
Abstract
Background:
Aromatherapy, massage and reflexology are widely used in palliative care. Despite this, there are questions about their suitability for inclusion in clinical guidelines. The need to understand their benefits is a public priority, especially in light of funding pressures.
Aim:
To synthesise current evidence on the effectiveness of aromatherapy, massage and reflexology in people with palliative care needs.
Design:
A systematic review of randomised controlled trials (PROSPERO CRD42017081409) was undertaken following international standards including Cochrane guidelines. The quality of trials and their pooled evidence were appraised. Primary outcomes on effect were anxiety, pain and quality-of-life.
Data sources:
Eight citation databases and three trial registries were searched to June 2018.
Results:
Twenty-two trials, involving 1956 participants were identified. Compared with a control, four evaluated aromatherapy, eight massage and six reflexology. A further four evaluated massage compared with aromatherapy. Trials were at an unclear risk of bias. Many had small samples. Heterogeneity prevented meta-analysis. In comparison with usual care, another therapy or an active control, evidence on the effectiveness of massage and aromatherapy in reducing anxiety, pain and improving quality-of-life was inconclusive. There was some evidence (low quality) that compared to an active control, reflexology reduced pain.
Conclusions:
This review identified a relatively large number of trials, but with poor and heterogeneous evidence. New clinical recommendations cannot be made based on current evidence. To help provide more definitive trial findings, it may be useful first to understand more about the best way to measure the effectiveness of these therapies in palliative care.
Aromatherapy, massage and reflexology are widely used in palliative care.
Patients themselves often report that these therapies are helpful.
It is important to demonstrate value for money in health care service provision including in palliative care.
This is the first systematic review to focus on aromatherapy, massage and reflexology in palliative care and to synthesise the evidence using established systematic review methodology.
Low-quality trials, and differences in the nature of the comparison arms and in the type of evaluation between trials made it difficult to draw any firm conclusions about the effectiveness of these therapies.
Although there was limited evidence on the effectiveness of aromatherapy, massage and reflexology equally no evidence of harm was reported.
Heterogeneity across the body of trials suggests the need for theoretical research to understand more clearly how complementary therapies are delivered in palliative care and the best way to measure any purported benefits.
Background
People with advanced illness can experience a range of problems, such as anxiety, fatigue and pain, 1 for which conventional treatments may not provide sufficient relief. In these circumstances, people may seek complementary therapies as adjuncts to conventional care. Complementary therapies may be offered as part of a holistic package in palliative care settings such as hospices. In the United Kingdom, a significant proportion of the funding for palliative care is from the government. As with all public expenditure, there is a need to demonstrate value for money. Without clear evidence derived from robustly designed studies, the place of publicly funded complementary therapy services is already in question.2,3
A systematic review on the effectiveness of aromatherapy, massage and reflexology in palliative care is needed for several reasons. In a UK national prioritisation initiative, research about the benefits of complementary therapies in palliative care was identified as a public and clinical health priority. 4 Aromatherapy, massage and reflexology are some of the most popular complementary therapies among the general public. 5 In the United Kingdom, these three therapies are commonly offered in palliative care settings. While these therapies may not cause harm, it is important to confirm this as well as their benefits. Their provision incurs service costs even though in palliative care settings they may often be provided by therapists volunteering their services. 6 Costs can include dedicated room use, massage couches, reception services and materials for the therapies. There are a number of trials that have evaluated these therapies, but there has been limited systematic, critical review of the evidence about the effectiveness of these therapies in palliative care. Such a review will generate conclusions beyond single studies, instead evidence from across studies can be critiqued, compared and pooled together. Thereby it will be able to provide more informed recommendations for funders, clinical providers and practitioners, and for future research.
It is important to look at evidence specific to palliative care, as conclusions drawn from elsewhere may not necessarily accommodate the different requirements that are relevant to people at a palliative stage of their illness. People with advanced illness frequently experience increased frailty and co-morbidities, and it is possible that the effects of any treatments or therapies in this situation may be different from those experienced in other situations. The criteria by which the success or otherwise are judged may also differ, for instance, it may not be possible for a dramatic improvement in symptoms to occur when someone is terminally ill and their condition is deteriorating day-by-day. The preferred ways the therapies may be provided and the expectations in this population compared with those less compromised and not facing existential issues may also differ.
It is important to highlight here that there are existing reviews of complementary therapies in palliative care. These reviews took a broader and different focus on the literature. For example, two reviews looked at both complementary and alternative medicines.7,8 Their search strategies did not include terms to describe different types of complementary therapies, thereby studies on specific therapies are likely to have been missed. Moreover, they only included studies written in the English language. Since some complementary therapies including reflexology have their roots in Eastern countries, for example, China, the reviewers may have missed studies published only in other languages. These reviews also included in their search strategy terms to describe specific symptoms of pain, nausea, vomiting, anxiety, fatigue, insomnia and dyspnoea; therefore, any trials that did not consider these specific symptoms would not have been identified. The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) was used in the most recent review. 9 However, new methodological advances 10 have led to an ongoing update of PRISMA. 11 In the systematic review presented in this article the focus and methods differ. We critically review, using current standard Cochrane methods that include methodological advances post publication of PRISMA,12–14 evidence from trials of complementary therapies commonly provided in palliative care settings.
Objectives
To examine the current evidence on the effectiveness of aromatherapy, massage and reflexology in people who are at a palliative stage of an illness.
Method
The review protocol is registered on PROSPERO (CRD42017081409). The systematic review approach followed Cochrane guidelines on the evaluation of evidence from randomised controlled trials on effectiveness.10,13 The Template for Intervention Description and Replication (TIDieR) was used to ensure we extracted key features of the intervention. 12 The Grades of Recommendation, Assessment, Development and Evaluation (GRADE) tool was used to provide a level of the quality of evidence per primary outcome on effectiveness.14–16 It provides a structured and transparent approach for rating confidence in estimates of effect.
