
Abstract
Background:
The prevalence of dementia is rising worldwide and many people will die with the disease. Symptoms towards the end of life may be inadequately managed and informal and professional carers poorly supported. There are few evidence-based interventions to improve end-of-life care in advanced dementia.
Aim:
To develop an integrated, whole systems, evidence-based intervention that is pragmatic and feasible to improve end-of-life care for people with advanced dementia and support those close to them.
Design:
A realist-based approach in which qualitative and quantitative data assisted the development of statements. These were incorporated into the RAND/UCLA appropriateness method to achieve consensus on intervention components. Components were mapped to underlying theory of whole systems change and the intervention described in a detailed manual.
Setting/participants:
Data were collected from people with dementia, carers and health and social care professionals in England, from expert opinion and existing literature. Professional stakeholders in all four countries of the United Kingdom contributed to the RAND/UCLA appropriateness method process.
Results:
A total of 29 statements were agreed and mapped to individual, group, organisational and economic/political levels of healthcare systems. The resulting main intervention components are as follows: (1) influencing local service organisation through facilitation of integrated multi-disciplinary care, (2) providing training and support for formal and informal carers and (3) influencing local healthcare commissioning and priorities of service providers.
Conclusion:
Use of in-depth data, consensus methods and theoretical understanding of the intervention components produced an evidence-based intervention for further testing in end-of-life care in advanced dementia.
The number of people worldwide dying with and from dementia is increasing and many have similar needs to those dying from cancer or major organ failure.
Care towards the end of life for people with advanced dementia is fragmented and many may die with unrecognised and untreated symptoms, in particular pain.
There are few evidence-based interventions available to improve care.
An in-depth approach to developing a complex healthcare intervention in advanced dementia as death approaches (the COMPASSION intervention).
The feasibility of undertaking systematic engagement with experts across the United Kingdom to enable wide consensus on intervention content and take account of context and new ideas for change.
An example of how theories underlying the professional behaviours required to implement the intervention and deliver an integrated approach to care can be explored.
The COMPASSION intervention may facilitate integrated care at the end of life in advanced dementia; it includes training and support to enable this to occur.
COMPASSION has the potential to inform commissioners on processes, mechanisms and potential costs of an integrated multi-disciplinary model for end-of-life care in advanced dementia.
Use of rigorous methods, including theoretical perspectives, in developing this intervention may increase the likelihood of its feasibility and acceptability in practice.
Introduction
Dementia affects approximately 835,000 people in the United Kingdom and trends suggest that 70 million people will be living with the condition worldwide by 2020. 1 Dementia typically involves a gradual, unpredictable decline in cognition, behaviour and function and may be considered a terminal neurodegenerative disease. 2 It is estimated that one-third of people aged over 65 years in the United Kingdom will die with some form of dementia 3 and 70% with advanced dementia reside in care homes. 1
End-of-life care in dementia
Symptom management near the end of life in dementia is often sub-optimal, although symptom burden may be similar to cancer, chronic obstructive pulmonary disease (COPD) or advanced heart failure.4–7 In frail older people, dementia may exist with several co-morbid conditions, and death may occur from various causes. In the advanced stages, survival is unpredictable 8 and death may be due to dementia or another inter-current illness. People may show challenging behavioural and psychological symptoms, and while these may lessen as dementia progresses, care requires skill, compassion, attention to detail and patience. Good person-centred care9,10 using simple measures may help. Quality standards for dementia and end-of-life care have been published in the United Kingdom;11–14 a systematic review of international guidelines found another four documents (from United States, Australia, Singapore and Malaysia) that considered palliative care, 15 and consensus from 23 countries and the European Association for Palliative Care 16 highlights symptom control, comfort measures, communication, shared decision making, including families with care planning, timely recognition of dying, attention to continuity of care, and psychological and spiritual support.
Care homes
In England, there are 32,937 care homes currently registered with the Care Quality Commission, most privately owned. General practitioners have responsibility for the clinical care of residents but staffing in care homes varies, often with a few trained nurses supported by a larger pool of healthcare assistants. Use of the UK Department of Health Gold Standards Framework 17 may enhance staff skills, although implementation and outcomes vary.18–20 Relationships with external services such as community geriatricians and mental health and palliative care teams differ and depend on local commissioning priorities, interactions with care home owners and managers, and local clinicians’ levels of interest, knowledge and confidence in dementia care.21–23
A feasible, context appropriate and sustainable intervention for end-of-life care in dementia is needed. Here, we describe how, in an iterative process, we used empirical data from our 3-year programme of research on end-of-life care in dementia 24 and expert opinion to develop the COMPASSION intervention. We achieved consensus on core components using the RAND/UCLA appropriateness method (RAM) 25 and mapped the components to theories of change in complex healthcare systems. Our methods reflect the importance of theoretical understandings and an iterative approach in devising an intervention to improve dementia care. 26
Aim
We used a realist framework 27 and rigorous processes, guided by the literature on development and implementation of complex healthcare interventions for whole systems change, to develop an intervention to enhance multi-professional detailed management of care home residents with advanced dementia who are approaching death and facilitate integrated care.
