
Abstract
Background:
Palliative care is well suited to support patients hospitalized with COVID-19, but integration into care has been variable and generally poor.
Aim:
To understand barriers and facilitators of palliative care integration for hospitalized patients with COVID-19.
Methods:
Internists, Intensivists and palliative care physicians completed semi-structured interviews about their experiences providing care to patients with COVID-19. Results were analysed using thematic analysis.
Results:
Twenty-three physicians (13 specialist palliative care, five intensivists, five general internists) were interviewed; mean ± SD age was 42 ± 11 years and 61% were female. Six thematic categories were described including: patient and family factors, palliative care knowledge, primary provider factors, COVID-19 specific factors, palliative care service factors, and leadership and culture factors. Patient and family factors included patient prognosis, characteristics that implied prognosis (i.e., age, etc.), and goals of care. Palliative care knowledge included confidence in primary palliative care skills, misperception that COVID-19 is not a ‘palliative diagnosis’, and the need to choose quantity or quality of life in COVID-19 management. Primary provider factors included available time, attitude, and reimbursement. COVID-19 specific factors were COVID-19 as an impetus to act, uncertain illness trajectory, treatments and outcomes, and infection control measures. Palliative care service factors were accessibility, adaptability, and previous successful relationships. Leadership and culture factors included government-mandated support, presence at COVID planning tables, and institutional and unit culture.
Conclusion:
The study findings highlight the need for leadership support for formal integrated models of palliative care for patients with COVID-19, a palliative care role in pandemic planning, and educational initiatives with primary palliative care providers.
Keywords
• Palliative care is well suited to support patients hospitalized with COVID-19, but integration has been variable and generally poor.
• Primary palliative care knowledge, patient and family factors, COVID-19 specific factors, palliative care service characteristics, as well as institutional leadership and culture affected palliative care integration in the management of COVID-19.
• Many barriers remain centered on a misunderstanding that palliative care is relevant only for those as end of life, or those with comfort related goals of care.
• Perceived threats of poor availability to specialized palliative care services, as well as personal protection equipment and medication shortages were not realized by participants.
• Our research indicates the need for high-level support for formal palliative care integrated models of care, a palliative care role in pandemic planning as well as the need for ongoing educational initiatives with primary palliative care providers to overcome barriers of palliative care integration in COVID-19 care.
Introduction
During the Coronavirus disease 2019 (COVID-19) pandemic, there have been calls to action by international colleagues to support the palliative care needs of patients with COVID-19.1–3 Data to date indicate that almost 349 million people have contracted COVID-19, with over 5.6 million deaths worldwide, 4 yet palliative care involvement and its integration into the management of these patients has been variable and poor in many centres.5–10 It is unclear why some centres mobilized their palliative care skills and resources more than others.1,10,11
Few studies explore the barriers to palliative care in previous epidemics or pandemics. These studies based out of Africa and Asia outlined shortages in equipment, medications and trained healthcare workers as well as poor organization and coordination of services as the main barriers to accessing palliative care during a pandemic.7,12 No studies have evaluated the challenges in integrating palliative care into the care provided to patients with COVID-19.
The aim of this prospective qualitative study is to explore the facilitators and barriers to palliative care integration in the care of patients with COVID-19. We describe the perceptions and opinions of intensivists and internists who cared for patients with COVID-19, as well as those of palliative care specialists to help understand the challenges of integrating palliative care into COVID-19 management.
Methods
The aim of this study is to describe the facilitators and barriers to palliative care integration in the care of patients with COVID-19.
Study design
We conducted a qualitative study with physicians that worked in hospitals across Canada during the COVID-19 pandemic. Our study design utilized a postpositivist framework which recognizes that our participants may have multiple perspectives rather than a unified single perspective of reality. 13 This study was approved by the University Health Network Research Ethics Board (ID: 20-5933).
Setting
We recruited physicians in practice during the COVID-19 pandemic from September 2020 to March 2021 (corresponding to the beginning of Canada’s Wave 2 and the start of Wave 3 of the pandemic). Our study included intensivists (e.g., critical care specialists) and internists (e.g., general internal medicine specialists) who provided care to hospitalized patients with COVID-19 and specialist palliative care physicians who worked in hospitals caring for patients with COVID-19 but may or may not have provided direct care for these patients. All participants practiced medicine in Canada.