Inclusion and exclusion criteria
Types of studies
Studies were included if they were randomised controlled trials (RCTs).
Types of participants
People aged 18 years or over in a palliative care setting (e.g. hospices) or who were described by the authors as having an advanced disease such as metastatic cancer or renal failure. We included studies of patients at an earlier stage of disease, if at least 50% of the sample were described as palliative or at an advanced stage.
Types of intervention and comparison
Aromatherapy, massage and/or reflexology. There was no restriction on how the intervention was provided or who provided it. There was no restriction on what the comparative arm involved. This could involve, for example, usual care or another type of intervention. Restrictions were not applied as we wanted to capture all trial evaluations. In our analysis, we distinguish between different characteristics in mode of delivery and type of comparison.
Studies were not restricted to English language. We did not include studies involving as the only recepients of the therapy children or family carers.
Types of outcome measures
The primary outcomes of interest were impact within a week of the end of the intervention on anxiety, pain and quality-of-life, and the occurrence of adverse events. Anxiety, pain and quality-of-life were selected as they are common issues in palliative care and are often the focus of evaluation in trials of complementary therapy. Secondary outcomes included mood, sleep and physical symptoms other than pain. We also sought measures of care satisfaction, such as self-report and attrition.
Data sources and searches
Database searches were conducted from inception to June 2018 in The Cochrane Trials Register, MEDLINE, EMBASE, PsycINFO, AMED, CINAHL, KoreaMed and ProQuest. Variations of the terms ‘palliative’, ‘aromatherapy’, ‘massage’ and ‘reflexology’ were used as search terms (see supplementary material). The MetaRegister of controlled trials, clinicaltrials.gov and The WHO Trials Registry were also searched. For any relevant studies, we checked their reference lists and reviewed papers citing the study, and sought contact with authors to ask if they knew of any studies we had missed.
Study selection
Screening was undertaken in duplicate independently. One author (M.A.) screened all citations (records of title with if available abstract) and other authors (B.C./N.K./S.W.) each screened a third. When a citation appeared relevant, or did not have sufficient information to decide, we retrieved the full-text paper. Should we have found any discrepancies in eligibility at screening and at full-text, we planned for these to be discussed for resolution by the wider review team. We documented reasons at full-text for any studies excluded.
Data extraction
Using Cochrane and TIDieR reporting guidelines, data were extracted for each study by one reviewer (M.A./B.C.) and checked by a second (B.C./V.V.).12,13 Key trial characteristics were extracted. These included type of trial, aim, demographics of participants, number of participants randomised and number analysed, details about the content of the intervention and comparison, interventionist, number of sessions, length of sessions, duration, and when and how the outcomes were measured. Where information was lacking, we attempted to contact the authors.
Risk of bias
One author (M.A.) assessed risk of bias for each study using the criteria recommended by the Cochrane Collaboration; 13 this was checked by a second (B.C.) resolving any disagreements by discussion. We assessed risk relating to selection, performance, detection, attrition and sample size.
Statistical analysis
Results were analysed according to type of therapy. At baseline where there were substantial differences between trial arms in key characteristics (such as psychological or physical symptoms), we did not report the trial findings because these difference may have obscured any differential effect between arms. When treatment effects were reported as continuous variables, we extracted (if appropriate) the mean difference (MD) between trial arms. When effects were reported as dichotomous, we extracted (if appropriate) the relative risk (RR) and confidence intervals (CI). If we were unable to standardise results to a RR or MD between trial arms, we report alternative statistical results as presented in the relevant paper. We considered, as detailed in our PROSPERO protocol, combining data across trials in a meta-analysis. It was based on sufficient homogeneity in key characteristics across more than two trials. Due to the nature of the included studies, a priori analysis was not feasible.
Quality of evidence
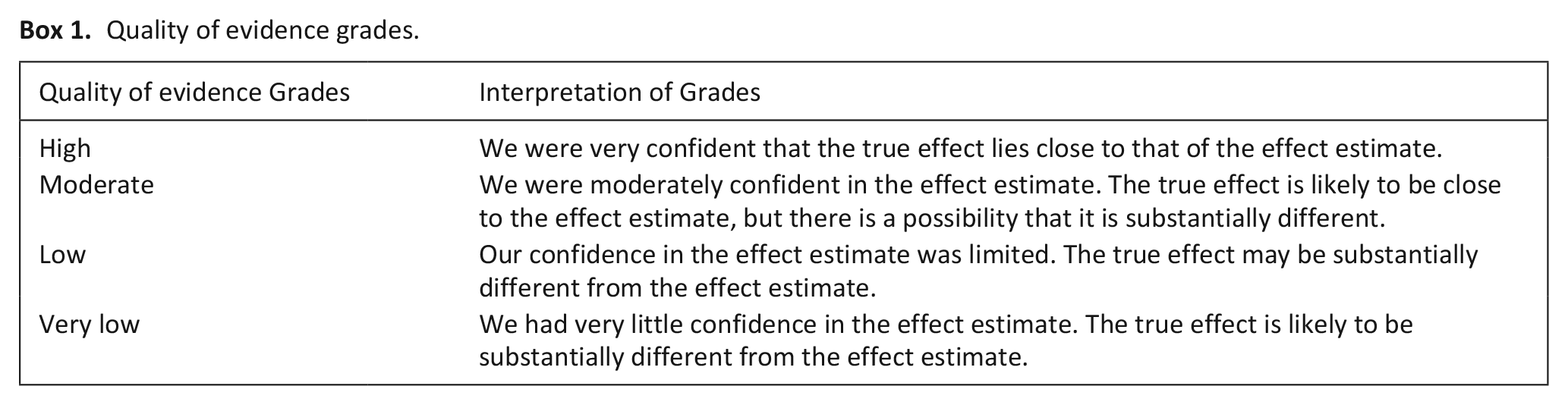
We used the GRADE system to assess the quality of the evidence of the primary outcomes on symptoms and quality of life.14,15 Evidence is graded as either, high, moderate, low or very low. We first assumed that the quality of the evidence was high, and downgraded by one level if there were serious limitations in risk of bias, indirectness, inconsistency, imprecision or publication bias (Boxes 1 and 2).
