
Abstract
Background:
People with dementia have different care and support needs at their end of life compared to people with other life-limiting illnesses, and general palliative care models may not meet the needs of people with dementia and their carers and families. Some dementia-specific end-of-life care models have been implemented, and a summary of existing models was undertaken to inform development of a local model.
Aim:
To identify best-practice models of care for people in the advanced and end stages of dementia, and their families and carers.
Design:
A rapid review with narrative summary of peer-reviewed articles and grey literature was conducted.
Data sources:
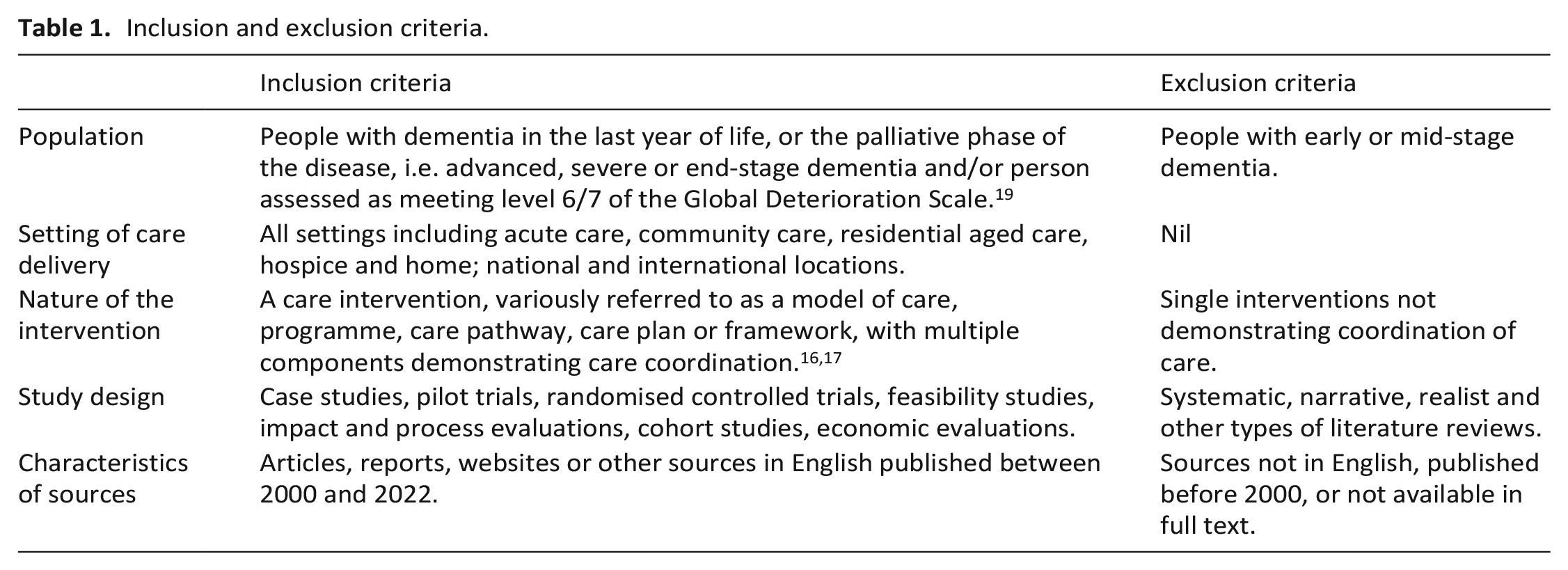
Ten databases were searched for articles published between January 2000 and April 2022. Inclusion criteria were: all care settings; AND the model focuses on people with end-stage or advanced dementia; AND contained multiple components.
Results:
Nineteen articles or reports, describing twelve dementia-specific models of end-of-life care in a range of care settings were identified for inclusion in the review. There is strong evidence that the principles of best practice palliative care for people with advanced dementia are well known, but limited examples of translation of this knowledge into integrated models of care. The key issues that emerged from the findings were: referral and admission to care, integration of care, sustainability and evaluation.
Conclusions:
Findings can be used to inform development of improved end-of-life care pathways for people with dementia, but well-designed research studies are needed to evaluate the effectiveness of integrated models of care for this vulnerable population.
Keywords
A palliative care approach is beneficial for people with advanced or end-stage dementia and the best practice components to guide such approaches are well known.
Few models of end-of-life care to meet the needs of people with dementia have been implemented, and generic models may not be appropriate or responsive to their needs.
Dementia-specific models of end-of-life care are required to meet the needs of growing numbers of people with dementia, and their families and carers.
All included models had elements of care integration (such as a care coordination role, interdisciplinary collaboration and person-centred care); but the level of integration varied considerably.
Few models of dementia-specific end-of-life care have been systematically evaluated.
Sustainability of models of care depends on long-term funding, particularly for a dedicated care coordinator role.
Findings are relevant for developing locally responsive, integrated and person-centric models of end-of-life care for people with dementia, their families and carers.
Recognition that dementia is a terminal disease requiring a needs-based approach to care is key to developing a model of integrated palliative care for people with advanced dementia.
Long-term planning is needed by policy makers and health service managers to support ongoing investment in sustainability and evaluation of models of care.
Introduction
People with dementia have different care and support needs at end of life compared to people with other life-limiting illnesses.1,2 People with advanced dementia may not be able to communicate their needs for pain management, assistance with eating and drinking or spiritual support. 2 Hospitalisation is also common for people with end-stage dementia who experience symptoms including confusion, infection, pain, constipation and loss of appetite. 3 A study of nursing home deaths across six countries found that between 60% and 83% of residents had a diagnosis of dementia, and a higher Quality of Dying in Long-Term Care score for all residents was associated with, among other factors, absence of dementia (p = 0.001). 4
Quality end-of-life care is a fundamental human right for all, including people with dementia. However there is evidence that either people with dementia were not routinely referred for palliative care or that the end-of-life care models being used in aged care settings were not responsive to the needs of residents with dementia and their family or carers.5,6 For example, a recent retrospective study of 5804 people diagnosed with dementia in the United Kingdom, who died between 2016 and 2019, found that only one in three were identified as having palliative care needs in their last year of life. 7 This is despite evidence of potential benefits of a palliative approach to end-of-life care for people with dementia, 8 and the European Association for Palliative Care’s inclusion of dementia palliative care as an emerging specialty area in its recent review of standards and norms for palliative care in Europe. 9
One reason for the low rate of referral of people with dementia to palliative care services is that dementia is often not recognised as a terminal illness.2,5,10,11 Another argument is that few models of end-of-life care have been developed specifically for people with advanced dementia, despite strong consensus on the optimal elements of palliative care for people with dementia.8,12 The impact of dying and death without quality or dignity has a profound negative effect on not only the person, but also their family and healthcare professionals. 13
This rapid review aims to identify existing models of end-of-life care which are specific to people with advanced or end-stage dementia. The terms palliative care, and end-of-life care are challenging to separate and definitions for what constitutes end-of-life for persons with dementia are varied. 14 In this review, palliative care includes both a palliative approach to care from all care providers (as defined by Dementia Australia 15 ), delivered at any time the person with dementia has need of it during their illness, and/or a specialist palliative care service at the end of life (when death is judged as likely to occur within 12 months). 15
A model of care is defined as a multi-dimensional concept which defines the underlying principles and core components of healthcare and other services delivered to patient or population groups, including how a person might access and travel through such services.16,17 An integrated model of care for people with advanced dementia was identified by the Central Coast Local Health District (CCLHD) in New South Wales, Australia, as a local priority. A research team from CCLHD was supported by a grant to develop a co-designed model of care for people with advanced dementia and their carers. A rapid review to identify existing models was chosen as it offers an efficient approach to identify and summarise existing published evidence in a timely and cost effective manner. 18 Findings of the review, together with results of a clinical audit and a survey of bereaved carers of people who died with dementia, supported the development of a model of care.