Population
Inclusion criteria for this study were: English speaking and being either (1) an intensivist or internist providing care to patients with COVID-19, or (2) a specialist palliative care physicians working in a hospital environment supporting the care of patients with COVID-19. Exclusion criteria included: non-English speaking physicians that did not provide care in hospitals during the pandemic as well as intensivists and internists that did not provide care to patients with COVID-19. Eligible participants were approached and consented virtually.
Recruitment
To recruit participants, we posted study information on a COVID-19 website hosted by the Canadian Society of Palliative Care Physicians, and potential participants were encouraged to contact the research team. We also employed snowball sampling, wherein current participants identified potential participants and reached out to them with the research team’s contact information or asked them if they preferred the research team to contact them.
Data collection and measures
Participants completed a demographic questionnaire virtually prior to the semi-structured, open-ended interview. The interview guide (Appendix 1) was developed with insight and guidance from clinicians and researchers and then pilot tested with a physician meeting the inclusion criteria. Questions were designed to gather information on the participants’ practice and the care provided to patients during the COVID-19 pandemic, including their provision of palliative care and the barriers and facilitators to the integration of palliative care. The interview guide was amended after each of the first four interviews. Interviews were conducted and audio recorded by three researchers (KW, AW, and LH) who did not have a close relationship with the participants, and subsequently de-identified. All participants were assigned a unique study ID for data collection and analysis, and recordings were subsequently transcribed verbatim by a 3rd party company. We determined we had reached a sufficient sample size by ascertaining the point at which we reached thematic saturation. As we were collecting data, we were coding transcripts, and we determined we had hit saturation once no new themes were identified in the new transcripts.
We used thematic analysis to describe participant’s understanding of the barriers and facilitators of palliative care integration for patients with COVID-19. Palliative care integration refers to the provision of palliative care (such as symptom management, goals of care discussions, end of life care, etc.) that occurs along with other focused medical management (i.e. cancer care, infection treatment, etc.). As palliative care may have been provided by their current care team, or by consulting specialists, we explored two concepts: integration of palliative care via primary palliative care provision (i.e., palliative care provided by attending internists or intensivists) or via specialized palliative care provision (i.e., referral to and integration of specialist palliative care teams). 14 Thus, we looked at the barriers to physicians integrating and providing palliative care themselves, as well as the barriers to involving specialist teams to do so.
Data analysis
The coding team (KW, KTW, LH and AW) first reviewed over 50% of the transcripts and then worked collaboratively to compile a list of high-level concepts inductively using thematic analysis.15,16 Once the codebook was finalized, two team members (KW and KTW) consensus coded all 23 transcripts using Nvivo (Nvivo Qualitatitve Data Analysis and Software Version 12. 2018). Themes were further reviewed and refined by team members (KW, KTW, AW, LH, SRI and CZ).
Results
A total of 23 physicians, including 13 specialists in palliative care, five intensivists, and five internists were interviewed. Two additional clinicians (one intensivist and one palliative care physician) also agreed to participate but were unable to find a convenient time to complete an interview. The participant average age was 42 years (SD 11) and 61% were female (Table 1). Twenty-one participants were from the province of Ontario, one from Nova Scotia and another from Quebec. Participants were employed at 18 unique health care institutions. All intensivist and internist participants indicated that they had cared for patients with COVID-19 on a general medicine unit, on a dedicated COVID-19 ward, or in an intensive care setting. All palliative care physicians indicated they worked in a hospital setting, but 7 of these physicians also provided care in the community and/or on a palliative care unit or hospice. Two palliative care physicians indicated they did not care for any patients with COVID-19, and another stated they provided care for patients with COVID-19 only outside their hospital (in a long-term care home). All intensivists and internists indicated they provided primary palliative care to their patients both before and during the pandemic and claimed familiarity with their institutional specialist palliative care team, had referred patients before, and had positive relationships with these teams.
Participant Demographics.