Methods
Theoretical basis of intervention development
We define a theory as ‘a system of ideas or statements held as an explanation or account of a group of facts or phenomena’. 28 Our work was informed by Medical Research Council recommendations 29 on the development and testing of complex interventions, and the MORECare guidance statements that were published to enhance methodological rigour in palliative care research. 30 To develop an effective but feasible intervention, we were careful to include preliminary evidence both from empirical work and expert opinion and to consider theoretical principles underlying whole systems healthcare change.
Realist methods
Our 3-year research programme was based on a realist framework.24,27 This approach highlights barriers to good care but also identifies mechanisms that may improve care; it is consultative and iterative, taking into account local and contextual factors. We collected qualitative and quantitative data from multiple sources combining findings with evidence from reviews of the international literature and policy documents across the four countries of the United Kingdom. The generation of new ideas was enabled by an interactive process in workshops and interviews during which both researchers and participants contribute 27 (see Figure 1). A final realist programme theory based on all elements of our wider research programme (National Institute for Health Research (NIHR) reference CRN-PCRN 12621; 12623) is in preparation.
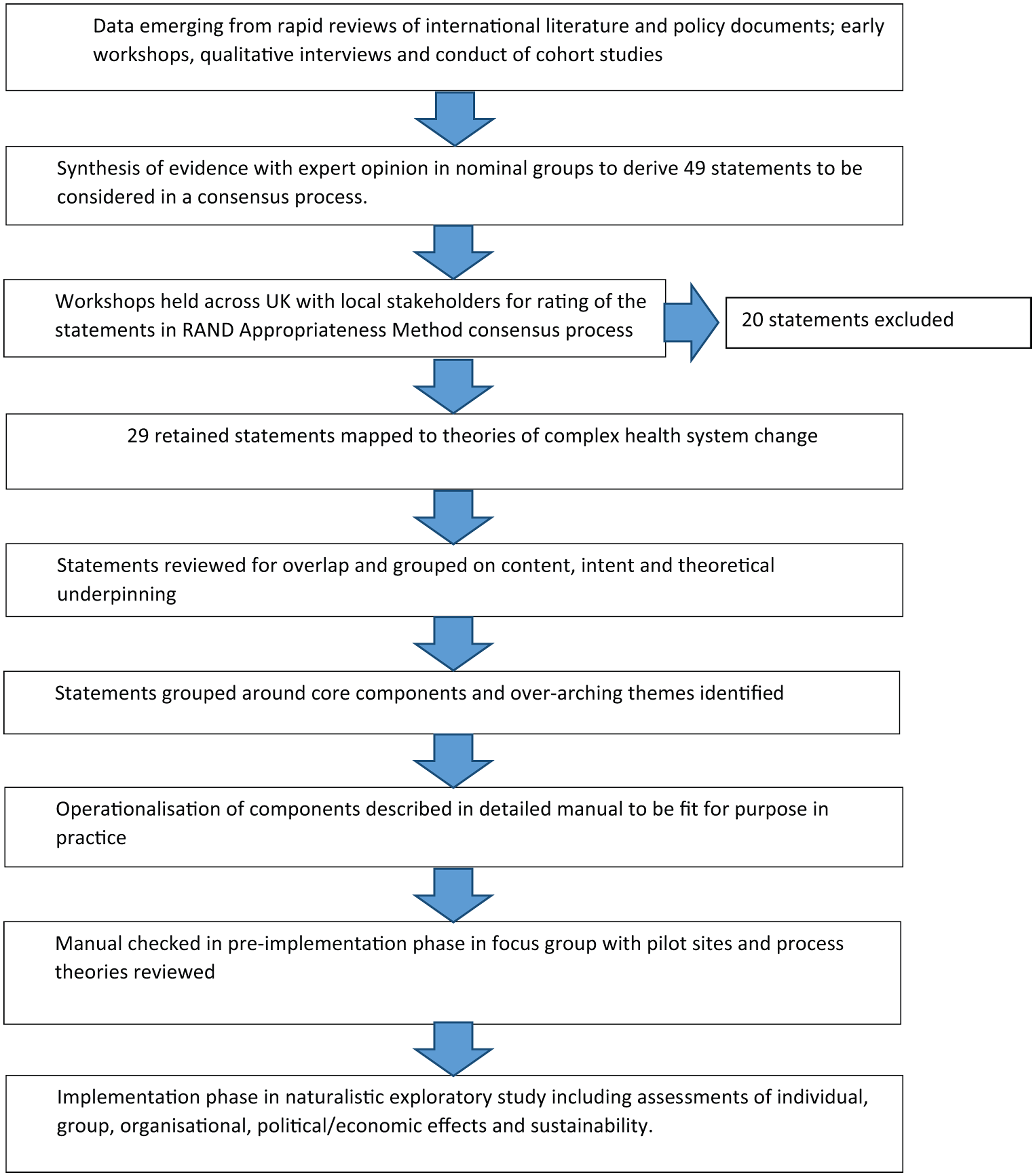
Process for the development of the COMPASSION model of care for people with advanced dementia at the end of life and those close to them.