Methods
Design
A rapid review methodology was used to identify published articles and grey literature to answer the question, what models of integrated, palliative care currently exist for people in the advanced and end-stages of dementia? As the main purpose of the review was to summarise information about existing models of care, quality appraisal of the evidence sources identified was not included and a narrative summary of the findings was planned. 18
Inclusion and exclusion criteria
The inclusion and exclusion criteria are listed in Table 1 below.
Inclusion and exclusion criteria.
Search strategy
A six-step search strategy was used: (1) an initial scoping search was run in PubMed, resulting in a test set of 20 citations to articles assessed by review team members as relevant to the topic; (2) the articles’ PubMed unique identifiers were entered into the PubMed PubReminer (https://hgserver2.amc.nl/cgi-bin/miner/miner2.cgi) open source data mining tool and a frequency table of Medical Subject Headings (MeSH) and keywords was produced; (3) the frequency table then informed development of a logic grid of MeSH terms and keywords relevant to the concepts of advanced dementia, palliative care and models of care; (4) MeSH terms and keywords were then used separately and in combination with Boolean operators (e.g. OR, AND) to search the Medline (Ovid) database; and (5) the search strategy was then adapted for the following databases: Embase (Ovid), CINAHL (EBSCO), PsycINFO (Ovid), ProQuest, Informit Collection, Joanna Briggs Institute, The Cochrane Library, The Campbell Collaboration and Google Scholar. Searches were run in April 2021 and updated in November 2021 and April 2022. The final step (6) used citation tracking, reference lists, Google Scholar, Google advanced searching and hand searching of key journals to identify further relevant sources. The search strategy for the Medline (Ovid) database is provided in Supplemental File 1.
Study selection
Retrieved references underwent up to three stages of screening using title and abstract, with the initial screening performed by a single reviewer (SL). A smaller number of articles (n = 264) were then reviewed by two independent team members (two out of SL, NG, SC, SJ, DD and CC) for full-text retrieval. Any disagreements were resolved via further screening by a third reviewer (ZT) or, in a few cases, the review team. The selected articles were then divided between team members for full-text screening and selection. The review team included healthcare professionals working in palliative, end-of-life and dementia care contexts, social scientists experienced in conducting systematic and literature reviews and a senior health librarian. Additional articles identified during full text review also underwent multiple screening processes to arrive at a final set of articles for inclusion in the review.
Data extraction and analysis
Data extraction and analysis took place in three stages. First, data from included studies were extracted by all authors in a template developed by the review team (Supplemental File 2) and then three reviewers (SL, CC and ZT) summarised in table format data including citation details, context (country, delivery setting), intervention and funding details and whether studies or models had been evaluated.
Next, the European Association for Palliative Care framework for optimal palliative care for older people with dementia 12 was used as a best practice guide against which the included models of care were mapped. The framework has successfully been used for conducting quality appraisals and mapping palliative care domains.8,20 We adapted the framework in the following ways: (1) the first domain, which considers the appropriateness of palliative care for advanced dementia, was removed because models of end-of-life care for people with dementia are based on the premise that advanced dementia requires palliative care; (2) domains 2 and 3 (relating to person-centred care, shared decision-making, setting care goals with the person with dementia and their family and advance care planning) were combined into a single domain as these often overlap in practice; (3) domains 6 and 7 (relating to avoiding burdensome treatment and optimising treatment to provide comfort), were combined into one domain; we expanded domain 10 (relating to education of the healthcare team) to include other workforce issues such as communication, collaboration and barriers to integration. The adapted European Association for Palliative Care framework with nine domains is shown in Table 2.
Dementia-specific end-of-life model of care framework: 9 domains a .
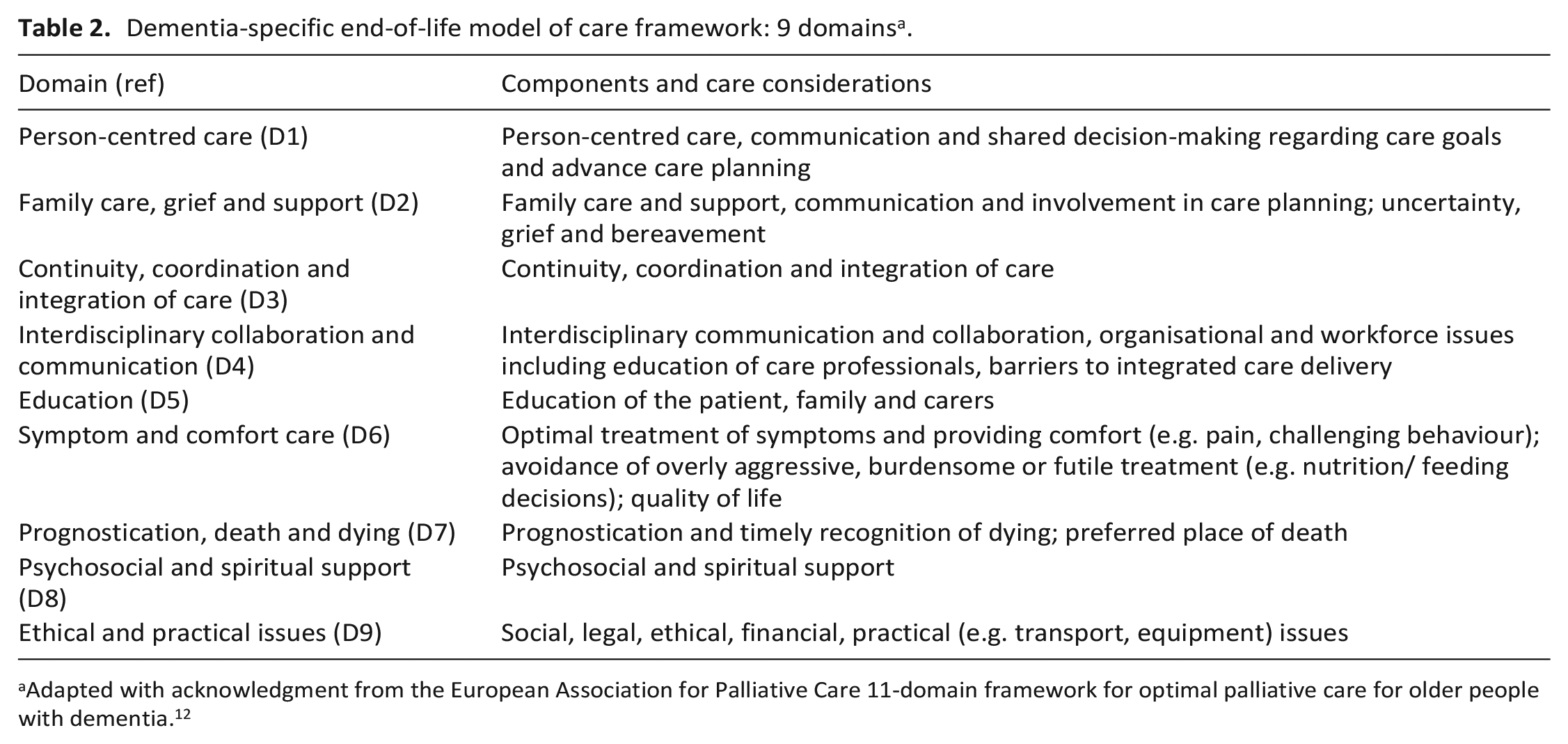
Adapted with acknowledgment from the European Association for Palliative Care 11-domain framework for optimal palliative care for older people with dementia. 12
Finally, the extracted data were presented in a narrative summary which highlights four main issues critical for rapid translation of findings from the review to inform development of a local model of care.
