
Abstract
Background:
Studies evaluating the impact of prognostication in advanced cancer patients vary in the outcomes they measure, and there is a lack of consensus about which outcomes are most important.
Aim:
To identify outcomes previously reported in prognostic research with people with advanced cancer, as a first step towards constructing a core outcome set for prognostic impact studies.
Design:
A systematic review was conducted and analysed in two subsets: one qualitative and one quantitative. (PROSPERO ID: CRD42022320117; 29/03/2022).
Data sources:
Six databases were searched from inception to September 2022. We extracted data describing (1) outcomes used to measure the impact of prognostication and (2) patients’ and informal caregivers’ experiences and perceptions of prognostication in advanced cancer. We classified findings using the Core Outcome Measures in Effectiveness Trials (COMET) initiative taxonomy, along with a narrative description. We appraised retrieved studies for quality, but quality was not a basis for exclusion.
Results:
We identified 42 eligible studies: 32 quantitative, 6 qualitative, 4 mixed methods. We extracted 70 outcomes of prognostication in advanced cancer and organised them into 12 domains: (1) survival; (2) psychiatric outcomes; (3) general outcomes; (4) spiritual/religious/existential functioning/wellbeing, (5) emotional functioning/wellbeing; (6) cognitive functioning; (7) social functioning; (8) global quality of life; (9) delivery of care; (10) perceived health status; (11) personal circumstances; and (12) hospital/hospice use.
Conclusion:
Outcome reporting and measurement varied markedly across the studies. A standardised approach to outcome reporting in studies of prognosis is necessary to enhance data synthesis, improve clinical practice and better align with stakeholders’ priorities.
Keywords
Currently, there is no gold standard for evaluating how different methods of prognosticating in advanced cancer impact on patient care.
Prognostic models are principally evaluated by their statistical performance, determining their discrimination and calibration. However, before any prognostic model can be recommended for use in clinical practice, it is necessary to demonstrate whether or not it has a beneficial impact on patient care.
There is a lack of consensus among stakeholders about how to assess the impact of prognostication in advanced cancer, with prognostic studies varying in the outcomes they select.
We identified a wide variety of outcomes and measures used in published studies, which makes inter-study comparability problematic.
Our findings highlight the widespread effect that prognostication in advanced cancer has on patients and informal caregivers.
The lived experiences of patients and informal caregivers regarding prognostication in advanced cancer are not always represented in the outcomes quantitative prognostic studies measure.
Further research is needed to identify and prioritise outcomes to measure the impact of prognostication in advanced cancer.
Patients’ and informal caregivers’ experiences and perspectives should always be incorporated when evaluating the impact of prognostication.
Outcome selection in prognostication studies needs to be more consistent and standardised.
Introduction
Prognostication of a person’s likely length of life is a vital component of palliative care, patient care and decision-making.1,2 Accurate prognoses aim to provide patients, their families and informal caregivers with sufficient time to prepare for the end-of-life such as making financial plans and identifying their preferences for place of death. 3 Accurate prognoses also enable clinicians to identify appropriate treatment strategies based on individual patient's prognostic factors and symptoms. 2 Conversely, inaccurate prognoses of end-of-life can damage patients' psychological wellbeing and sense of hope.4–6
No method of prognostication is completely accurate. In daily practice, prognostication about end-of-life is often a clinical estimate based on clinicians’ skills and experiences. 3 However, clinicians' estimates are often inaccurate, inconsistent and over-optimistic.7,8 Various prognostic tools have been validated for use in people with advanced cancer, but none has yet demonstrated clearly superior discrimination, calibration or accuracy over clinicians’ predictions. 3 It is possible that methods of prognostication may vary in other respects, such as ease of use or interpretation. However, the comparative impact of different prognostic methods has yet to be established, and variation in outcome reporting among studies makes it difficult to distinguish the impact of different methods of prognosticating with similar levels of accuracy.
Developing a standardised set of outcomes is integral to improving the consistency of reporting of outcomes, inter-trial comparisons and informing clinical decision-making in the context of prognostication in advanced cancer. 9 Such guidance for outcome reporting in prognostic studies does not exist, and no systematic review has been conducted to explore the extent of variation in outcomes reported in prognostic studies. Our review aimed to identify studies reporting on all outcomes or experiences of prognostication in advanced cancer, as a first step in developing a core outcome set for use in future prognostic impact studies. We sought therefore to include the broadest possible range of studies, so as not to pre-emptively exclude any potentially relevant outcomes in advance of testing with stakeholders.
We analysed the results of this systematic review in two subsets, exploring: (1) quantitative studies of the impact of end-of-life prognostication in advanced cancer; (2) qualitative studies of patient and informal caregiver experiences and perspectives.
The main review question was:
What outcomes for end-of-life prognostication in advanced cancer have been identified in research studies to date?
The subsidiary review questions were:
What quantitative outcomes are measured in studies of advanced cancer where survival estimates are provided?
What are patients and informal caregivers’ qualitative experiences and perceptions of prognostication in advanced cancer?
Methods
This systematic review was conducted according to the Cochrane Handbook for Systematic Reviews of Interventions 10 and reported as per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. 11 The protocol was registered prospectively on the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42022320117, 29/03/2022, https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022320117).
We were aware that papers reporting on studies of populations relevant to our study aim might be heterogeneous in the populations they included. We therefore formulated a term and a working definition to encompass all relevant populations, so as to ensure that all papers with potentially relevant participants were included, and none excluded due to an over-narrow definition. Informed by previously published papers,12–18 we decided on the term ‘advanced cancer patients’, meaning individuals diagnosed with a cancer in the advanced stages (metastatic, locally advanced or recurrent). Studies including any patients who were receiving treatment or care without curative intent (i.e. with the objective being to improve symptoms and quality of life, and/or slow disease progression, but not to cure the cancer) were eligible for inclusion.
Eligibility criteria
Eligibility criteria are shown in Table 1. Papers were screened for study type rather than using limits to restrict the results. Where only abstracts were found, we contacted authors for a published article.
Eligibility criteria.