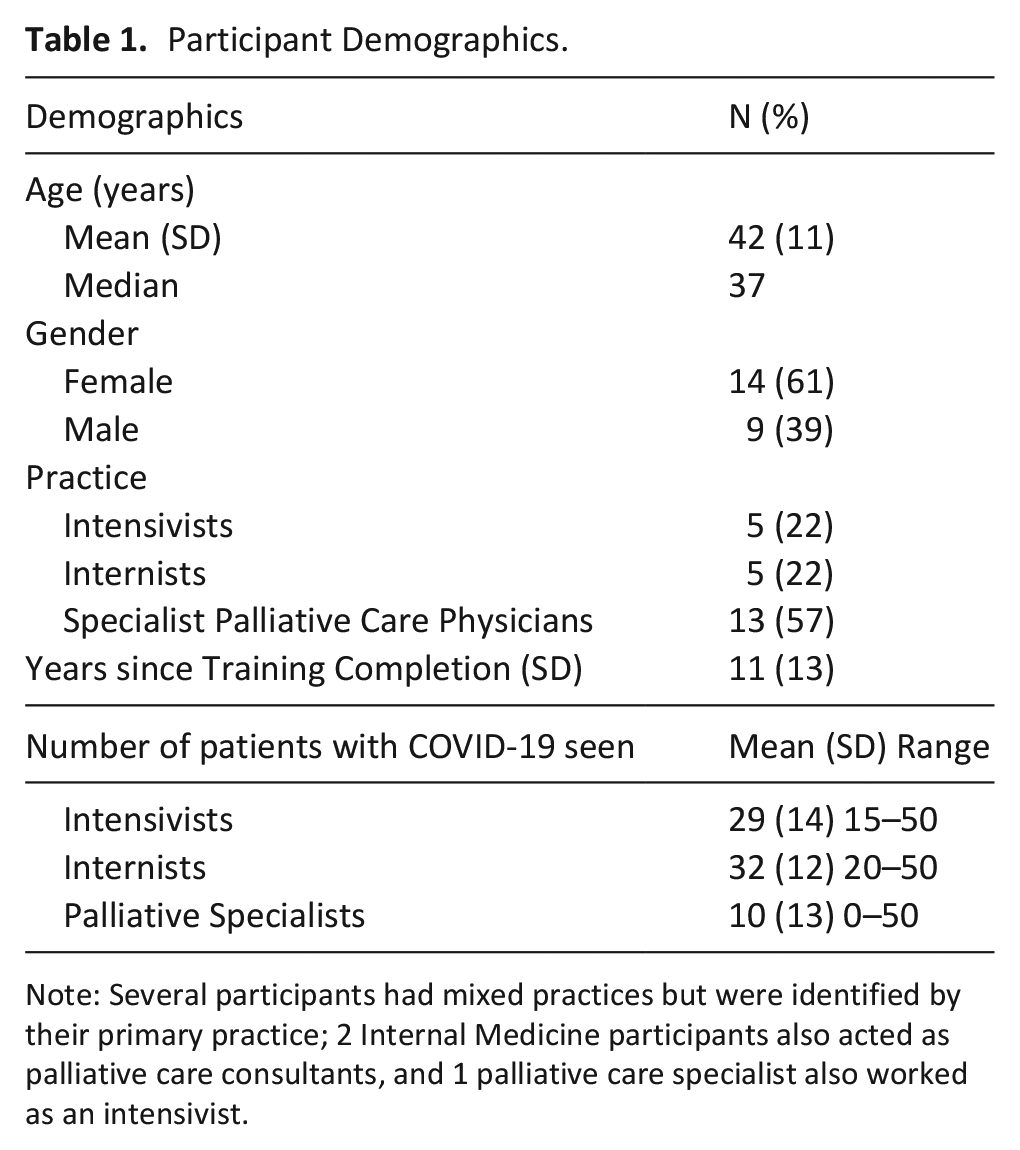
Note: Several participants had mixed practices but were identified by their primary practice; 2 Internal Medicine participants also acted as palliative care consultants, and 1 palliative care specialist also worked as an intensivist.