Theories affecting complex healthcare systems
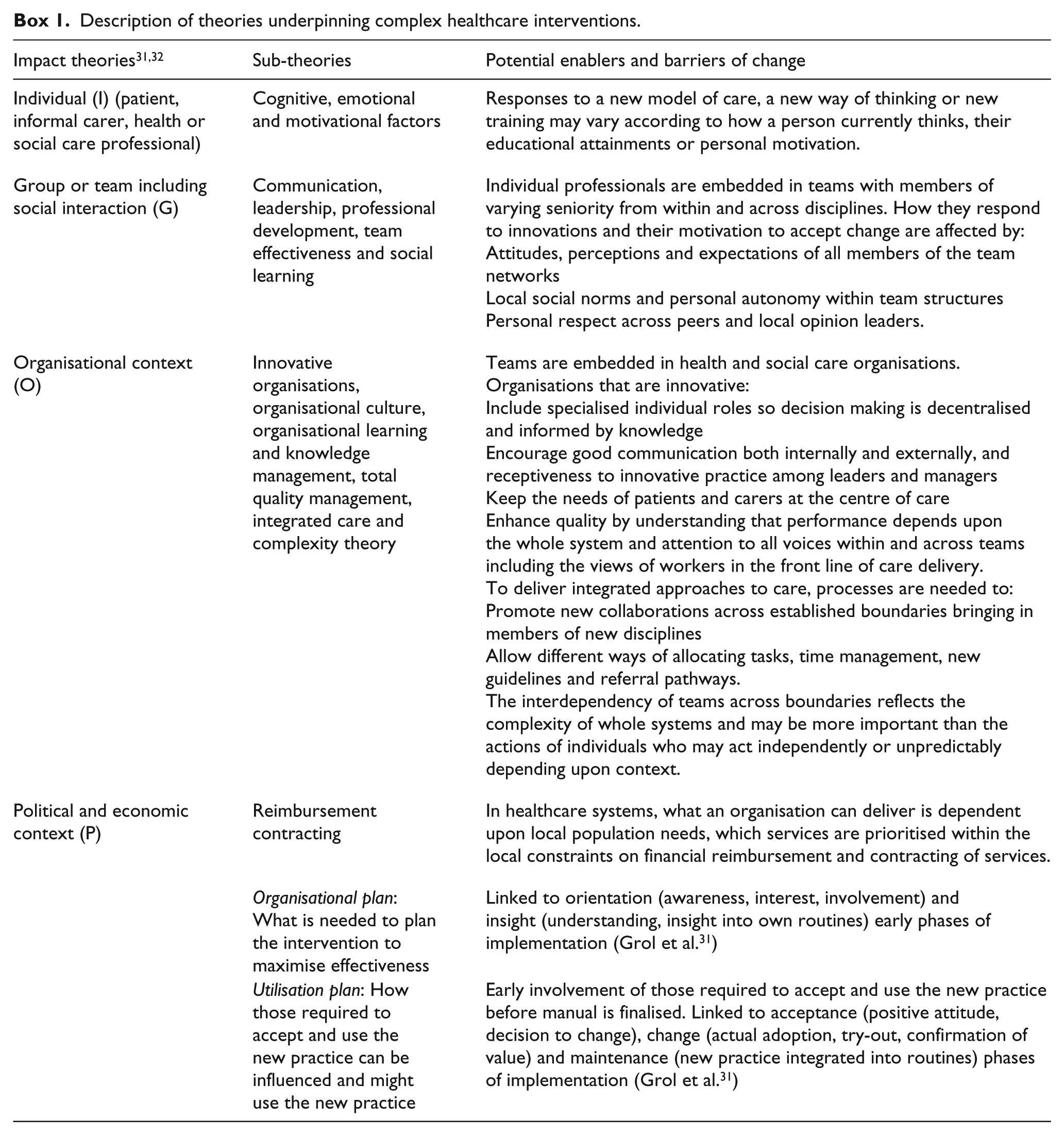
We considered the general impact and process theories31,32 that might underlie potential components of our intervention to understand how these might operate in practice; these are described in Box 1. This provided a framework for our integrated care model. 31
Description of theories underpinning complex healthcare interventions.
Early evidence synthesis and derivation of statements on intervention components
We combined information from the following sources: 24 (1) our rapid review of the literature and policy documents, (2) research team field observations, (3) advice from the programme expert steering group, (4) emerging results from our cohort study, (5) preliminary workshops and interactive qualitative interviews with professional and informal carers and (6) a workshop with people with early dementia. We used these data to generate case vignettes to illustrate emergent findings. Our team consisted of international experts in palliative care, dementia and complex intervention theory, and field researchers collecting data directly from care home residents. 24 The expert steering group, including lay representation and national experts in health and social care, provided detailed feedback as our intervention developed.
