
Abstract
Background:
Broad consensus exists on the relevance of advance care planning in dementia. Although people with young-onset dementia and their family are hypothesized to have distinct needs and preferences in this area, they are hardly ever included in studies.
Aim:
We aim to explore the experiences with and views on advance care planning of people with young-onset dementia and their family caregivers.
Design:
A qualitative study was conducted, analyzing semi-structured interviews through the method of constant comparative analysis.
Setting/participants:
We included 10 people with young-onset dementia and 10 of their family caregivers in Flanders.
Results:
Participants lacked awareness about the concept of advance care planning, especially as a communication process. They had not or barely engaged in planning future care yet pointed out possible benefits of doing so. Initially, people with young-onset dementia and their caregivers directly associated advance care planning with planning for the actual end of life. When discussing advance care planning as a communication process, they paid ample attention to non-medical aspects and did not distinguish between medical, mental, and social health. Rather, respondents thought in the overarching framework of what is important to them now and in the future.
Conclusions:
Engagement in advance care planning might be hindered if it is too medicalized and exclusively patient-centered. To accommodate advance care planning to people with young-onset dementia’s and their caregivers’ needs, it should be presented and implemented as a holistic, flexible, and relational communication process. Policy and practice recommendations are provided on how to do so.
Despite consensus on its relevance, the uptake of advance care planning in dementia is low.
People with young-onset dementia and their caregivers are hypothesized to have distinct needs and preferences for palliative care and advance care planning.
There is a dearth of studies which include people living with young-onset dementia and their family.
People with young-onset dementia and their caregivers strictly associated advance care planning with medical planning for the end of life and reported to have not or barely engaged in this.
Respondents were unacquainted with the concept of advance care planning as a communication process, yet when discussing advance care planning as such, they broadened their narratives to “what matters to them now and in the future”; in doing so they did not make a division between their medical, social, or mental health.
An overly medicalized approach to advance care planning, restricted to planning death, might impede people’s engagement in the process.
Within our sample, advance care planning was solely known as a narrow medical term, namely as documentation of end-of-life decisions. However, conceptualizing advance care planning as a communication process about what matters most might resonate better with their actual needs. Advance care planning can best be implemented in practice as a holistic, flexible, and relational communication process.
As the majority of our respondents’ preferences were not directly linked to their younger age, our findings, and recommendations could possibly help guide research regarding the implementation of advance care planning in other patient populations.
Policy makers and clinicians jointly hold responsibility for raising awareness and for uniform messaging about the evolved concept of advance care planning as a broad communication process.
Introduction
A precondition for appropriate care for people with dementia is efficient and timely communication between patients and their caregivers. 1 Providing an opportunity for advance care planning is regarded as an essential element of sound palliative care 2 and of ethically responsible long-term care after a diagnosis of dementia. 3 Advance care planning has been conceptualized as a process of communication between patients, family, and professionals to explore patients’ preferences for future (medical) care, including care at the end of life. 4 It has been 50 years since the concept of advance care planning arose as a movement for establishing advance directives as legal guiding mechanisms to refuse treatment. 5 Back then, documenting an agreement between patient and physician in an advance directive was the primary focus of advance care planning, 6 centrally aimed to respect patient autonomy. 7 Advance care planning has conceptually evolved over time, 8 and especially in recent years has undergone a shift in focus from documentation to a process of ongoing support in communication and shared decision making.9,10 However, a recent review on advance care planning intervention studies showed the lack of unity within the scientific and clinical field on what constitutes advance care planning, as studies use varying definitions, target different aspects of advance care planning and put forward a large variety of outcome types. 8 Nonetheless, a review of 2021 showed that the evolved concept of advance care planning as a process has been adopted in recent, as opposed to older, studies with only 4% equating advance care planning to the completion of an advance directive. 8
The overall aim of advance care planning is to increase the chance that the care received is in accordance to the care desired, even at times when people are no longer able to make or express their own choices. 11 As such, advance care planning can be particularly important for people with dementia, given that Alzheimer’s disease and related neurodegenerative disorders are characterized by progressive cognitive decline, which may ultimately result in decisional incapacity. 3 Since family caregivers are highly likely to be faced with difficult care decisions for their loved one, it is recommended to involve them in advance care planning as early as possible.12,13 Despite consensus of its possible significance in dementia, the average uptake of advance care planning is particularly low in this patient population.14,15
Although dementia is typically associated to older age, it is estimated that globally 3.9 million people live with young-onset dementia, implying their condition developed before the age of 65. 16 These younger patients and caregivers have been presumed to have distinct needs and preferences in terms of palliative care, and specifically in terms of advance care planning. 17 This hypothesis is based on their active phase of life, with significant social, financial, and professional commitments.18,19 Nonetheless, this particular patient population and their family caregivers remain an underrepresented group in research. Moreover, studies that include people with young-onset dementia themselves are nearly non-existent. Yet, gathering a broader understanding of patients’ insights and views is indispensable for conceptualizing advance care planning in a manner that is adjusted and accommodating to them.
This study’s research question is: “What are the experiences with and the views on advance care planning of people with young-onset dementia and their family caregivers?” Through this study we wish to gather insights and formulate recommendations for policy and practice on what to take into consideration when initiating or engaging in advance care planning in young-onset dementia.
Methods
Design
Given both the exploratory nature of our research question and the sensitivity of the topic, a qualitative study design was deemed most appropriate. Qualitative data were collected through face-to-face in-depth interviews, which were semi-structured for allowing respondents to elaborate on topics not prompted by the researcher. For reporting, COREQ guidelines were followed.
Participants
Setting
Respondents were recruited from two provinces in Flanders (Antwerp and West Flanders) and from Brussels Capital Regions by two neurologists, the coordinator of a day care center and the founder of a non-profit organization for people with young-onset dementia.