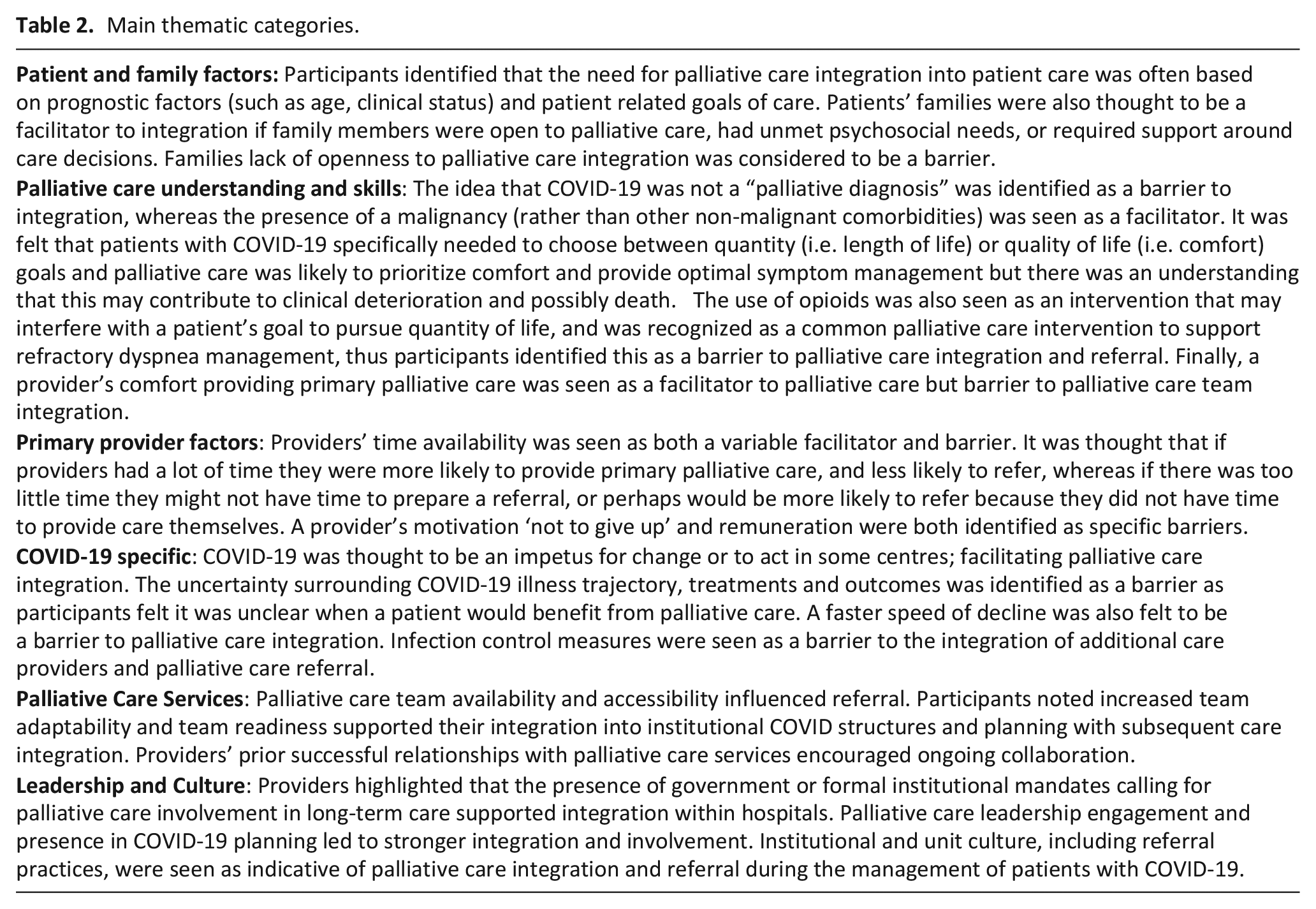
We identified five main thematic categories that outline the barriers and facilitators to palliative integration: patient and family factors, palliative care knowledge, primary provider factors, COVID-19 specific factors, palliative care service factors, and leadership and culture (Table 2).
Main thematic categories.
Patient and family factors
Participants indicated that certain patient characteristics, prognosis, as well as patient goals of care influenced the need for palliative care integration into their management of COVID-19. These descriptors often implied prognosis and included patient age, number of comorbidities, and clinical status; with older patients, those with more comorbidities, poorer clinical status and poorer prognosis more likely to be deemed appropriate for palliative care integration. Patients with unclear or comfort-related goals were perceived as more likely to be provided palliative care. Younger patients, those that were previously healthy, or had goals in line with intensive care were felt to be less likely to receive palliative care.
I’ve involved palliative care in non-palliative patients [with COVID-19] for symptom management, but because most . . . families wanted to be quite aggressive with their goals . . .. I wasn’t sure what palliative care was going to provide me. Intensivist 5 Male
Patients’ families were thought to be a facilitator to integration if family members were interested or open to palliative care, had clinician-identified unmet psychosocial needs, or required support around care decisions. Family members not being open to palliative care was seen as a barrier to referral.
I explained to the families. . . I’m. . . involving palliative care and they freaked out because it means that I’m going to stop aggressively treating their patients . . . when that’s not in keeping with what they had envisioned. That’s happened a few times and the family will say why is palliative care. . . becoming involved when we’re aggressively treating this pneumonia. Intensivist 5 Male
Palliative care knowledge: understanding and skills
Participants highlighted that in some cases palliative care was still stigmatized due to an association with end of life, and that this was seen as a barrier to palliative care integration into COVID-19 care.