Nominal groups
Within our realist framework, solutions were generated at a series of meetings attended by the whole research team at which we used our case vignettes as a basis for discussion. Using flip charts and field note recordings, possible solutions were noted and grouped for potential impact according to the four levels (individual, group, organisational or political/economic) at which system change operates (Box 1).31,32 This included consideration of the mechanisms required to implement the solution. Using nominal group techniques, in a three-round iterative process, solutions were ranked according to their feasibility within existing dementia care provision in the United Kingdom. The group considered how the solution might be operationalised and what staff or resources and which key decision makers might be required. This process generated a set of statements for consideration in a national consensus process.
Achieving national consensus on intervention content
We used the RAM 25 to achieve consensus on which statements derived from our evidence synthesis should form the components of our intervention. The RAM process took place over three rounds (two online and one face-to-face in workshops) in which participants considered the statements and ranked them for appropriateness 25 and necessity, 25 irrespective of potential costs.
RAM workshops
To take account of context, RAM workshops were held in each of the four countries of the United Kingdom; two in England (London and Birmingham), and one each in Wales, Scotland and Northern Ireland. Acting as a local contact point, facilitators in Marie Curie hospices in Birmingham, Edinburgh, Belfast and Cardiff identified potential participants. Each liaised with a number of diverse agencies with an interest in people with advanced dementia and palliative care within their wider local health and social care system to include professionals from a range of disciplines and levels. In London, we accessed a network of contacts across 11 care homes. We aimed to include 10 locally based health and social care providers for people with dementia in each workshop; to achieve this, the research team circulated up to 30 invitations at each site. Interested individuals were sent an invitation and study information sheet to consider participation (via post or email). If they wished to take part, they were asked to sign and return a consent form either beforehand or on the day of the workshop. Each workshop lasted 2 h and was co-facilitated by two members of the research team (K.L., J.H. – London, Birmingham, Cardiff; S.S., S.D. – Edinburgh and K.L., S.S. – Belfast).
RAM process
The concept of appropriateness refers to the relative weight of the benefits and harms of a healthcare intervention. An appropriate component is one in which the expected health benefit exceeds the expected negative consequences by a sufficiently wide margin that the intervention is worth doing, exclusive of cost. 25 Participants rate the benefit–harm ratio of each statement on a scale of 1–9, where 1 means the expected harms greatly outweigh the expected benefits and 9 that the expected benefits greatly outweigh the expected harms. A middle rating of 5 can mean either that the harms and benefits are about equal or that the rater is unable to decide.
The concept of necessity refers to opportunities for interventions that must be offered to patients fitting a particular clinical description. The RAM definition of necessity is that
the intervention is appropriate, i.e. the benefits exceed the risks by a sufficient margin to make it worthwhile; it would be improper care not to offer the intervention; there is a reasonable chance of benefit; the magnitude of the expected benefit is not small.
25
Ratings are also made on a scale of 1 unnecessary to 9 necessary.
Round 1 responses completed online prior to the RAM workshops, rating for appropriateness. Invitees were emailed an online survey including the set of statements and asked to complete their ratings 2 weeks prior to each workshop. Participants rated each statement from 1 to 9 for appropriateness. The research team collated responses and ranked them as (1) ‘Appropriate’: ALL responses from the group rate that statement as 7–9, (2) ‘Uncertain’: At least ONE individual rated that statement 1–6 and (3) ‘Inappropriate’: At least TWO individuals rated that statement 1–3.
Round 2 responses completed in person at the end of the RAM workshops, rating for appropriateness. The local workshop was then held and all statements rated by the group as either ‘uncertain’ or ‘inappropriate’ were discussed. After the group discussion, all participants again rated all statements for appropriateness. They were instructed that if an individual felt their response remained the same they were under no obligation to change it. The research team collated responses as ranked appropriate, uncertain or inappropriate by the group.
Round 3 responses completed online 2 weeks after the RAM workshops, rating for necessity. Within 2 weeks of each workshop, participants completed a second online survey consisting of only those statements that had been ranked by that workshop as appropriate. Participants rated each of these statements for necessity. Responses were collated and ranked by the research team as either (1) ‘Necessary’: ALL responses (or all except one) from the group rated that statement as either 7–9, (2) ‘Uncertain’: At least TWO individuals rated that statement 1–6 and (3) ‘Unnecessary’: At least TWO individuals rated that statement 1–3.
Collating of results
Upon completion of Round 3, results from the five RAM process workshops were collated, and those statements rated as necessary by attendees at three or more of the workshops were retained.
Mapping to theory
Three senior members of the research team (L.J., E.L.S. and B.C.) not actively involved in data collection independently considered each statement retained after the RAM process and assessed (1) which of the four theoretical levels of impact (individual, social interaction, organisational context, political and economic context) were likely to be targeted by the statement and (2) which sub-theories might be operating (Box 1). Results were compared for consistency and statements on which two or more of the raters agreed were retained. Statements were then reviewed for overlap by the research team and combined to simplify language and clarify their operational aims.