Results
An overview of the included models of care is provided, followed by a narrative summary organised according to the following issues: referral and admission to care, integration of care, evaluation and sustainability.
Study selection
A total of 1098 records resulting from searches of databases and other sources were screened at title/abstract stage; a total of 54 full text articles and reports were assessed for eligibility; and a final set of 19 studies describing 12 models of care was selected for inclusion in the review. The PRISMA 21 flowchart (Figure 1) summarises the study identification and selection process.
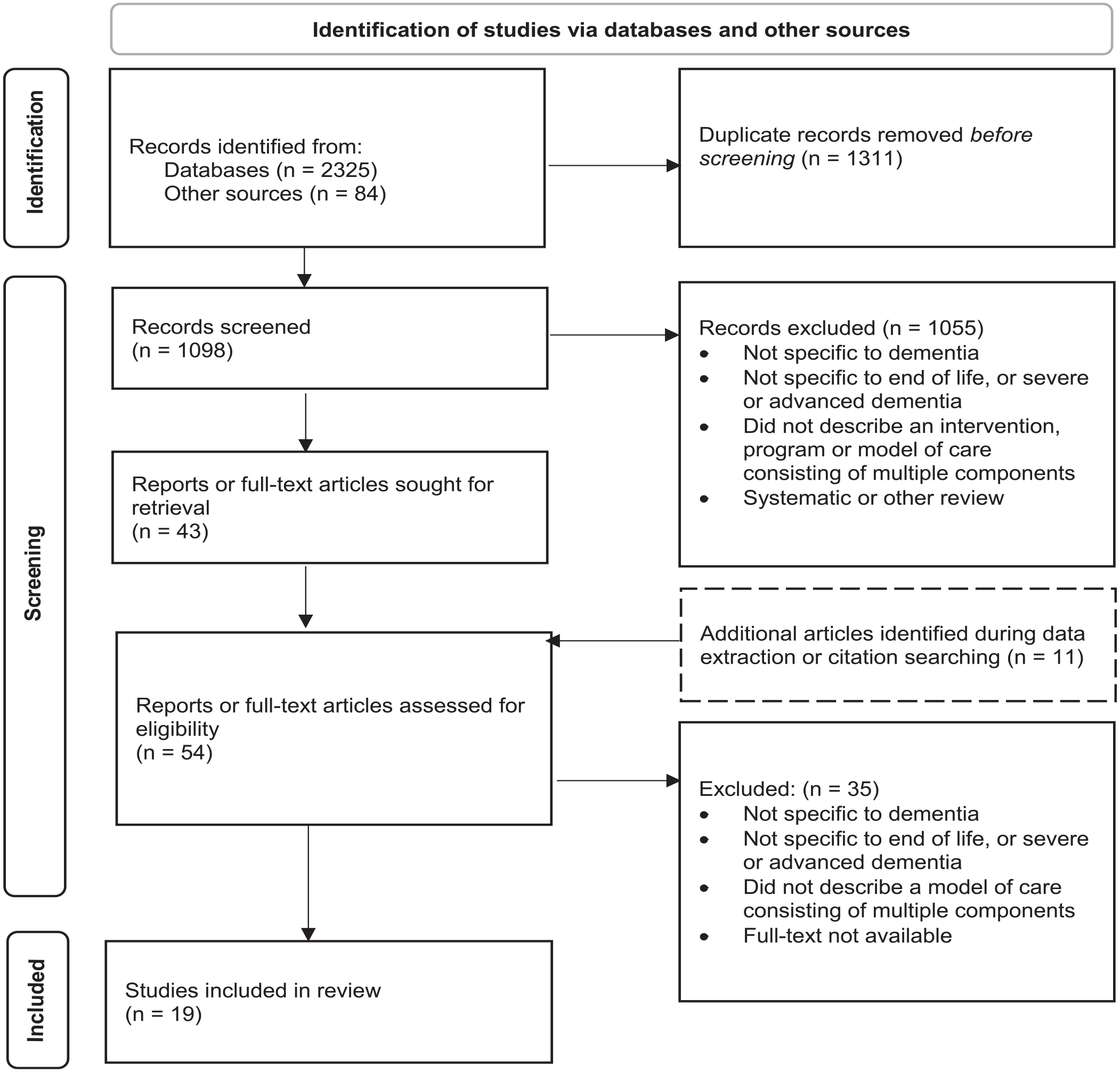
PRISMA diagram: identification, screening and selection of articles.
Description of included studies
All the included models of care were complex interventions comprising multiple components and services delivered by a range of healthcare professionals. The key components of each model of care are described in Table 3. Delivery settings for the models of care included residential aged care (n = 5),13,22–29 hospice (including hospice in the home; n = 5),28–33 community and home-based care (n = 9),3,13,27–29,31–37 primary care clinics (n = 2),28,29,37 and hospital (acute care; n = 4)3,13,27–29,35,36settings. Some models were delivered in multiple settings. Four models of care were located in England,23–26,32,33,37 three in both Australia22,27,34 and the United States,13,28–30,38 and one each in Singapore3,35,36,39 and Wales. 31
Key components of models of care.
