
Abstract
Background:
During the SARS-CoV-2 pandemic’s initial waves, bans on visiting and isolation measures placed limits on providing services for seriously ill and dying people and their relatives. Pandemic response teams at governmental level (macro), at federal state and municipal level (meso) and in healthcare facilities (micro) played their role in pandemic management procedures.
Aim:
To explore pandemic-related challenges and solutions of pandemic response teams regarding the provision of care to seriously ill and dying people and their relatives. Findings were to be integrated into a national strategy (PallPan).
Design:
Semi-structured expert interviews (10/2020–2/2021) analysed via structured content analysis.
Setting/ Participants:
We interviewed 41 members, who discussed the work of 43 German pandemic response teams (micro n = 23; meso n = 20; no members were available at macro level) from 14 German federal states.
Results:
Twenty-nine of 43 teams took account of the needs of seriously ill and dying. Their main challenges resulted from pandemic-related legal requirements in hospitals and long-term care facilities. The implementation of such was in the remits of the meso level. Dysfunctional or non-existent communication between the levels was reported to be challenging. To foster patient-related solutions the micro level pandemic response teams supported individual decisions to enable patient-relative contact for example, visiting and saying goodbye outside, meeting via digital solutions.
Conclusions:
Pandemic response teams evidently struggled to find appropriate solutions to ease pandemic-related impact on the care of seriously ill and dying patients and their relatives. We recommend bringing palliative care expertise on board.
When it first emerged, the SARS-CoV-2 pandemic was an unprecedented situation that required an immediate response.
Germany’s public sector has various organisational structures for responding nationally and locally to critical situations such as pandemics.
Analysis if and how pandemic management procedures engage to maintain the provision of care to seriously ill and dying and their relatives in pandemics.
Indications of instances in which the care for seriously ill and dying risks being treated as secondary to other pandemic-related challenges or in which pandemic management fails to take this group into account.
Examples of action taken by pandemic response teams to facilitate and maintain care for seriously ill and dying and relatives during the SARS-CoV-2 pandemic.
Implications for practice, theory or policy.
Pandemic preparedness strategies should include improved infrastructure for communication among the national, federal and community administrative levels and the healthcare facilities delivering end of life care. Specific named contacts for activities related to caring for seriously ill and dying patients should be available at all levels.
End of life care and palliative care expertise should be on board during the design of pandemic plans and action to be taken by pandemic response teams.
Background
The SARS-CoV-2 (severe acute respiratory syndrome coronavirus type 2) pandemic has created a substantial burden on healthcare systems worldwide since the disease associated with the virus, COVID-19, first appeared in December 2019 and particularly since the World Health Organization (WHO) declared a pandemic on 11 March 2020. WHO recommended strict infection control measures and physical distancing (often known as ‘social distancing’) to prevent the further spread of the infection. 1 Numerous countries imposed several periods of lockdown to the end of safeguarding the capacity of health systems to care for patients severely affected by COVID-19 and the provision of essential health services to patients with other complaints. 2
It is vital to public health that continuous high-quality care for patients approaching or at the end of their lives – with and without COVID-19 – and support for their relatives remain available.3,4 This is particularly true for pandemic situations that increase palliative care needs due to increasing mortality and COVID-19 symptoms. 5 The focus of palliative care is on quality of life, pain and symptom control, advance care planning and support for patients’ relatives and those bereaved. 6 The bans on visiting and isolation measures imposed in response to the COVID-19 pandemic limit the quality of the care for seriously ill and dying.7,8 Several services and professional associations responded rapidly and provided recommendations on palliative care measures and care pathways,9 –11 other recommendations on patient care under pandemic conditions tended to neglect key issues of palliative care.7,12,13
In Germany, pandemic management is covered by the prevailing federal political system, where centralised and decentralised administrative structures exist alongside one another. 14 To provide support to general operational crisis structures, additional pandemic response teams emerged in responding to the emergency, mainly at federal state and municipal levels (meso) and in healthcare facilities (micro level). Pandemic response teams have taken a prominent role in pandemic management in Germany, covering the coordination and implementation of public infection control measures and the provision of information. Nevertheless, it was unknown whether pandemic response team members determined the provision of care to seriously ill and dying to be among their remits and took a role upon it and if so, the challenges and solutions found on varying levels of scale.
Aim
This article aims to describe whether and in which way the provision of care to seriously ill and dying people and their relatives was determined within pandemic response teams to be part of their remits and to explore their challenges and solutions. Findings were to be integrated into a national strategy on care of seriously ill and dying people and their relatives in pandemics (PallPan).
Methods
Design
The study is part of the PallPan project run by the Netzwerk Universitätsmedizin (NUM; University Medicine Network) to the end of creating a national strategy on palliative care in pandemic conditions. 15 Due to the need for the rapid development of recommendations applicable to and usable in the current pandemic, the project was ‘fast-tracked’ and took place over a duration of 8 months. The study’s research design, encompassing semi-structured interviews and qualitative content analysis met the need to explore an unprecedented pandemic situation and the complex public health and healthcare challenges to which it gave rise. We drew on a constructivist research paradigm 16 assuming that gaining insights into the actual pandemic management regarding the seriously ill and dying and their families might be given by people involved who made subjective meaning of their experiences during their tasks performed. Reporting is in line with the COREQ reporting guidelines for qualitative studies. 17 Registered Trial: DRKS00025013 and part of the PallPan project (BMBF grant no. 01KX2021)
Setting
We studied pandemic response teams as key instruments of pandemic management at varying levels of scale.