Population
Participants were recruited as dyads of a person formally diagnosed with young-onset dementia of the Alzheimer Type (symptom onset before the age of 65) and his/her primary caregiver.
Recruitment
Inclusion criteria and phases within recruitment are described in detail in Table 1.
Detailed overview of recruitment procedure.
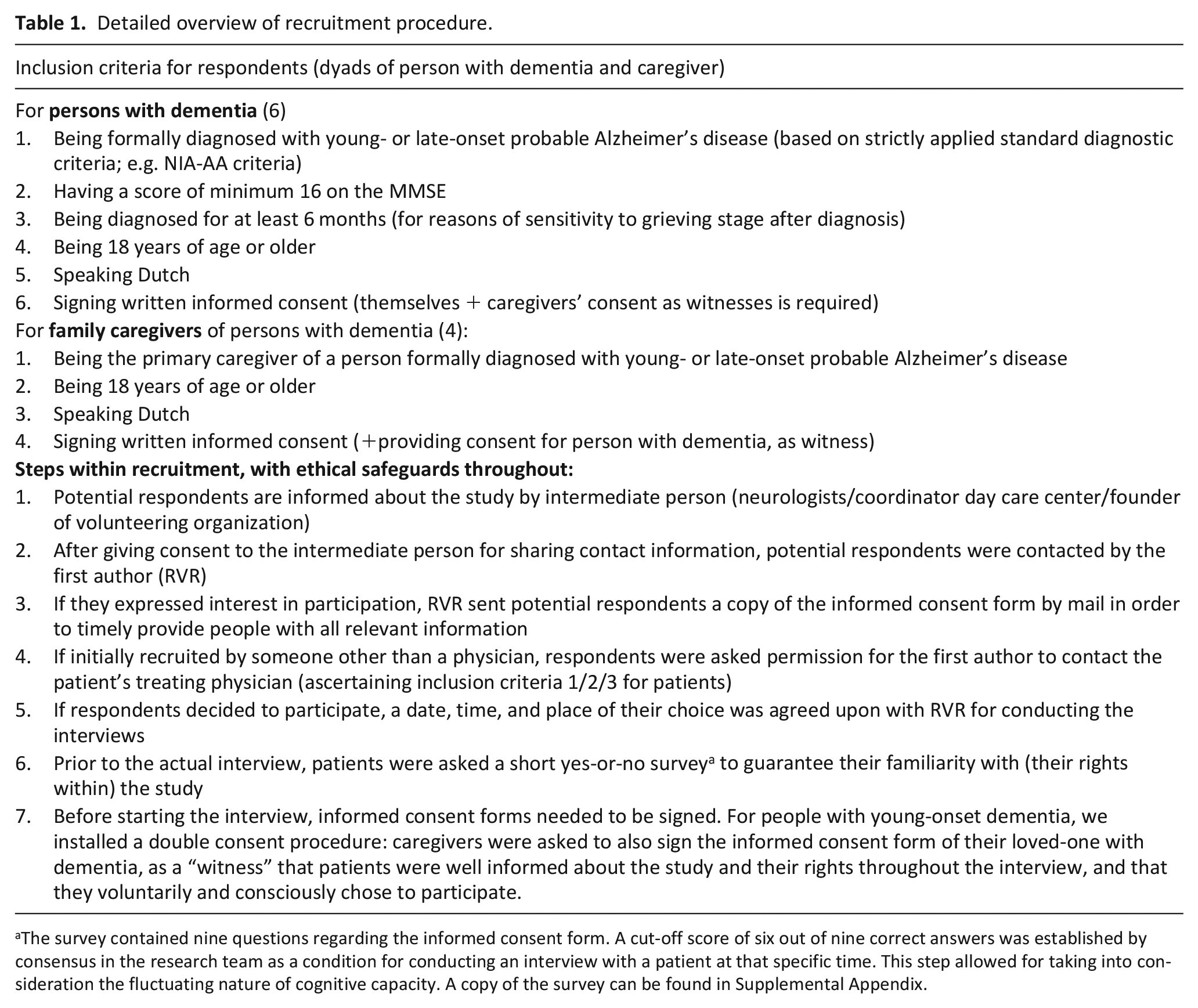
The survey contained nine questions regarding the informed consent form. A cut-off score of six out of nine correct answers was established by consensus in the research team as a condition for conducting an interview with a patient at that specific time. This step allowed for taking into consideration the fluctuating nature of cognitive capacity. A copy of the survey can be found in Supplemental Appendix.
Data collection
Interviews were standardly conducted individually, yet as an ethical safeguard, persons with young-onset dementia were given the option of having their caregiver present if it made them feel more comfortable. Interviews were based on a topic guide, as shown in Figure 1, and took place at a location of respondents’ choosing, which was their home or the day care center. They took place from August until December 2019.