Preparation of a written manual
We prepared a written manual describing in detail the content of the intervention and the steps needed to put it into practice, to maximise the potential for transferability and replication. 33
Checking prior to implementation – orientation and insight phase
We developed a protocol for an exploratory naturalistic implementation study. 34 We began implementation with a local focus group including clinical leads for care of the elderly, palliative care, old age psychiatry, social care and care home managerial staff. We discussed the content of the manual and adjustments were made as needed. This approach addressed process theories 35 of how the intervention would be put into practice (Box 1) and forms part of the orientation and insight phases required for successful implementation. 31
Results
First draft of ‘COMPASSION’ intervention components
Table 1 shows our early synthesis of existing evidence with data emerging from our wider research programme. After discussion in our nominal groups, we drafted 49 statements for consideration in the RAM process (Table 2).
Synthesis of evidence from wider programme of research NIHR portfolio reference CRN-PCRN 12621; 12623.
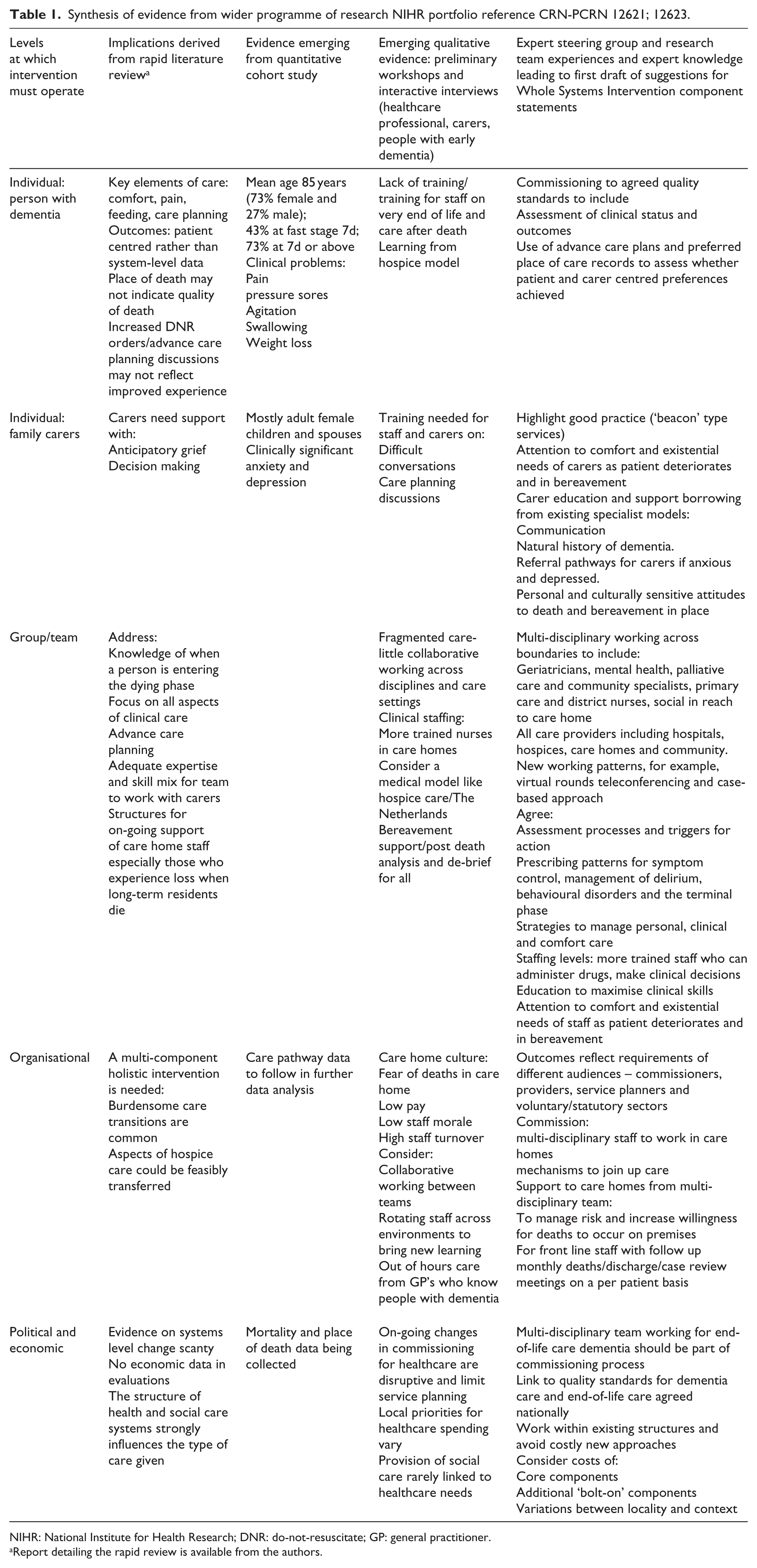
NIHR: National Institute for Health Research; DNR: do-not-resuscitate; GP: general practitioner.
Report detailing the rapid review is available from the authors.
Statements considered in RAM process (N = 49).