Recruiting strategy
Germany has neither a formal definition of a pandemic response team nor an official overview or list of those in operation. We therefore employed multiple methods for recruiting participants: (a) asking the members of the PallPan consortium to put us in touch with potential participants; (b) contacting, by email, administrative authorities in all German cities with populations of over 100,000 and those in the two most populous administrative districts of each German federal state; (c) internet searches using key terms such as ‘pandemic response team’, ‘COVID-19 task force’, ‘crisis teams’ and ‘health services’.
Those participants included in the study were adults (aged ⩾18 years) involved in pandemic management as a staff member attached to a healthcare facility or public (administrative or legislative) institution responsible for healthcare issues. Exclusion criteria were age under 18 years or involvement exclusively in a non-healthcare-related aspect of pandemic management.
Sampling
When selecting participants for inclusion in the study, we paid conscious attention to variables such as the region in which they worked (population density), the incidence of SARS-CoV-2 infection in that region, their occupational background, their workplace and the level (micro, meso, macro) at which they were involved in pandemic management activities. We prioritised the inclusion of those working in areas with a high incidence (at least 14 consecutive days of over 50 new infections per 100,000 inhabitants over the previous 7 days, between the months of March and October), due to our assumption that pandemic management in high-incidence areas might be better-equipped and its actors more experienced. This notwithstanding, we included some participants working in low-incidence areas for comparison and contrast purposes.
Data collection
We conducted semi-structured expert interviews by video call or telephone between October 2020 and February 2021. The interviewers received training beforehand and were Ursula Kriesen (UK), medical doctor; Maria Heckel (MH), nursing researcher and social worker; Isabell Klinger (IK), research associate; Sophie Shahda (SoSa), student of medical process management; Carolin Schneider (CS), research nurse; and Silke Stellmacher-Kaiser (SSk), study documentation coordinator. The interview guide covered among others: personal and job-related information pertaining to the participants; the pandemic response team’s activities and activities of the participants around care of seriously ill and dying patients during pandemic restrictions; and care of bereaved family members. No definition of palliative or end of life care was given during the interview.
All participants gave written informed consent to take part in the study. Few interviewers and participants knew each other from occupational context, most of them had no relationship established prior to study commencement. The study received approval from the relevant local ethics committees on 10 July 2020 (Erlangen, 397_20 B; Rostock, A-2020-0226).
Data analysis
Interviews were audio-recorded and transcribed verbatim. 18 We used MAXQDA 2020 (release 20.04.0) 19 for data processing and analysis. The unit of analysis chosen was passages of text from one participant referring to one pandemic response team, as three participants discussed their involvement in two different pandemic response teams each and two participants reported on their work on the same pandemic response team.
We conducted qualitative content analysis, a qualitatively orientated category based text analysis as proposed by Mayring. 20 The interviews were coded deductively to pre-defined nominal categories formed in accordance with our research questions and the interview guide. For intersubjective comprehensibility and transparency, we documented our defined rules for coding, adjustments that had emerged as necessary, and decisions for further coding processes in memos as well as using MAXQDA’s logbook feature.
After piloting, interviews were coded deductively (MH, IK, SoSa) using the structure of categories as defined. We supplemented these with inductively formed categories such as ‘understanding of palliative care’ and ‘role of local public health authorities’ (see Table 1). We tested inter-code agreement to assure quality and to prevent subjectivity bias. Consistency checks on coded interviews reviewed the consistency of codings and distinctions between the categories. We revised categories and codings after each round of checks. The final stage of analysis entailed summarisation of the codings in the various categories and subcategories, using MAXQDA’s summary features, and the establishment of interconnections among the codings to the end of answering our research questions. The analysis paid particular attention to differences emerging between statements pertaining to the meso and micro levels of pandemic response team operation, due to their correlation with different responsibilities, powers and areas of application.
Overall category system (main categories and fist level of sub-categories).