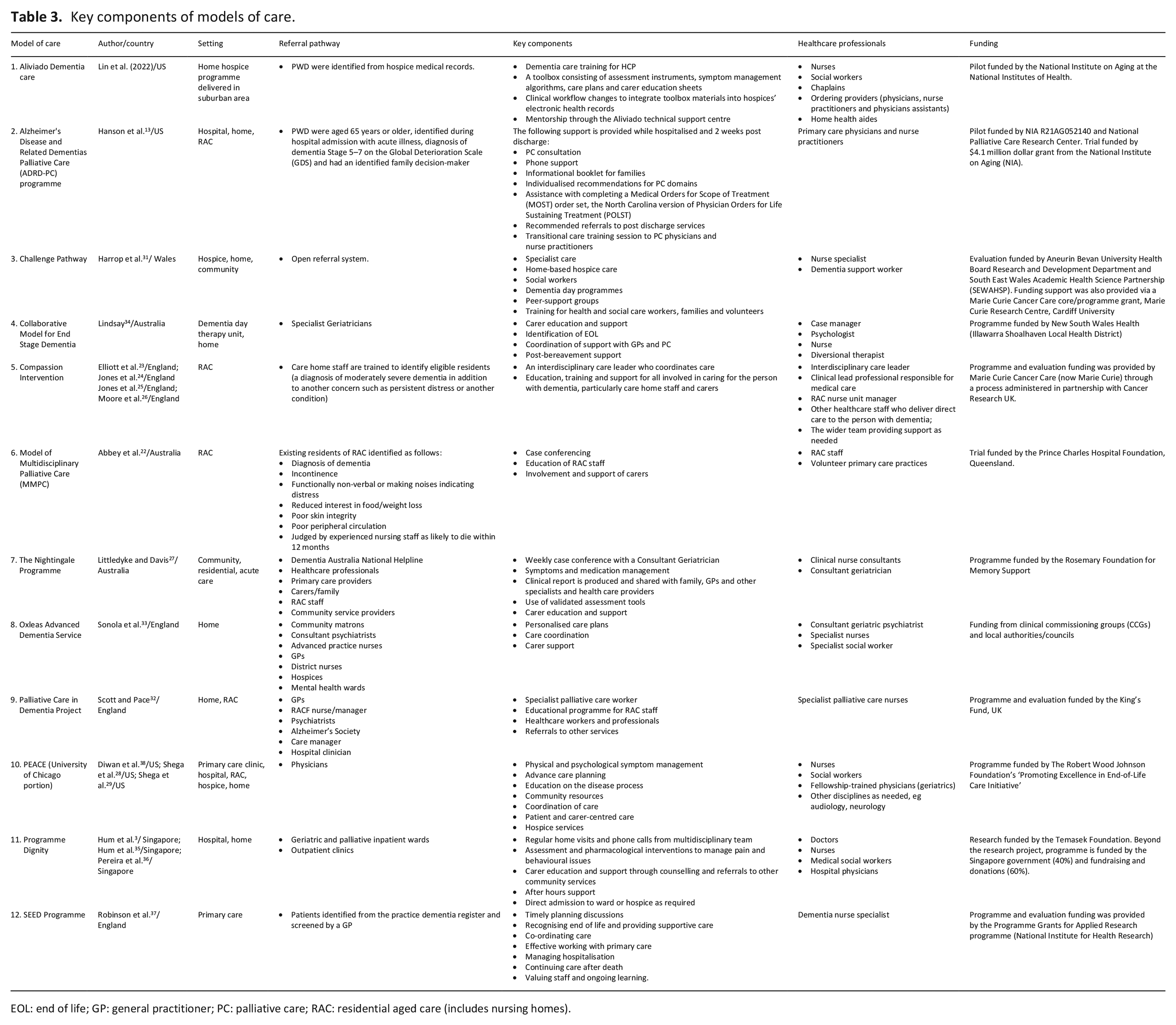
EOL: end of life; GP: general practitioner; PC: palliative care; RAC: residential aged care (includes nursing homes).
The study designs used to test or evaluate the models included a randomised controlled trial, 37 a pilot trial, 13 feasibility studies,23,28–30,37 impact and process evaluations,31,33,37 and a prospective cohort study.3,35,36 Qualitative, quantitative and mixed methods were used in the included papers (e.g. surveys, interviews, patient chart/ medical record audits, field notes, ethnographic observations, case study). Some models of care were described in a single paper; other studies provided detailed descriptions and evaluations of care models in two or more papers and reports, implementation manuals and/or online websites. Two models had not been systematically or formally evaluated.27,34 See Table 4 for a summary of evaluation of the included models of care.
Evaluation of models of care.
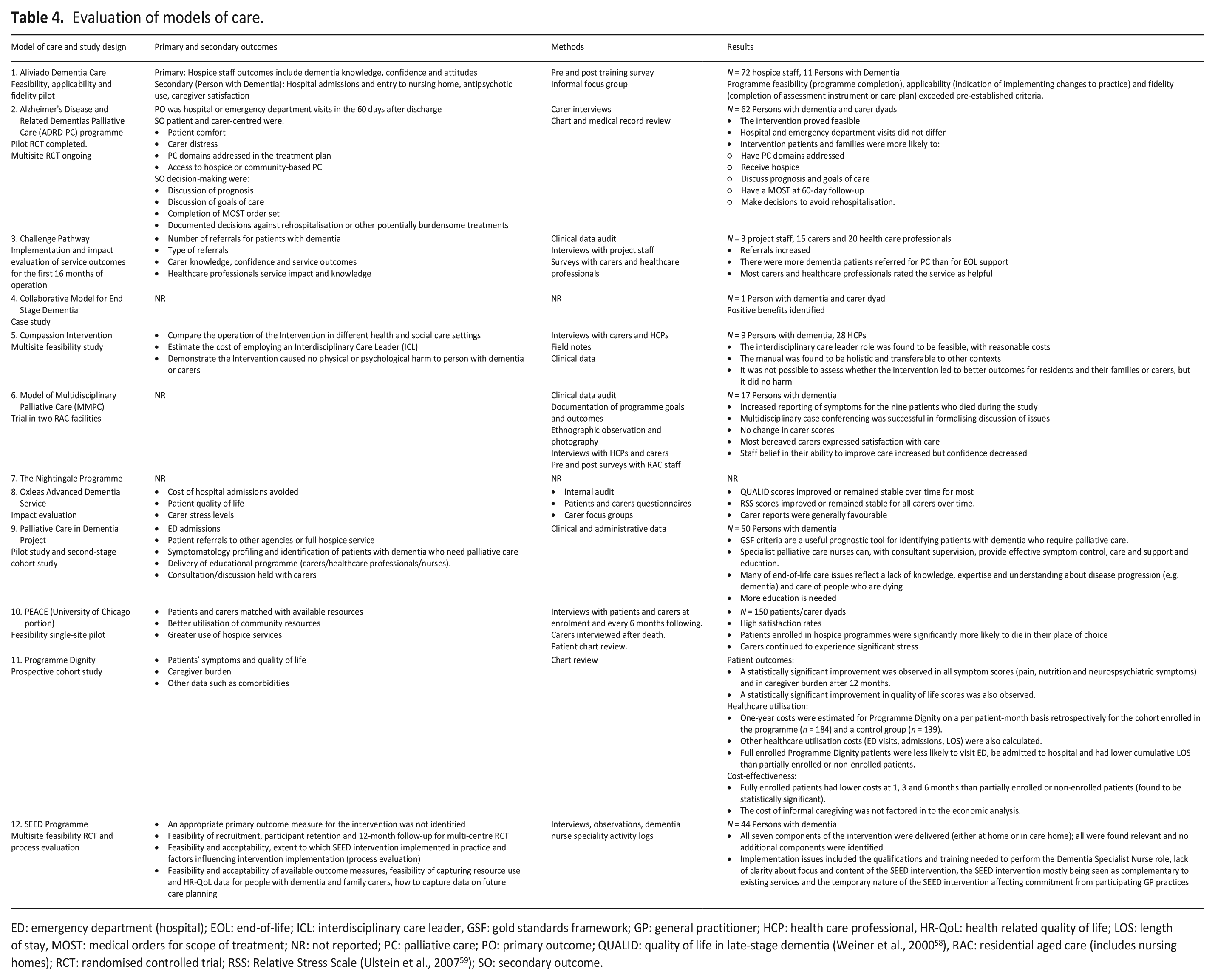
ED: emergency department (hospital); EOL: end-of-life; ICL: interdisciplinary care leader, GSF: gold standards framework; GP: general practitioner; HCP: health care professional, HR-QoL: health related quality of life; LOS: length of stay, MOST: medical orders for scope of