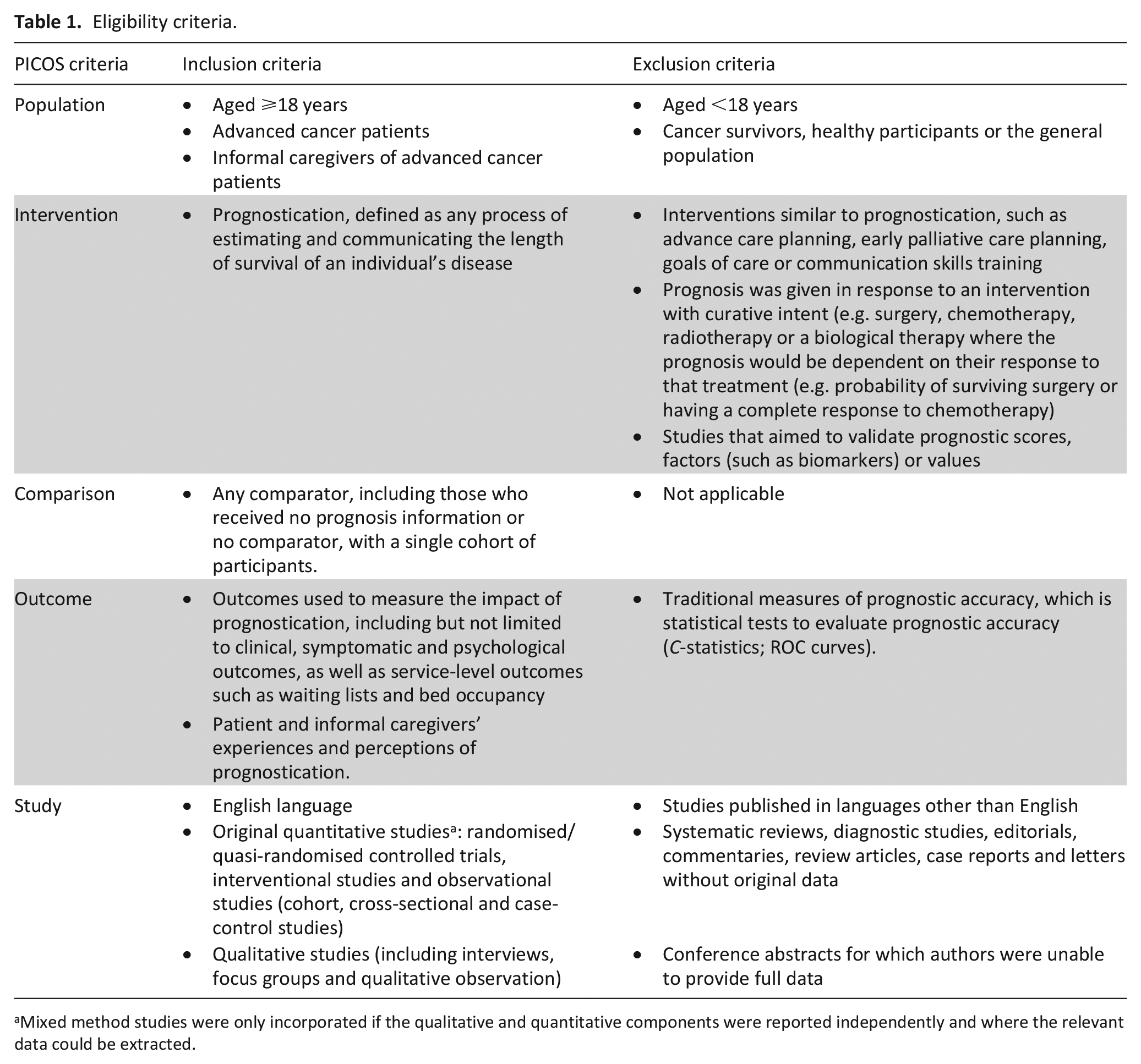
Mixed method studies were only incorporated if the qualitative and quantitative components were reported independently and where the relevant data could be extracted.
We piloted the screening process prior to full data extraction. The piloting confirmed that studies’ descriptions of their samples varied considerably. We therefore decided that, for studies to be eligible for inclusion, if papers did not specify that the population was in the advanced stages of disease, the sample description should include one or more of the following:
Life-limiting
Terminal
Palliative
End-of-life
Deceased, where cancer was the primary cause of death
Connected to a palliative care team, service, unit or hospice
Predicted prognosis of ⩽12 months or a ‘poor’ prognosis
Survival time at most 9 months
Information sources
MEDLINE, EMBASE, PsycINFO, CINAHL, the Cochrane Controlled Register of Trials and the Cochrane Central Register were searched from inception to September 2022. Search limits were applied to restrict results to a human, adult population and studies published in English language only due to limitations in resources.
The search included trials registered at ClinicalTrials.gov and The International Clinical Trials Registry Platform Search Portal. Grey literature searches were conducted using OpenGrey and ProQuest-Digital Dissertations and Theses. Finally, study references of included studies were searched forward and backward.
Search strategy
Keywords related to prognostication, palliative care, advanced cancer and outcomes and cognate terms were included in the search strategy (Supplemental Appendix 1).
Selection process
Search results were imported into the software Rayyan 19 and de-duplicated. Four authors (CS, AB, GR and PXK) independently screened titles and abstracts against eligibility criteria. Those that met the inclusion criteria for either review question were read in full by at least two authors. Discrepancies were resolved through discussion between authors. If no consensus could be reached, a third author was consulted.
Data collection process and data items
Four authors (CS, AB, GR and PXK) extracted key information (author/s, year of publication, geographical setting, methodology, sample size, population, study setting, data collection methods, data describing outcomes of prognostication) from eligible studies using a data extraction form (Supplemental Appendix 2) designed by CS and piloted by four authors (CS, AB, GR and PXK) on a random sample of five studies before being fully implemented.
Study quality assessment
The Mixed Methods Appraisal Tool (MMAT) was used to assess the quality of included studies. 20 This tool is useful for systematic reviews of studies of mixed methodology because it enables critical appraisal of all study methodologies, including randomised and nonrandomised. 20 It also includes criteria for critically appraising mixed methods studies, which are lacking in other tools. For each included study, the authors chose the appropriate category of studies (qualitative, quantitative or mixed methods) and rated the criteria of the chosen category using the following responses: ‘yes’, ‘no’ or ‘can’t tell’. The number of ‘yes’ responses for each study were aggregated, to provide an overview of the scores for methodological quality of the current literature. The aim of the review was to comprehensively identify and synthesise outcomes reported in extant studies; therefore, we did not exclude studies on the basis of quality.
Synthesis methods
We anticipated heterogeneity of included studies and therefore decided that a narrative synthesis was the most appropriate method for synthesising findings. We summarised study characteristics using descriptive statistics.
A table of quantitative outcomes was generated, including descriptions of outcomes, measures and frequency of reporting. Outcomes were categorised using the taxonomy for core outcome sets recommended by COMET. 21 This taxonomy consists of five core areas: (1) death; (2) physiological/clinical; (3) life impact; (4) resource use and (5) adverse events. A narrative description was provided for each outcome.
Relevant findings from qualitative studies are not necessarily presented in ways which translate directly to the COMET taxonomy. We therefore identified themes from these qualitative study findings, which we then categorised by COMET areas and domains. CS performed a thematic synthesis using NVivo version 11, 22 extracting data from verbatim quotes provided in the included studies and supporting author interpretations. The synthesis had three stages: 23 (1) coding data pertaining to patient and informal caregiver experiences and perceptions of prognostication; (2) grouping codes into descriptive themes and (3) developing analytical themes using the COMET taxonomy 21 as a framework, to enable later combination of results of both sets of studies. We produced a narrative description of each theme in relation to the review question, to support our thematic analysis and allocation of themes to COMET taxonomy areas and domains. Any disparities or discrepancies that arose at any stages of thematic synthesis were resolved through discussion and consensus with other authors.