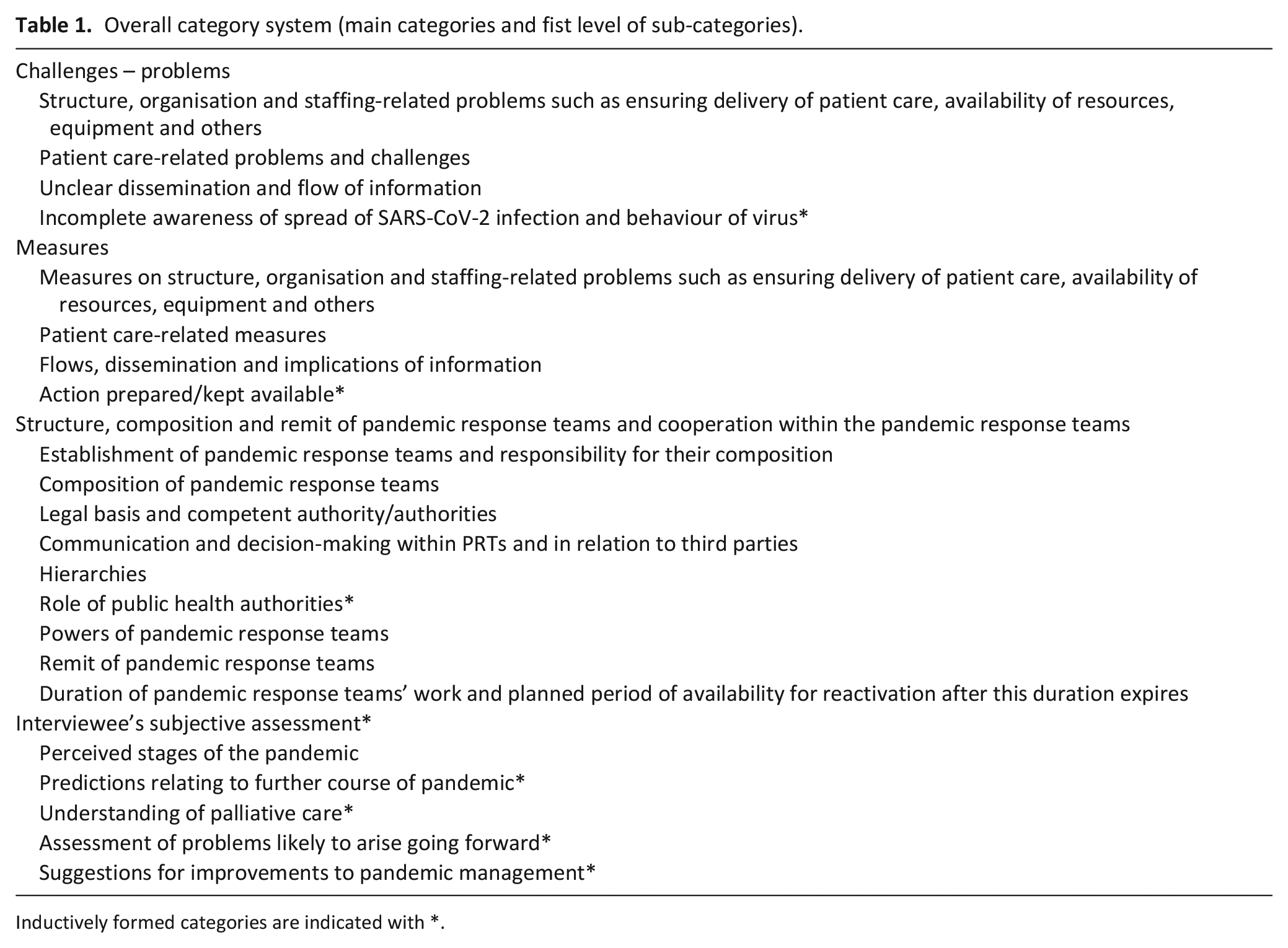
Inductively formed categories are indicated with *.
Results
Members of the PallPan consortium nominated 20 potential participants, of whom 11 took part in the study. We contacted 103 local administrative authorities (first round of recruitment: 2 October 2020, second round: 9 November 2020) by email; four suggested a potential participant. The internet searches between 22 October 2020 and 15 January 2021 identified 100 individuals, of whom 27 took part. We did not systematically record people’s reasons for declining to take part; those with whom we spoke directly mostly cited a lack of time or interest.
Study population
Finally, 41 members of pandemic response teams took part in the study (40 per video call, 1 per phone) and reported on 43 response teams instituted by public administration (n = 20) on meso level, and n = 23 instituted by healthcare facilities/services (micro level). Members of pandemic response teams on macro level were not available. The average age of participants (n = 41) was 49.9 years (SD: 9.19)). Most (90.2%) held management positions in their organisations or institutions. Their professional backgrounds were largely in the fields of healthcare and civil protection. Table 2 provides an overview of participants’ demographic and job-related characteristics.
Characteristics of participants (n = 41).
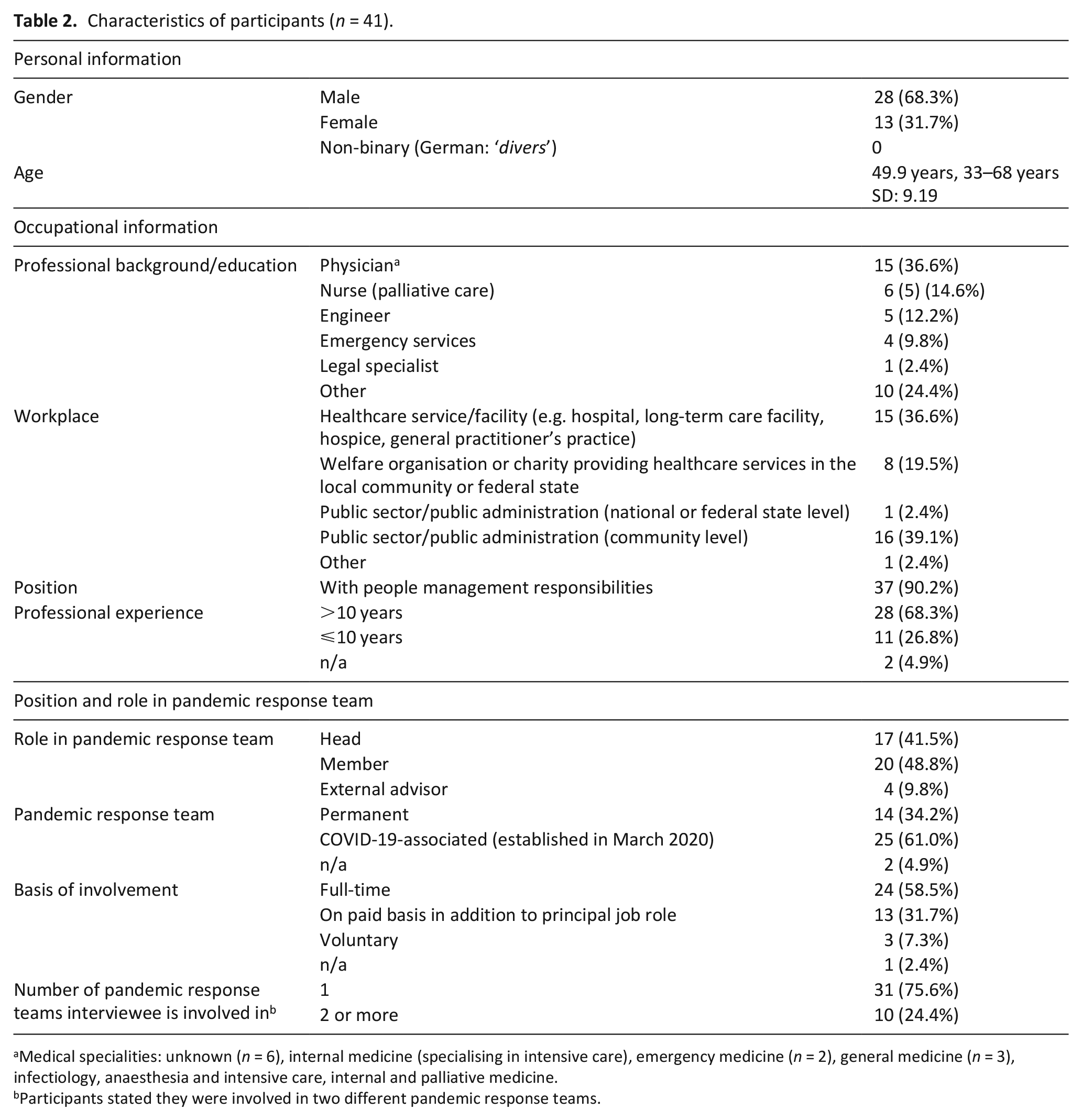
Medical specialities: unknown (n = 6), internal medicine (specialising in intensive care), emergency medicine (n = 2), general medicine (n = 3), infectiology, anaesthesia and intensive care, internal and palliative medicine.
Participants stated they were involved in two different pandemic response teams.
Examined pandemic response teams according to levels of scale and other characteristics
The study covered roughly equal numbers of pandemic response teams at the micro (n = 23) and meso (n = 20) levels, based in a total of 14 federal states. At the micro level, there was less of a balance in evidence with regard to the type of healthcare service or facility for which the participants worked (inpatient, n = 19; home care, n = 9) and the bodies by which facilities were run (charity, n = 7; publicly-managed, n = 11; or privately-managed services, n = 5; see supplemental appendix). Few of the meso level pandemic response teams represented were based in rural areas (n = 3). Most were in regions with a high incidence of COVID-19; for comparison and contrast purposes, we included three meso level and four micro level teams in low-incidence areas. Members of 22 pandemic response