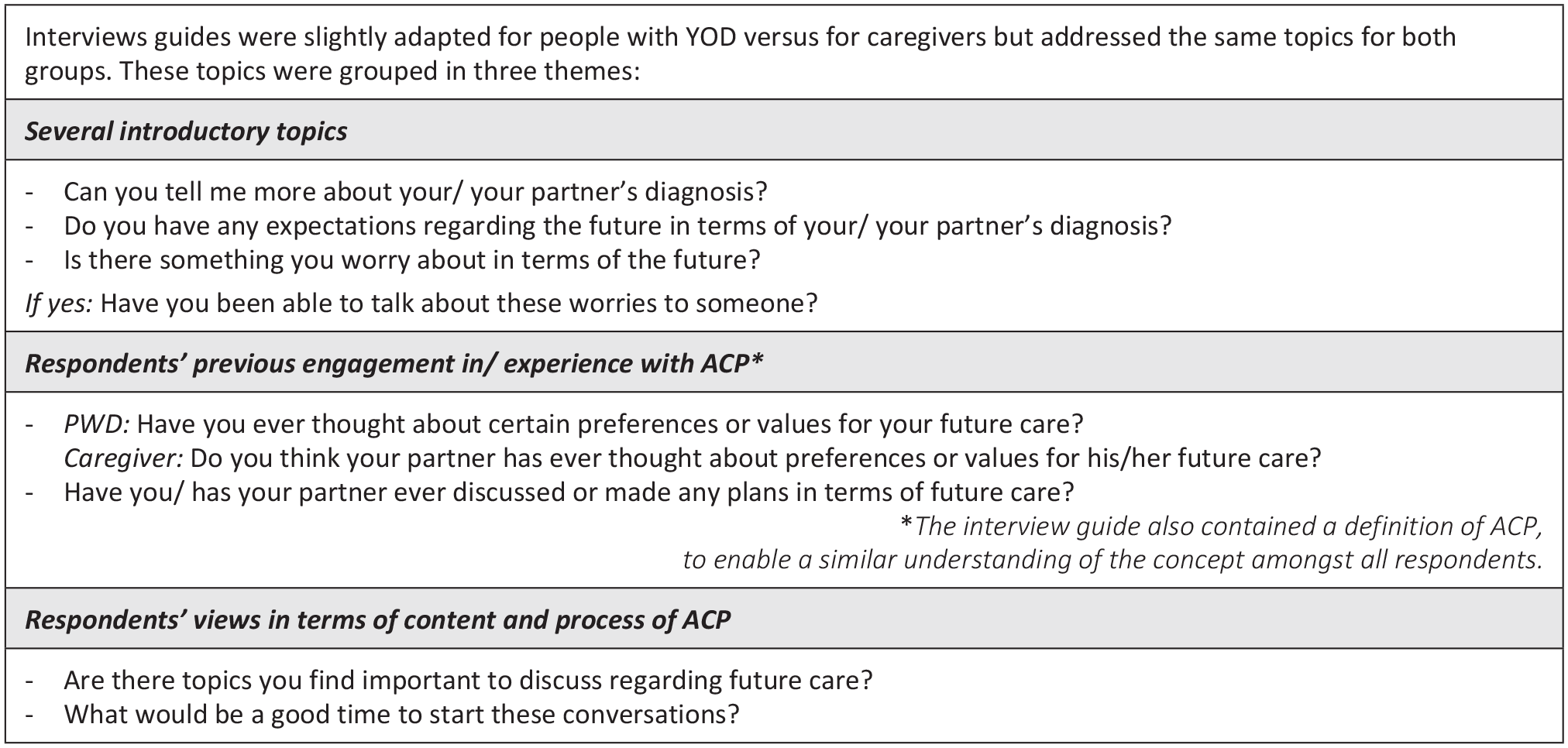
Summary of interview guide with exemplary questions for each theme.
Data analysis
All interviews were conducted and transcribed verbatim by the first author and were subsequently analyzed through constant comparative analysis, 20 a qualitative method that entails consistent and comprehensive coding of open-ended data. 21 Transcripts were reviewed line-by-line and discrete text fragments representing a certain idea or concept were assigned a descriptive code. The first five transcripts were coded independently by two researchers (RVR and ADV), the others were coded solely by the first author. No software was used. The next phase in analysis, constructing a “coding tree” of overarching themes that emerge from comparing codes both within and between interviews, was again done collaboratively by two researchers (RVR and ADV).
Ethics
This study was approved by the Ethics Committee of the University Hospital Brussels (B.U.N. 143201939497) as the central commission and by GZA Antwerp (190304ACADEM) and ZNA Antwerp (approval n° 5208) as local commissions.
Results
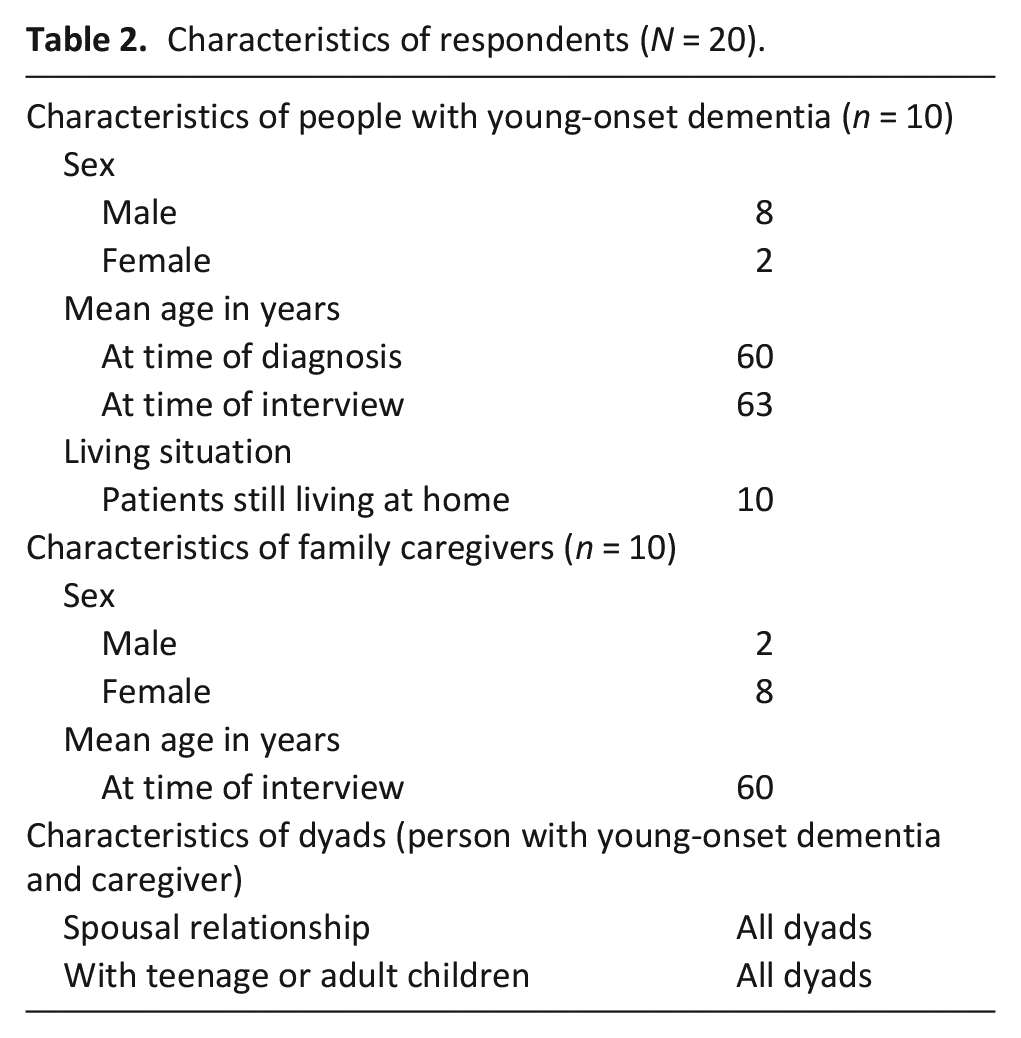
Sample characteristics
Characteristics of respondents (N = 20).
