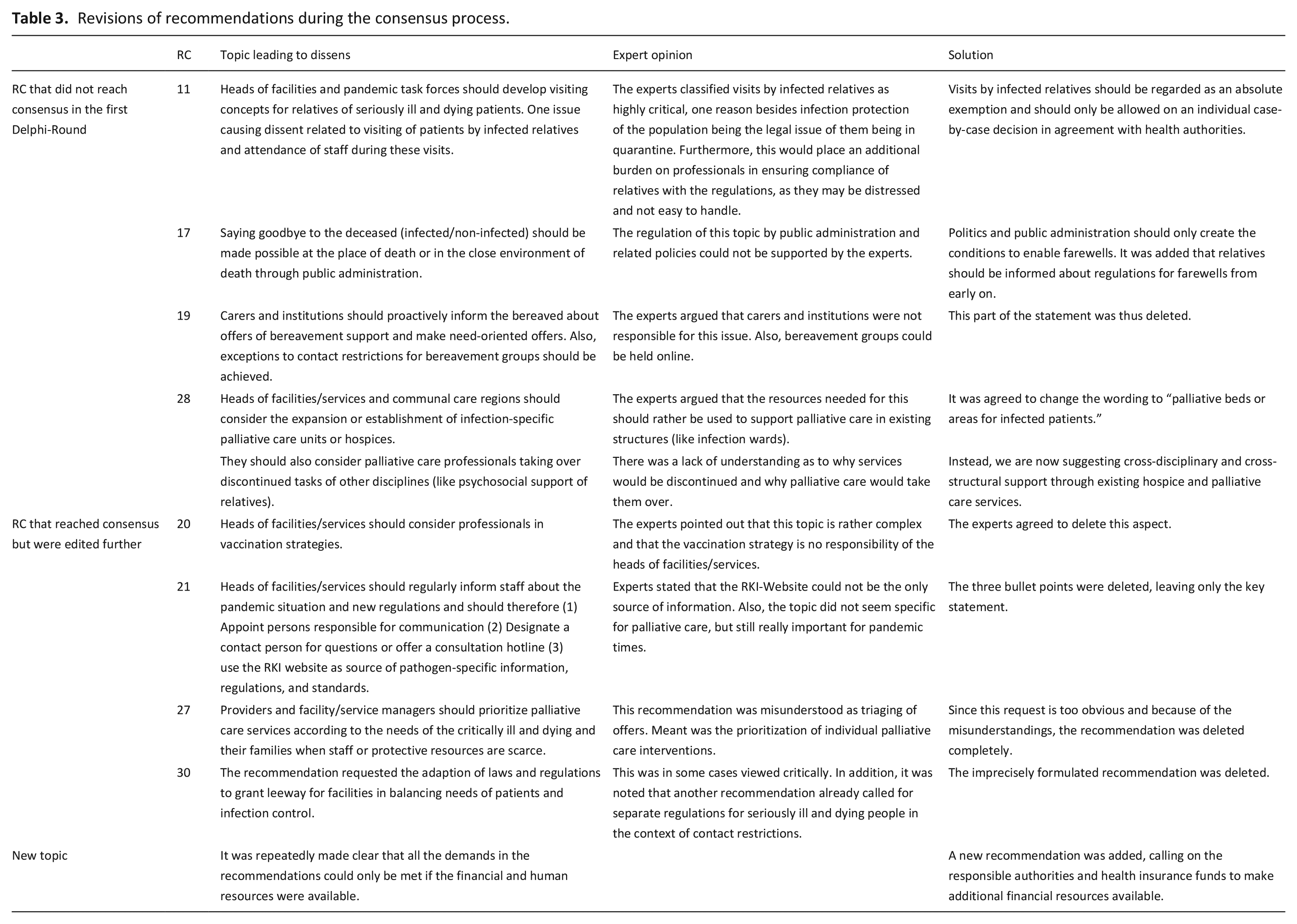
Of 101 statements put to vote, 95 reached consensus. The six statements that were not consented originated from four recommendations (no. 11, 17, 19, 28). Thus, 30 of 34 recommendations reached consensus in the first Delphi round. A total of 979 free text comments were submitted. The four recommendations that did not reach consensus were revised based on the analysis of the free text comments by two members of the research group (AP, STS).