Quality of evidence grades.
Criteria for judging quality of the evidence.
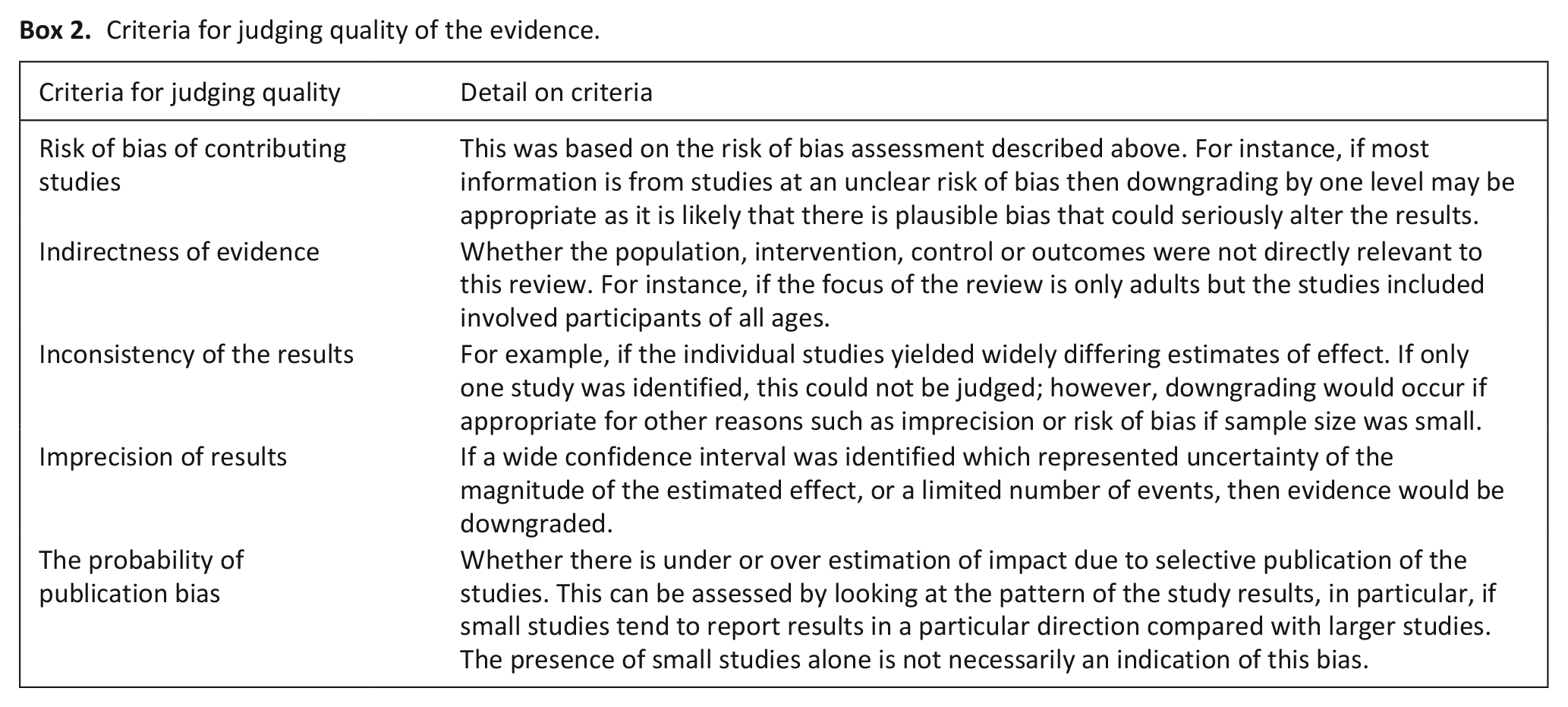
In certain circumstances, for very serious limitations, we adjusted the overall rating by several levels for a particular outcome as recommended by GRADE guidelines. 16 For example, where there were so few data that the results were highly susceptible to the random play of chance.
Judgements were made by one author (B.C.) and checked by another (M.A.). Any disagreements were resolved through discussion, or where necessary, with reference to another author.
Results
The database search yielded 13,304 unique citations. At screening 179 were deemed to be potentially relevant. At full-text we excluded 157. This exclusion was most commonly because the study population not was not at a palliative stage of a disease (n = 46). These included, for example, studies of healthy populations, and patient populations with progressive diseases but not at a palliative stage. Twenty-two RCTs met the inclusion criteria17–38 (Figure 1).
