
Abstract
Background:
Rectal tenesmus is a distressing symptom in patients with advanced cancer and challenging to treat. There is lack of consensus on the appropriate management of tenesmus in this patient population.
Aim:
To identify and examine the effectiveness of interventions to palliate rectal tenesmus caused by advanced cancer when surgery, radiotherapy or chemotherapy are no longer treatment options.
Design:
A systematic review of the literature following standard systematic review methodology and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidance.
Data sources:
A comprehensive search of the electronic databases MEDLINE, EMBASE and the Cochrane Library was conducted from date of inception to April 2016. PubMed ‘related articles’ search, grey literature search and hand-searches of the bibliographies of relevant papers and textbooks were also performed. Non-cancer patients were excluded. Any studies involving surgery or radiotherapy to treat tenesmus were excluded. Studies involving interventions to treat pelvic pain syndromes without specific outcome measures on severity of tenesmus were excluded. The quality of the studies was assessed using a National Institute for Health and Clinical Excellence–recommended quality assessment tool.
Results:
From 861 studies, 9 met full criteria and were selected. All were case series investigating the use of pharmacological interventions (diltiazem, nifedipine, methadone, mexiletine hydrochloride, lidocaine and bupivacaine), anaesthetic interventions (lumbar sympathectomy, neurolytic superior hypogastric plexus block), and endoscopic laser interventions. The included studies showed substantial heterogeneity, and therefore, a meta-analysis was not feasible.
Conclusion:
From this review, we identified a significant gap in research into the palliation of rectal tenesmus. A multimodal approach may be necessary due to the complexity of the pathophysiology of tenesmus. Future research should focus on randomised controlled trials of drug therapies whose potential effectiveness is suggested by case series.
Rectal tenesmus caused by malignant disease is a distressing symptom that significantly affects quality of life.
The prevalence of rectal tenesmus in the cancer population is unknown. In patients with recurrent rectal carcinoma, the reported prevalence is around 14%.
The pathophysiology is complex and not fully understood.
Varying treatment options exist with unclear rationale.
Weak evidence based on case series exists for diverse treatments including pharmacological interventions (diltiazem, nifedipine, methadone, mexiletine hydrochloride, lidocaine and bupivacaine), anaesthetic interventions (lumbar sympathectomy and neurolytic superior hypogastric plexus block) and endoscopic laser interventions.
There is a significant gap in research for palliation of tenesmus.
The information gained from these case series should be used to generate hypotheses that lead to focused studies of stronger designs, ideally randomised controlled trials.
A multimodal approach may be necessary due to the complexity of the pathophysiology of tenesmus.
Background
Rectal tenesmus is the painful sensation of incomplete evacuation of the bowel, resulting in the sensation of needing to defaecate many times daily.
The most common malignancy resulting in tenesmus is rectal carcinoma; however, any pelvic malignancy can cause the symptom. Non-malignant conditions (e.g. inflammatory bowel disease) and treatment side effects (e.g. radiation proctitis) can also result in tenesmus.1–3
Prevalence of tenesmus in the cancer population is unknown. In patients with recurrent rectal carcinoma, the reported prevalence is around 14%. 4 Despite low prevalence, tenesmus is acknowledged clinically as a very distressing symptom that affects quality of life. 5
The pathophysiology of tenesmus is not fully understood. It is proposed to be caused by tumour invasion of the lumbosacral plexus resulting in neuropathic pain, tumour inflammation transmitting pain through somatic afferents and smooth muscle contraction transmitting pain through autonomic afferents. 6
Definitive treatment targeting underlying malignancy includes surgery, chemotherapy and radiotherapy. In patients without these options due to disease status or patient status, pain control is challenging. Tenesmus is largely unresponsive to opioids. 7 Benzodiazepines and phenothiazines, traditionally used to treat tenesmus, have no evidence base. 8
This systematic review was conducted to investigate treatments available for the palliation of malignancy-related tenesmus, when surgery, radiotherapy or chemotherapy are no longer treatment options.
Objective
To identify and examine the effectiveness of interventions to palliate rectal tenesmus in cancer patients.
Methods
This systematic review was performed in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline. 9 All study designs were eligible for inclusion, apart from single-case reports.
Adult patients with tenesmus caused by cancer were included. Any palliative intervention intended to treat tenesmus was included. Disease-modifying interventions (surgery, chemotherapy and radiotherapy) were excluded. Although radiotherapy is beneficial for palliation of malignant pelvic pain, it was excluded due to the frequently described side effect of radiation proctitis (incidence rates from 2% to 39%), commonly resulting in severe tenesmus.1–3
The primary outcome measure was reduction in severity of tenesmus (measured by numerical rating scales (NRS), categorical scales (complete, partial and no relief), reduced sensation to defaecate or patient’s account of improvement). Secondary outcome measures varied. Side effect profile of each intervention was included in the data analysis.