Overview of results
Two overarching themes, with respective subthemes, emerged from our data. The first theme is centered around the finding that our participating people with young-onset dementia and their caregivers barely engaged in medical care planning as part of advance care planning. The second overarching theme that emerged shows respondents’ thought framework of “what matters now & in the future” when they conceptualize advance care planning as a communication process.
Respondents barely engage in planning medical care as part of advance care planning
Most of the responding people with young-onset dementia and their caregivers were unaware of what the term advance care planning means or entails. If they had a notion of advance care planning, they discussed it as strictly related to medical end-of-life decisions. It emerged that only one couple had completed an advance directive (living will). A few caregivers and patients stated they rather impulsively and in panic had mentioned or had very briefly discussed the possibility of ending life, mostly right after being diagnosed. Some couples had documented that the caregiver would be the legal representative for the patient. People with young-onset dementia and caregivers elaborated on matters they had planned for the future. However, due to respondents’ very limited engagement in planning care as part of advance care planning, our results cannot fully cover the original research question of people’s experiences with the process. Our respondents provided several reasons for not discussing/planning future (medical) care. Moreover, they described potential benefits of doing so.
Planning for non-medical domains
Regardless of their self-described lacking knowledge about young-onset dementia, most people with young-onset dementia and their caregivers were aware of the progressive nature of Alzheimer’s disease, the inevitable decline in functioning and ultimately the end of life.
“The disease trajectory is not important in my case because they don’t know anyway how it’s going to progress, does it go fast, does it go slow. But the result is all the same huh. We are very well aware of that.” (person with young-onset dementia, woman)
As such, many patients and caregivers made plans for non-medical domains as they arranged financial wills and documented their spouse’s right to control finances once the person with dementia would no longer be able to. Several patients also commented on their preferences following death such as funeral arrangements or donating their body to science.
“It seemed like a normality to me to arrange that -finances-” (person with young-onset dementia, man)
“That I joke about that -funeral- and say like ‘no fuss around that, as simple as possible’. . . Yeah that’s for later, but of course it can be there quicker than you might think.” (person with young-onset dementia, man)
Reasons for not discussing care
Patients’ attitudes hindering advance care planning communication
Although the majority of caregivers endorsed the idea of engaging in advance care planning, barely any had done so with the patient. Certain attitudes of the person with young-onset dementia, described by themselves and their caregivers, appeared to be hindering for actually discussing future care. More specifically, not worrying about their (future) situation, not experiencing a sense of urgency to arrange matters, and patients resigning in and accepting their situation seemed counter-productive for advance care planning.
“Maybe in the far future, it might still be too early. I’m still way too young. . . Plus, I’m still having fun, so at this point that -discussing care- is not necessary.” (person with young-onset dementia, man)
“I actually don’t think about that yet, what the future will bring. It’s not going to keep me up at night, let me put it that way. Not at all.” (person with young-onset dementia, man)
“That’s how these things go. I imagine if things get more serious, then I will get more serious too.” (person with young-onset dementia, man)
“To me it’s more like, it has to be done one day. . . But now I don’t have the feeling like, yes, I have to -discuss care- as soon as possible.” (person with young-onset dementia, man)
Not knowing what the future holds impedes planning for medical decisions
A topic that emerged frequently among both persons with young-onset dementia and their caregivers was the uncertainty and the unpredictability of the disease trajectory. The majority of both patients and caregivers commented on how difficult it is to know what’s coming throughout the progression of Alzheimer’s disease and at what speed.
“It progresses differently for everyone, so you can’t focus on that, right. So yes, we know something is coming, but we don’t know what.” (caregiver, woman)
The “individuality” of each person’s disease trajectory complicated advance care planning, in the sense that respondents were doubtful regarding which decisions to prepare for. Additionally, some caregivers suggested advance care planning to be a flexible and vivid process; both as a response to the disease’s erratic progression, and as a way to meet patients’ potential fear for advance care planning’s binding nature.
“Yes, it can change. . . I always have difficulty with ACP -advance care planning- on paper because it changes. Right, not wanting a few things any longer, yeah, until the time is there. . . To me it has to remain vivid. I am under the impression that if I write it down, then it’s somewhere outside of me -my control-.” (caregiver, woman)
“You can discuss certain scenarios like ‘I think of it like this’, but at the moment it happens, you can never say like ‘this is exactly identical to what we have discussed’.” (caregiver, woman)
Uncertainty about what the future holds, appeared associated to living with a “day-to-day” attitude. Focusing attention to the present, trying to enjoy, and “learning to live with it” on a daily basis were examples of such mindset, manifested by both patients and caregivers.