Results
Study selection
The search returned 8075 results. Following de-duplication, we screened 5906 records by title and abstract against the eligibility criteria, and 65 of these were potentially eligible. After reading these articles in full-text, 42 fulfilled the inclusion criteria: 32 quantitative, 6 qualitative and 4 mixed-methods. Figure 1 summarises the study selection process. 11
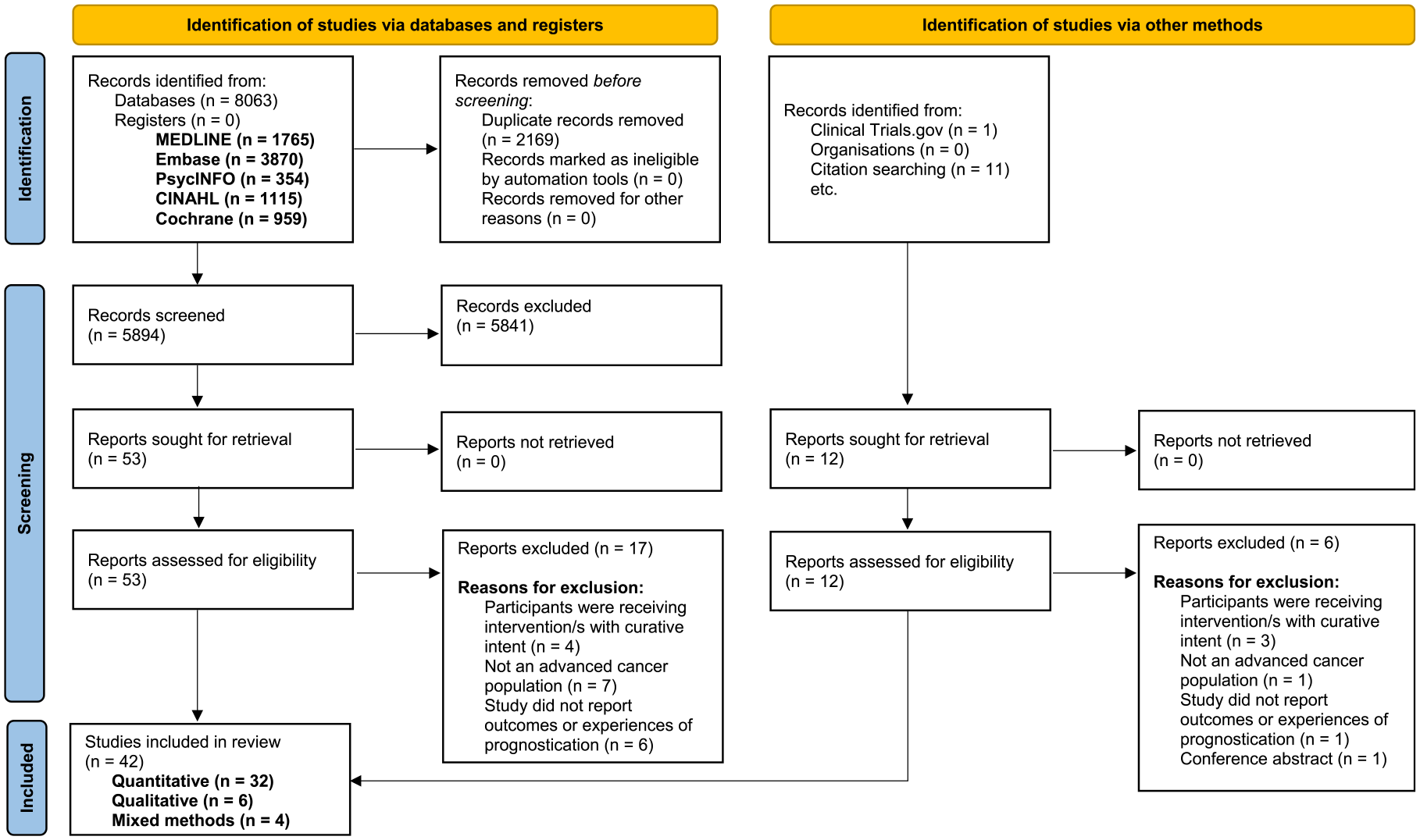
PRISMA flow diagram.
Study characteristics
Table 2 summarises the characteristics of included studies. Studies most frequently came from the United States of America (USA; n = 13) and Taiwan (n = 9). Sample sizes ranged from 14 to 3445. Many studies (n = 27) included patients only, 8 included patients and informal caregivers and 7 included informal caregivers only.
Characteristics of included studies.
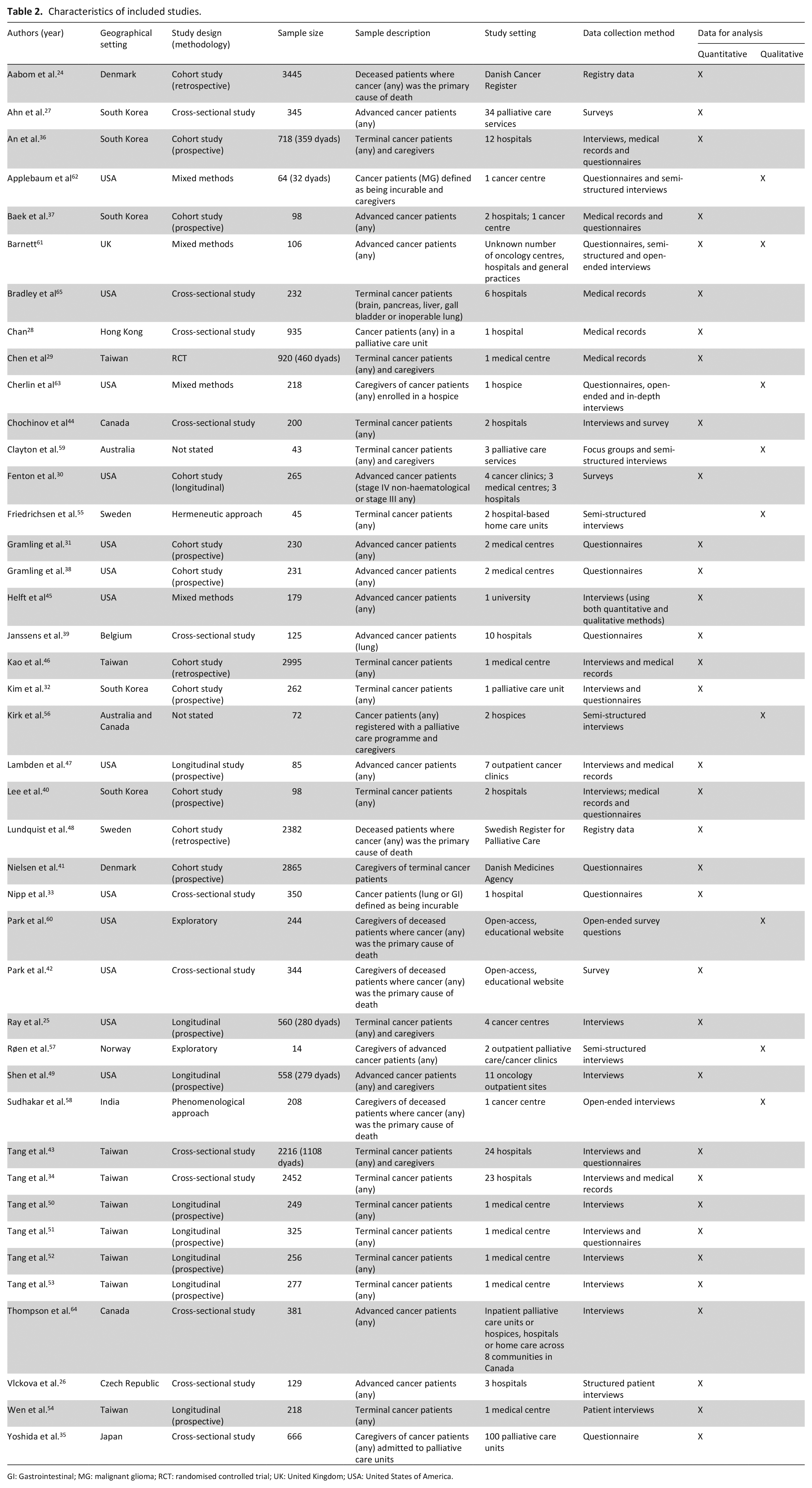
GI: Gastrointestinal; MG: malignant glioma; RCT: randomised controlled trial; UK: United Kingdom; USA: United States of America.
