
Abstract
Objective
To conduct a systematic review of the effectiveness of facial exercise therapy for facial palsy patients, updating an earlier broader Cochrane review; and to provide evidence to inform the development of telerehabilitation for these patients.
Data Sources
MEDLINE, EMBASE, CINAHL, Cochrane Library, PEDro and AMED for relevant studies published between 01 January 2011 and 30 September 2020.
Methods
Predetermined inclusion/exclusion criteria were utilised to shortlist abstracts. Two reviewers independently appraised articles, systematically extracted data and assessed the quality of individual studies and reviews (using GRADE and AMSTAR-2, respectively). Thematic analysis used for evidence synthesis; no quantitative meta-analysis conducted. The review was registered with PROSPERO (CRD42017073067).
Results
Seven new randomised controlled trials, nine observational studies, and three quasi-experimental or pilot studies were identified (n = 854 participants). 75% utilised validated measures to record changes in facial function and/or patient-rated outcomes. High-quality trials (4/7) all reported positive impacts; as did observational studies rated as high/moderate quality (3/9). The benefit of therapy at different time points post-onset and for cases of varying clinical severity is discussed. Differences in study design prevented data pooling to strengthen estimates of therapy effects. Six new review articles identified were all rated critically low quality.
Conclusion
The findings of this targeted review reinforce those of the earlier more general Cochrane review. New research studies strengthen previous conclusions about the benefits of facial exercise therapy early in recovery and add to evidence of the value in chronic cases. Further standardisation of study design/outcome measures and evaluation of cost-effectiveness are recommended.
Introduction
Bell's palsy is the most common form of acute spontaneous peripheral facial paralysis, with poor recovery affecting a patient's long-term quality of life. 1 The cause still unclear, 2 although the condition has long been associated with reactivation of latent virus infection, 3 with evidence showing a rise in incidence in the United States thought to be linked to increasing herpes infection rates. 4 The majority (60%) of these facial nerve paralysis cases are Bell's palsy, 5 and this condition affects 11–40 people per 100,000 in the population each year, most commonly in the age group 30–45. 6 It is also estimated that one in sixty individuals will be affected over the course of their lifetime.7,8 Population studies show that facial palsy is more commonly associated with people who are immunocompromised or pregnant, or those with obesity, hypertension, diabetes, or upper respiratory conditions.1,7,9 With the appearance of COVID-19 caused by SARS-CoV-2, reports are also emerging of Bell's palsy as a presenting symptom this for infection.10,11 Although most patients eventually recover without any treatment,6,12 one in three (29%) have a poor recovery resulting in a permanent deficit of facial function.6,13 This can affect important functions such as eating and speaking, 14 or non-verbal communication mediated by expression of emotion (e.g. smiling), 15 as well as chronic facial pain.6,16 Patients living with incomplete recovery experience long-term psychological distress and depression, with many moving away from public-facing roles resulting in social alienation.6,16–19
The evidence base for therapy in acute and chronic cases remains limited. Currently, a range of treatment options may be offered, with a recent study identifying considerable variation in the care pathways experienced by patients in the United Kingdom. 20 These range from medication and physical therapies to surgery. Evidence of the effectiveness of surgical interventions remains limited, with a Cochrane systematic review reporting insufficient proof of benefit and further trials judged to be unlikely. 21 Cochrane reviews have identified one pharmaceutical treatment (prednisolone) as an effective treatment (versus placebo) for Bell's palsy, but only if administered within 72 h of symptom onset.22–24 Use of adjunctive antiviral therapy was reported to be of uncertain value, 22 although more recent evidence of its value in the treatment of Ramsay Hunt syndrome, the second most common cause of facial palsy, has emerged. 25 In addition to medication, a number of physical therapy options are available. Facial exercise therapy (facial neuromuscular retraining) is the most widely evaluated.26–31 A Cochrane review of physical therapies published in 2011 reported some evidence that facial exercise therapy could improve facial function for moderate paralysis and chronic cases and reduce sequelae in acute cases, but it recommended the need for further studies. 32 We have therefore undertaken a systematic review to identify and appraise any further studies that have examined the effectiveness of facial exercise therapy. Updated evidence on effectiveness is required to inform the planned development of facial remote activity monitoring eyewear to enable telerehabilitation in a patient's own home.20,33
Aims and methods
The review aimed to identify and assess recent evidence of the effectiveness of facial exercise therapy, draw out any clinically relevant findings, and identify future research needs. The review protocol was submitted for peer-review to the International Prospective Register of Systematic Reviews (PROSPERO), ID: CRD42017073067. 34 A mixed-methods approach to evidence synthesis was specified in the protocol to allow for the inclusion of different study designs, in addition to randomised controlled trials.35,36 The peer-reviewed protocol also specified the inclusion of evidence from post-2011 reviews to maximise the evidence identified. There was strict adherence to international guidelines on Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). 37
Literature searches were undertaken by an Academic Librarian (CB) qualified in systematic reviews. Databases searched included MEDLINE, EMBASE, CINAHL, Cochrane Library (Database of Systematic Reviews and Central Register of Controlled Trials) and PEDro; plus the Allied and Complementary Medicine Database). The latter was not included in the original Cochrane review. Searches were replicated covering the period 1 January 2011 to 30 September 2020, allowing for a slight overlap with the search end date (28 February 2011) of the earlier Cochrane review. 32 Tailored search strategies were used for the six databases and details are presented in Appendices 1–6.