treatment; NR: not reported; PC: palliative care; PO: primary outcome; QUALID: quality of life in late-stage dementia (Weiner et al., 2000 58 ), RAC: residential aged care (includes nursing homes); RCT: randomised controlled trial; RSS: Relative Stress Scale (Ulstein et al., 2007 59 ); SO: secondary outcome.
Domains and components of end-of-life care
Analysis and mapping of the included models of care against the nine domains of optimal palliative care for people with dementia showed that not all domains were consistently met (see Table 5). The domain for which there was the least demonstrated evidence was ethical and practical issues (D9), followed by psychosocial and spiritual support (D8) and person-centred care (D1). For some models of care, the supporting evidence for each domain was minimal or difficult to identify.
Included models of care mapped to the nine domains of palliative care.
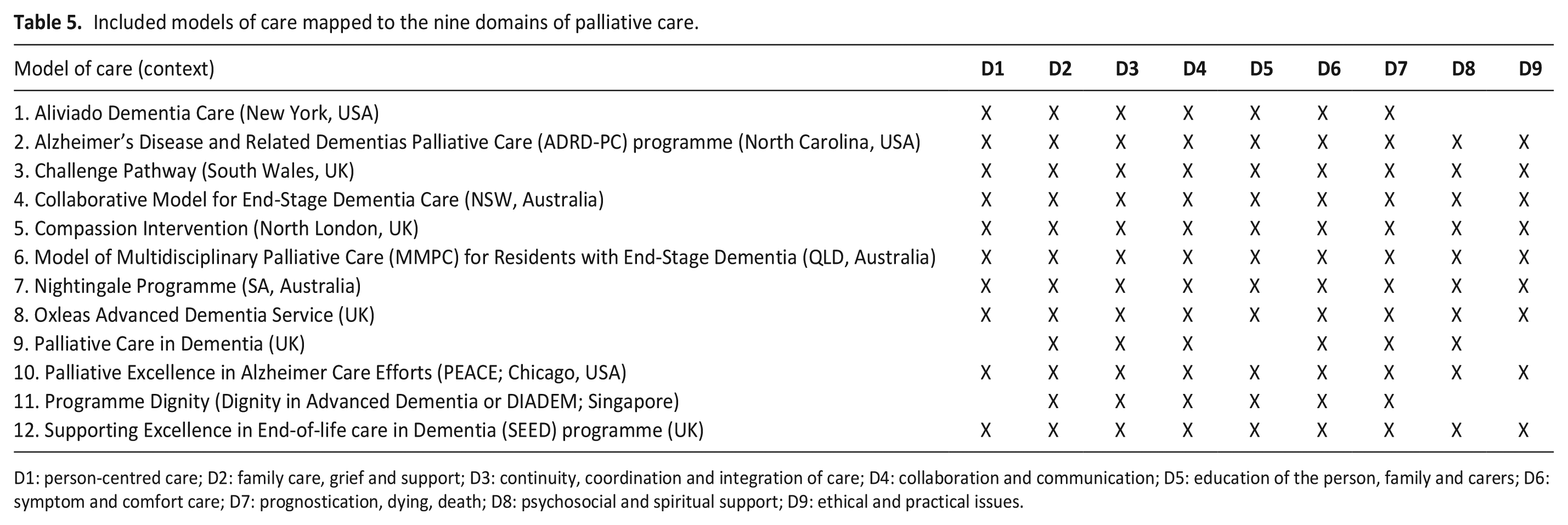
D1: person-centred care; D2: family care, grief and support; D3: continuity, coordination and integration of care; D4: collaboration and communication; D5: education of the person, family and carers; D6: symptom and comfort care; D7: prognostication, dying, death; D8: psychosocial and spiritual support; D9: ethical and practical issues.