Methodological quality
We assessed the quality of the 32 quantitative studies as high in 12 studies,24 –35 moderate in 9,36–43 and low in 11.44 –54 We assessed the quality of the six qualitative studies as high in four,55–58 and moderate in two.59, 60 We assessed the quality of the four mixed methods studies as moderate in one, 61 and low in the remaining three.62–64 The quality assessments are summarised in Supplemental Appendix 3.
Results of quantitative synthesis
Of 42 studies identified, 34 reported on outcomes used to measure impact of prognostication in advanced cancer.24–40,42–54,61,64–66 From quantitative data, 58 outcomes of prognostication were identified. Table 3 lists identified outcomes.
Outcomes and measures of prognostication in advanced cancer identified in the quantitative data, according to the core areas and domains within the COMET taxonomy.
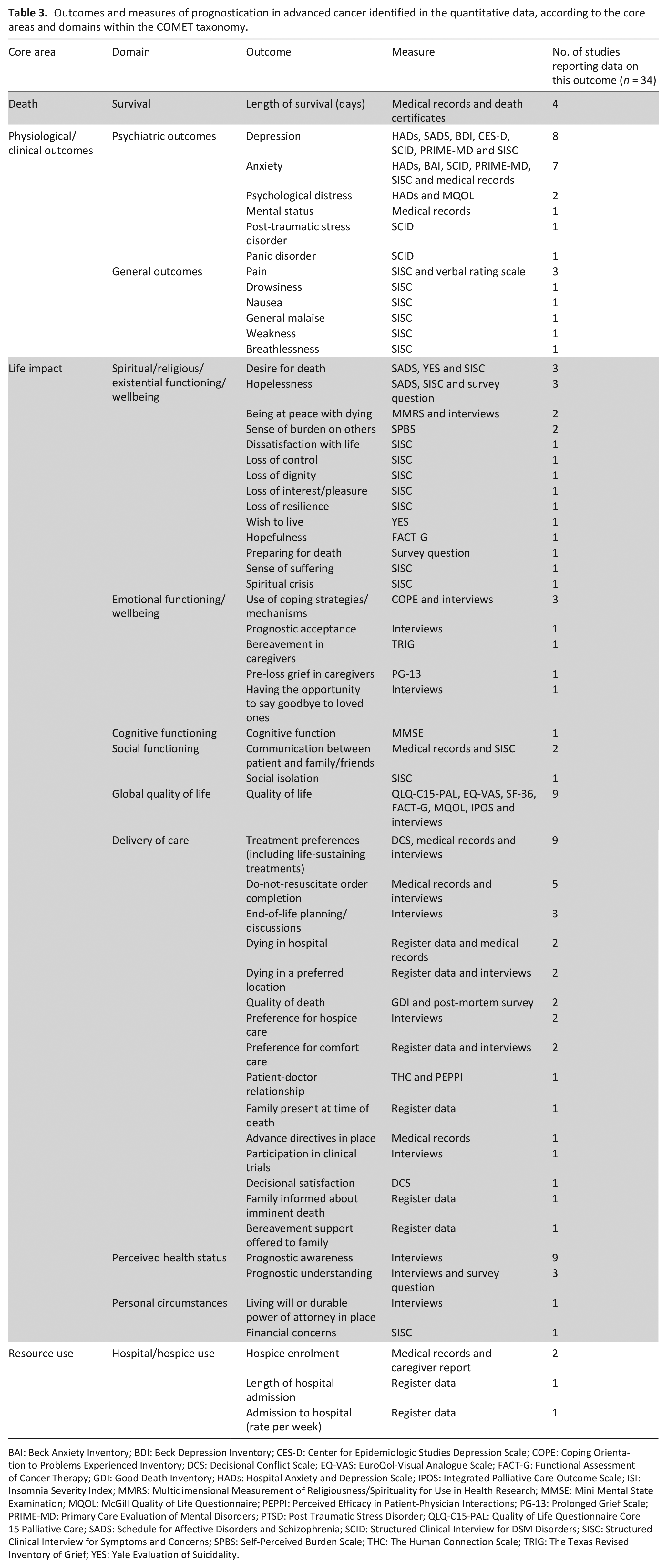
BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; CES-D: Center for Epidemiologic Studies Depression Scale; COPE: Coping Orientation to Problems Experienced Inventory; DCS: Decisional Conflict Scale; EQ-VAS: EuroQol-Visual Analogue Scale; FACT-G: Functional Assessment of Cancer Therapy; GDI: Good Death Inventory; HADs: Hospital Anxiety and Depression Scale; IPOS: Integrated Palliative Care Outcome Scale; ISI: Insomnia Severity Index; MMRS: Multidimensional Measurement of Religiousness/Spirituality for Use in Health Research; MMSE: Mini Mental State Examination; MQOL: McGill Quality of Life Questionnaire; PEPPI: Perceived Efficacy in Patient-Physician Interactions; PG-13: Prolonged Grief Scale; PRIME-MD: Primary Care Evaluation of Mental Disorders; PTSD: Post Traumatic Stress Disorder; QLQ-C15-PAL: Quality of Life Questionnaire Core 15 Palliative Care; SADS: Schedule for Affective Disorders and Schizophrenia; SCID: Structured Clinical Interview for DSM Disorders; SISC: Structured Clinical Interview for Symptoms and Concerns; SPBS: Self-Perceived Burden Scale; THC: The Human Connection Scale; TRIG: The Texas Revised Inventory of Grief; YES: Yale Evaluation of Suicidality.
Death
The core area of death consisted of one outcome domain: survival.
Survival
Four studies reported length of survival, measured in days27,32,40,44 most frequently measured using medical records (n = 3), apart from one study which used patients’ death certificates to confirm length of survival (n = 1).
Physiological/clinical outcomes
The core area of physiological/clinical outcomes consisted of two outcome domains: psychiatric outcomes and general outcomes.
Psychiatric outcomes
The most frequently reported outcomes in this domain were depression and anxiety. Eight studies reported depression, seven in patients25,33,39,40,44,61,64 and one in informal caregivers. 42 In the eight studies, the Hospital Anxiety and Depression Scale (HADS) was the most common measure (n = 3). Anxiety was reported in seven studies.25,28,33,39,40,61,64 Like depression, anxiety was most frequently measured using HADS (n = 3).
Other psychiatric outcomes included psychological distress (feeling depressed, anxious, sad, nervous or worried) (n = 2),25,34 mental status (n = 1), 27 post-traumatic stress disorder (n = 1) 25 and panic disorder (n = 1). 25
General outcomes
The most frequently reported general outcome was pain (n = 3 studies).40,44,64 This outcome was measured using the Structured Clinical Interview for Symptoms and Concerns (SISC) and numerical rating scales. Other general outcomes were drowsiness (n = 1), nausea (n = 1), general malaise (n = 1), weakness (n = 1) and breathlessness (n = 1). 64
Life impact
This consisted of eight outcome domains: spiritual/religious/existential function/wellbeing, emotional functioning/wellbeing, cognitive functioning, social functioning, global quality of life, delivery of care, perceived health status and personal circumstances.