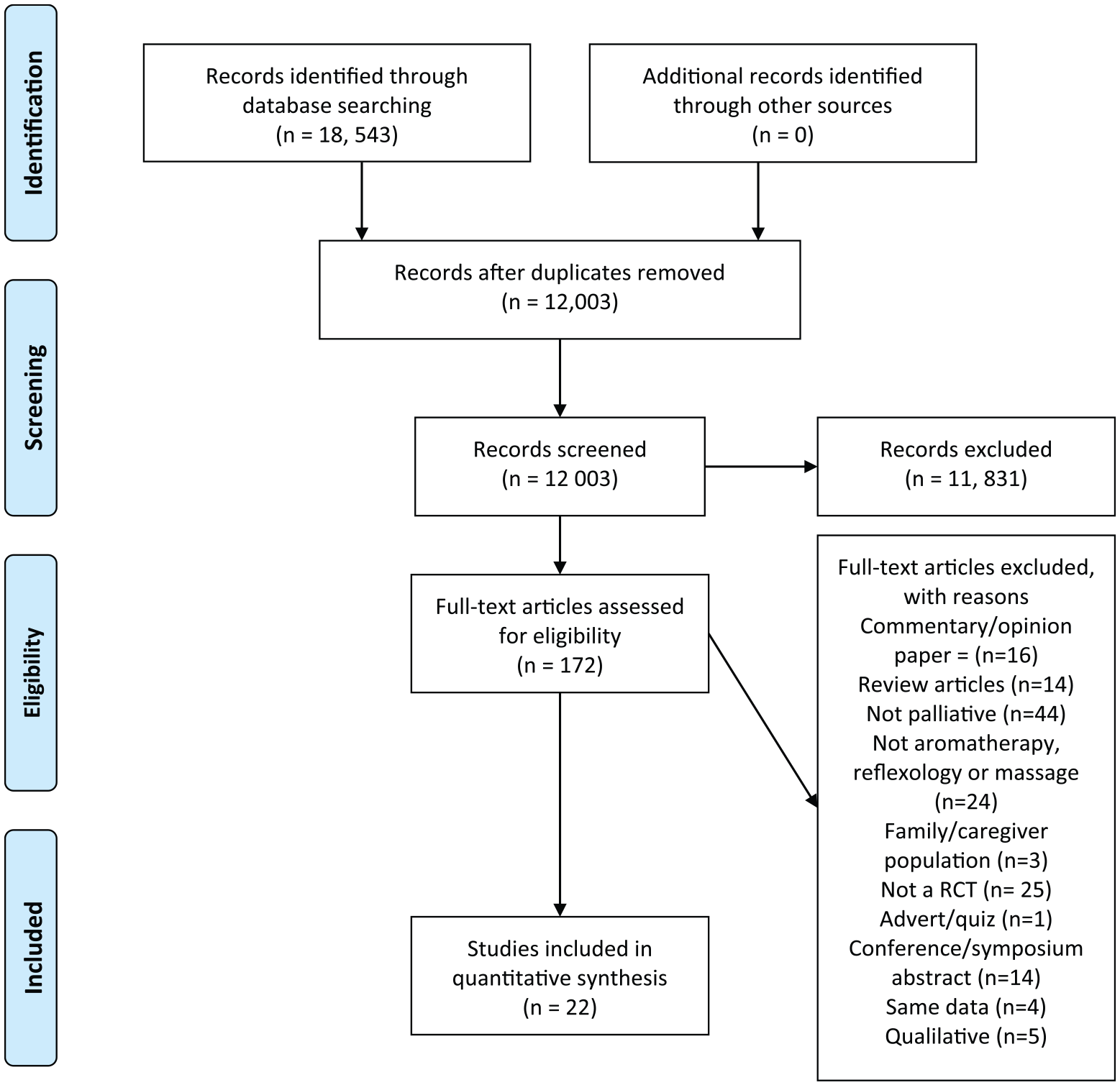
PRISMA flow chart.
Included studies
The included trials involved 1,956 participants, with most (n = 17) having samples of less than 50 participants per trial arm. Eight studies evaluated aromatherapy, 12 massage, and six reflexology. Of these, four compared aromatherapy with massage. Most involved participants with advanced cancer (n = 15). One of the other trials involved participants with end-of-life AIDS, 29 another end-stage renal disease, 17 and five participants with palliative needs with no details on their disease.18,23,24,26,36 Most trials had been conducted in the United States (n = 9) or the United Kingdom (n = 7). Others were conducted in Iran (n = 2), Germany (n = 1), China (n = 1), Poland (n = 1) and Taiwan (n = 1). All trials were published in English. In most of the trials, the main follow-up time point was immediately post intervention (n = 15) (Table 1).
Characteristic of included randomised controlled trials.
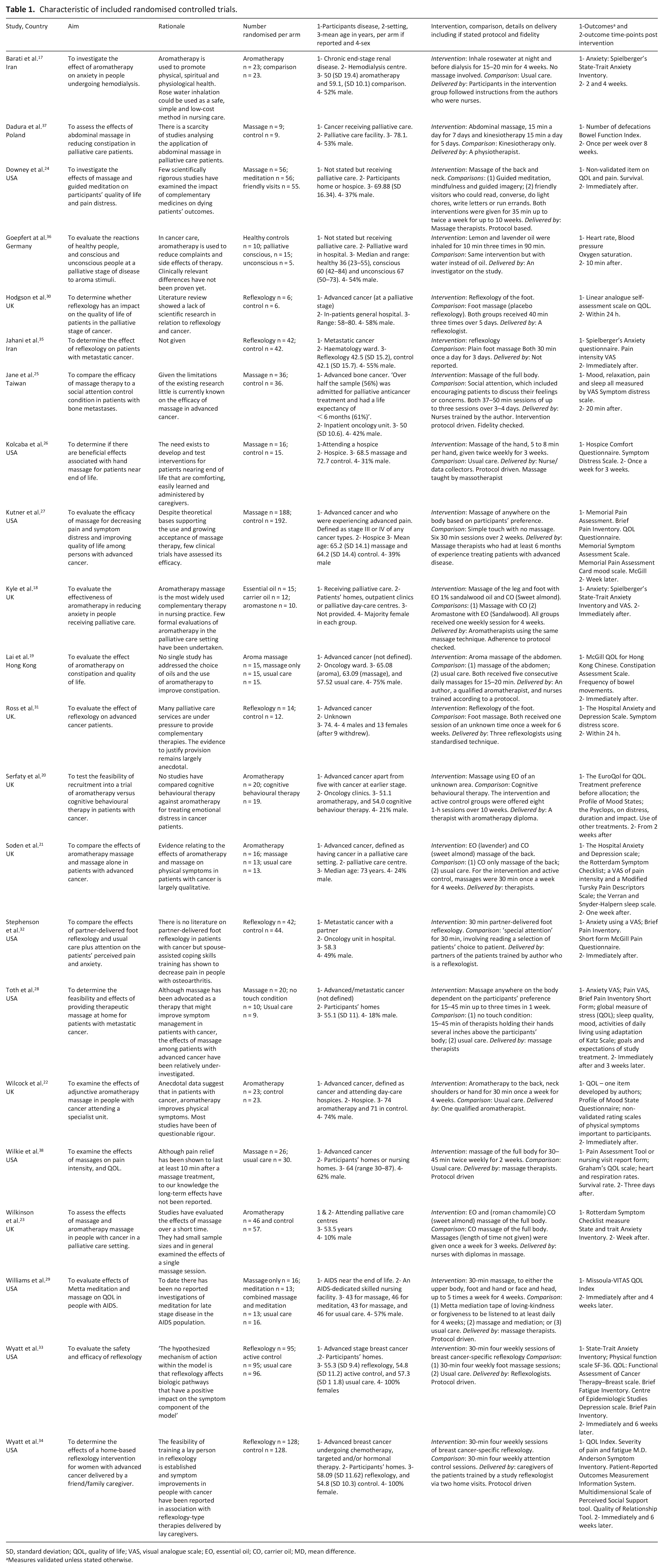
SD, standard deviation; QOL, quality of life; VAS, visual analogue scale; EO, essential oil; CO, carrier oil; MD, mean difference.