The analysis of the comments on the consented recommendations also led in part to adjustments. In 20/30 consented recommendations some editorial revisions were necessary and six were adopted without further change. The remaining four recommendations (no. 20, 21, 27, 30) were edited further. The content of two recommendations (no. 20, 21) was changed due to discrepancies in the free text comments. Two other consented recommendations (no. 27, 30) were judged to be redundant. Therefore, they were put to vote on deleting them. An additional recommendation was formulated, as a new aspect emerged from the experts’ comments.
Part 2: Workshop
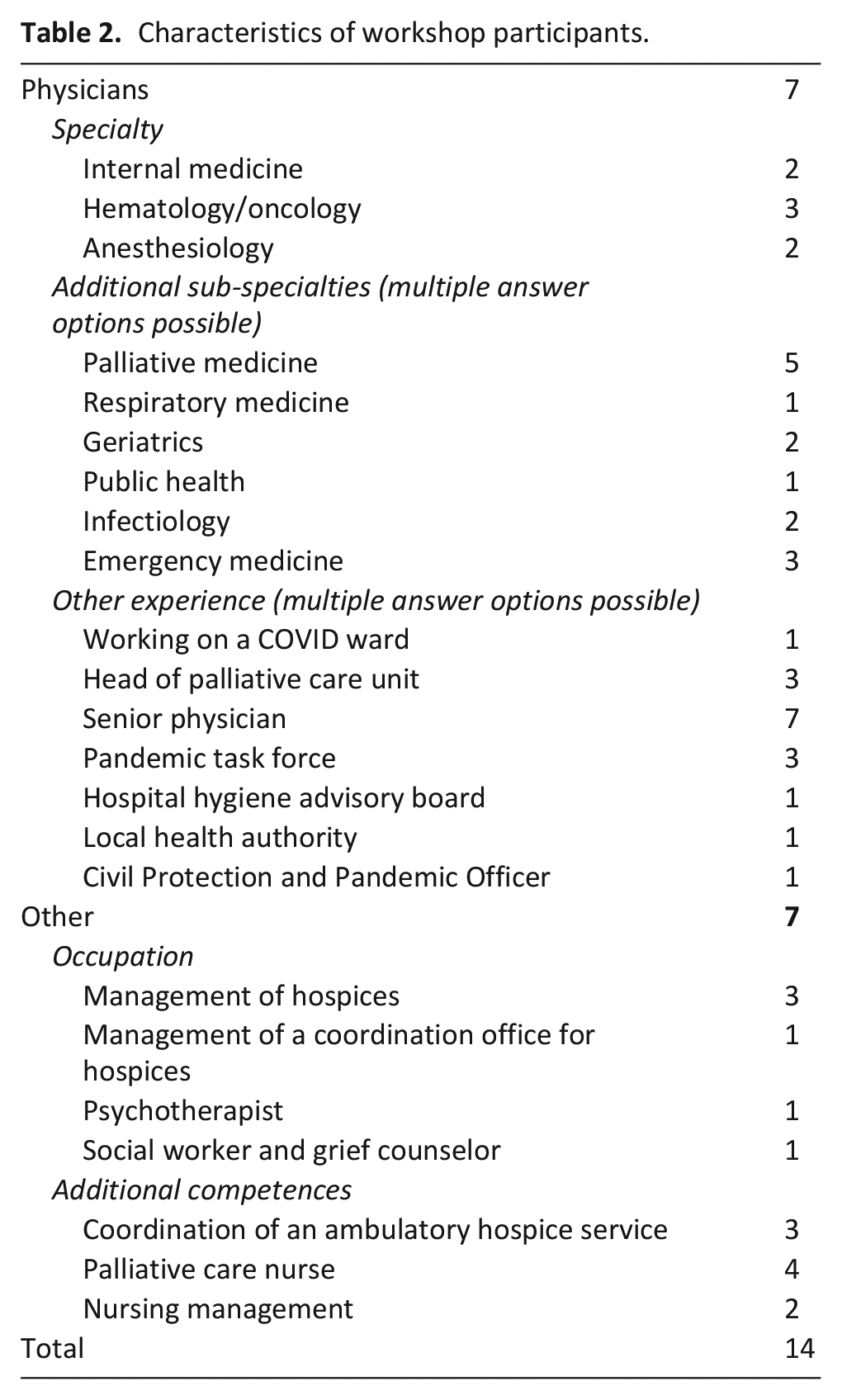
Of 28 experts invited to the workshop, 14 participated. In addition to the experts, the two project leads participated in discussions and voting. The participants were predominantly female (n = 10). The median age of the workshop participants was 53 years (range 50–59 years). The composition of occupations and competences in the workshop is presented in Table 2. Experts represented most settings and competencies, only the macro level was not represented.