Spiritual/religious/existential functioning/wellbeing
The most frequently reported outcomes for the domain of spiritual/religious/existential functioning/wellbeing were desire for death and hopelessness. Desire for death was reported in three studies,25,44,64 measured via the Schedule for Affective Disorders and Schizophrenia (SADS) scale, the Yale Evaluation of Suicidality (YES) and the SISC. Hopelessness was also reported in three studies,35,44,64 measured via the SADS scale, the SISC and a survey question. Other outcomes included being at peace with dying (n = 2),25,42 sense of burden on others (n = 2),51,64 the wish to live (n = 1), 25 dissatisfaction with life (n = 1), 64 loss of control (n = 1), 64 loss of dignity (n = 1), 64 loss of interest/pleasure (n = 1), 64 loss of resilience (n = 1), 64 hopefulness (n = 1), 45 preparing for death (n = 1), 35 sense of suffering (n = 1) 64 and spiritual crisis (n = 1). 64
Emotional functioning/wellbeing
The most frequently reported outcome in this domain was use of coping strategies/mechanisms, reported in three studies33,39,45 and measured using the Coping Orientation to Problems Experienced (COPE) inventory and patient interviews.
Other emotional functioning/wellbeing outcomes were prognostic acceptance (n = 1), 64 bereavement in caregivers (n = 1), 42 pre-loss grief in caregivers (n = 1) 67 and having opportunity to say goodbye to loved ones (n = 1). 42
Cognitive functioning
Only one study reported cognitive function, defined as any cognitive impairment or decline, as an outcome of prognostication, measured using the Mini Mental State Examination (MMSE). 40
Social functioning
Two studies reported outcomes in this domain, one of which was communication difficulties between patients and family/friends,28,64 measured using patients’ medical records and SISC. One study also reported on social isolation as an outcome of prognostication, measured using SISC. 64
Global quality of life
Quality of life was reported in nine studies.25,26,32,33,39,40,43,51 MQOL was the most common measure used in four of the studies.
Delivery of care
The most frequently reported outcome in this domain was treatment preferences, including preference to receive life-sustaining treatments such as cardiopulmonary resuscitation, intensive care unit, mechanical ventilation, tube feeding, ‘heroic’ measures, chemotherapy and antibiotics. Nine studies reported on patients’ and informal caregivers’ preferences regarding life sustaining treatments post-prognostication.25,29,34,37,38,47,50,54,65 This outcome was measured most frequently via interviews with patients or informal caregivers (n = 5), followed by medical record reviews (n = 4). Similarly, do-not-resuscitate order completion was reported in five studies,25,46,47,49,65 measured via interviews with patients or informal caregivers (n = 3) and patients’ medical records (n = 2). End-of-life planning/discussions were reported as outcomes of prognostication in three studies,25,47,52 ascertained from interviews with patients or informal caregivers.
Other outcomes of delivery of care were patient-doctor relationship (n = 1), 30 dying in hospital (n = 2),24,38 dying in a preferred location (n = 2),38,67 quality of death (n = 2),25,27 preference for hospice care (n = 2),34,36 preference for comfort care (n = 2),34,48 having family present at time of death (n = 1), 48 having advance directives in place (n = 1), 65 participation in clinical trials (n = 1), 47 decisional satisfaction (n = 1), 37 family being informed about patient’s imminent death (n = 1) 48 and bereavement support being offered to family (n = 1). 48
Perceived health status
Prognostic awareness, defined as the awareness of shortened life expectancy, was reported as an outcome in nine studies.25,26,32,43,45–47,51,54 All studies measured this by interviewing patients. Prognostic understanding refers to the perception of prognosis and was reported in three studies (n = 3) measured by interviews and survey questionnaires.34,39,49
Personal circumstances
These were defined as outcomes relating to patients’ finances, home and environment. 21 One study (n = 1) ascertained whether knowing their prognosis affected if patients had a living will or durable power of attorney in place (measured through interviews). 25 Another study (n = 1) reported the outcome of financial concerns, 64 measured via the SISC.
Resource use
This area consisted of one outcome domain: hospital/hospice use.
Hospital/hospice use
The most frequently reported outcome of this domain was hospice enrolment, reported by two studies (n = 2).31,38 This outcome was measured via informal caregiver reports and patients’ medical records.
One study (n = 1) reported admission to hospital (rate per week) as an outcome, as well as length of hospital admission (in days). 24 Both outcomes were ascertained from national register data.
Results of qualitative synthesis
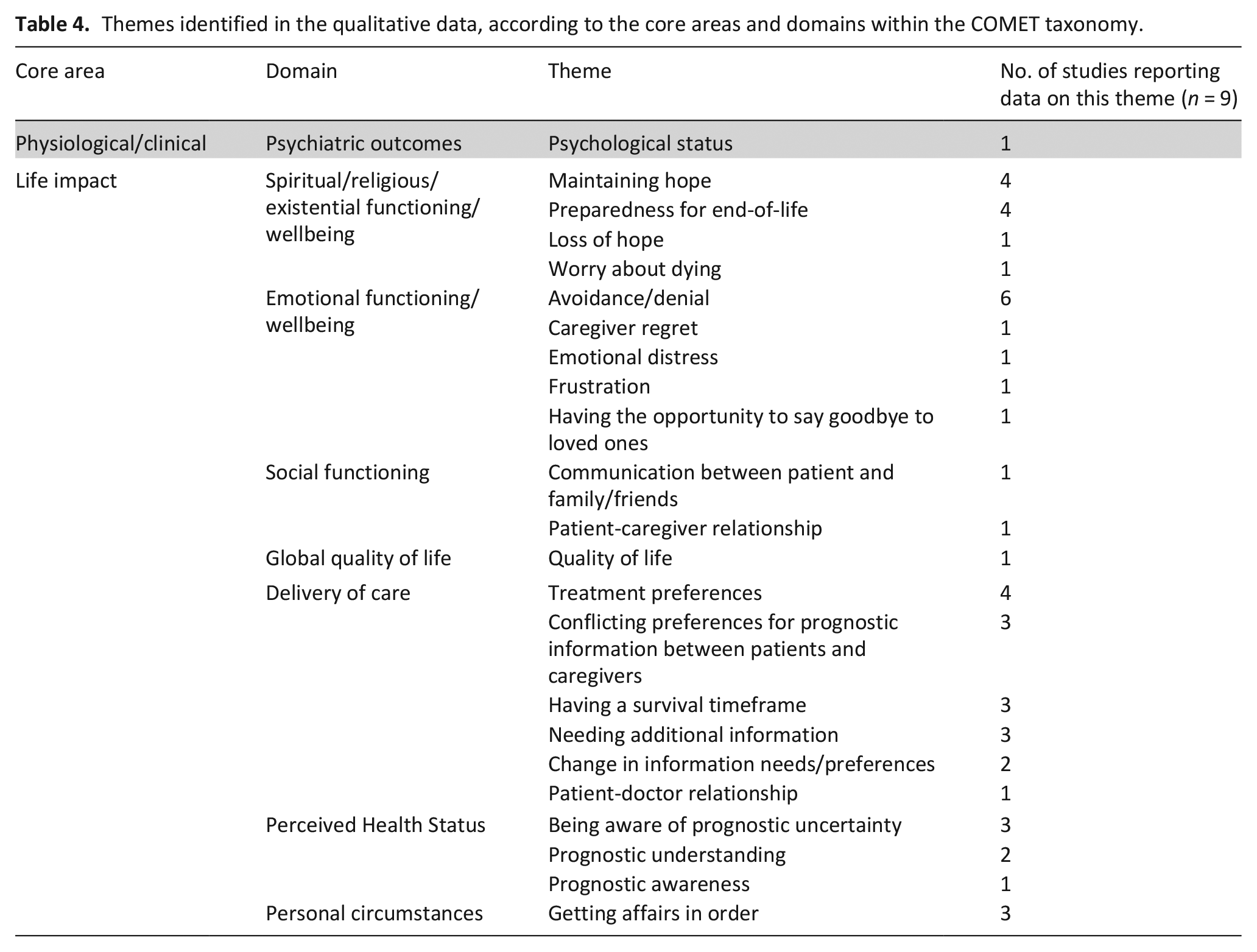
Nine studies provided qualitative evidence on patients’ and informal caregivers’ experiences and perceptions of prognostication in advanced cancer.55–63 Across the qualitative data, 23 outcomes of prognostication were identified. Table 4 shows the themes identified in the qualitative data. Additional quotations are presented in Supplementary Appendix 4.