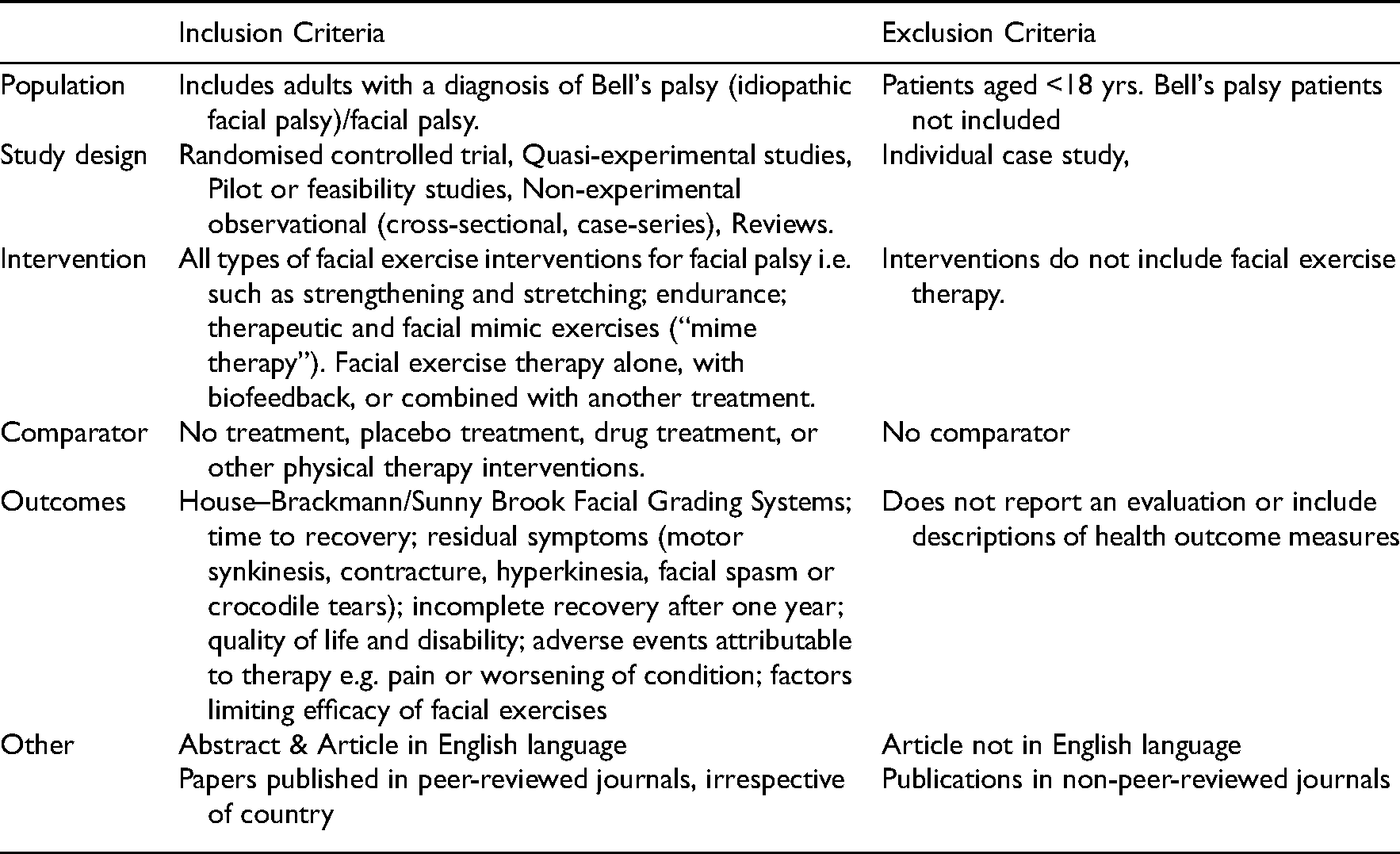
Abstracts were screened against predetermined inclusion/exclusion criteria (see Table 1), and abstracts shortlisted against these. Study designs included both individual studies and reviews. All identified records were first imported into the Refworks Pro database. A separate file was prepared for each database. Full articles were downloaded and shortlisted based on content by two independent reviewers (blind review). Shortlists were compared by a third reviewer and any differences resolved by discussion between the two original reviewers; if arbitration was required this was provided by another member of the review team (AK, AS, CT, HM, and DT participated in this process).
Selection criteria.
Shortlisted articles were read carefully and assessed by two independent readers (AK and DT) for inclusion in the review. Some articles were discarded if these repeated information provided in another version. Details of all articles were entered into an Endnote library and bibliographies were scrutinised to identify possible additional studies. Screening and shortlisting data were presented as a PRISMA flow diagram. 37
For data extraction and management, articles were organised into two groups (i) individual primary research studies and (ii) reviews. Summary Tables were piloted for data extraction from both types of articles. Common information extracted from all articles included author names, publication date, and country of publication. For individual research studies, additional data recorded included: study design; sample size & patient demographics; details of clinical diagnoses/conditions; details of intervention and comparator(s); outcome measures; main findings; and conclusions. For review articles, data extracted also included type and number of studies reviewed, publication dates, and total number of patients. Information was extracted and entered into the Summary Table initially by two author (AK, DT). This was then checked and amended and expanded where necessary by other reviewers, separately for individual studies (CT, HM, AS) and for reviews (CN, SP).