Characteristics of workshop participants.
A total of nine recommendations were discussed, revised, and voted on. For seven recommendations, agreement on the wording could be reached. The experts agreed on deleting the two recommendations in question. This decision along with the seven revised recommendations were put to vote for the full expert-panel in the second Delphi round.
Part 3: Second Delphi round
All seven recommendations reached consensus. The experts agreed on the deletion of the two recommendations in question. No new topics or differing views emerged in the free text comments. Thus, the consensus process resulted in 33 consented recommendations for the care of seriously ill and dying individuals and their relatives in pandemics. Figure 1 summarizes the procedure of the consensus process. In Table 3, detailed information about the revisions of the recommendations during the consensus process is presented. Table 4 summarizes the contents of each recommendation, broken down by subchapters. The full recommendations (translated) can be found in the Supplemental Appendix.
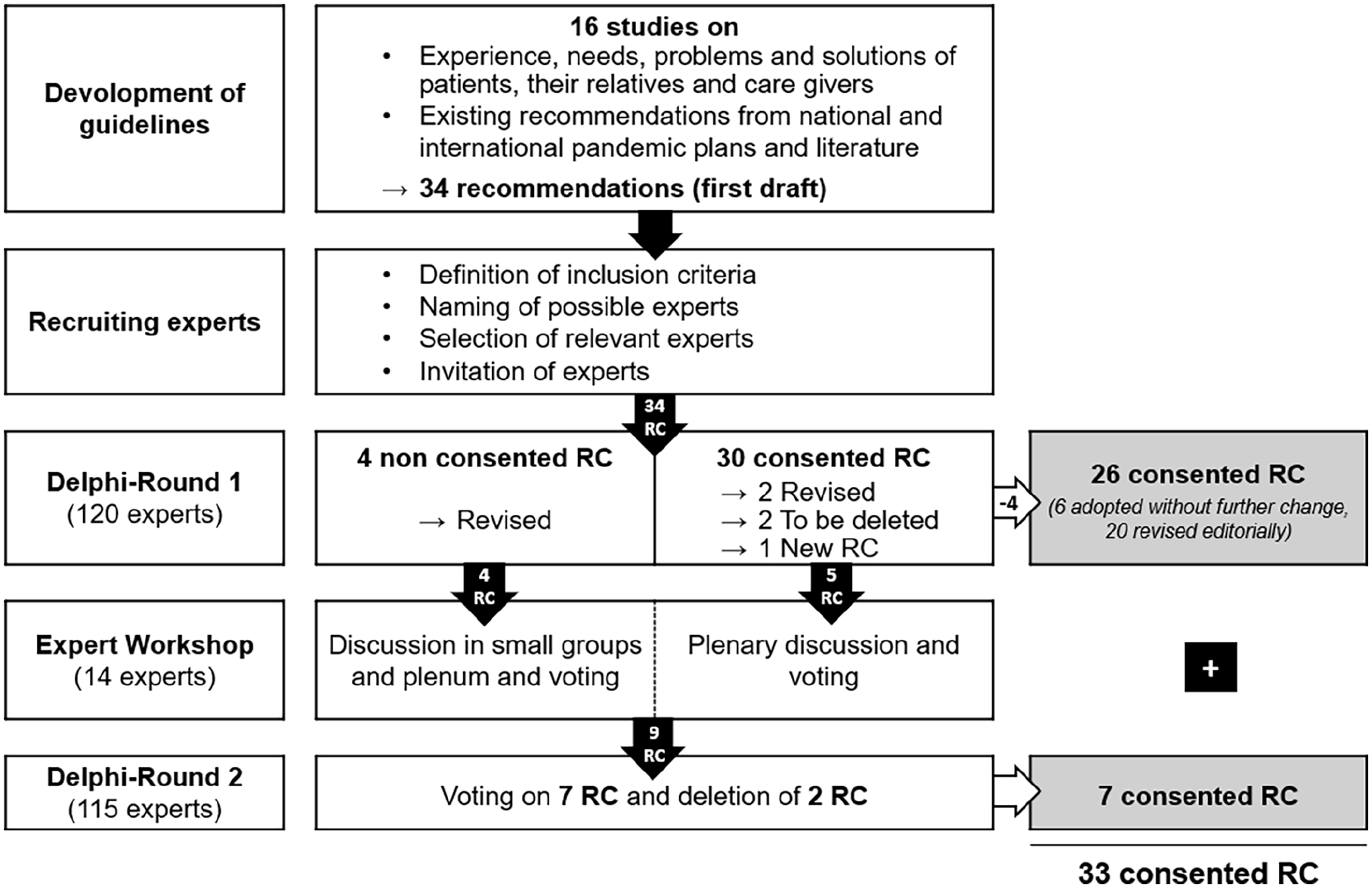
Flowchart of the consensus process (RC equals Recommendations).
Revisions of recommendations during the consensus process.
Summarized content of the recommendations.*
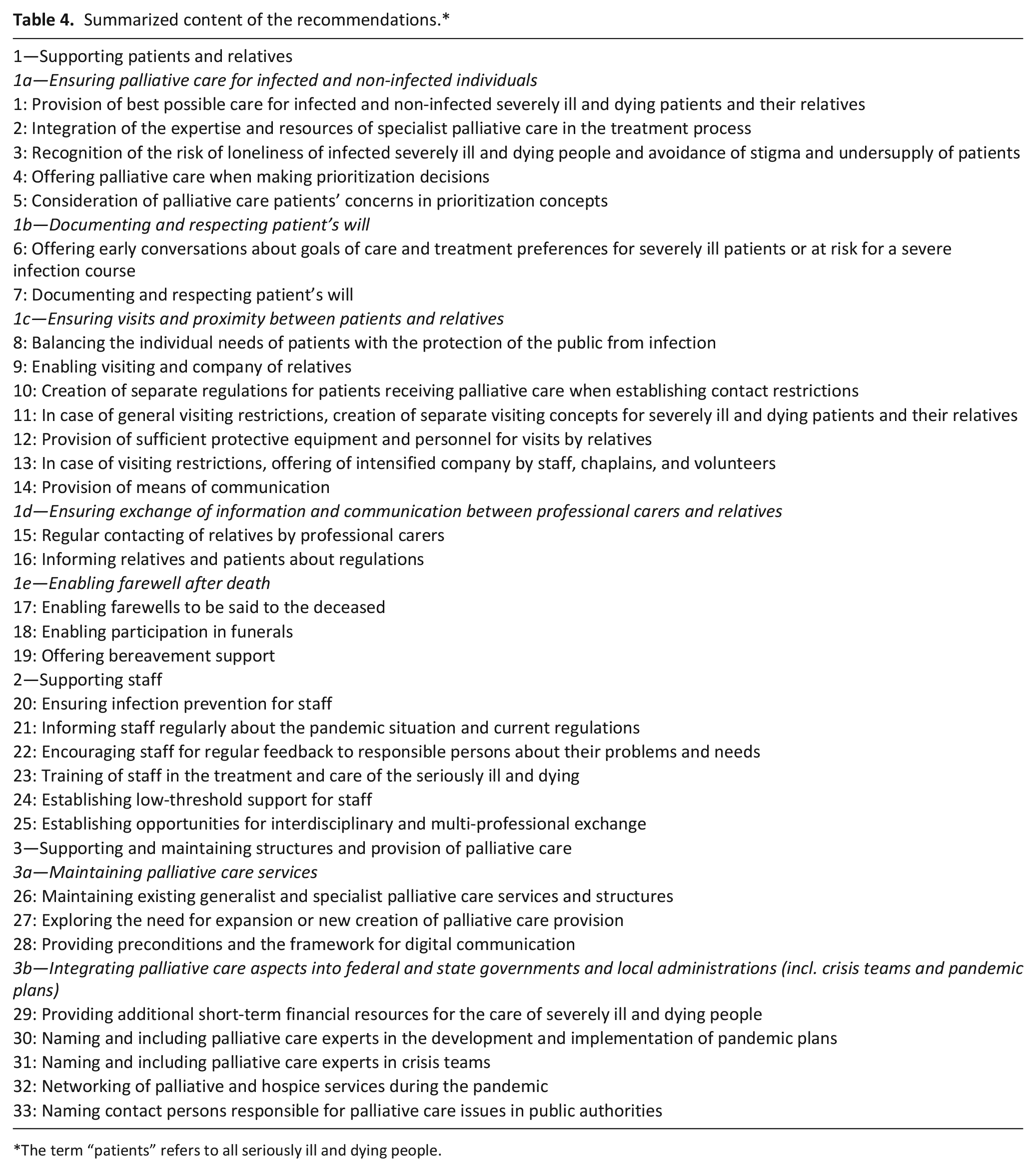
The term “patients” refers to all seriously ill and dying people.
Discussion
We present a national strategy with 33 evidence and consensus-based recommendations for the care of seriously ill and dying people and their relatives in pandemic times. The strategy comprises three chapters on “supporting patients and relatives,” “supporting staff,” and “supporting and maintaining structures and provision of palliative care.” The 33 recommendations are supported by results from related studies, explanatory texts, and best practice examples and are presented on a national website (www.pallpan.de). The final recommendations address the proposed