teams reported that their team had one or more experts for the care of the terminally ill and dying, mostly named ‘palliative care experts’ as permanent members; this was most frequently the case at the micro level (n = 13), and less so at the meso level (n = 9). Another six interviewees said their pandemic response teams consulted experts as the need arose (micro: n = 5, meso: n = 1). The definition of ‘palliative care experts’ by the interviewees for these purposes encompasses palliative care nurses, palliative care physicians, anaesthetists, gastroenterologists, nurses, general practitioners, members of ethics committees and chaplains/pastoral support workers.
Data collection and analysis
The average duration of the interviews was 35.73 min (SD 15.17), with a minimum of 10 and a maximum of 70 min. Interviewees were asked to respond on the basis of the period between March 2020 and the date of their interview.
Findings
Members of 20 pandemic response teams reported that their teams took specific action in terms of the provision of care to seriously ill, dying and their families. We define ‘specific action’ as a conscious awareness and active consideration of the issues and pandemic-related difficulties facing seriously ill, dying and their families, and a clear intention to mitigate this situation. In a further nine pandemic response teams, the care situation of seriously ill and dying patients and families came under consideration but did not result in specific action. Fourteen pandemic response teams did not discuss the situation of seriously ill and dying patients and families.
Foci and priorities of pandemic response teams at the outset of the pandemic: A meso level perspective of challenges
Participants active in meso level pandemic response teams reported a predominant focus on securing the provision of acute and emergency care in hospitals and protecting users of long-term care. Pandemic response team members in some regions described a situation in which services such as palliative care units and long-term care facilities fell below the radar of the pandemic response teams.
Infection control measures as top priority
At the outset of the pandemic, some pandemic response teams did not initially consider issues relating to the care for seriously ill and dying patients and families. All participants reported that compliance with infection control measures had been a top priority at this stage. Particularly during the first wave of infections, palliative care facilities were subject to official orders regarding isolation, quarantine and bans on visiting.