Measures validated unless stated otherwise.
For the eight trials involving aromatherapy, two provided this by inhaling oil only.17,36 The other six provided aromatherapy in the form of a massage with essential oils. Sessions ranged from a one-off 10-min session 36 to eight 1-h sessions over 10 weeks. 20 In two, the intervention was delivered at the participants’ homes,17,18 in two in a purpose built unit, such as a hospice.20,22 The other studies did not describe the setting. In five studies, the aromatherapy was delivered by qualified aromatherapists or nurses who had received training;18–20,22,23 in two studies participants administered the intervention themselves (inhaling an aromatherapy oil).17,36 One study did not describe who delivered the intervention. 21 In the 12 trials involving massage, sessions ranged from three 15- to 45-min massages25,28 to a 15-min massage daily for 8 weeks. 37 All of the studies that described the setting were conducted in the participants’ homes.24,28,29,38 Interventions were delivered by massage therapists, other than one study that involved nurses, 25 and one that did not describe the interventionist. 26 In the six reflexology studies, the sessions ranged from a one-off 30-min session 32 to a session a week for 6 weeks. 31 The reflexology was conducted in hospital,30,32,35 at a participants’ homes33,34 and a day-care centre. 31 The reflexology was conducted by trained reflexologists30,31,33 and participants’ caregivers or partners.32,34 One study did not report on this. 35
As listed in Table 1, most studies used validated scales for assessing outcomes. Comparators varied; in eight this was usual care, six a placebo control, two social attention and the others different active interventions.
Risk of bias
All trials were limited in quality (Figure 2). For example, 10 had an unclear risk of bias due to a lack of reporting.17,21,24,28,30–32,36–38 Only, five studies adequately described methods to conceal group allocation, namely by using, for example, sealed packs and opaque envelopes.21,22,27,33,34 Four studies had a high risk of bias as the assessors were not blind.22,24,25,28 Five studies had a high risk due to high attrition rates.18,19,22,37,38 Thirteen studies had a high risk of bias due to small sample size (<50 per trial arm).16–21,24,25,27,29–31,34
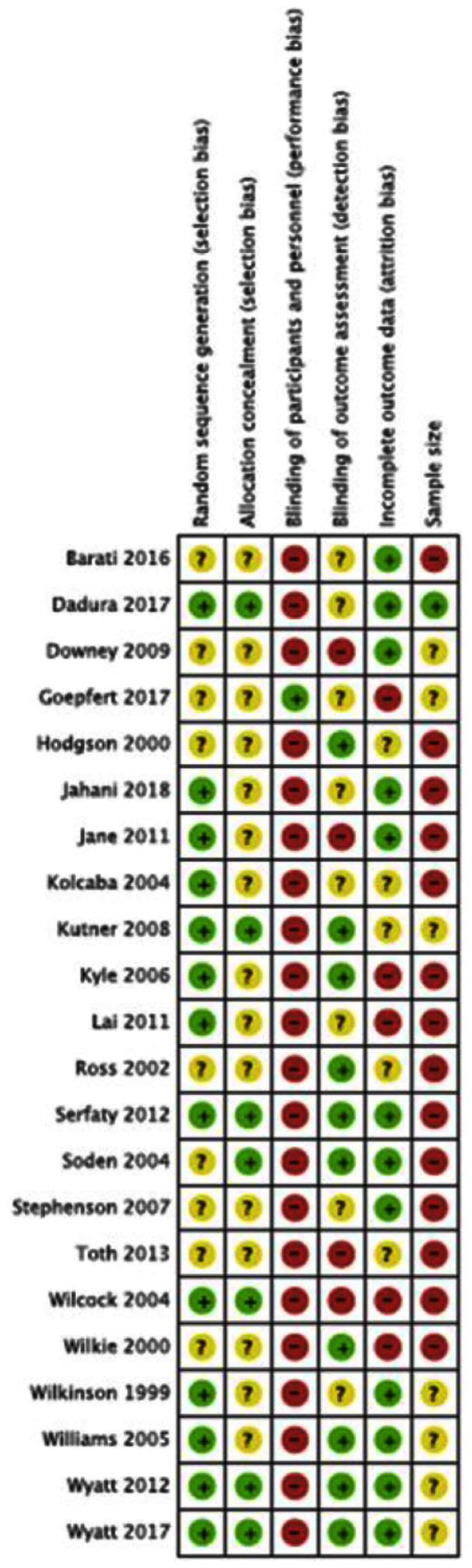
Risk of bias.