“Day by day, that is actually my motto. And there have been relatively many good days.” (person with young-onset dementia, man)
Needing to know more
Several caregivers and patients also emphasized their need for information both regarding young-onset dementia as a diagnosis and prognosis, and regarding advance care planning. Such information provision was deemed lacking and inaccessible by some.
“It’s only by knowing what exists, that you know how you can be helped. . . The more you know, the better the trajectory will be. I am convinced of that.” (person with young-onset dementia, man)
“There is information, but you always have to go look for it yourself. . .. Information is the most important step -within advance care planning.” (caregiver, woman)
On the other hand, some patients expressed not experiencing a desire for more information.
Answering question on wish for information:
“Not too much at once. It’s not going to get better, right.” (person with young-onset dementia, man)
“No, I don’t think so. It’s more the situation of, yeah, I didn’t have anything left to say or do, it didn’t matter.” (person with young-onset dementia, man)
Patients’ and caregivers’ hypothesized benefits of advance care planning
Several motives, expressed by both patients and caregivers, emerged that would encourage engagement in advance care planning. One reason for engaging in advance care planning was found in the fact that persons with young-onset dementia would be enabled to participate in decision making. A more frequently emerging motivation was found in the relief that planning in advance would bring for the caregivers.
“I don’t have any problem with that -advance care planning-. Of course it is something that needs to be arranged, and now I still have a say in it. I mean, now I can still say myself how I would like things.” (person with young-onset dementia, woman)
“To me it’s like, actually we have to do that now, because imagine he is suddenly not able to any longer, then we are too late and that’s especially what I want to prevent. While I think that X (patient) is more like, yeah okay, I’ve still got some time for that, it’s not necessary for now. To me it would actually be a relieve like, okay, you’ve arranged that too, you’ve got one less worry.” (caregiver, woman)
“Actually, if you do that -advance care planning, document a will-, at this point I think that you do it more so for your relatives than for yourself. Because I am not yet convinced that those people -people living with more advanced stages of dementia- actually suffer pain or that those people experience an unbearable feeling.” (person with young-onset dementia, man)
“I have to do that for myself as well, not just for him.” (caregiver, woman)
Patients and caregivers broaden their thought framework to “what matters now and in the future” when thinking of advance care planning as a communication process
When respondents were informed about the concept of advance care planning as a communication process, they broadened their narratives to “what their future might hold” and reflected in depth about what matters to them throughout their/their loved-one’s disease trajectory. Doing so, they provided meaningful insights into several broader care preferences, needs in young-onset dementia care, and into the inter-relational approach toward people with young-onset dementia.
Values expressed by patients and caregivers as important to them within care
Many recommendations and comments were formulated regarding care provision by both persons with young-onset dementia and their caregivers. These revolved around three major themes, which were mostly mentioned by respondents in relation to patients’ younger age. Firstly, the need to enable people with young-onset dementia to remain socially and physically active according to their (remaining) possibilities.
“Every day I fight a battle with boredom.” (reason for going do day care) (person with young-onset dementia, man)
“That I still have contact with the outside world, that I can still have conversations with people or a small talk, that is important to me. That I am not completely isolated, that is what I fear.” (person with young-onset dementia, woman)
Secondly, a wish for family-centered care emerged. It was emphasized by both patients and caregivers that the condition does not solely affect the patient, and that support should be extended toward children and spouses.
“Especially with young-onset dementia I do miss a bit the information -about care availability- and the support toward a young family with children, with adolescents.” (caregiver, woman)
Lastly, several patients and caregivers referred to the indispensability of autonomy and dignity within care provision.
“I was once allowed to join -in support group for patients and caregivers- and then the first time I could be with the group, uum. . . it was a meeting. And then the second time I wasn’t allowed to participate anymore, only those who were not sick were allowed in that room. And I had to make drawings, do another thing. And then I was a bit angry. . . I was very angry actually.” (person with young-onset dementia, man)
“It’s about being occupied with these people and leaving them in their dignity. And about actively doing things with them, go outside, I mean. . ., don’t -leave them- in a wheelchair for entire days.” (caregiver, woman)
The importance of receiving high quality care
Our respondents generally perceived residential care provision as lacking quality. All, except one patient, were unwilling to address the topic of residential care, according to their caregiver, or had expressed their wish to stay home for as long as possible. Only one person with young-onset dementia stated to be at peace with the idea of someday moving to a facility. The majority of caregivers expressed fear for one day having to make the decision of transferring their loved-one to residential care.
“I hope something happens, so I never have to do that. Because knowing that he has always said “I do not want to end up there” and then for me, I also find it very difficult to have to admit to myself that this is where it ends at home now.” (caregiver, woman)
“They get you out of bed and then they put you back in at night. And for the rest it’s done, I mean, as a figure of speech. . .. That you are not treated like small children or anything like that. Because that’s what you see at times, right, in certain hospitals, that’s what you still see. And that is not how I want to end up, no I don’t want that.” (person with young-onset dementia, woman)
The public perception of (young-onset) dementia
The stigma and taboo that is still associated to dementia and their impact on patients’ self-esteem emerged throughout several patients’ narratives. These usually revolved about people assuming that the person with young-onset dementia was unable to do or understand certain things.
“It’s frustrating for somebody else that I’m not capable of doing some things, and it’s a little difficult to deal with. . . be patient with me and don’t make fun of me in some sense. . .. then I don’t feel very comfortable in life anymore.” (person with young-onset dementia, man)
“That they -people in general- do not have to immediately think or say to others ‘oh, but he doesn’t know it anyway’. Okay, that will be the impression these people have, you can’t blame them, that a group of people still have that taboo and that they don’t know. . .” (person with young-onset dementia, man)
Discussion
Summary of findings
It emerged that our respondents lacked awareness about advance care planning, particularly with its concept as a communication process. They had not or barely engaged in future (medical) planning, for which they provided several reasons. Nonetheless, they did also mention the hypothetical advantage of planning future care, and this mostly in relation to the caregiver. Throughout interviews, participants initially associated advance care planning with medically planning for the actual end of life. When discussing advance care planning as a communication process, they paid a lot of attention to non-medical aspects of care and did not compartmentalize medical, social, and mental health.