The example of visiting bans in elderly care facilities. [. . .] where people were already very old, sometimes also seriously ill in addition to their age. They were perceived as dying, although of course one only knows afterwards when the dying phase took place. [. . .] And suddenly it was politically decreed that these people could no longer receive visitors. (ID_A, pos. 19)
Participants cited the initial uncertainty among experts around the transmission of SARS-CoV-2 as a reason for this. Long-term elderly care facilities in particular implemented the restrictions robustly to protect their vulnerable residents, whose wishes were often secondary to protective measures.
Yes, the elderly homes were the focus [. . .]. At the beginning, the main issue was safety in the old elderly homes and protective equipment. The issue of social life did not play a role. (ID_Bb, pos. 37)
Participants reported instances of palliative care patients who had tested positive for COVID-19 who were not in hospices but in hospital isolation wards. Others experienced patients who had recovered from COVID-19 and could have been discharged from hospital not being permitted to return to their long-term care facility.
Caring of the deceased exclusively discussed with regard to minimising transmission risks
Discussion in the pandemic response teams of issues around the management of deceased individuals took place in relation to ‘infection-related restrictions’. Questions were raised about the capacity for cold storage and burial (body bags, crematoria) and the risk of transmission from handling bodies. Pandemic response teams at meso level received feedback from care providers and relatives that stressed the importance of end-of-life care as a service and criticised a lack of consideration for families’ needs to personally care for their dying loved ones or to say goodbye in accordance with cultural customs. Support services for bereaved people were barely in operation at this time, and open-casket farewells and burials in individuals’ countries of origin were not possible.
Structural requirements and responsibilities
Pandemic response team members working in civil protection emphasised the existence in Germany of sufficient crisis management resources (emergency services, patient transport services, religious organisations, bereavement support groups, volunteers, police, armed forces) to manage the needs of seriously ill and dying people and their families, which they felt were not deployed effectively enough during the pandemic’s initial stages.
After the first wave, the provision of care to seriously ill and dying was increasingly determined to be in the remits of pandemic management services at meso level, a development advanced by the official designation of hospices, funeral directors and support services for bereaved people, and staff in these areas, as essential services/‘key workers’ (German: ‘systemrelevant’).
Balancing infection control and care needs: A micro level view on challenges
Participants at the micro level reported fears of staff shortages and a need for the setting of priorities, accompanied by the closure of hospital wards, including palliative care units, to release staff. Some hospital pandemic response teams restricted patient transfers between wards and the activities of inpatient palliative care support teams. Interviewees spoke of severe emotional strain on patients and families, increased staff workloads, and a reduced quality of care due to strict visiting bans for relatives, volunteers and chaplains:
The relatives were only allowed to come on a limited basis, the volunteers
weren’t coming at all any more [. . .] the quality of support was different, it was no longer about what was the best we could do for each resident. (ID_S, pos. 23)
Challenges on ensuring safety for visitors and defining exceptions
Participants reported a lack of resources for visitors, such as rapid tests. Hospices in particular missed out in this regard, as they did not receive any funding from federal government support funds. In some cases, palliative care units were able to make exceptions to visiting bans for relatives of dying patients. Patients receiving specialist palliative care and people dying on other wards (intensive care, acute care) were not considered for exceptions. Setting rules for exceptions and defining who was at the imminent end of life proved a challenge to pandemic response teams. Some instances of conflict with families arose; palliative care and hospice staff struggled to reconcile their own ideals regarding care of the dying with the prevailing circumstances.
This was a great strain on the staff because this had never been the way we had done things in hospice work, and because supporting relatives is one of the key aspects of our work and because, of course, it
doesn’t pass the people we care for by when their relatives can no longer visit like they used to. (ID_S, pos. 21)
The restrictions inspired fears of dying alone in residents of long-term care facilities and people living alone with care support needs.
At one point we had an emergency intervention, an old lady died by suicide and she had all the articles about Covid and the situation in the nursing homes [. . .] spread out on the table. So there was a good deal of fear in the population, yes, but we could never really respond to it. (ID_G, pos. 25)
Particular challenges for long-term care facilities to comply with regulations
Pandemic response team members associated with long-term care facilities noted that some proposals for isolation, such as cohorting COVID-19 patients, were inappropriate. Cohorting would mean taking residents from their familiar surroundings and regular staff, which would, suggested interviewees, have been difficult particularly for cognitively impaired patients such as those with dementia. Participants felt this would have caused an imbalance between infection control on the one side and quality of life and residents’ wishes on the other and that it would have represented a substantial restriction on patients’ liberty and self-determination.
The RKI [Robert Koch Institute] recommendations in the spring [of 2020] were that cohorting was proposed [. . .] And cohorting would mean that I say, for example, residents’ area 1 is our Covid area. [. . .] From a purely infection-centred point of view, this would make sense for us, but it makes no sense at all from a social point of view. Because residents are taken out of their rooms and put with others they don’t know, with staff they might not know, and that’s why we don’t do it. (ID_Bb, pos. 85)
Rather than cohorting, some long-term care facilities preferred admission to hospital for SARS-CoV-2-positive residents:
We [. . .] prefer to send people to hospital than to put them in a room here where they don’t
know anyone. Because the hospital situation, especially for older people, is different from the care home situation. The care home is where they live; in the hospital they know, here
I’m ill, here there are other rules, here I’m
not at home. (ID_Bb, pos. 87)
On the other side some pandemic response teams faced challenges by the tendency of some healthcare facilities to require prioritisation of outpatient care over hospital admission and to take decisions using inappropriate categories such as age.