RAM: RAND/UCLA appropriateness method; I: Individual professional; G: Social interaction; O: Organisational context; P: Political and economic context, and sub-theories likely to operate; NHS: National Health Service.
Retained statements in italics (N = 29) mapped to levels at which complex healthcare systems operate.
RAM process, collation of results and mapping to theory
Table 3 shows characteristics of participants in each RAM workshop and the results of the ratings for appropriateness and necessity. Collation of data from Round 3 resulted in the retention of 29 statements which were mapped to their proposed theoretical levels of action (Table 2).
RAM workshops with healthcare professionals.
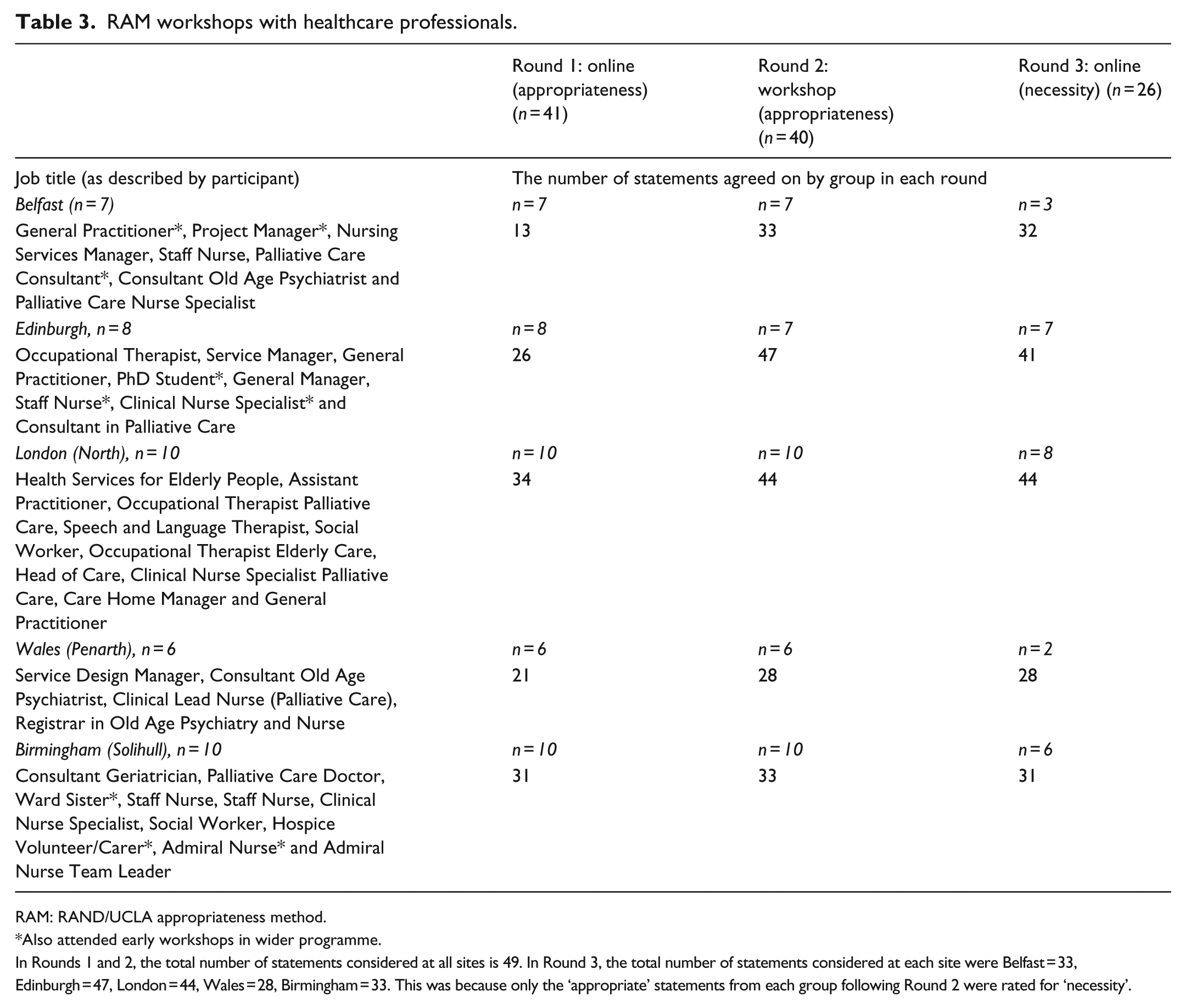
RAM: RAND/UCLA appropriateness method.
Also attended early workshops in wider programme.
In Rounds 1 and 2, the total number of statements considered at all sites is 49. In Round 3, the total number of statements considered at each site were Belfast = 33, Edinburgh = 47, London = 44, Wales = 28, Birmingham = 33. This was because only the ‘appropriate’ statements from each group following Round 2 were rated for ‘necessity’.