elements (stuff, staff, space, systems) and dimensions (physical, psychological, social, and spiritual suffering) for a palliative care pandemic plan as suggested by Downar and Seccareccia and the WHO.1,25 However, the recommendations follow a different structure to enable clear, user-oriented implementation in practice. It is also important to note that the recommendations compromise general statements, for example about patient care, as well as specific statements, for example for responsible people in pandemic boards. They address various organizational structures and different settings of care provision. Accordingly, some recommendations will apply to only some settings or structures or will apply to them in slightly different ways. This is to be expected and welcomed, given the purpose and form of the recommendations. General recommendations on symptom control were not included in the strategy since we only included pandemic-specific topics. Instead, we refer to existing guidelines for symptom control.26,27
The first chapter of the recommendations relates directly to generalist and specialist palliative care of infected and non-infected people. All patients should receive the best possible palliative care in a pandemic.2,7,25 Palliative care skills can be used to prevent loneliness and stigmatization of patients and provide compassionate care for patients who are at the end of life.1,28
The second chapter addresses the needs of professionals and staff both on information, protective equipment and help in dealing with pandemic related stress and problems.1,29 A system for interdisciplinary consultation and advice to staff should be established so that professionals are given the opportunity to support each other as a team.25,30 Additionally, in a pandemic, all professional caregivers of critically ill and dying people should be supported and trained regarding palliative care measures. Basic palliative care measures such as symptom relief, communication strategies, goal of therapy discussions, and support during bereavement and at the end of life should be taught.1,7,29,31