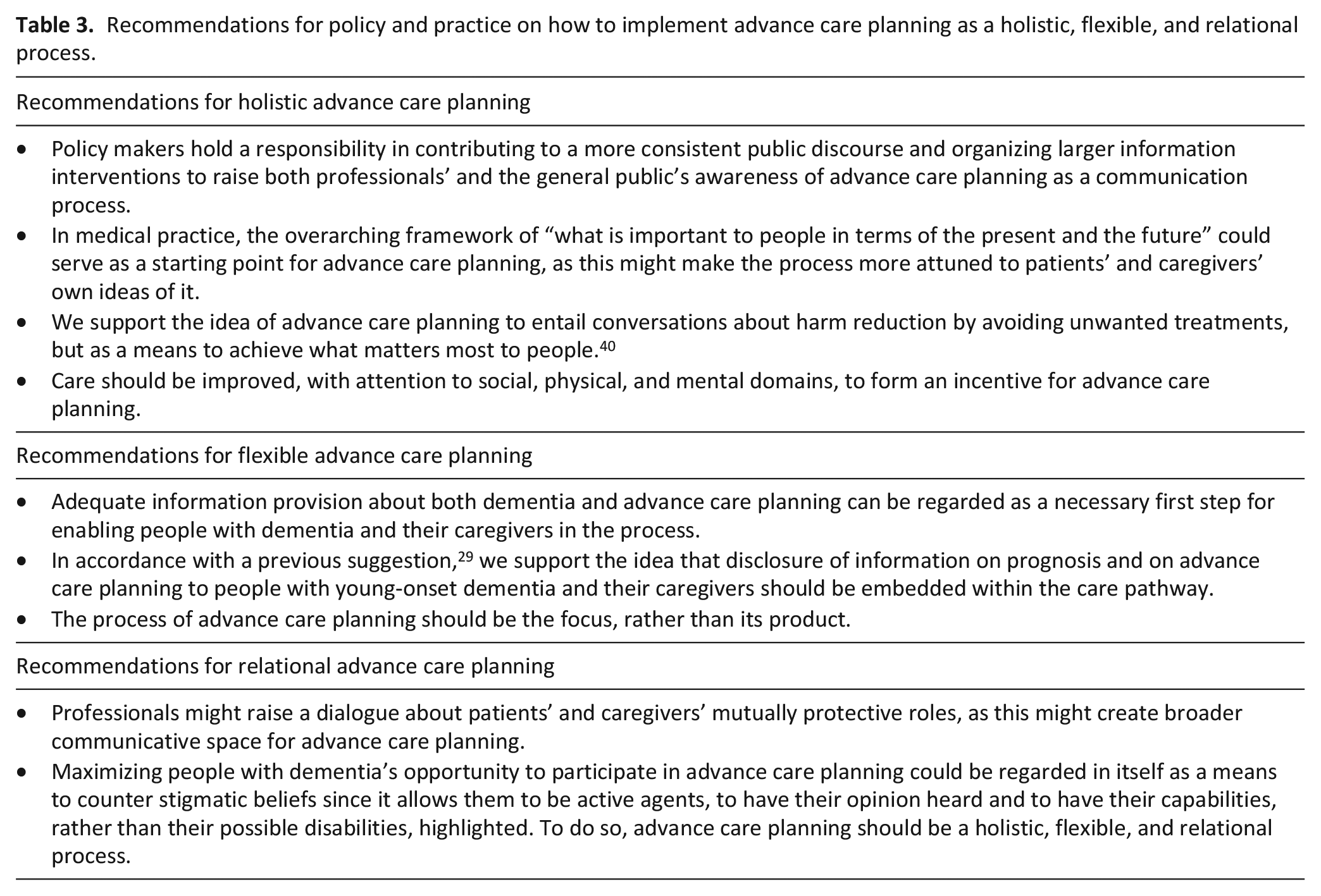
To attune advance care planning to our respondents’ views, we suggest the process to be approached holistically, flexibly, and relationally as shown in Figure 2. We provide several recommendations for policy and practice on how to do so in Table 3.