Combining statements to derive pragmatic components
The wider research team considered the retained statements finding that several could be combined, both on theoretical underpinning and stated practical aims. Since it is difficult to separate individual professional behaviours from interaction with colleagues and teams, we combined the levels of individual and social interaction under the pragmatic theme of ‘training and support based’. We retained the themes ‘organisational context’ and ‘political and economic context’. We describe three core components (Table 4):
Influencing how local services are organised;
Providing education, training and support for formal and informal carers;
Influencing the political and economic environment.
The COMPASSION intervention version final draft for detailing in a written manual.
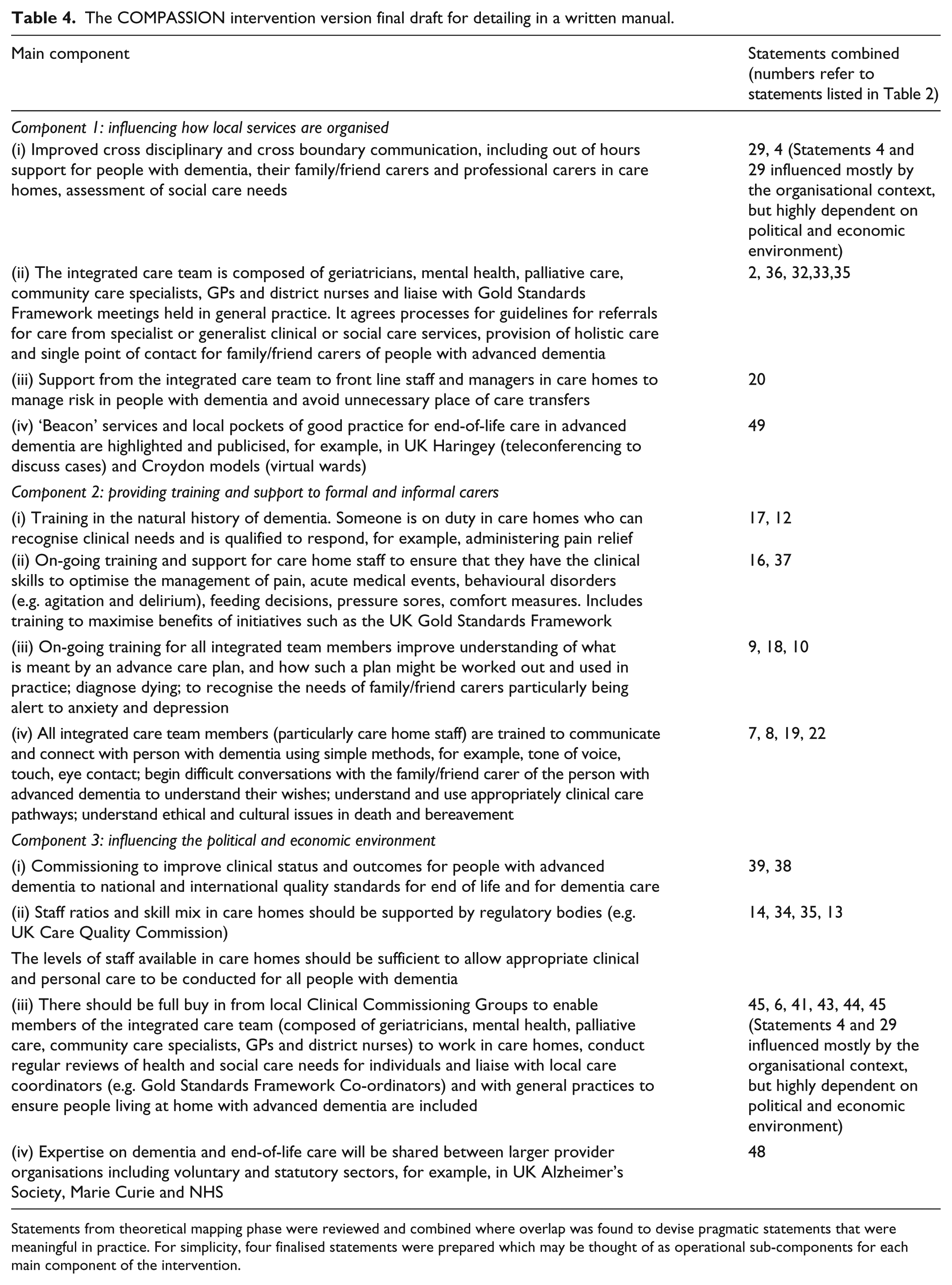
Statements from theoretical mapping phase were reviewed and combined where overlap was found to devise pragmatic statements that were meaningful in practice. For simplicity, four finalised statements were prepared which may be thought of as operational sub-components for each main component of the intervention.
Components 1 and 2 require dedicated time from a professional, with experience of working with people with dementia in care home settings, to lead integrated approaches to care. They work within existing systems to (1) understand current service provision and practice; (2) develop joint working between providers across primary, secondary and tertiary care; (3) support local staff to establish processes for regular assessment of those progressing towards the end of life; (4) alert members of the multi-disciplinary team to those people with dementia who require additional care planning and management and (5) address educational and training needs (linked to nationally agreed core competencies) through shared working, use of online resources and formal topic-based teaching if required.