Themes identified in the qualitative data, according to the core areas and domains within the COMET taxonomy.
Physiological/clinical outcomes
Psychiatric outcomes
One study described patients’ and informal caregivers’ experiences of prognostication in association with psychological status.
58
Not knowing their prognosis evoked uncertainty in some patients, which in turn affected their psychological state. However, awareness of prognosis was also noted to affect patients psychologically: He was aware of his prognosis. But during the final week he slipped into depression suddenly and the final two days were the worst (Informal caregiver, page 115).
58
Life impact
Spiritual/religious/existential functioning/wellbeing
Seven studies identified spiritual/religious/existential functioning/wellbeing experiences associated with prognostication. Themes were developed in relation to maintaining hope,55,56,60,62 preparedness for end-of-life,55,57,58,60 loss of hope, 56 control, 56 and worry about dying. 61
It was clear from narratives that many patients and informal caregivers, while aware of the limited life expectancy, had a continuing need for hope. This need was intertwined with their experience of prognostic disclosure, where it was generally felt that the mode and manner of communication of prognosis should maintain hope. For example, one patient described their desire for ‘a little bit of hope’, regardless of their prognosis.
56
Conversely, others avoided specific prognostic discussions in order to preserve hope: I don’t know how much time (the patient) has left. We always approach things, every therapy, with the notion of hope, that it will either control or hopefully cure his condition. (Informal caregiver, page 820).
62
Linked to this, one study highlighted how prognostic information could also produce loss of hope in patients: [The doctor] is not God so he can’t say exactly you have six months. I think he gave away hope. In dad’s eyes I can see that he lost a bit of hope. (Informal caregiver, page 5).
56
Study findings were mixed on how prognostication affected patients’ and informal caregivers’ preparedness for end-of-life.55,57,58,60 In general, patients and informal caregivers were prepared for end-of-life because they were fully informed of their prognosis, whilst a lack of prognostic information impacted negatively on informal caregivers’ preparedness, such as funeral arrangements.
Finally, prognostication evoked worries about dying in some patients, with concerns about ‘what will happen at the end,’ such as when and how they might die and who might find them. 61
Emotional functioning/wellbeing
Six studies discussed this theme in relation to experiences of avoidance/denial,55,56,60 –63 caregiver regret, 60 emotional distress, 56 frustration, 61 and having the opportunity to say goodbye to loved ones. 60
Prognostication had a profound effect on patients and informal caregivers who had to come to terms with limited life expectancy, which could produce emotional distress
56
and frustration.
61
Information around prognosis evoked frustration in some patients, with one, in particular, stating that they had ‘still lots of things’ they wanted to achieve.
61
Similarly, some prognostic information, particularly about palliative care referral, caused emotional distress: And she said I have come to talk to you about palliative care, and he just went into an absolute heap. And of course, that word when you say ‘palliative care’ he immediately thought death in three months. He just went into absolute shock—burst into tears. . . It was too soon. (Informal caregiver, page 5).
56
Patients and informal caregivers mitigated the emotional impact of prognostication by avoiding information about their prognosis or denying the implications of the information they received.55,56,60 –63 Reasons for avoidance included being ‘too scared to ask’ 61 and to preserve hope.
Avoidance was not always preferable, however, and some informal caregivers wished that they had received prognostic information sooner. Others misunderstood prognostic information, leading to regrets. Some informal caregivers voiced regrets for not using their remaining time with their loved ones better due to not receiving prognostic information earlier: Maybe we could have changed our discussions from the fight and the forward thinking of what we’ll do next, to what needed to be said to each other right then, right when our last few conversations meant the most. (Informal caregiver, page 1474).
60
Similarly, one informal caregiver expressed a desire to have known their loved one's prognosis sooner so that they could have had the opportunity to say goodbye. 60
Social functioning
Two studies observed an association between prognostication and social functioning.56, 57 The patient-caregiver relationship was affected by not discussing impending death: We haven’t talked about death, for example. . .And not having those kind [sic] of talks has affected our relationship. . . (Informal caregiver, page 1415).
57
There was also evidence that communication changed between patients and informal caregivers, who, after receiving the prognosis, no longer communicated openly with each other. 56
Global quality of life
One study highlighted the benefit for patients’ quality of life of having an indication of potentially increased life expectancy rather than no prognosis at all: Her oncologist said to her, ‘I want to continue with the treatment, there’s a 30% chance here.’ He has not ever said a 30% chance of what or for how long, but just hearing that has been what has kept her quality of life for these past six months so much more bearable and better than without hearing that. (Informal caregiver, page 5).
56
Delivery of care
Seven studies noted that prognostication had an impact on patient-doctor relationships, 56 treatment preferences,56,59,60,63 change in information needs/preferences,55,56 conflicting preference for prognostic information between patients and caregivers,56,57,62 having a survival timeframe,56,59,60 and needing additional information.56,60,62
Prognostication and the extent of its communication affected patient-doctor relationships. Some patients felt supported by clinicians who disclosed their prognosis, whilst others experienced feelings of abandonment and betrayal after their doctor did not contact them again after this disclosure. 56
Prognostication also influenced treatment preferences of patients and informal caregivers.56,59,60,63 Informal caregivers identified the need for a timeframe for planning care.
62
Some described how prognostication provided an opportunity to explore alternative treatments, such as herbal therapies,
56
whilst others felt they would not have continued with cancer treatment if they had a better understanding of the patient’s prognosis: Well, none of us would have made the decisions we did [to continue treatment] if we had known the truth about her illness. I just don’t know if the doctors knew, but they must have. Why wouldn’t they tell us? You have got to wonder why they put her through all that—I mean the chemo and especially the radiology and all those burns. She was in pain and had burns everywhere from the radiation. It was awful. She wouldn’t have gone through it if she had known what they knew, but they told us it was curable; so what are you going to do? (Informal caregiver, page 1182).