Quality assessment was undertaken using validated tools. For individual research studies, quality and risk of bias were assessed using GRADE (Grades of Recommendation, Assessment, Development, and Evaluation) appraisal tools.38,39 Assessment was performed independently by pairs of reviewers (AK, CT, HM, and DT). Studies were categorized into three levels of bias (low, unclear, and high risk of bias); a third researcher (AS) assisted with any disagreements that arose. For the published reviews shortlisted, quality was assessed using AMSTAR-2 by two independent reviewers (SP, CN). Confidence in the quality of each review was categorised as high, moderate, low, or critically low, based on the number of critical and non-critical flaws identified. 40
In preparation for final analysis, all papers were read in full, with data and results extracted, regardless of the study design (AK, CT, HM, and AS participated in this process). For individual studies, data entered into the Summary Table included study design, diagnoses, therapies considered, results, limitations, and study quality rating. A further table collated the main findings and conclusions drawn (CT, HM, AS, SP, CN). As anticipated, authors used differing study designs, papers considered a mix of therapies and controls, and adopted different outcome measurement tools. Statistical combination of numerical data from separate studies to strengthen review conclusions (meta-analysis) was not possible due to variations in study design and quality. A thematic analysis framework was therefore used to create a descriptive synthesis and address the heterogeneity of studies identified. 41 Where available, the results of individual randomised controlled trials were reported separately, as were the findings of cohort studies. The authors coded all the studies before discussing and agreeing on descriptive categories and themes for synthesis.
Results
Figure 1 presents a PRISMA flow diagram summarising the review process. The database searches identified a total of 4943 titles and abstracts for possible inclusion. A total of 58 articles were shortlisted for the review; seven further articles were discarded because only the abstract was in the English language. In total, 51 articles were selected for reading the full text; 22 further papers were removed, with reasons recorded, and three further items were discarded because they were narrative revisions over time of the same study, making a total of 25 publications excluded. This left 25 articles for inclusion in the final review; 19 were individual studies; and 6 reviews (in addition to the original Cochrane review).