Effect of therapies
The use of trial data in this review was limited. Some findings are not reported for six trials because there were baseline differences between trial arms that were not controlled for in all or some of the analyses.17,18,22,23,37,38 In one trial, findings were not reported as it did not assess any of our outcomes of interest. 36 The trial focused on physiological outcomes such as heart rate. We included it because we wanted to document the existence of all trials of these therapies in palliative care. A further limitation on use of the data is that not all trials assessed differential effects between trial arms, instead they reported outcomes within each trial arm, from baseline to follow-up(s). Meta-analyses were not possible because of heterogeneity across the trials in key characteristics including comparators and outcome measurements, and also because data were not provided in an appropriate format.
Aromatherapy
Primary outcomes
One of the eight trials on aromatherapy measured short-term impact on anxiety and pain. 21 In each of its three arms (aromatherapy, massage or no intervention), there was no statistical significant differences in change from baseline in symptoms of anxiety or pain. The trial did not directly measure differential effect between the arms and full data were not reported.
Two trials measured short-term impact on quality-of-life,19,21 and both involved three arms (aromatherapy, massage or no intervention). Neither found a statistically significant differential impact between trial arms at follow-up. Although in one study, for two of the five subscales (social and support) of the McGill Quality-of-Life Scale, there was a statistically significant difference favouring aromatherapy in comparison to the other arms. 19 Neither trial reported full data. We judged as very low the quality of evidence that aromatherapy has no differential impact in the short-term in comparison with massage or no intervention on quality-of-life. This was because of serious study limitations, in that the trials were underpowered to demonstrate effectiveness (small samples of 15–20 per trial arm).
One trial reported an adverse event, a rash following the aroma massage. 22 Three trials reported uneven levels of attrition across trial arms but none provided information about whether the reason for discontinuation was related to the intervention.18,22,23
Secondary outcomes
Two trials measured longer term impact on anxiety.17,20 In one there was no statistically significant difference between trials arms in state or trait anxiety at 2 or 4 weeks. 17 For example, at 2 weeks for state anxiety MD = −0.33; 95% CI = −27.54, 26.88. In the other trial, in both arms, symptoms of anxiety improved at both 3 and 6 months (20). Between-group comparisons at 3 and 6 months were also not statistically significant. Likewise, in this trial, improvements were not statistically different between trial arms with regard to impact on depression, vigour, anger and confusion. No trials measured long-term impact on pain or quality of life.
Two trials evaluated mood.20,22 In both trials, there was an improvement in mood in all trial arms, but no statistically significant difference between the arms: immediately after the intervention between the aromatherapy group and usual care MD = −0.4; 95% CI = −3.4, 2.5; 22 at 2 weeks after the intervention between aromatherapy and the control group of cognitive behavioural therapy MD = 3.00; 95% CI = −12.75, 18.75. 20
In the one trial that evaluated sleep, there was a statistically significant difference favouring the combined groups of massage and aromatherapy compared with the control group who received no intervention (p = 0.04). 21 This trial also measured impact on other symptoms. Using the Rotterdam Symptom Checklist, there were no statistically significant differences in impact on physical or psychological symptoms in any of the arms. Full data were not reported.
One trial measured satisfaction. 22 It reported that all patients were satisfied with receiving aromatherapy and wished to continue. It did not report on satisfaction in the arm receiving usual care.
Massage
Primary outcomes
Two of the 12 trials on massage measured short-term impact on anxiety, neither measured differential effects between trial arms.21,28 In both trials, there were no statistically significant changes in anxiety between baseline and follow-up in all trial arms (massage, aromatherapy, no-touch and usual care). We did not GRADE the evidence as differential effects were not measured.
Five trials measured short-term impact on pain.21,25,27,28 One reported a statistically significant difference favouring massage compared with social attention (MD = −1.60, 95% CI = −2.65, 0.55). 25 In another trial, there was a statistically significant difference favouring massage compared with simple touch (MD = −0.90; 95% CI = −1.19, −0.61). 27 In another two, there was no statistically significant change between baseline and follow-up in all trials arms.21,28 Full data were not provided in either trial. In the fifth trial, there was no statistically significant differential effect in impact on pain between trial arms a week after the end of the intervention (pain intensity MD = 0.20; 95% CI = −0.82, 1.22). 38 We judged as very low the quality of evidence about the effect of massage on pain. We downgraded the score by three levels because of study limitations (small sample size), inconsistency in findings and indirectness (variation in comparison arm).
Five trials assessed short-term impact on quality-of-life.19,21,24,27,28 In four, there was no statistically significant difference in improvement between trial arms.19,21,24,27 In one, this was in comparison with simple touch (MD = 0.08; 95% CI = −0.37, 0.53). 27 The other three did not provide full data. In the fifth, using the McGill scale, there were three outcomes (physical, psychological and total). 28 There was a significant (p = 0.03) difference at 1 week in total quality-of-life score favouring massage compared with the other arms (no touch and usual care), and in physical wellbeing in favour of touch (p = 0.005). Full data were not provided. We judged as very low the quality of evidence about the effect of massage on quality-of-life because of study limitations (small sample size), inconsistency in findings and indirectness (variation in comparison group).
One trial reported on adverse events, stating that there were few, with similar rates per trial arm. 27 None of the adverse events described in this trial or the other two trials that reported on adverse events28,29 appeared to be related to the intervention. Two other trials reported uneven levels of attrition across trial arms but none provided information about whether the reason for discontinuation was related to the intervention.19,38
Secondary outcomes
Two trials measured mood at the end of the intervention.24,26 One found no statistically significant difference between trial arms in mood (MD = −2.40; 95% CI = −7.64, 2.8). 25 The other found statistically significant improvement in the massage group compared with control (simple touch) (MD = 0.61; CI = 95% 0.35, 0.87). 27 One trial measured impact on sleep 28 and found no significant differences between massage, no touch control and usual care after 1 week (p = 0.25) or 1 month (p = 0.49) after the intervention.