Practical examples of how each of the domains of care was demonstrated in the included models were limited for the following reasons:
lack of detail in the reporting of some models of care, for example the Challenge Pathway 31 and the Collaborative Model for End-Stage Dementia 34 ;
resources were not freely available, for example the Aliviado Dementia Care resources 40 ; or
resources no longer exist, for example the Massive Open Online Course (MOOC) developed for carers of people with advanced dementia as part of the SEED Programme. 37
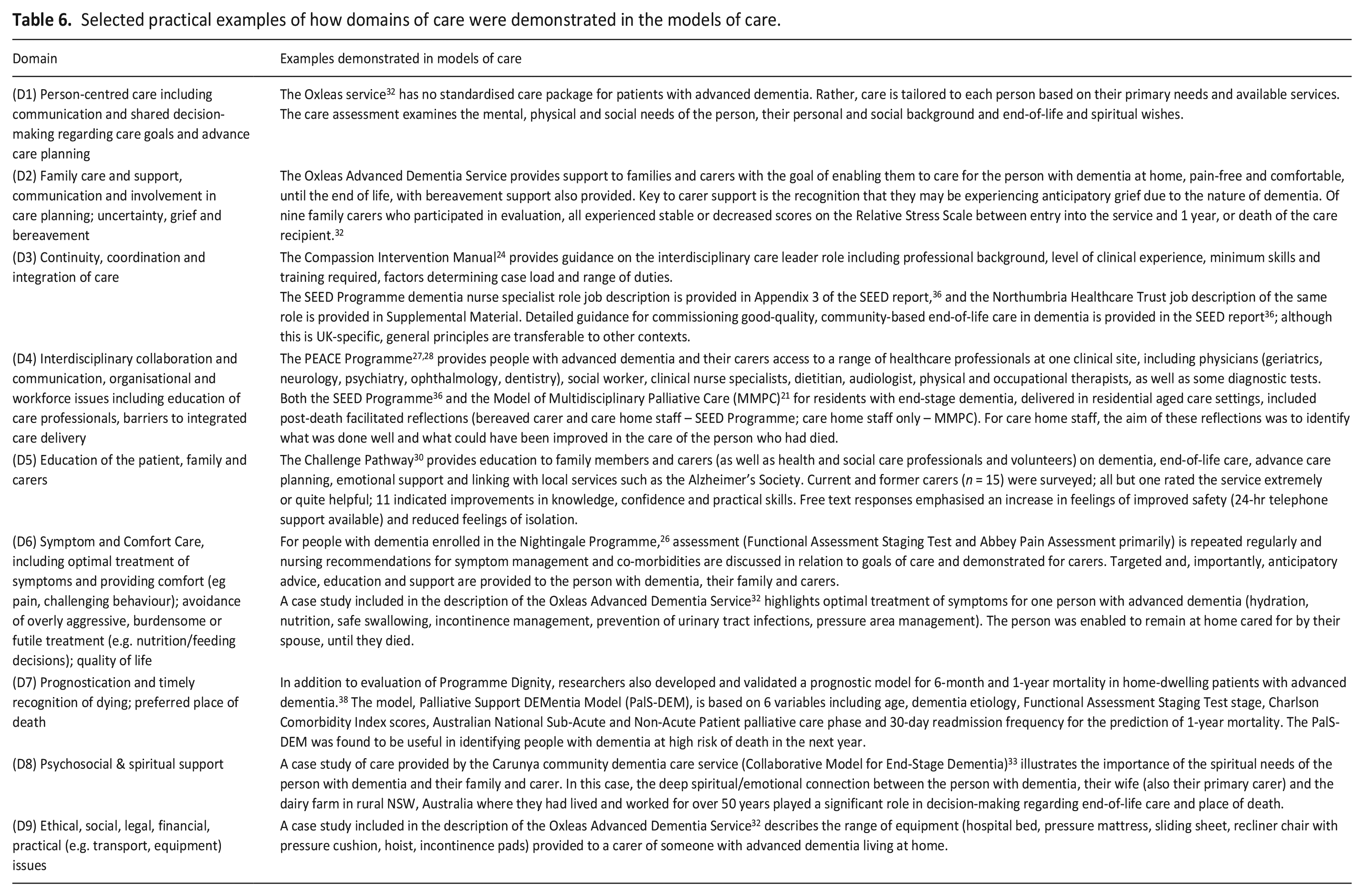
However we have selected practical examples of how the domains of care were demonstrated, which may be useful to readers seeking to develop a locally-responsive model of care for people with advanced dementia (see Table 6).
Selected practical examples of how domains of care were demonstrated in the models of care.
Referral and admission to care
The included models of care demonstrate a range of referral pathways and assessment for admission to a palliative care service or programme (see Table 3 for details). People with dementia were admitted to the models of care based on criteria that were often described in general terms, for example being likely to derive benefit from the intervention. In a few cases criteria were provided in more detail. For example, inclusion in the Model of Multidisciplinary Palliative Care (MMPC) programme depended on a number of the following admission criteria: existing resident of a residential aged care facility, diagnosis of dementia, incontinence, functionally non-verbal or making noises indicating distress, reduced interest in food/weight loss, poor skin integrity, poor peripheral circulation, judged by experienced nursing staff as likely to die within 12 months. 22 Evaluation of Programme Dignity included development and validation of a prognostic model (the PalS-DEM model) for 6-month and 1-year mortality in people with advanced dementia living at home. 39 None of the included studies reported any analysis regarding accuracy of prognostication, in other words, whether the study/programme participants were appropriately identified for the interventions delivered, and whether they were admitted into the model of care at the appropriate time based on their level of need.
Integration of care
All included models had elements of integrated care (such as a care coordination role, interdisciplinary collaboration and person-centred care); but the level of integration varied considerably. Issues considered in relation to evaluating the degree of care integration provided by the models were: duration of care, location of care, care coordination role, interdisciplinary collaboration and communication and evidence of person-centred care.
Duration of care
Duration of care varied from a brief, time-limited intervention such as the ADRD-PC programme (specialist inpatient palliative care consultation, information and referrals to post-discharge services, covering the period of hospitalisation and 2 weeks after discharge), 13 to the majority of models in which care was provided to the person with dementia from enrolment in the programme to their death. Some models such as the Collaborative Model for End Stage Dementia 34 and the SEED Programme, 37 also provided post-bereavement support to families and carers.
Location of care
Several models of care were specific to one care location only. For example, the Compassion Intervention23–26 and the MMPC 22 were developed for residential aged care (RAC), with an emphasis on education and training in both dementia care and palliative care for RAC staff. Other models, such as Aliviado Dementia Care, 30 the Challenge Pathway 31 and the Oxleas Dementia Service, 33 provided hospice-in-the-home care. In contrast, Programme Dignity3,35,36 spans a number of locations of care, all of which may be needed during the advanced stage of dementia. In addition to a range of support provided to families caring for someone with dementia at home, the programme also provides after hours support and direct admission to acute or hospice care if needed. Importantly, all members of the team have access to patient information in the national medical health records, which are also accessed by hospital and hospice staff if the patient is admitted to either facility.
Care coordination role
A common inclusion in the models reviewed was the use of a dedicated Clinical Nurse Consultant, Palliative Care Nurse or Social Work Coordinator (n = 9), whose role was to identify and enrol people with dementia (and their family and carers) into the service; conduct assessments; communicate regularly with consultant geriatricians, specialists, general practitioners, allied health and palliative care providers (e.g. through weekly case conferences) to ensure continuity of care and assist with care planning; provide education to healthcare professionals, people with dementia, their carers and families about dementia and end-of-life issues (e.g. stages of dementia disease progression, symptom management/ comfort care, what to expect when death is approaching); and provide referrals to outside support such as bereavement counselling for carers. Some models such as the Challenge Pathway 31 and Oxleas Advanced Dementia Service 33 also provided access to 24/7 crisis support for carers supporting a person with dementia in their home.