63
Information preferences of patients and informal caregivers were variable and prone to change.55,56 Many patients decided that they no longer wanted updates regarding their prognosis, 56 whilst some patients and informal caregivers had conflicting preferences for prognostic information.56,57,62
Information preferences of patients and informal caregivers included being given a survival timeframe.56,59,60 Both positive and negative aspects of this were identified; some felt that it allowed for future planning and facilitated saying goodbye to loved ones.59,60 Study respondents in favour said that they could be told the average survival time of patients with their illness or even just a rough range.
59
On the other hand, some felt that having a timeframe could make it difficult for patients to come to terms with their limited survival,
56
and even cause distress: The danger is that if you put a time frame on it, that person will believe you. . .the closer it gets the more freaked out they get. That happened to me wife, that is the median, she believed it and was almost counting the weeks away. (Informal caregiver, page 737).
59
Some patients and informal caregivers stated that they needed additional information about their prognosis, which they obtained either from their clinicians 60 or from secondary sources to supplement what clinicians had told them.56,62
Perceived health status
Three linked themes were developed in relation to perceived health status, including prognostic awareness, 58 prognostic understanding,56,60 and being aware of prognostic uncertainty.57,59,60
Prognostic awareness was something that patients could neither escape nor ignore. Often, patients who were not initially aware of their prognosis were said to become aware, or at least suspect it, due to the progression of their disease and decline in physical state: He was aware of his diagnosis, but he did not know of the prognosis. He was very much worried about his condition and started fearing that something bad was going to happen. (Informal caregiver, page 115).
58
On the other hand, prognostic understanding was something that had to be sought by patients and informal caregivers or encouraged by clinicians.56,60 It was viewed to be clinicians’ responsibility to nurture prognostic understanding in patients and informal caregivers so that they might make decisions accordingly.
Regardless of whether patients and informal caregivers had awareness or understanding of their prognosis, they were unanimous that clinicians should be honest about the level of uncertainty that comes with making an estimate of life expectancy.
57
Some patients acknowledged the uncertainty of prognostication and sympathised with clinicians who had to provide such estimates.
59
Other studies found that informal caregivers considered that clinicians were not always open about prognostic uncertainty: We were never given any indication that my wife was going to die. . .Only after her death, when I questioned him did he acknowledge that his prognosis of a cure had changed and he was just hoping to put her into remission (Informal caregiver, page 1473).
60
Personal circumstances
Prognostication impacted the way in which patients and informal caregivers handled their personal circumstances.56,58,59 Discussing prognosis allowed individuals to settle their responsibilities, plan for the future and get their affairs in order: As I said no-one’s god and no-one can say your time’s going to be up in 6 months, but I think if you’ve got some idea. . .you can put your life in order and get your family and that prepare a but, I think that’s good. (Patient, page 737).
59
Combined results
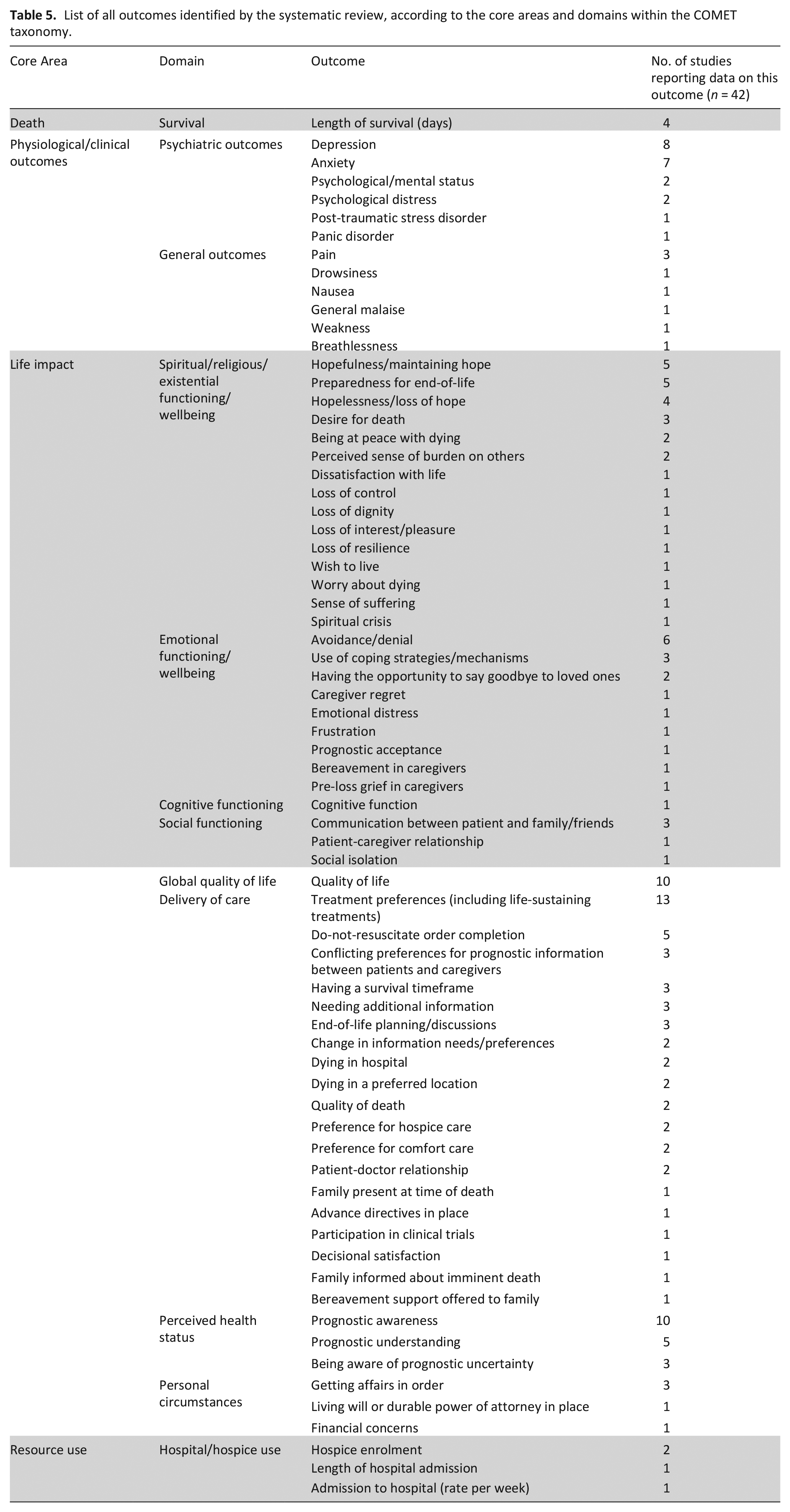
Outcomes with similar definitions were merged in order to combine outcomes identified in both types of studies into a single list. For example, psychological status and mental status were merged as psychological/mental status. This resulted in a final list of 70 outcomes of prognostication in advanced cancer (Table 5).
List of all outcomes identified by the systematic review, according to the core areas and domains within the COMET taxonomy.