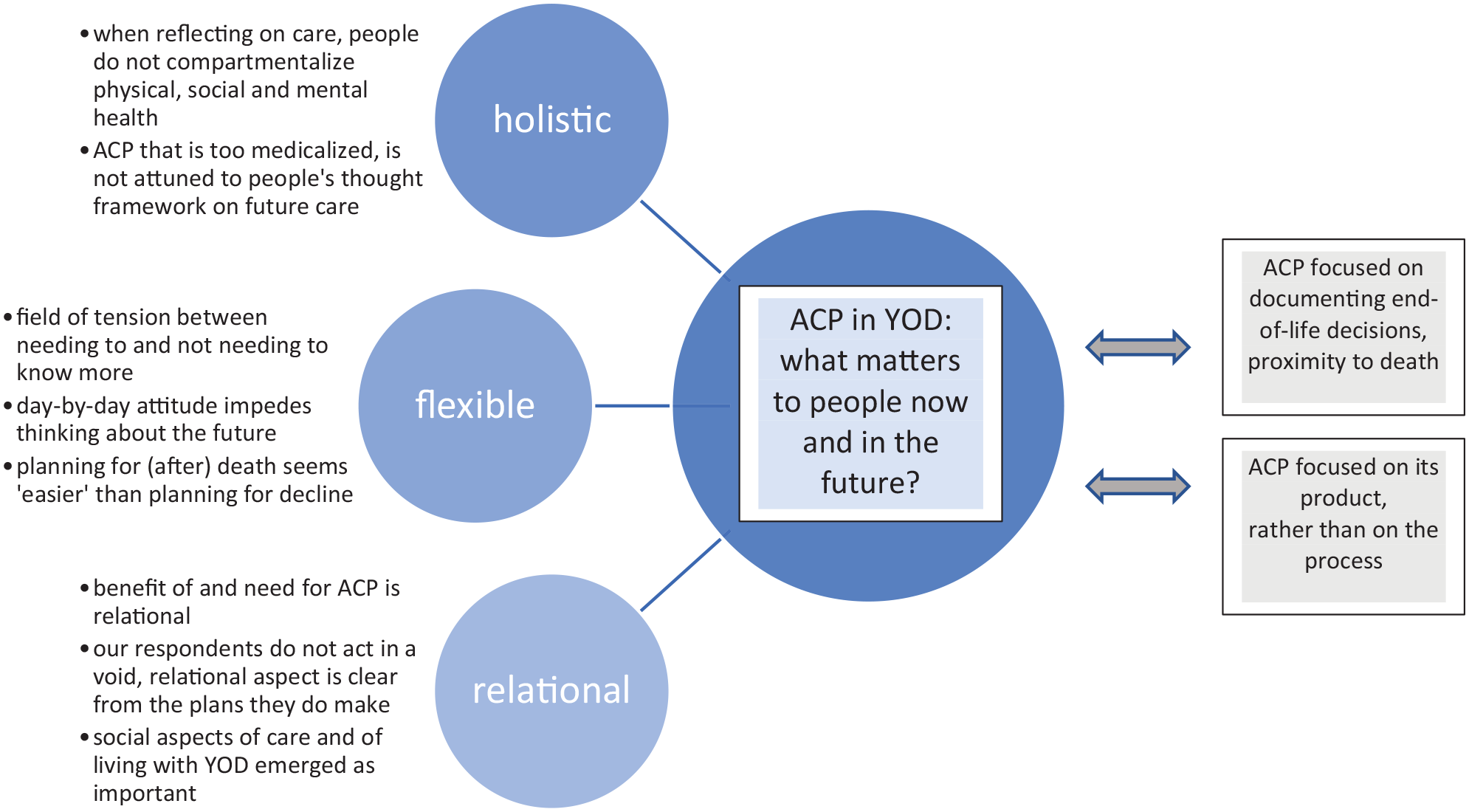
Conceptualization of advance care planning as holistic, flexible, and relational.
Recommendations for policy and practice on how to implement advance care planning as a holistic, flexible, and relational process.
Strengths and limitations
The main strengths of this study are the inclusion of people with young-onset dementia themselves and our method of in-depth interviews which allowed for rich and innovative data. Our insights shed renewed light on how to provide adequate long-term care for this specific population, yet likely sparks further questions regarding care needs in other patient groups as well. This paper is, to our knowledge, the first interview study on advance care planning to include people with young-onset dementia themselves. Meeting the at times challenging issue of ethically sound inclusion of people with young-onset dementia, we have combined multiple (novel) methodological ways for ensuring so. We believe this might serve other researchers in designing their study. However, as we recruited dyads, we were unable to gather insights of people with young-onset dementia without close informal caregivers, which would be a recommended topic for future research. Our sample was rather homogeneous, which can be regarded as both a strength and a weakness, since it has been shown that the caregiving experience for people with dementia is intertwiningly shaped by the relationship to the patient and by gender of the caregiver. 22 Our oversampling of female caregivers and male patients is a limitation. Solely interviewing spousal caregivers is a strength, as it enables future studies to compare our results with those of caregivers of a younger generation and, as such, identify whether our results are due to a cohort effect (i.e. related to our spousal age characteristic) or are shaped by the specificity of caring for someone with young-onset dementia.
Advance care planning as a holistic, as opposed to purely medicalized, process would match respondents’ views
Our respondents themselves shared their views on care in a manner that did not compartmentalize its elements, but that entailed medical, social, and mental health intertwiningly. The narrow and “academically outdated” conceptualization of advance care planning as mainly documenting end-of-life care preferences and focusing on proximity to death, emerged from our interviews as still being dominant. Since its broadened concept is more attuned to respondents’ views and needs, the understanding and awareness of advance care planning as the more holistic communication process it has evolved to needs to be increased. Our results underscore the importance of reciprocity between theory and practice: what is by now a consensus, process-oriented view on advance care planning in academia,8 –10 does not yet appear to be embraced by practice or the larger community.
The interconnectedness of physical, social, and mental wellbeing became apparent from our results regarding patients’ reluctance to discuss residential care, their clear wish not to be admitted there and caregivers’ concern of ever having to make that decision. The more sedentary services that are developed for older people’s care are not adequate for younger persons with more physical possibilities, as also reported by our respondents. 23 Additionally, the need for dignified care and the fear of being socially isolated emerged. Unavailability of age-appropriate care for people with young-onset dementia and their caregivers is a durable issue: a review showed that findings about its limited availability remain largely unchanged during the past 26 years. 24 In line with previous research, the lack of high-quality care might cause people to not feel incentivized for engaging in advance care planning, since the care they will receive would be flawed anyway. 25 The current study shows that this finding might also apply to patients themselves, as our respondents with young-onset dementia also expressed concerns regarding inadequate residential care or simply stated wishing to never be admitted there.