Person-centred care
Person-centred care, defined by the Australian Commission on Quality and Safety in Health Care as ‘care that is respectful of, and responsive to, the preferences, needs and values of the individual patient’, 41 was implied in all the included models of care. However, the level of evidence varied and clear evidence of person-centred care, including advance care planning, was not identified in either the Palliative Care in Dementia 32 model or Programme Dignity.3,35,36 In many of the models of care, the main mechanisms whereby the person with dementia was included in decisions relating to their care appeared to be advance care planning, (in other words, decisions made according to goals and wishes documented in the past) and interpretation of the person’s wishes by family and carers. The review found scant evidence of supported decision-making for people with advanced dementia. The ‘supportive toolbox’ of ‘skills, strategies, techniques and resources’ required by healthcare professionals to enable people with even advanced dementia to have meaningful involvement in decision-making is an area for further research. 42
The people with dementia receiving care within each of the included models were generally described in terms of demographic detail and symptom profile. Other information, such as culturally and linguistically diverse backgrounds, Indigenous populations or identification as LGBTIQ+, was not included. Therefore, it is not known whether these models potentially benefit diverse populations of people with dementia.
Evaluation of models of care
Primary and secondary outcomes reported in the included studies targeted patient- and carer-level outcomes (such as symptom control, evidence of advance care planning, documentation of care goals, carer distress/satisfaction/confidence and knowledge, preferred place of death achieved); care provider outcomes (such as increased knowledge and confidence in delivering care, acceptability of changes in practice); and system-level outcomes (such as improved accuracy and completeness of clinical documentation, avoidance of hospital admission, cost of employing a care coordinator, utilisation of community resources). Few models were evaluated using large, robust study designs; most were feasibility studies23,28–30,37
Sustainability
Some of the models of care included in the review, such as the SEED Programme 37 and the MMPC, 22 had ceased operating. Reasons for this were unclear but could be assumed to be lack of funding beyond the initial pilot phase, which was dependent on research project funding. Insufficient human resourcing and/or reduced feasibility due to changes in health care policy, guidelines and delivery systems may also have been factors. For other models of care such as the Challenge Pathway 31 and the Collaborative Model for End Stage Dementia, 34 it was unclear whether they were still operating.
Implementation of three models of care included production of detailed documentation which is freely available. Pro-forma documents such as assessments, work instructions, flowcharts and audit tools, were developed during the trial of the MMPC and are included as appendices in the final report. 22 The SEED Programme report 37 provides a range of useful documents such as a job description for a dementia nurse specialist and an activity checklist for timely end-of-life care planning discussions with people with dementia and their families. Similarly, the Compassion Intervention Manual 25 provides detailed guidance on commissioning and implementation of the intervention, although it is unclear whether it has been implemented beyond the initial pilot in two nursing homes in North London between 2014 and 2015. Resources such as these enhance the impact of models of care by facilitating transfer of the model to other contexts.
Discussion
The review identified relatively few models of palliative care for people with advanced dementia, and these varied considerably in setting, scope, degree of integration of services and evaluation. All models demonstrated at least some evidence of at least six of the nine domains of optimal palliative care (based on the 11 EAPC domains 12 ). From the narrative summary of the included models, the following four main issues emerged as key to successful translation of the research evidence into a local pilot model of care.
Referral and admission to care
Despite a range of referral pathways to a palliative care service or programme, the included models of care provide limited insights about when, where and how to identify people with advanced dementia who are in need of end-of-life care and to initiate such care. Where the criteria for admission were provided, people with dementia have to demonstrate a significant level of deterioration from multiple and complex symptoms to be offered interventions. 25 Yet the burden of symptoms is not the whole picture; admission to care should also encompass the psychosocial needs of people with dementia, their families and carers. 14 Programme evaluation of models of care for people with advanced dementia should also include investigation of referral pathways and admission criteria to identify whether these were needs-based and applied consistently. This review also showed that accurate prognostication for people with advanced dementia was not a major element of most of the included models of care. Prognostication tools to accurately identify people in need of end-of-life care (e.g. the Supportive Palliative care Indicators Tool (SPICTTM)43,44 have been developed and implemented successfully. However tools that rely on a chronological disease trajectory are less useful for people with advanced dementia, and recent research has identified lack of consistency in how end of life in dementia is defined, and called for a move beyond prognostication to a needs-based approach. 14
Integration of care
Traditional models of palliative care are designed to be delivered in the last 6 months of life. Given the variable disease trajectory of dementia, a longer-term palliative approach to care is needed for people with advanced dementia. A relatively brief, time-limited model of care such as the ADRD-PC programme 13 may provide only short-term benefits for people with advanced dementia; this is acknowledged by the authors of the study. Models built around one care delivery location, for example residential aged care,22,24,26 run the risk of fragmenting care when transitions between care locations are required, for example an acute medical episode requiring hospitalisation.
The models that provided care from the time the person and their family/carer enrolled in the service until their death, and in some cases post-bereavement support, and included a care coordinator role, and were not specific to one care location, were better aligned with the optimal domains of palliative care for people with advanced dementia. For example, the Nightingale Programme based in South Australia, 27 is an integrated model of care (referrals accepted from a range of sources; nursing assessment, care planning, interdisciplinary collaboration, coordination of services provided by a care coordinator; and support for carers), in which the person with dementia remains until their death, regardless of whether their care setting changes.
Best practice models of palliative care should be built around the person with dementia, regardless of their care setting, and how long they need to receive care. Most importantly, while best practice models of care should incorporate all nine domains of palliative care, they should also be flexible enough to take into account the needs of each individual, particularly regarding psychosocial and spiritual support, and needs relating to self-determination, familiarity and safety.2,45
This applies particularly to people with dementia who are Indigenous, or identify as LGBTIQ+, or live in rural or remote locations, or are culturally or linguistically diverse or live with a disability. While consideration of these factors should be implicit in person-centred care, it is worth noting explicitly that they may impact access to, and suitability of, dementia palliative care. For example, a recent scoping review identified a gap in the literature on dementia palliative care in rural areas, and a need for more research on whether technology can be used to mitigate barriers to accessing care. 46
The Australian Commission on Quality and Safety in Health Care identifies one of the key dimensions of person-centred care as involvement of carers and family. 41 Therefore the emotional, psychological, spiritual and practical support needs of family carers should be considered in any model of dementia palliative care. Ideally, families and carers should be meaningfully engaged in shared decision-making processes with healthcare professionals involved in providing care. 6
The quality of end-of-life care and death experience is shaped by the care needs, preferences and experiences of both the person with dementia, and their carer and family. 47 The needs of family carers and the person with dementia are often interdependent (but not always congruent).5,48 For example, interviews with residential aged care staff and review of case notes for people enrolled in the MMPC model of care revealed several instances in which the person with dementia had an advance care directive but their family member was reluctant for it to be followed. 22 It is important therefore, that families and carers are appropriately engaged in care planning and considered when developing end-of-life models of care.