There’s a lot of cases where we feel that palliative care involvement would have been useful and it hadn’t been activated yet. . . because the patient was . . .fairly new or the family or the primary MRP (most responsible physician) didn’t feel that the family was yet ready to have conversations with palliative care because of the assumed stigma. Intensivist 3 Female
Some participants felt that COVID-19 was not a ‘palliative diagnosis’, purporting that COVID-19 was an acute illness, unlike a diagnosis of cancer or other ‘advanced serious illnesses’ or ‘chronic palliative illness’, thus questioning the need for palliative care integration in this patient population.
It’s a summation that we generally did not need [palliative care]. So I didn’t really need it because as I mentioned is that often palliative care is extremely helpful for us in patients with complex oncological history with the symptoms that are outside shortness of breath or patients that they are chronically palliative care, right those patients that have chronic palliative clinical illness. . .. This was not a COVID case. It was an acute illness. Intensivist 2 Male
Several participants described how they felt that patients with COVID-19 specifically needed to choose between quantity (i.e., length of life) or quality of life (i.e., comfort) goals and opting for quantity of life goals was seen as a barrier to palliative care integration.
I guess one of the reasons was on some of the wards the openness of the treating physician to consult palliative care. . . .for symptom management because I think they wanted to focus. . . They didn’t want us to interrupt or interfere with active medical management or management that would increase quantity of life. Palliative Care 11 Male
Specifically, it was felt that patients with moderate or severe COVID-19 will suffer from discomfort (i.e., dyspnea, cough, etc.) and to survive COVID-19 it would necessitate living with this discomfort or suffering because management of this could jeopardize survival. Alternatively, it was felt that palliative care could prioritize comfort and provide optimal symptom management but there was an understanding that this may contribute to clinical deterioration and possibly death.
I think one of the main barriers is there’s still the stigma that palliative care involvement will increase the likelihood that someone dies. So on a few occasions, they were patients who were quite symptomatic. But the team perceived them as having a chance of “pulling through” so I would ask the nurse and I hear that this individual is having a lot of dyspnea and would it be okay if we [palliative care] were involved. . . to co-manage their symptoms and with certain staff the answer, let’s give it another day, it’s I think that stigma where getting us involved will increase the likelihood that they will die resulted in unnecessary suffering for those patients. Palliative Care 3 Male
The use of opioids was seen as an intervention that may interfere with a patient’s goal to pursue quantity of life, likely due to its risk of respiratory depression. As opioids were recognized as a common palliative care intervention to support refractory dyspnea management, participants identified this as a barrier to palliative care integration and referral.
As far as I know like physiologically there isn’t a lot of reason why a small dose of opiates would increase the likelihood that some of them will pass away with COVID. It’s rare that they have hypercapnia as a predominant symptom. So that’s why I felt very comfortable. Even when I was on medicine giving small amounts regularly to patients who were dyspneic with COVID, but I think at the end of the day, it was an individual decision. . Palliative Care 3 Male
Both intensivist and internist participants indicated they felt that palliative care was part of their speciality, and that they had provided primary palliative care to their patients and were comfortable doing so.
I think most of us. . .we think that we can do a lot of the symptom management and the family support. I say that when we do get palliative care involved. . ., it’s mostly to help with the family support component of things because we can be quite stretched and sometimes the support that the palliative care consultants can offer can be quite invaluable. . . When . . . it’s just a question of symptom management. . . I think I have a level of comfort whether or not I’m all that good at it.. Intensivist 1 Male
Palliative care participants also recognized that their internist and intensivist colleagues had skills in primary palliative care, but both groups questioned whether the palliative care provided by both groups was equivalent.
I think there are some staff who feel like they know how to do palliative care and so they don’t feel like they need to involve us, but . . .we would suggest our involvement and maybe there are things that are missed that they’re not even aware of. Palliative Care 1 Female
In terms of integration, a provider’s comfort providing primary palliative care was seen as a facilitator to palliative care provision but a barrier to specialist palliative care team involvement.
Primary provider factors: available time, attitude, and reimbursement
Several provider characteristics were highlighted as factors in supporting palliative care integration. Providers’ time availability was seen as both a facilitator and barrier; it was thought that if internist and intensivist providers had more available time, they were more likely to provide their own palliative care, and less likely to refer.