MEDLINE (Ovid MEDLINE® In-Process & Other Non-Indexed Citations and Ovid MEDLINE® 1946 to Present), EMBASE (1974 to 7 April 2016) and Cochrane Library were electronically searched. Detailed search strategies were developed for each database (sample search strategy available in supplementary online material). A PubMed ‘related articles’ search was conducted on the final list of articles. 10 There were no language or date restrictions due to the paucity of studies available. References from palliative care textbooks and grey literature were also searched.
Following the search method outlined above, studies were reviewed to determine which met inclusion criteria (inclusion/exclusion criteria available in supplementary online material). A final list of inclusion studies was then selected and data extracted. Data extraction was performed by one reviewer using predesigned data extraction forms. RefWorks software managed citations and ensured tracking of studies at various stages.
Risks of bias of each study were assessed using a National Institute for Health and Clinical Excellence (NICE) 11 -recommended quality assessment tool. Meta-analysis could not be performed due to heterogeneity among the studies included.
Results
Following electronic database search and removal of duplicates, 861 studies were identified. One study was found through PubMed-related articles’ link search. 12 After reviewing the titles and/or abstracts of 861 studies, 19 articles were deemed to meet inclusion criteria. Nine were subsequently suitable for inclusion in the analysis.13–20
All nine studies included were case series: seven prospective and two retrospective. Interventions used to treat tenesmus included pharmacological, anaesthetic and endoscopic laser therapy (ELT) interventions. Six different drug treatments were used: diltiazem, nifedipine, methadone, mexiletine hydrochloride, bupivacaine and lidocaine. The anaesthetic interventions were lumbar sympathectomy and neurolytic superior hypogastric plexus block from a posteromedian transdiscal approach. Endoscopic treatment with Nd-YAG laser was the method used in both ELT studies. Characteristics of included studies are summarised in Table 1.
Characteristics of included studies.

NRS: numerical rating scale; ELT: endoscopic laser therapy; OME: oral morphine equivalent.
Sample sizes within the included studies were small: largest sample size 26 and smallest 2. Two studies were conducted in the United Kingdom; the remaining studies took place in America, Japan, Belgium, Spain, Turkey, Poland and Ireland. Patient’s settings included hospices, acute hospitals or home.
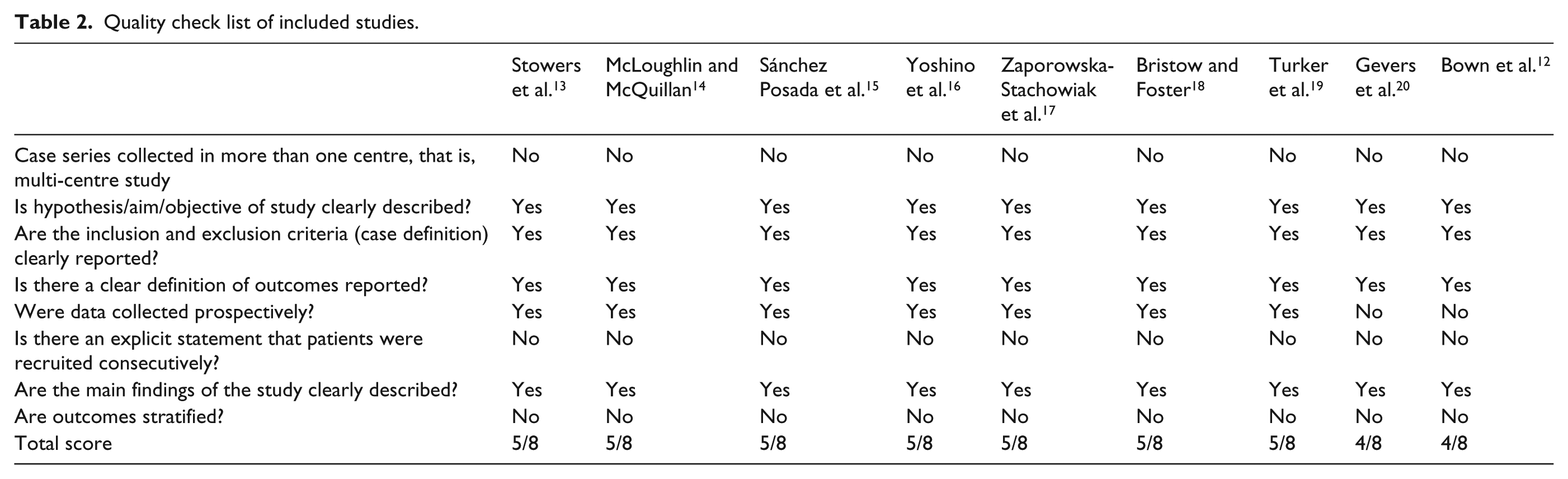
Using the quality assessment form, seven studies scored 5/8 and two studies scored 4/8 11 (Table 2). Multiple limitations of included studies need to be acknowledged. First, case series have no control population and are prone to bias. Another limitation is small sample size (mean sample size of eight). Selection bias is an issue in most of the studies as consecutive patient enrolment was not explicitly stated. The outcome measures are clinically relevant in all included studies; however, they were collected retrospectively in two studies. These factors limit generalisability of findings.