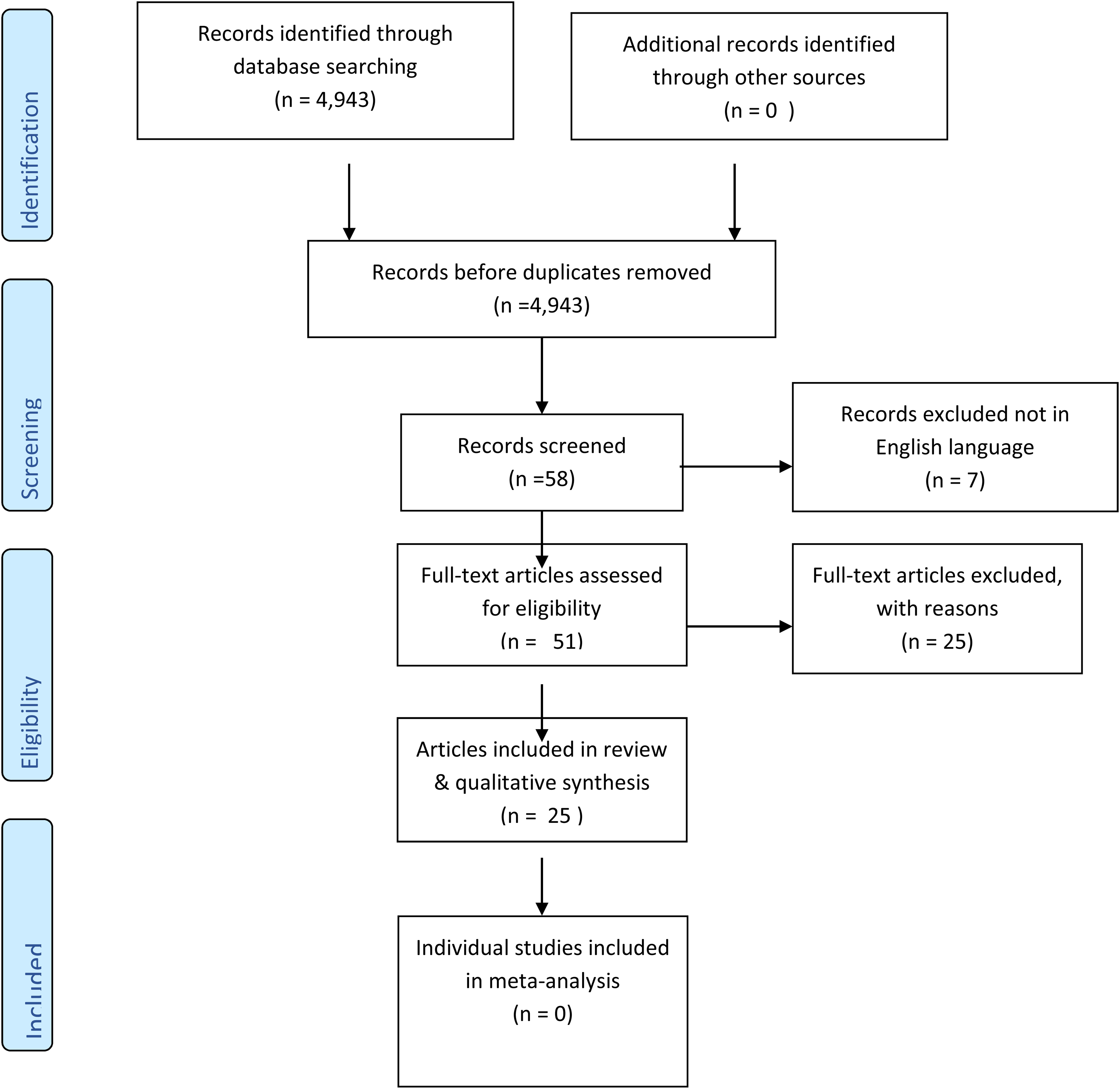
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram outlining the study design.