Five trials measured impact on other symptoms or measures of well-being.25–28,37 In one trial, comparing abdominal massage and kinesiotherapy (a movement therapy) with kinesiotherapy only, no significant improvement was found in measures of bowel function. 37 Another trial measured relaxation and found no significant difference between trial arms (MD = −1.10; 95% CI = −2.27, 0.07). 25 In one, they found no significant differences between trial arms for comfort and symptoms of distress (symptom distress over time between groups (time × group interaction: F = 0.617, p = 0.548)). 26 In another, they found no significant differences between the trial arms in terms of analgesic use, respiratory and heart rate or symptom distress. 27
One trial involving four arms (meditation, massage, both massage and meditation or standard care) found that the combined group of massage and meditation showed improvements from baseline to 4 weeks after intervention in quality-of-life (p = 0.005) and transcendence (p = 0.01), which were significantly greater (p < 0.05) than improvements in the other groups. 29 Full results were not reported.
No trials measured longer term impact of the interventions on pain or anxiety. No trials reported on satisfaction. Although one reported that patients enjoyed the massage. 31
Reflexology
Primary outcomes
Two of the six trials on reflexology measured short-term impact on anxiety.32,35 In one, the comparison group was sole touching 35 and in the other it was attention control. 32 In one, there was a significant difference favouring those receiving reflexology (RR 5.53, 95% CI 2.16, 14.15). 32 In the other, there was no significant difference between the trial arms (MD = −2.53, 95% CI = −10.18, 5.12). We judged as very low the quality of the evidence on the impact of reflexology on anxiety in the short-term. We downgraded the quality of evidence by three levels because of study limitations (unclear risk of selection bias), imprecision (wide confidence intervals) and inconsistency of findings.
Three trials measured short-term impact on pain.32,34,35 In two, the comparison was attention control32,34 and in the other it was sole touching. 35 In all three, there was a significant difference favouring those receiving reflexology: MD = −3.57, 95% CI = −4.35, −2.79; 34 MD = −0.90, 95% CI = −1.52, −0.28. 33 The other trial did not provide full data. 31 We judged the quality of evidence that reflexology reduced the symptoms of pain in the short-term as low. We downgraded the quality of evidence by one level because of study limitations (sample sizes) and one because data were under reported.
One trial measured short-term impact on quality-of-life. 30 There was a statistically significant difference favouring reflexology compared with placebo reflexology (RR = 4.0; 95% CI = 1.66, 9.64). We judged the quality of evidence that reflexology improved quality-of-life in the short-term as very low. We reduced the quality of evidence by three levels because of very serious study limitations (sparse data).
One trial reported that adverse events occurred in reflexology arm, foot discomfort was mentioned most often. 31 The level of discomfort is not described. There were reports of other symptoms possibly attributable to therapy (e.g. nausea) but the incidence of these were balanced between trials arms.
Secondary outcomes
Three trials measured other symptoms: one study measured symptom distress 31 and two fatigue.33,34 One analysed 10 symptoms. 31 They found no difference between groups apart from a significantly greater improvement in appetite and mobility in the control (foot massage) group compared with reflexology. Full data were not reported. Another found participants reported statistically significantly lower scores on fatigue severity following the massage control (p = 0.02), but not following the reflexology (p = 0.38). 33 The third found significant improvements in symptom severity for reflexology compared with attention control (MD = −4.34; 95% CI = −7.97, −0.71) and in the interference that these symptoms had between 5 and 11 weeks on daily living (MD = −3.69, 95% CI = −6.41, −0.97). 34 No trials measured mood or sleep as outcomes. One study measured the long-term impact of reflexology on anxiety. 33 There was no statistically significant difference at 5 or 11 weeks for reflexology compared with usual care or placebo. This study also measured the long-term impact of reflexology on pain and found no statistically significant difference between arms. Two studies measured the long-term impact of reflexology on quality-of-life.33,34 In both averaged over 5 to 11 weeks, there was no statistically significant difference between reflexology and attention control (e.g. using Quality of Life Index, group coefficients 0.599 (SE = 0.36), p = 0.99). 33
No trials reported on satisfaction. Two reported that patients enjoyed receiving either reflexology or the comparison arm.30,31 None of the trials were at high risk of attrition bias.
Discussion
This systematic review has critiqued the current evidence on aromatherapy, massage and reflexology in palliative care. It included 22 trials involving 1,956 participants. Overall, there was no statistically significant difference between aromatherapy and massage with comparator arms (usual care, active control or another therapy) in terms of short-term effect on anxiety, pain or quality-of-life. There was some evidence, albeit from a small pool of studies (n = 3), that reflexology reduced pain in the short-term.31,33,34 Few adverse events were reported, none of the studies stated that they led to loss to follow-up.21,26–28,30 However, all these findings are limited because of heterogeneity across trials and low quality with many having small sample sizes. The findings should not therefore be regarded as definitive.
To our knowledge, this is the first systematic review specifically examining aromatherapy, massage and reflexology to critically evaluate trial evidence in palliative care populations. Other reviews of complementary therapies in palliative care differ. One, for example, is broader in focus, but without using search terms to identify different complementary therapies. 8
The lack of overall positive effect found is perhaps not surprising given that previous reviews of these therapies in other populations have also failed to find robust evidence on effectiveness. 39 At the same time, qualitative evidence on patients’ perceptions of aromatherapy, massage and reflexology has highlighted that these therapies are highly valued by patients.40–44 It remains a challenge to reconcile the mismatch between qualitative and quantitative findings in this area. The problem may lie in the outcome measures used in the trials being insensitive to what patients value about the therapies. It may also be that previous trials were poorly designed and under-powered and that better trials are needed to assess whether these therapies are truly effective.