Hindered final farewell and taking care of the final things
Most participants reported the impossibility of enabling families to say final farewells in a setting that preserved dignity. A small number of interviewees said that two relatives were allowed in the patient’s room to say their goodbyes; in all other cases, staff members accompanied the dying. If they needed to speak to families in person, they found themselves compelled to do so in inappropriate settings, such as outside the entrance to the building or in the car park. Family members sometimes had to speak with insufficiently trained staff recruited from other areas of the facility. In some cases, bereavement support effectively stopped completely. Other challenges included the closure of rooms dedicated to family farewells and the lack of opportunity for a religious minister to attend the patient to bless them or perform other end-of-life rituals. Although the rooms in some facilities reopened in the course of time, final goodbyes took place with physical distancing, personal protective equipment and restricted numbers. Few funeral services were conducted outdoors.
The handling of administrative issues and enquiries from relatives had to take place by telephone. Some interviewees reported that deceased people’s possessions were placed outside the home for relatives to collect:
Normally, when someone passes away, the relative can go into the home and pick up the [resident’s] personal belongings. Of course, this was no longer possible. [. . .]. Unfortunately, the janitor had to put their furniture outside by the door to be picked up. Or how do I deal with official matters? [. . .] Then we stated quite clearly: No, they can’t go to the office in person. It has to be done by phone. (ID_B, pos. 56)
Solutions regarding the provision of care to seriously ill and dying and families Creating necessary conditions for patient-related measures: A meso level view on solutions
Some meso level institutions reported that they have created the necessary conditions and initiated the implementation of measures at the micro level. Those pandemic response teams and health authorities that were less restrictive tried to tackle the problem of end-of-life visits in the first wave of the pandemic. All this notwithstanding, some pandemic response teams and public health authorities whose practices were less restrictive sought to tackle the issue of visits for people at the end of life as early as the pandemic’s initial wave. Healthcare facilities received exceptions from visiting bans for family members and pandemic response teams were encouraged to pursue individually designed solutions for communication with relatives (open windows, phone calls). Meso level pandemic response teams cited legal provisions for visits, under strict infection control measures, to people whose end of life was imminent. Some pandemic response teams informed healthcare services and facilities about the importance of advance care planning documents; some mediated between long-term care facilities and hospitals to resolve re-admission challenges for patients recovered from COVID-19.
We have always issued explanations of the current rules to hospices [and] outpatient palliative care providers. (ID_Aa, pos. 35)
Implementation of patient-related measures: A micro level view on solutions
Mostly micro level pandemic response teams reported on concrete solutions and measures to support seriously ill and dying and their families.
Enabling in-person or digital contact between patient and next of kin
During the visiting bans in the first wave, micro level pandemic response teams made use of ‘grey areas’ within national and regional regulations to enable in-person contact between patients/residents and their families. Facilities set up outdoor visiting areas such as tents in their gardens and chairs separated by plexiglass sheets in outside areas, so that patients could meet with family members wearing personal protective equipment and observing physical distancing.
The result in the summer [of 2020] was, for example, that we fenced in all our buildings with construction fences and created visiting spaces in the outdoor areas. We had folding outdoor tables and benches because they were long enough. The relative and the person being cared for sat at the heads of the tables. There was a plexiglass pane in the middle, so they could meet. This meant the visitors
didn’t have to go into the building, [it] minimise[d] the risk of infection, and the residents could still see their relatives as far as the situation allowed. (ID_Bb, pos. 37)
Facilities promoted contact by phone and using digital solutions such as tablets. However, digital communication options, where they exist, cannot sufficiently ease the situation for elderly and dying patients with cognitive difficulties.
Justifying and defining exceptions of visiting bans for the families of the dying, cooperating services and volunteers
Pandemic response teams of hospitals and other healthcare services designed plans to enable visits for terminally ill patients and those at the imminent end of life. Visits under these conditions entailed, for example, limits to one person at a time for 1 hour a day, under rigorous infection control precautions, with the visitor required to register in advance. One pandemic response team reported extensions to visiting hours and easier registration for visits over the Christmas period. Another participant described exceptions to the requirement to wear a mask during physical contact if patients and relatives hugged without speaking.
Hospice services drew up individualised access regulations with cooperating services. Hospices and palliative care services contacted local health authorities, national and regional government ministries of health and social affairs, and other bodies to protest the absolute nature of visiting bans, with the result that the authorities instituted official exceptions from the bans for patients at the end of life:
That was a [. . .] very important message - including from us – to the politicians, that we said we had to find a way of managing this, and relatively quickly the ban on visits for dying people was actually lifted. So regulations for visits were introduced, with all infection control measures observed. (ID_A, pos. 19)
The degrees of access granted to chaplains and spiritual supporters, ministers of religion, volunteers and providers of additional therapies (physiotherapy, music therapy) varied among facilities. Pandemic response teams sought solutions in instances of ‘psychosocial hardship’:
Then in the care facilities, [it was established] that cases of psychosocial hardship can also be counted in addition to the regular two visitors. That at the end-of-life stage you can come to a hospice untested if
you’re told at 10 p.m. that your mother is dying now. (ID_Cc, pos. 32)
Pandemic response team members reported that in some hospitals, particular units were allowed to take decisions on relaxations of visiting bans for patients in end-of-life care on a case-by-case basis.