Discussion
Main findings
We identified 70 outcomes used to measure the impact of prognostication in 42 included studies pertaining to 12 of the COMET taxonomy domains. The most prevalent outcomes were treatment preferences (n = 13), prognostic awareness (n = 10), quality of life (n = 10) and depression (n = 8). Prognostication was shown to have a widespread impact on patients and informal caregivers, with the highest number of outcomes categorised under the delivery of care domain (n = 50), followed by spiritual/religious/existential functioning/wellbeing (n = 30) and psychiatric outcomes (n = 21).
Half of the outcomes (n = 35) were identified in only one study each, and no outcome was reported by all studies, reflecting the diversity of outcomes chosen. This systematic review thus demonstrates the variation of outcomes used for assessing impact in prognostic studies in advanced cancer. The results of the quantitative analysis, in particular, highlight the heterogeneity and inconsistencies in the outcomes included in studies and how they are assessed. Some studies used non-validated methods, such as unstructured patient or caregiver reports, for assessing outcomes, risking reporting and recall bias. 68 Studies that used validated outcome measures varied widely in the measures chosen. Seven different measures were used to assess depression and six to assess quality of life, each with varying quality and validity for use in palliative care.69,70 Evaluation of specific measures was outside the scope of this review; further research is needed to evaluate the suitability of outcome measures used in prognostic studies within an advanced cancer population.
The patient perspective is increasingly understood as important for assessing and identifying healthcare outcomes. 71 By including qualitative data on the personal experiences of patients and informal carers, we identified key outcomes of prognostication that are meaningful to people receiving care that quantitative studies did not identify. The discordance between the number of qualitative and quantitative papers identified in our search indicates a dearth of literature on lived experiences of prognostication in advanced cancer. Patients’ and informal caregivers' experiences of prognostication can provide insights about care preferences and how these align with or differ from current clinical practice. 71 There is, therefore, a need for further consideration of which outcomes of prognostication are deemed important to patients and informal caregivers to capture these outcomes in future prognostic research.
What this study adds?
An important component of study design is choosing suitable outcome measures. It can be difficult to compare study findings across specific areas of research when endpoints are incompatible, reducing the potential for meta-analyses and perpetuating outcome reporting biases. 72 Prognostic studies have often focused on outcomes deemed important by academics and clinicians, and outcomes used in some studies may not be meaningful for patients or informal caregivers.72,73 Studies should always account for the opinions and experiences of patients and other personally affected stakeholders, not least in order to facilitate the translation of findings into clinical practice.74–77 Our systematic review identified considerable heterogeneity in outcome reporting across included studies and under-representation of patients’ and informal caregivers’ experiences. These findings could now be used to inform the development of a core outcome set for prognostication in advanced cancer in consultation with relevant stakeholders.
Strengths and limitations
This is the first systematic review to synthesise data on outcomes from both quantitative and qualitative studies of prognostication in advanced cancer reported in English. An extensive search ensured a transparent, replicable report. Rigorous screening identified all relevant studies, so this review synthesises all available evidence written in English.
This review has some limitations. The research questions and analysis only included adult participants; therefore, results are not generalisable to a paediatric population. We only included publications written in English. However, international publications were included, reducing the likelihood of selection bias. 78
Six of the non-randomised studies were all conducted by the same authors in homogenous populations.34,43,50 –53 These studies were conducted in different years, but we could not determine whether the same individuals had been enrolled in more than one of these studies, which might have biased effect sizes. 79 However, since the aim of our review was to narratively synthesise the outcomes of prognostication rather than investigate effect sizes, this does not affect our findings.
Prognostic interventions used in the included studies were not discussed in this review, due to heterogeneity or inadequate descriptions of the methods of prognostication used. Future exploration of interventions used in prognostic studies may allow for the interpretation of our findings regarding the relationship between prognostic interventions and outcomes of prognostication.
We were unable to distinguish between outcomes due solely to prognostication and outcomes arising from the underlying disease, such as pain or fatigue, and our review did not seek to make such distinctions. However, there is likely to be some confounding when assessing the relationship between prognostication and these kinds of outcomes, which further supports the need for a core outcome set for prognostication in advanced cancer.
Finally, there is currently no universally accepted method of classifying outcomes into domains. The COMET taxonomy 21 provided useful guidance about how to systematically group outcomes but posed some challenges. The COMET guidance on how to allocate outcomes to a specific domain was sometimes ambiguous, and some domains lacked suitable sub-categories for some outcomes, particularly those relating to spiritual, religious and existential functioning/wellbeing. The taxonomy developers permit and encourage further development of sub-categories to provide finer classification within each of the outcome domains. 21 Duplication or overlap of outcomes or domains does not lead to loss or misclassification of information when developing a core outcome set. We, therefore, created our own domain and sub-categories for this particular group of outcomes.
Conclusion
This review demonstrates that studies of prognostication in advanced cancer vary widely in how they report and measure outcomes. In addition, experiential outcomes for patients and informal caregivers are not always represented. In order to conduct future research into the impact of prognostication, a standardised approach to outcome reporting in prognostic studies is required. This should be done in consultation with key stakeholders to ensure outcomes reported are relevant and meaningful to those the research affects the most.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231191148 – Supplemental material for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231191148 for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies by Caitlin Spooner, Bella Vivat, Nicola White, Andrea Bruun, Gudrun Rohde, Pei Xing Kwek and Patrick Stone in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163231191148 – Supplemental material for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies
Supplemental material, sj-pdf-2-pmj-10.1177_02692163231191148 for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies by Caitlin Spooner, Bella Vivat, Nicola White, Andrea Bruun, Gudrun Rohde, Pei Xing Kwek and Patrick Stone in Palliative Medicine
Supplemental Material
sj-pdf-3-pmj-10.1177_02692163231191148 – Supplemental material for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies
Supplemental material, sj-pdf-3-pmj-10.1177_02692163231191148 for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies by Caitlin Spooner, Bella Vivat, Nicola White, Andrea Bruun, Gudrun Rohde, Pei Xing Kwek and Patrick Stone in Palliative Medicine
Supplemental Material
sj-pdf-4-pmj-10.1177_02692163231191148 – Supplemental material for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies
Supplemental material, sj-pdf-4-pmj-10.1177_02692163231191148 for What outcomes do studies use to measure the impact of prognostication on people with advanced cancer? Findings from a systematic review of quantitative and qualitative studies by Caitlin Spooner, Bella Vivat, Nicola White, Andrea Bruun, Gudrun Rohde, Pei Xing Kwek and Patrick Stone in Palliative Medicine
Footnotes
Acknowledgements
We thank Marie Curie and the Economic and Social Research Council for supporting this review via a PhD Studentship grant. We also thank Katie Abranson (UCL Library Services) for assisting with the search strategy for this review.
Author contributions
PS, BV, NW and CS contributed to the design of the review and protocol development. CS, AB, GR and PXK contributed to the screening of articles. CS led on data analysis. CS led on drafting of the manuscript. All authors contributed to revisions and approved the final version.
Data availability
All data relevant to the study are included in the article or available in supplementary files/appendices.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council and Marie Curie Cancer Care [grant number: ES/P000592/1].
Research ethics and patient consent
Ethical approval was not required for this review as there was no direct patient contact or access to individual participant data. However, the overarching study that this review is part of was reviewed and approved by the London-Camberwell St. Giles Research Ethics Committee and the Health Research Authority on 6th September 2022 (reference 22/LO/0469).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.