Actually, what we noticed was because there was one staff for the COVID patients and it’s actually less patients for a staff on GIM (general internal medicine) to only have like eight or nine patients with COVID. I think they had the time to have those conversations independently of us. So I actually wonder if we could have been involved in more patients but because the GIM staff had the time because of this new organizational structure we weren’t always involved in the goals discussions. Palliative Care 1 Female
If clinical demands were high clinicians might not have had time to make a referral, or conversely would be more likely to refer because they didn’t have time to provide primary palliative care themselves.
It wasn’t the forefront of my mind because generally the times that I had COVID patients they were very sick COVID patients. Got acutely worse so quickly that you’re calling ICU or you’re calling the family to say that they’re dying. I didn’t have a situation where there was a middle ground where there would have even been time my palliative care colleagues to come support. But if I look back. . .there were times when it would have been helpful to have backup support. Internist 2 Female
A provider’s attitude of ‘not giving up’ or ‘never saying die’ was seen as a specific barrier.
That is the never-say-die attitude of so many of our colleagues. All with good intention and whether it’s their approach to care or they’re just reluctant to have the important conversations independent of COVID. Internist 5 Male
Participants also identified physician remuneration as a barrier to referral as government billing only allows for one physician to bill for certain provisions of palliative care per patient.
The biggest thing is that everyone here is fee for service. . . Everyone is making sure that they look after themselves. And so sometimes people might be hesitant to make referrals or to transfer out. Palliative Care 12 Male
COVID-19 specific factors: the impetus to act, uncertainty, and infection control measures
Participants identified several factors specific to COVID-19 that acted as facilitators or barriers to palliative care. COVID-19 was thought to be an impetus for change or action, which facilitated palliative care integration and collaboration.
It was certainly COVID that got [collaboration] going. It lit the fire. Palliative Care 8 Female
The uncertainty surrounding COVID-19 treatments, illness trajectory, and outcomes was identified as a barrier, as participants felt it was unclear when or if a patient would benefit from palliative care.
I think it just shook everyone. I just think the way people were dying was shocking to everyone, - just how quickly it happened and how well they looked the day before they died. So I think maybe it was just such a new thing.. Palliative Care 6 Female
A more rapid clinical decline, which was noted to occur at times with COVID-19, was felt to be a barrier to palliative care integration and referral.
The trajectory of when they acutely (got) worse.. that happened so quickly that they would either get immediately intubated or passed away so quickly that there just wasn’t time. Internist 2 Female
Infection control measures were also seen as a barrier to palliative care referral as clinicians tried to limit the number of providers in contact with patients as well as limit the use of personal protection equipment.
I think there was a sense from the MRP of minimizing staff on and off the unit if they don’t need to be. . . Especially staff that are supporting the rest of the hospital. We really didn’t get called. Palliative Care 8 Female
Of note, none of the participants indicated that they faced any specific shortages of personal protection equipment.
Palliative care service factors: accessibility, adaptability and successful relationships
Palliative care team availability and accessibility were seen as influencers of palliative care team integration and referral practices. If palliative care teams were perceived as being available to their patients with COVID-19, participants felt they were more likely to involve them.
All of our palliative care doctors are great to work with- they keep us posted with their plans or their discussions. We work quite closely together, especially with family meetings. They’re always available by phone. Internist 4 Female
At times, virtual structures were seen as less effective at meeting the needs of referrers and a barrier to referral.
On occasion when I asked palliative care to come to the unit to help with some of the dynamics there’s been sort of a push back. So at a certain stage, I just decided that I needed to become more comfortable with doing a lot of that work myself. . . So I think the contexts where I would be contacting palliative care would be to help with supporting families and it just didn’t come up as a something that seemed to be feasible just given that everybody was operating remotely. . .. We had less support from the consultative service that we did prior to COVID because people weren’t coming to the hospital. Intensivist 1 Male
Participants noted increased palliative care team adaptability and team readiness supported their integration into institutional COVID-19 planning and subsequent care integration, including new clinical models that were developed to better meet the needs of patients and families with COVID-19.
We developed like an embedded model with the general medicine teams that we’ve continued since the first wave where we actually attend the medicine rounds daily, which we haven’t done in the past and it’s our chance to kind of identify patients including COVID positive patients who would benefit from our involvement. Palliative Care 3 Female
Providers’ prior successful relationships with specialist palliative care services were thought to encourage collaboration. Of note, none of the participants mentioned any significant palliative care resources as a barrier to integration (i.e., medication or staffing shortages).