Facilitating advanced care planning
In some instances, intensive care units had ‘non-COVID-19’ and ‘COVID-19’ areas in order to facilitate relatives’ access for visits and meetings on matters such as shared decision-making. Discussions at an early stage between physicians, patients and relatives about what is to happen if the infection takes a severe course, and assessment and recording of patients’ wishes in this context, have increasingly become part of clinical routines in these settings. Pandemic response teams provided guidelines to facilitate advance care planning, drew up factsheets on powers of attorney and advance decisions (‘living wills’) for patients, residents and their families, and set up hotlines and regular contact hours for enquiries on these issues.
Discussion
Main results
Our results show that the provision of care to seriously ill, dying and their families is scarcly considered in meso level pandemic response teams. Albeit micro level pandemic response tended stronger to determine this to be in their remits. Those pandemic response teams and local health authorities in Germany who considered the issues faced challenges resulting from pandemic-related measures in hospitals and long-term care facilities, such as isolation and visiting bans, dysfunctional or non-existent communication between the pandemic management levels, lack of infrastructure and resource, and staff shortage. Overall changes over time in terms of focus on seriously ill and dying and their families mirror societal and systemic developing responses to the pandemic for example, intensified discussions on acceptable care and mitigable risks involved due to pandemic. Pandemic response teams being sensible for the developments managed to consider the situation of seriously ill, dying and families using strategies such as onboarding palliative care expertise. The extent to which the required expertise is in place depends on the personal preferences of the individual tasked with establishing the pandemic response team in each case. Whether and which expertise is considered for the care of seriously ill and dying in pandemic response teams reveals varying understanding of ‘palliative care’. Considering the German health care context, each facility who cares for patients until their death for example, long-term care facilities for the elderly, acute hospital wards provides general palliative care. Specialised palliative care includes facilities and services who exclusively care for the seriously ill and dying for example, palliative care units, inpatient hospices and specialised palliative home care teams. In most instances, there is no designation of a functional role on palliative care within the pandemic response team; instead, an individual who, more or less by chance, has a degree of experience in this field will take on the task. The definition of palliative care expertise in some pandemic response teams was rather broad and not all of them were trained specialist palliative care experts.
Strengths and limitations of the study
One of the study’s strengths is its focus on the structural conditions of palliative care delivery in a pandemic situation. Its incorporation of micro and meso level activities provides valuable insights into the interfaces between administrative levels. An open constructivist approach without predefining needs of and care for seriously ill, dying and their families revealed varying understandings and a lack of knowledge and allowed to identify information on the topic even if it is not labelled as ‘palliative care’.
The dynamic pandemic situation and the short timeframe of the study (fast track) prevented the inclusion of pandemic response team members at macro level and this viewpoint was not represented in the interviews. As a substitute one person counselling a macro level pandemic response team and active in health policies had been interviewed, the interview was not part of the analysis but served for insights to the macro level for the authors. Purposeful sampling enabled us to cover views from most German federal states, regions with various population densities, varying incidence rates of SARS-CoV-2, and meso and micro level. The number of participants from pandemic response teams based in rural areas was low, as many small towns do not have an official pandemic response team. Despite the careful sampling, the generalisability is limited. The constructivist approach leaned on for data collecting, the focus of data analysis was on structural aspects of pandemic management and deductive data collection focussed on structures, challenges and solutions of pandemic response teams to the end of informing the national strategy of structures to be considered and responsible persons to be addressed. We did not predominantly concentrate on exploring construction of meaning structures and their changes influenced by the pandemic in the systemic micro and meso levels that would have required an inductive approach of data analysis and might have revealed different definitions and understanding of care and responsibility as well as care ethics in times of pandemics.
What this study adds
The study identified some best practices, such as providing policymakers with feedback on regulations, networking among facilities providing palliative care and practical support in the relaxation of visiting bans and facilitation of final family goodbyes. Others, such as the CovPall consortium examined how palliative care services and hospices were responding to the COVID-19 pandemic. They found ‘specialist palliative care services have been flexible, highly adaptive and have adopted low-cost solutions’. 21 Greater collaboration between services was suggested. 21 In our own study group (PallPan) responses to pandemic situation from different kinds of services and patient and family experiences were explored in detail.22,23 Distinct from those approaches our study aimed to explore the organisational context of pandemic management and connections of levels rather than how services respond, we were interested in the pandemic management itself. Nevertheless, findings indicate that pandemic management in Germany leaves the concrete performing and therefore the response to pandemic with the healthcare services and facilities’ pandemic response teams. A more explicit definition of the scope and officially pre-determined remits referring to end-of-life care were missing so far. This claim is now integrated in the national strategy (PallPan) to foster better care for the seriously ill a dying in future pandemic occasions. The advantage might be the possibility to act flexibly, the shortcoming lays in parallel efforts of different services all over the country and lacking support concerning infrastructure and information from higher levels. 15
We found a notable lack of consideration of palliative care issues in the pandemic response, across the meso and micro levels. International literature is indicative of similar states of affairs in other countries.8,13,24 The study evidences barriers to bespoke solutions for the issues arising for patients at the end of life where the administrative level fails to designate individuals as having responsibility for this vulnerable group of patients and where pandemic response teams fail to incorporate trained specialist palliative care expertise, particularly at regional level. Several international palliative care stakeholders have noted the relevance of general and specialist palliative care to pandemic response and recommend the active engagement of palliative care experts in pandemic response action.3,4,23 Challenges to pandemic response teams in the area of palliative care arise in part from the dynamic pandemic situation, which involves a rapidly changing flow of information and entails a need to adapt at short notice.24,26,27 Our findings reveal missing pre-determined remits and a lack of clarity in communication structures between the macro, meso and micro level and in pandemic response teams’ efforts to structure and share incoming information with relevant groups. In Germany, federalistic governmental structures contributed to complexities in pandemic management, yet also aided flexible responses in accordance with regional variations in the incidence of SARS-CoV-2. Therefore, the findings of our study informed the development of a German national pandemic response strategy for palliative care 15 and will hopefully help to ensure pandemic preparedness in defining national planning and needs for action to the end of maintaining the delivery of appropriate palliative care.