The third chapter of the strategy aims to support structures for the care of seriously ill and dying people. Hospice and palliative care can contribute to providing holistic care in a pandemic if services are maintained and can operate flexibly. 29 Additionally, palliative care must be available in many different settings, including intensive care units, hospital wards, emergency departments, and long-term care facilities. 7 It must ensure that resources are available to care for the seriously ill and dying with dignity and respect. This results in an obligation for the health care system to provide adequate funding, sufficient trained staff, and equipment.1,29,32 Governments should recognize the essential contribution of palliative care to pandemics and ensure that palliative care is integrated into the health system’s approach to the pandemic.1,33
Although the recommendations are developed for the German health care context, many aspects can be transferred to other countries and health care systems as orientation for future pandemics. Until 2020, the international policy literature mainly focused on palliative care in humanitarian crises1,34 but little was available on palliative care during pandemics. Publications on the actual SARS-CoV-2 pandemic mainly relate to specific aspects of palliative care such as description of the population,35,36 palliative care service activities,29,37,38 symptom management 39 and other topics. However, no national strategy for the care of severely ill and dying people and their relatives in generalist and specialist palliative care as the one presented here was developed up to now. Therefore, the recommendations presented here could serve as a basis for similar strategies and consensus processes in other countries, which then need to be adapted to the respective structures and conditions.