Leadership and culture factors
Providers highlighted the role of leadership and culture in facilitating palliative care integration. Many participants identified that the government had mandated their acute care hospitals to support regional long-term care homes that were facing COVID-19 outbreaks. Although these mandates were not specific to palliative care nor did they outline a call for palliative integration, some institutions interpreted these mandates as a need for palliative involvement in the planning and provision of this support.
(The hospital) was called in the first wave to support long term care homes in the region. . . A lot of our rehab docs, geriatricians they went into every long-term care in the region. Palliative care was sent in to help with that aspect. Palliative Care 8 Female
Palliative care leadership engagement and presence at COVID-19 planning tables was felt to lead to stronger integration and involvement.
I think it was sort of coming in both directions, we were reaching out and we were being invited. They invited us to sit at tables- our own sort of (regional health) community set up weekly meetings. . . There was a palliative care presence on both of those and the infectious disease outreach had a palliative care physician as well. Palliative Care 5 Male
Participants highlighted that institutional and unit culture, including referral practices, were seen as indicative of palliative care integration and referral of patients with COVID-19. Several participants revealed it was less common for palliative care teams to care for patients in the intensive care unit outside of particular circumstances, and that certain physician groups (i.e., cardiologists) were less likely to refer or integrate palliative care when managing COVID-19 wards.
I think the culture of cardiology at our hospital is one that is not conducive to palliative care. Whereas it seems like the general culture for respirology and Internal Medicine, they are much more likely to give us a call. . . That was reflected on the COVID ward as well. . . I think depending on which ward it was, each ward was managed by different physicians. The ward managed by the cardiologist team like any time we came there, we felt like we were bothering them. . . The team that was managed by infectious disease were very receptive, the team managed by the respirologist were also very receptive and as well as the internists were receptive. Palliative Care 11 Male
Discussion
Main findings
We conducted a prospective qualitative study to explore physicians’ perceived facilitators and barriers to the integration of palliative care into COVID-19 management. Participants described six main thematic categories: patient and family factors, palliative care knowledge, primary provider factors, COVID-19 specific factors, palliative care service factors, and institutional leadership and culture.
What this study adds
Although several studies have outlined the planning and implementation of palliative care initiatives for current and past pandemics,7,12 to our knowledge this is the first study to explore the factors influencing the integration of palliative care into the management of patients with COVID-19 and their families. Previous studies have explored barriers to integrating palliative care into care for general medical populations,17,18 as well as for those with cancer, 19 advanced heart disease,20–22 chronic obstructive pulmonary disease (COPD)23–25 and dementia. 26 The most prevalent barriers concern education, including lack of knowledge concerning what palliative care is (and what it is not), clarity around referral processes, and lack of primary palliative care skills.17–19,21,22,24–26 In our study, all internist and intensivist participants indicated they had a good understanding of palliative care, were familiar with their institutional specialist palliative care teams, and provided primary palliative care to their own patients when applicable. Many Palliative care participants also recognized their colleagues’ comfort and confidence in provision of primary palliative care while managing patients with COVID-19.
This confidence of primary providers in their palliative care knowledge and skills was at odds with participants identifying that patient characteristics such as age and clinical status (used as prognostic indicators), as well as overarching goals of care, were being used to determine palliative care integration and referral. Some internist and intensivist participants also indicated that COVID-19 was not considered a ‘palliative diagnosis’, and that palliative care was more appropriate for patients with cancer than patients with COVID-19 or those with other non-malignant diseases. Despite their acknowledged role as a palliative care providers, there was a disconnect with understanding that palliative care is relevant to all patients facing a life-limiting disease, is not prognosis-dependent, is based on patient need, and can be provided alongside life-sustaining treatments. It seemed that their definition of palliative care was equivalent to the provision of comfort or end of life care, rather than a more holistic perspective on the definition of palliative care. Thus, although provider’s comfort in providing primary palliative care acted as a facilitator to palliative care integration for some patients at end of life or with comfort-focused goals, it may have also acted as a barrier for others not as close to death or with more medically-focused goals.