It could be argued that palliative care should be offered at the point of diagnosis for any life-limiting illness including dementia.
However some people with dementia may not welcome a palliative approach to their care soon after diagnosis. They may not be ready to discuss advance care plans or end-of-life decisions, or even seemingly minor issues such as eating and drinking problems.49,50 Models of care that continuously and gradually support people with dementia through all stages of their experience of the disease, are likely to provide the best opportunity for them to have meaningful engagement in care decisions and experience person-centred care.
Evaluation of models of care
The wide range of outcome measures used in evaluating some of the included models of care indicates the difficulties in assessing the effectiveness of complex interventions to improve end-of-life care for people with dementia. Further research is needed to develop methodologies for evaluating the effectiveness of complex models of care in real-world settings, including (1) outcome measures for patients, carers and healthcare professionals that are targeted, easy to deliver and not burdensome 29 ; (2) patient and carer experience measures that capture a more nuanced picture beyond the commonly used experience indicators of patient comfort and carer distress; and (3) quality indicators that focus on processes, outcomes and structure of care.
Evaluation of models of care should also take into account the costs of caring. Only two of the included models reported any economic evaluation measures, namely the Compassion Intervention which calculated the cost of employing a care coordinator 26 and the Oxleas Advanced Dementia Service which estimated savings due to hospital admissions avoided. 33 None of the models evaluated the substantial unpaid care provided by families and carers.
Sustainability
This review found very limited evidence to identify the conditions needed to support long-term sustainability of any model of end-of-life care for people with dementia, but it can be inferred that adequate, guaranteed ongoing funding of the programme and the position of care coordinator as a dedicated role, not an addition to other, existing duties, are key. In a resource-constrained environment, some organisations may have to be selective in which components of a model of care could be implemented depending on local context and availability of existing resources. However there is clear evidence to support what a best practice end-of-life model of care for people with dementia should look like,9,12,20 and ideally all domains of care should be addressed in any model. At the same time, this review demonstrates that models must be context responsive to be sustainable. Models such as the Compassion Intervention 25 and the MMPC 22 designed for residential aged care facilities will necessarily focus on different domains than models such as the Challenge Pathway 31 and the Nightingale Programme 27 designed to deliver care primarily in the community. Flexibility and agility to scale up or down as a pragmatic approach to implementing models of care may be needed to improve sustainability while managing deviation from the original design of the model. 51
What this study adds?
This rapid review provides an overview of end-of-life models of care that are specific to the needs of people with advanced or end-stage dementia. Examples of models of care are provided, including some with useful, freely available supplementary resources. Table 3 (Key components of models of care) and Table 4 (Evaluation of models of care) may be valuable sources of information for clinicians and health service managers seeking to develop a context-specific, model of end-of-life care for people with dementia. The selected practical examples of how the domains of care were demonstrated in the included models of care may also be useful (see Table 6).
Strengths and limitations of the study
The focus in rapid reviews is on rapidly producing high-quality evidence to support health system decision-making and policy in a time-limited and cost-effective manner 18 ; hence, an inherent limitation is that some articles may not be identified during searching. Furthermore, the pragmatic decision to use one reviewer for initial screening of references may have resulted in some relevant studies being excluded at this stage.
Publication bias may also be a limitation of this review. Some relevant models of care may not have been reported and others, implemented as research projects, may have continued after the life of the project but not reported further.
Screening for relevance was challenging due to definitional issues around the concepts of end of life for people with dementia 14 and models of care. 16 This ambiguity was reflected in the multiple and ongoing team discussions held in reaching consensus about several models found.
Further, several models of care were identified that were still under development and therefore not included in this review. These were the Model for Palliative Care Project (Ireland; https://pallcare4dementia.com/the-project/),52–54 the Partnership Model of Hospice Enabled Dementia Care (Ireland), 55 and the Empowering Better End of Life Dementia Care (EMBED-Care Programme; United Kingdom; https://www.ucl.ac.uk/psychiatry/research/marie-curie-palliative-care-research-department/research/centre-dementia-palliative-care). 56 An evaluation of the Partnership Model was published too late for inclusion in this review. 57 These models are noted here for monitoring and future review.
Conclusion
This review adds to the growing body of literature on end-of-life care for people with dementia by identifying and examining models of care implemented in a range of real-world settings. We sought examples of how the substantial body of evidence on the optimal components of a model of care for this vulnerable population group had been translated into practice and, ideally, evaluated and embedded in health and social care delivery. While a comprehensive, fully integrated, appropriately funded and sustainable model of care was not found, many of the included models offer valuable evidence to assist clinicians and healthcare managers to develop and implement best-practice, context-responsive models of end-of-life care for people with dementia.
Supplemental Material
sj-pdf-1-pmj-10.1177_02692163231171181 – Supplemental material for Models of care for people with dementia approaching end of life: A rapid review
Supplemental material, sj-pdf-1-pmj-10.1177_02692163231171181 for Models of care for people with dementia approaching end of life: A rapid review by Suzanne Lewis, Zoi Triandafilidis, Cassie Curryer, Sarah Yeun-Sim Jeong, Nicholas Goodwin, Sally Carr and Daneill Davis in Palliative Medicine
Supplemental Material
sj-pdf-2-pmj-10.1177_02692163231171181 – Supplemental material for Models of care for people with dementia approaching end of life: A rapid review
Supplemental material, sj-pdf-2-pmj-10.1177_02692163231171181 for Models of care for people with dementia approaching end of life: A rapid review by Suzanne Lewis, Zoi Triandafilidis, Cassie Curryer, Sarah Yeun-Sim Jeong, Nicholas Goodwin, Sally Carr and Daneill Davis in Palliative Medicine
Footnotes
Acknowledgements
All authors meet the criteria for authorship as stated by the ICMJE authorship guidelines. All authors contributed to the concept and design of this work and/or screening and review of articles and models of care, and/or co-wrote the article and/or provided critical intellectual review and/or translation of findings for policy and practice. All authors have given final approval of the manuscript to be submitted for publication. During the course of this review the authors contacted several researchers and teams also working in the area of end-of-life care for people with dementia, and we thank them for their prompt and generous responses.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Australian Government’s Medical Research Future Fund (MRFF) as part of the Rapid Applied Research Translation Programme. The project was funded through a NSW Regional Health Partners Financial Agreement with Central Coast Local Health District for ‘Capacity building in research for palliative care staff to enable a better end-of-life experience for the Central Coast Community’. The funding body did not have any role in data analysis, interpretation and the writing of this manuscript.
Ethical approval
Ethical approval for this review was not required (Non-Research Activity application 0221-013C; Central Coast Local Health District Research Office, March 2021). The review protocol and registration was managed as part of the MRFF Palliative and End of Life Care Project contract and was not registered externally.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.