COMPASSION intervention manual
In the intervention manual, we provide detailed descriptions of processes to achieve these aims, to enable new working practices and to initiate and maintain an education training and support programme. 34 Components 1 and 2 are both dependent upon, and will influence to varying degrees, the local political and economic context, including commissioning priorities of local service providers.
Discussion
Key findings
We used an iterative process to develop COMPASSION, an integrated intervention for end-of-life care in advanced dementia. We combined information from existing literature, empirical data, opinions of expert policy makers and those working in the field with our theoretical frameworks. A realist approach enabled interactive discussions in workshops and interviews so that rather than describing problems, potential solutions could emerge. These were considered in workshops, ranked for appropriateness and necessity in the RAM process, and combined in pragmatic statements for use in practice. Understanding the theoretical underpinning enabled us to consider who needs to do what differently, which barriers and enablers need to be addressed according to context, and which behaviours and models of delivery might influence these issues. 36
We shall learn more about how COMPASSION operates as we complete our exploratory implementation study. 34 This will provide information on how the integrated model of care works in practice, and preliminary data on costs. 36 Describing sustainability is challenging and a number of theoretical models are available.37,38 We revisit the test sites twice within 12 months of implementation to assess which elements of the intervention have been incorporated into routine practice and look for ripple effects within the healthcare economy. An integrated approach to dementia care is needed as one discipline alone cannot manage the complex psychiatric, physical and social problems which occur. 39 Integrated care may improve outcomes, in particular quality of life, through improved diagnosis, treatment and management of problems as they arise. 40
Strengths and weaknesses
Our work concords with recent recommendations on research in dementia at the end of life, in particular gathering data from multiple sources, considering underlying theories and using an iterative approach to devise an intervention that is flexible and sensitive to context. 26 We focus on care homes as we identified very few people with end-stage dementia who remained in their own homes, and we incorporate views from across the United Kingdom. The RAM process is more often used for achieving consensus on simpler healthcare interventions. However, it facilitates some idealism as participants rate for appropriateness and necessity irrespective of economic considerations. This is consistent with our realist approach which encourages discussion of new solutions to problems. Other consensus methods such as Delphi processes or nominal groups are available, but advantages of the RAM include incorporation of data from the literature, confidential ratings plus group discussion and multi-disciplinary panels including views from a range of perspectives. Disadvantages include multiple rating rounds with a nine-point scale, the need for face-to-face meetings, problems of dominant forces within groups and risk of bias from the research team in preparation of the statements for consideration. 41
Additional bias may have occurred during our theoretical mapping phase which relied on choices of the research team. However, the benefits of gaining understanding from use of theories are well recognised in the field of healthcare innovations,36,42 and the incorporation of evidence on the views of recipients of an intervention at the design stage is increasingly understood.43,44
Conclusion
It is unusual for healthcare interventions to be developed using such thorough processes and our work provides a template of how this is possible. We hope, but cannot yet be sure, that COMPASSION has enhanced potential for feasibility, acceptability and effectiveness.
Through synthesising what may be most desirable in current practice, COMPASSION could be considered a ‘meta-intervention’. Rather than being innovative and suggesting radical changes to care, COMPASSION provides processes which maximise existing expertise. Care is enhanced through breaking down barriers between teams, placing the person with dementia at the centre of care, educating care providers and ensuring sensitivity to local context.
Footnotes
Acknowledgements
We thank professor Martin Marshall, Professor of healthcare improvement at UCL, for his methodological advice; Marie Curie Hospice Research Facilitators Kathy Armour, Anne Finucane and Noleen McCorry for assistance with workshops; Professor Steve Morris UCL as co-applicant in obtaining funding for the COMPASSION Programme and for advice on health economics; Mr Jeffrey Round UCL for advice on health economics; members of our expert steering group and all participants for their generosity in giving time to this programme of work.
Author contributions
Louise Jones and Elizabeth Sampson conceived the research and obtained funding for the COMPASSION Programme, managed all elements of the work and drafted the manuscript. Bridget Candy conducted the rapid evidence review and contributed to data interpretation. Sarah Davis, Jane Harrington, Nuriye Kupeli, Kathryn Lord and Sharon Scott collected data from participants and contributed to data analysis and interpretation. Margaret Elliott and Kirsten Moore finalised the COMPASSION intervention manual and contributed to analysis and interpretation of data. Victoria Vickerstaff and Anna Gola contributed to data analysis and interpretation. Rumana Omar, Michael King, Gerard Leavey and Irwin Nazareth (with Steve Morris) conceived and obtained funding for the COMPASSION research programme and provided expert advice throughout the programme. All authors contributed to the development of the manuscript and approved the final version.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethics
Ethics approval was obtained from University College London (UCL) research ethics committee (ref 3578/001).
Funding
This work was supported by Marie Curie programme grant funding to Marie Curie Palliative Care Research Department, UCL, grant ref. MCCC-FPR-11-U.