Quality check list of included studies.
Effects of interventions
The results of the included studies are summarised in Table 1. Stowers et al. 13 presented two patients with tenesmus treated with oral diltiazem. Both patients had reduction in pain intensity and reduction in total daily oral morphine equivalent (OME) use with no adverse effects. A case series of four patients, by McLoughlin and McQuillan, 14 reported that oral nifedipine improved severity of tenesmus in 75% (three patients) and was well tolerated. Sanchez Posada et al. 15 reported four patients with pelvic tumours and tenesmus, commenced on methadone as first-line opioid. Pain control was maintained until death or end of study period. Mild drowsiness was noted in two patients without need to adjust methadone dose.
Yoshino et al. 16 presented five patients treated with mexiletine hydrochloride. Intravenous lidocaine was administered to one of the five patients prior to switching to mexiletine. All five patients reported a resolution of tenesmus 1–2 days after intervention. No adverse effects were noted. Bupivacaine, administered intrathecally and rectally, was used in a two-patient case series by Zaporowska-Stachowiak et al. 17 Intrathecal administration reduced severity of tenesmus to 0–1/10 at rest and rectal bupivacaine reduced pain to 0/10 at rest. Transient hypotension was noted post intrathecal administration.
Lumbar sympathectomy resulted in 83% (10/12 patients) gaining complete relief of tenesmus. 18 Temporary hypotension occurred in one patient. Resolution/reduction in severity of tenesmus was seen in three patients who underwent neurolytic superior hypogastric plexus block, with no adverse effects. 19
ELT resulted in complete resolution of tenesmus in 80.8% (21/26 patients) in Gevers’ et al. 20 case series. With the same intervention, Bown et al. 12 reported that 50% (four patients) gained complete relief from tenesmus. Complications included blood or mucus per rectum and rectal discomfort initially after treatment. In Gevers’ study, however, serious complications were reported, with five deaths (2.3%) in the series ‘possibly’ complication-related.
Discussion
This limited systematic review set out to identify and examine the effectiveness of interventions to palliate rectal tenesmus in cancer patients. Following a detailed search strategy, nine case series were identified with varying interventions: pharmacological, anaesthetic and ELT.
It is not possible to make definitive recommendations for practice based on this review. The strongest evidence available for palliation of tenesmus is lumbar sympathectomy and ELT; however, this is based on case series. Lumbar sympathectomy has a more favourable side effect profile and may be more appropriate in this patient cohort. In case series described above, calcium channel blockers led to a reduction in pain severity, likely by targeting smooth muscle contraction. Neuropathic agents (mexiletine hydrochloride, lidocaine, methadone) also showed positive responses.21,22 However, all pharmacological studies are case series with small numbers; therefore, no drug recommendations can be made. A multimodal approach may be necessary due to the complexity of the pathophysiology of tenesmus.
A number of limitations are present in this review. Included case series have inherent methodological deficiencies and significant interstudy variability; therefore, it is difficult to make recommendations. One reviewer selected studies and extracted data; recommendations advise at least two independent reviewers. Electronic database searching was restricted to MEDLINE, EMBASE and the Cochrane library.
From this review, we are now aware of the significant gap in research for palliation of tenesmus. Six out of nine studies identified in this review are greater than 10 years old. A significant need to conduct further research into tenesmus exists. The information gained from these case series should generate hypotheses that lead to focused studies of stronger designs, ideally randomised controlled trials. These are challenging – but not impossible – in a patient population with advanced illness and limited life-expectancy.
Footnotes
Acknowledgements
This work was completed towards an MSc in Palliative Care at King’s College London.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethics/research governance approvals
This is a systematic review of primary studies. Further ethical approval is not applicable.