Strengths and limitations
Our review followed robust methods, including protocol registration, adherence to standard guidelines, and critiquing of both the trials themselves and the evidence derived. We aimed to locate all available peer reviewed published evidence. We searched nine databases and trial registries. However, grey literature was not specifically searched and therefore potentially relevant studies may have been missed.
We considered whether a reason for the lack of clear differences between the therapies and comparison groups was affected by our choice of primary outcomes. However, there were no other outcomes that were measured in more than one or two of the included trials. There are recognised difficulties in the assessment of complex interventions in palliative care. 45 Seven different quality-of-life measures were used in the trials; highlighting the lack of a gold standard outcome measure in this population and is consistent with previous findings within palliative care research. 46 Moreover, none of the trials used a specific outcome measure for use in patients receiving complementary therapy. Indeed, as far as we are aware, no such outcome measure has been developed.
Our conclusions are also limited by the low quality of the evidence found. Because of this, it is possible that the true effect of the therapies might be different from the estimated effect derived from the included trials. One prominent quality issue was small sample sizes, which is a common issue in palliative care research. 47 Many of the trials in this review were pilot/feasibility studies which never went on to be a full trial with sufficient power to identify a clinically significant effect. The trial characteristics also limited the strength and generalisability of the findings. In most of the studies, the participants had advanced cancer.
Across the studies, there was heterogeneity in characteristics. There were different comparison arms including treatment as usual, attention control and dummy complementary therapies. Using an appropriate comparison arm is important to fully understand the effect of an intervention, especially when it is not possible to blind the interventionist. 48 A control group should not include any of the active components that are present in the intervention. 49 For instance, it is possible that an active component of the complementary therapy may be engaging with the therapist and therefore an attention control group may not necessarily be the best comparator. The review found differences in choice of comparator but cannot make recommendations about the most suitable comparator in future trials. In the trials, the intervention was carried out by nurses or therapists both who had undergone training. It was also undertaken in two by family members who were given training as part of the trial. Such innovation could be very useful to practice, but it brings into question if reflexology can be taught so quickly and without harm, why is reflexology training extensive? Perhaps the potential mechanisms of action in these two trials differ?
Due to the heterogeneity of the study characteristics and the inappropriateness of combining the data, we were unable to conduct any sensitivity analyses (such as on difference in how the intervention was delivered). Research that has explored palliative care patients’ views on aromatherapy, massage and reflexology has reported that participants found that the therapist, the ability to have choices about the therapy, and time to relax were all aspects they valued highly.40–44 This suggests that the active components of the therapies may have been under-explored. Moreover, research design issues, including optimal components of the intervention, are known to be challenging in the evaluation of complex interventions in health care.50,51
Implications for clinical practice and future research
Our review can only draw limited conclusions about the effectiveness of aromatherapy, massage and reflexology, and we are unable to provide new recommendations for practice. However, none of the studies that we identified revealed any major harm to the participants engaging in these therapies. In most, 20/22, harms related to the therapies were not reported, where they were reported they involved following massage foot discomfort or a rash, none resulting in attrition. Combined with our knowledge of the qualitative evidence that finds that complementary therapies are highly valued, we suggest that hospices should continue to offer these therapies as part of their holistic approach at least until definitive research has been conducted.
This review highlights a clear need for more robust research on the effectiveness of aromatherapy, massage and reflexology on outcomes in a palliative population. However, repeating previous trial design risks contributing to waste.52,53 Researchers need to first understand the effective components of the therapies by developing the interventions in consultation with complementary therapists and palliative care patients. More research is needed to develop more appropriate outcome measures which reflect the qualitative experience of palliative care patients receiving complementary therapies. Future research should also consider how the therapies should be delivered and address the issue of what constitutes a suitable comparator arm.
Conclusion
Our review found no evidence of short-term benefits of aromatherapy and massage on quality-of-life, anxiety and pain for people with palliative care needs. For reflexology, some positive outcomes were found, but all conclusions were limited by the primary studies’ low quality and of the inability to conduct a meta-analysis. Further rigorous research is needed using appropriate outcome measures. While there was limited evidence on the effectiveness of the complementary therapies, there was no evidence of harm; therefore, we suggest hospices continue to provide complementary therapies while further research is undertaken.
Supplemental Material
Supplementary_materials – Supplemental material for The effectiveness of aromatherapy, massage and reflexology in people with palliative care needs: A systematic review
Supplemental material, Supplementary_materials for The effectiveness of aromatherapy, massage and reflexology in people with palliative care needs: A systematic review by Bridget Candy, Megan Armstrong, Kate Flemming, Nuriye Kupeli, Patrick Stone, Victoria Vickerstaff and Susie Wilkinson in Palliative Medicine
Footnotes
Acknowledgements
We would like to thank our service representatives, Judy Booth and Jill Preston, and lay representatives, Rose Amey and Veronica Maclean, for their involvement and support with this project. We also acknowledge the support of the UCLH BRC (Biomedical Research Centre).
Author contributions
B.C., N.K., P.S., S.W. and K.F. obtained funding for this research project. B.C., M.A., N.K. and S.W. undertook study selection. B.C. and M.A. contributed to data extraction and analysis and interpretation and drafted the initial manuscript. V.V. contributed to the analysis and interpretation of the data. All authors contributed to study design, critically reviewed and revised the manuscript and approved the final manuscript for submission.
Data management and sharing
Data will be made available upon request.
Research ethics and patient consent
As a systematic review and meta-analysis, the study did not directly involve human participants and required no approval from an Ethics Committee or Institutional Review Board.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work and Megan Armstrong’s post was supported by Marie Curie (grant number MCRGS-07-16-36). Professor Paddy Stone post is supported by Marie Curie Chair’s grant (509537). Bridget Candy and Vicky Vickerstaff post is supported by MCCC-FCO-16-U. Nuriye Kupeli is supported by Alzheimer’s Society Junior Fellowship grant (Grant award number: 399 AS-JF-17b-016).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.