Palliative care participants identified a misperception of the need to choose between supporting length of life versus quality of life in the management of patients with COVID-19. Due to the nature of severe COVID-19, including the risk of respiratory failure,9,27 clinicians felt that to optimize treatment for refractory dyspnea with opioids could negatively impact survival. These concerns and fears over the use of opioids for dyspnea have been outlined previously in patient populations with respiratory disease,28–30 despite evidence that management of refractory dyspnea with opioids is safe and effective in alleviating discomfort from refractory dyspnea.31–33
Several other COVID-19 specific barriers were described in our study. COVID-19 was seen as a new illness with evolving treatment regimes, unknown trajectory, and unclear outcomes. Intensivist and internist participants expressed concerns about the uncertainty in predicting when a patient would be at risk of death which was also complicated by the rapid clinical decline sometimes witnessed by our participants and documented in the literature.34,35 In previous studies concerning other non-malignant disease states such as heart failure, COPD, and dementia, an unpredictable disease trajectory similarly acted as a barrier to palliative care integration.20–26 Palliative care resource flexibility and collaboration have been outlined as facilitators to referral in COPD 24 and dementia populations 26 comparable to our findings of the facilitator ‘team readiness and adaptability’ of palliative services to manage patients with COVID-19.
In preparation for and during COVID-19 surges, many institutions prepared for a possible influx of patients and recognized the need to better integrate palliative care.36–38 Participants indicated that the drive to prepare for COVID-19 resulted in integration not seen previously. Similar to earlier research, 7 participants also thought this was reinforced when several provincial governments instituted a mandate for acute care hospitals to assist the long-term care sector due to extensive COVID-19 outbreaks. 39 However, the influence of these factors was variable as local institutional leadership was left to determine the need for palliative care involvement in initiatives to support patients.
Outside of the new palliative clinical structures, participants highlighted the importance of unit culture in determining palliative care penetrance. Intensive care unit and COVID-19 wards were felt by some participants to have decreased receptiveness to palliative care team involvement. Institutional, unit or practice-based cultural factors have been highlighted previously as barriers to palliative care integration. 40 Non-oncologic specialists (i.e., cardiology, respirology, etc.) have been identified as being less knowledgeable than oncologists about palliative care and more likely to associate it with end of life, and to believe services are better suited to patients with cancer and lack expertise in managing their patients’ palliative care needs.20,40,41
Limitations
Our study has limitations. Although this study included participants from several provinces, generalizability may be limited because providers came from a single country that may have different COVID-19 rates than other countries, with many participants practising in large, academic medical centres that had comprehensive palliative care programs. Participants therefore likely had pre-existing attitudes and preferences towards referral patterns to specialist palliative care teams, including comfort in defining when and how to provide primary palliative care. There also may be a potential response bias as those familiar with palliative care may be more likely to participate.
Conclusions
This study highlights that improving the integration of palliative care during the COVID-19 pandemic will require interventions at multiple levels, including for patients, families, primary care providers, palliative care consultants, and institutional leadership. To better facilitate palliative care integration into the care for patients and families facing COVID-19, palliative teams need to be accessible and adaptable. Leaders in the field will need to ensure their presence at pandemic planning tables that establish clinical models to meet the needs of people experiencing COVID-19. Despite efforts to educate health care providers that palliative care is not just for patients at end of life, many barriers to palliative integration in COVID-19 care continue to relate to this misconception. As the capacity of primary palliative providers improves during and beyond the pandemic, the principles of palliative care should be upheld so that patients and families reap the benefits of this care regardless of diagnosis, complexity, prognosis or goals of care.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221087162 – Supplemental material for Identifying barriers and facilitators to palliative care integration in the management of hospitalized patients with COVID-19: A qualitative study
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221087162 for Identifying barriers and facilitators to palliative care integration in the management of hospitalized patients with COVID-19: A qualitative study by Kirsten Wentlandt, Kayla T. Wolofsky, Andrea Weiss, Lindsay Hurlburt, Eddy Fan, Ebru Kaya, Erin O’Connor, Warren Lewin, Cassandra Graham, Camilla Zimmermann and Sarina R. Isenberg in Palliative Medicine
Footnotes
Authorship
Concept and design: KW, LH, AW, KTW, EK, WL, EO, CG
Acquisition, analysis, or interpretation of data: KW, LH, AW, KTW, EF, SI, CZ
Drafting of the manuscript: KW
Critical revision of the manuscript for important intellectual content: KW, LH, AW, KTW, EF, SRI, CZ, EK, WL, EO, CG
Statistical analysis: KW
Administrative, technical, or material support: KW, LH, AW, KTW, EF, SRI, CZ, EK, WL, EO, CG
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics and consent
This study was approved by the University Health Network Research Ethics Board record 20-5933.1.
Data sharing
All data submitted complies with Institutional or Ethical Review Board requirements and applicable government regulations
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.