Flexible advance care planning would meet multiple current challenges
Patients’ and caregivers’ uncertainty regarding disease progression, is a well-established research result in the field of dementia.15,26–28 The current study highlighted yet again that a lack of knowledge regarding what the future holds, at what pace and which planning can be undertaken, is an important complicating factor. However, the field of tension between needing to and not needing to know more about disease progression became apparent in former young-onset dementia research,29,30 and was corroborated by our findings, specifically for people with young-onset dementia themselves. Consistent with previous research,26,27,31 our respondents acknowledged the terminal nature of dementia, regardless of their uncertainty about the trajectory. This was apparent by their arrangements for non-medical and mainly post-mortem domains, like finances and funeral arrangements. As such, there seems to be a “different logic” when it comes to thinking about the future: planning for after death seems to be done more easily than planning for the period between the present and the end of life. Research by Sussman et al. 31 indeed showed that contemplating about decline is more challenging and threatening than thinking about death. Sensitive and step-by-step information provision on young-onset dementia and on advance care planning might to some extent incorporate thinking about the future into the above-mentioned attitude of living life on a day-to-day basis, and as such increase the readiness for the process in itself. This recommendation partly corresponds to the preference for advance care planning as a dynamic and flexible process, emerging from our current and from previous research,15,32 as it allows to synchronize the process with the individuality of each trajectory. Additionally, a recent study showed that physicians themselves struggle with “premature” decisions for medical events that may present themselves many years later. 33 The sum of these studies underscores the significance for all stakeholders of ongoing dialogue about what constitutes current and future adequate care. As such, we support the idea 10 that the meaning of advance care planning might be found in its process, rather than in the plans it produces.
The added value of a relational, instead of an individualized, approach to advance care planning emerged
Our respondents saw the advantages of advance care planning more clearly for caregivers than for patients themselves. Concordant with other recent research,31,34 our study highlighted the potential emotional benefits of advance care planning for family caregivers. Despite a wish for dialogue by most of the caregivers, advance care planning communication did not or barely take place within our sample. Caregivers appear confronted with conflicting demands in terms of not meeting their own and protecting their loved-one’s emotional needs. To meet this complex dilemma of possibly divergent wishes, it was previously suggested 31 to frame advance care planning as an act of care of the person with dementia toward his/her caregiver. Our results indeed confirm that people with young-onset dementia might regard advance care planning as a mechanism to help safeguard their caregiver’s emotional state. Additionally, our respondents with young-onset dementia who planned their finances and made funeral arrangements, clearly showed to prioritize their loved-ones’ wellbeing. Moreover, our respondents highlighted the need for care provision to target a family, rather than the individual with young-onset dementia. The former suggests that people with young-onset dementia do not think or act in a void centralized exclusively toward them as patients. This is aligned to the concept of relational autonomy, which acknowledges relations as an essential part of decision making and pays attention to how relationships might enhance the proper exercise of autonomy. 35 Our findings indeed underscore a relational, rather than an individual, benefit of and need for advance care planning.
The importance of social embeddedness also shows from our results that people with young-onset dementia experience stereotyping and discrimination: they reported feeling excluded from activities, underestimated by others in terms of remaining capabilities and feared becoming socially isolated. How dementia is portrayed within mainstream culture leads to an increased affective and social distance toward people with dementia. 36 Experiencing stigma negatively effects people with dementia’s self-identity and can lead to their social withdrawal. 37 Importantly, patients’ hesitation to reflect on future deterioration might be associated to the stigma that comes with dementia.31,38 Its impact might even be more tangible in young-onset dementia, as a recent study 39 showed that stigmatic attributions, such as stereotypes and negative emotions, were consistently higher when confronted with younger, as compared to older, people with dementia.
Implications of our study
Several recommendations are formulated based on our findings. These are aimed at policy makers and practice/professionals, yet also target care provision in general. Given that the current study is, to our knowledge, the first one to specifically ask people with young-onset dementia and their caregivers about their views on advance care planning, its insights form a solid basis for internationally extending the evidence base on this particular element of palliative care.
As the majority of our results were not explicitly associated to our respondents’ age, we do not rule out the possibility that our findings and recommendations are generalizable to people with late-onset dementia and their caregivers. Results regarding age-appropriate care and support aimed at a young family, might on the other hand not be dementia specific and as such, applicable for younger people living with another life-changing diagnosis than young-onset dementia.
Conclusion
Our participating people with young-onset dementia and their caregivers still equated the term advance care planning to medical decisions for the actual end of life. A view on advance care planning that is too medicalized and solely centered toward the patient might impede engagement in the process, since our respondents think in an overarching concept of what is important to them now and in the future. To attune advance care planning to this thought framework, the communication process should be presented and implemented as holistic, flexible, and relational in nature.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163221090385 – Supplemental material for A qualitative study with people with young-onset dementia and their family caregivers on advance care planning: A holistic, flexible, and relational approach is recommended
Supplemental material, sj-pdf-1-pmj-10.1177_02692163221090385 for A qualitative study with people with young-onset dementia and their family caregivers on advance care planning: A holistic, flexible, and relational approach is recommended by Romy Van Rickstal, Aline De Vleminck, Sebastiaan Engelborghs, Jan Versijpt and Lieve Van den Block in Palliative Medicine
Footnotes
Acknowledgements
The authors wish to genuinely thank our respondents for sharing their valuable experiences and insights. They also wish to thank misses D. Thys and misses G. Callewaert for their help with recruitment.
Author contributions
Study concept and design: Van Rickstal, De Vleminck, Van den Block. Recruitment of respondents: Van Rickstal, Engelborghs, Versijpt. Acquisition of data: Van Rickstal. Analysis and interpretation of data: Van Rickstal, De Vleminck, Van den Block. Drafting of the manuscript: Van Rickstal. Critical revision of the manuscript for important intellectual content: De Vleminck, Engelborghs, Versijpt, Van den Block.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Foundation—Flanders (FWO), grant number 1S75919N (Strategic Basic research mandate by Van Rickstal), and grant number 12ZY222N (post-doctoral mandate by De Vleminck). For publishing this article, we would like the acknowledge the support of the University Foundation of Belgium.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.