Conclusion
Our findings suggest that for the most part, pandemic response teams treated patients’ end-of-life care needs as secondary to other challenges of the pandemic situation or left them out of their considerations entirely. Pandemic response teams, depending on their members’ professional backgrounds and thematic priorities, provide awareness of and practical responses to end-of-life care issues. The inclusion of palliative care expertise when creating pandemic plans and when forming pandemic response teams would improve pandemic management and preparedness. Guidelines for end-of-life care in pandemic conditions should address macro, meso and micro level responsibilities and take account of federal structures. A key task in this context is to designate individuals at all levels to cover end-of-life care issues.
Supplemental Material
sj-docx-1-pmj-10.1177_02692163221099114 – Supplemental material for COVID-19: Challenges and solutions for the provision of care to seriously ill and dying people and their relatives during SARS-CoV-2 pandemic – perspectives of pandemic response team members: A qualitative study on the basis of expert interviews (part of PallPan)
Supplemental material, sj-docx-1-pmj-10.1177_02692163221099114 for COVID-19: Challenges and solutions for the provision of care to seriously ill and dying people and their relatives during SARS-CoV-2 pandemic – perspectives of pandemic response team members: A qualitative study on the basis of expert interviews (part of PallPan) by Isabell Klinger, Maria Heckel, Sophie Shahda, Ursula Kriesen, Carolin Schneider, Sandra Kurkowski, Christian Junghanss and Christoph Ostgathe in Palliative Medicine
Supplemental Material
sj-docx-2-pmj-10.1177_02692163221099114 – Supplemental material for COVID-19: Challenges and solutions for the provision of care to seriously ill and dying people and their relatives during SARS-CoV-2 pandemic – perspectives of pandemic response team members: A qualitative study on the basis of expert interviews (part of PallPan)
Supplemental material, sj-docx-2-pmj-10.1177_02692163221099114 for COVID-19: Challenges and solutions for the provision of care to seriously ill and dying people and their relatives during SARS-CoV-2 pandemic – perspectives of pandemic response team members: A qualitative study on the basis of expert interviews (part of PallPan) by Isabell Klinger, Maria Heckel, Sophie Shahda, Ursula Kriesen, Carolin Schneider, Sandra Kurkowski, Christian Junghanss and Christoph Ostgathe in Palliative Medicine
Footnotes
Acknowledgements
The authors extend their thanks to Clarisse Kugler (student) and Beatrice Wahlen (student) for their support with internet and literature searches and recruitment of participants to the study. The present work was performed by Isabell Klinger in partial fulfilment of the requirements for obtaining the degree ‘Dr. rer. biol. Hum’.
Author contributions
Maria Heckel (Dr. phil, Dr. rer. biol. hum., female) contributed substantially to the conception and design of the study and the collection, analysis, and interpretation of data, and drafted the manuscript with Isabell Klinger. She contributed to the funding proposal. Isabell Klinger (MSc, female) contributed substantially to the collection, analysis, and interpretation of data, and drafted the manuscript with Maria Heckel. Sophie Shahda (Student, female) contributed substantially to the collection, analysis, and interpretation of data and critically revised the manuscript for important intellectual content. Ursula Kriesen (MD, female) contributed substantially to the conception and design of the study, the development of the interview guide, and the recruitment of interviewees. Sandra Kurkowski (MSc, female) contributed substantially to the design of the data analysis, and the data analysis (consistency check) and critically revised the manuscript. Christian Junghanss (MD, male) contributed substantially to the conception and design of the study and the recruitment of interviewees. He critically revised the manuscript for important intellectual content. He contributed to the funding proposal. Christoph Ostgathe (MD, male) contributed substantially to the conception of the study and the interpretation of data, and critically revised the manuscript for important intellectual content. He contributed to the funding proposal.
Availability of data and materials
Our data protection information to participants guaranteed their anonymity in any presentation or dissemination of the study’s findings. As the participants’ responses contained detailed information on the pandemic response teams, it is not possible to anonymise data completely. The raw data is therefore unavailable. Please contact the corresponding author with specific enquiries; she may be able, within reason, to extract data relating to specific research questions.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics committee approval and informed consent
All participants received full information about the study and on their right to withdraw consent to take part at any time without giving reasons, and were able to ask questions prior to the interview. All participants gave written informed consent to take part in the study. The study was approved by the local ethics committee on 6 October 2020, Ethics Committee of the Medical Faculty in Erlangen, 397_20 B and the Ethics Committee of Medical Faculty in Rostock, A-2020-0226.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The PallPan project is funded by the German Federal Ministry of Education and Research (BMBF) (01KX2021, NUM COVID-19). Registration: DRKS00025013
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.