Strengths and limitations
A strength of this study was the use of the Delphi procedure, a scientifically justified formal consensus procedure. By following the RAND/UCLA Appropriateness Method (“RAM”), we used a modified Delphi method that provides panelists with the opportunity to discuss their judgments in an expert workshop between Delphi rounds. 40 The modified Delphi process allowed the inclusion of experts from various backgrounds and structural levels in the consensus process. By following this method, we identified barriers of change and tailored the recommendations accordingly, which makes the successful implementation of the guideline more likely. 41 It also helped us in view of the limited time resources available to speed up the process and publish the national strategy in time of need. These advantages outweigh the problems like missing anonymity in the workshop, possible influence through project leaders, or opinion leadership of individual experts in the expert workshop. The combination of a two-round Delphi process with an expert workshop was the most time-efficient and suitable way to achieve consensus on the recommendations. Using two online surveys and an online meeting, we were able to establish a national cooperation. 42
One possible limitation of the method is the potential bias in selecting experts for the process. 14 To counteract this, criteria and a composition for the recruitment of the experts were defined beforehand. The competencies of the experts sought for the Delphi process and the expert workshop were largely represented. The experts were thus representative of the topic and suitable for the process. However, because of the pandemic it was challenging to recruit sufficient numbers of experts as many of them were heavily involved in patient care and other pandemic-related commitments. The involvement of experts of the PallPan consortium in the Delphi process could be seen as a further limitation. However, it was felt that palliative care expertise and the experience of the whole development process were helpful for the discussion in the workshop. Another potential weakness is the revision of the recommendations based on the assessment of comments in the first Delphi round. To counteract this in the best possible way, two independent researchers familiar with the recommendations undertook the incorporation of comments. A fourth limitation is the limited number of two Delphi rounds. This was due to time restrictions as the funder of the project expected the whole project to be completed in less than 1 year. Being aware of this we chose a modification of the Delphi consensus process and included an expert workshop between the two Delphi rounds following the method of a Group Delphi process. This would allow us to speed up the process and discuss critical issues in the expert group. The results of the workshop were finally addressed in a second Delphi round with the wider group. We believe that this combination of Delphi rounds and expert group discussion resulted in valid recommendations for the national strategy.
Conclusion
The SARS-CoV-2 pandemic constantly impacts on patients’ lives and relationships, threatens their quality of life, and leads to anxiety and uncertainty. The health care system and its policy makers should work side by side with professional carers to provide better care for seriously ill and dying people and their relatives in the current and in further pandemics. 43 We provide a national strategy with 33 recommendations for generalist and specialist palliative care in pandemics in Germany that should be part of overall pandemic plans and thus improve the general pandemic preparedness. It hopefully increases the future palliative care response to a pandemic that nobody suffers mentally, physically, spiritually or socially and most important that nobody must die alone. We hope that our recommendations help professional carers and policy makers and can serve as example for the development of palliative pandemic plans internationally.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221114536 – Supplemental material for Development of a national strategy with recommendations for the care of seriously ill and dying people and their relatives in pandemics: A modified Delphi study
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221114536 for Development of a national strategy with recommendations for the care of seriously ill and dying people and their relatives in pandemics: A modified Delphi study by Sonja Gauder, Anne Pralong, Constanze Rémi, Farina Hodiamont, Isabell Klinger, Maria Heckel, Steffen T Simon and Claudia Bausewein in Palliative Medicine
Footnotes
Acknowledgements
We want to thank the experts and participants of the Delphi study and the expert workshop for their support of the project.
Declaration of conflicting interests
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PallPan project was funded by the German Federal Ministry of Education and Research (BMBF) and is part of the Network University Medicine (NUM) (netzwerk-universitaetsmedizin.de).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.