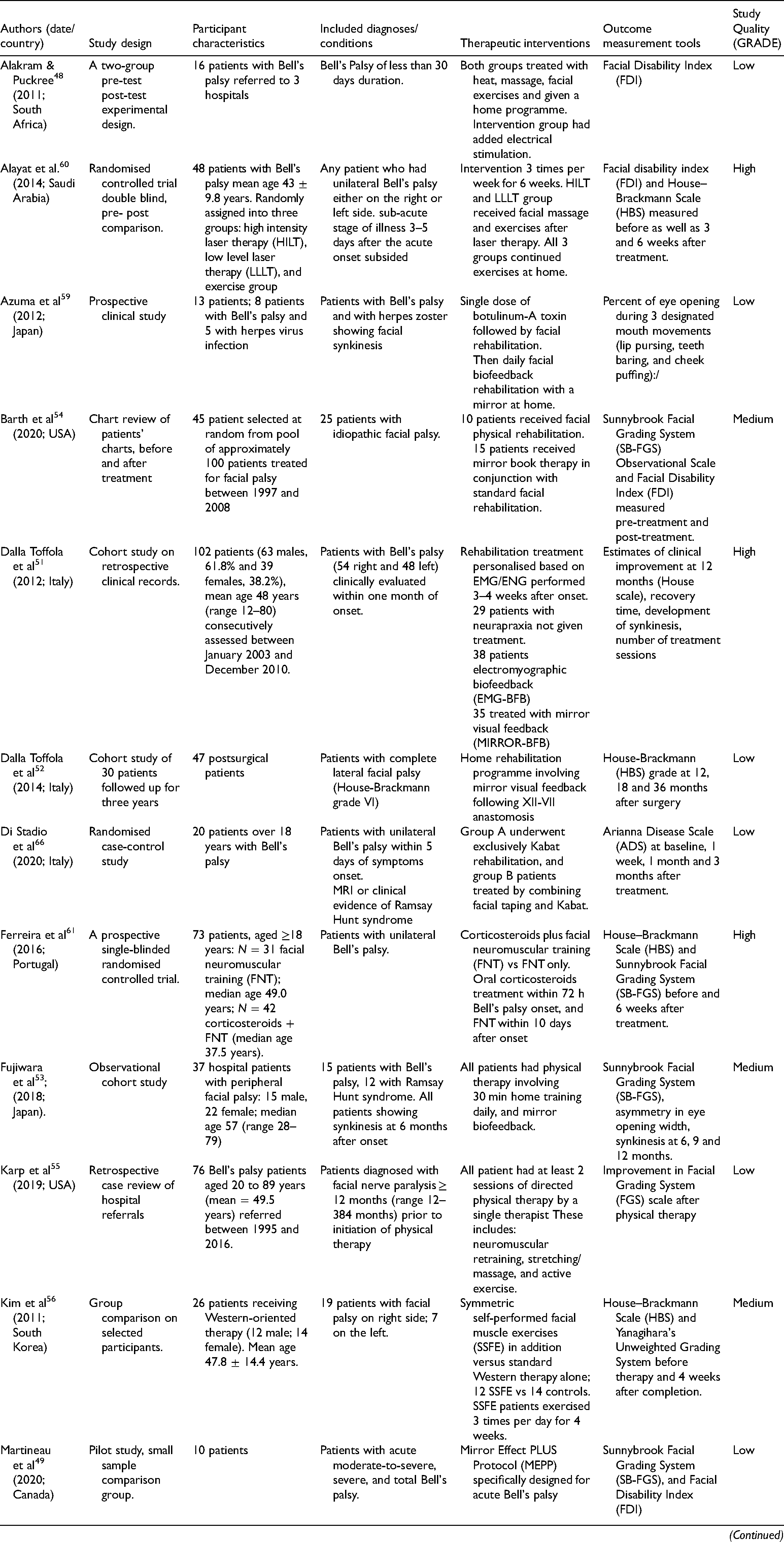
Table 2 (individual research studies) and Table 4 (reviews) present summaries of the characteristics of these 25 new studies identified for the review. Individual studies originated from 10 different countries, including Canada, Iran, Italy, Japan, Portugal, Saudi Arabia, South Africa, South Korea, Turkey, and the United States, emphasising the world-wide interest in physical therapy for facial palsy patients. The six new review articles originated from Australia, 42 Brazil, 43 Iran, 44 Italy, 45 New Zealand, 46 and Portugal. 47
Summary table: Characteristics of included individual research studies.
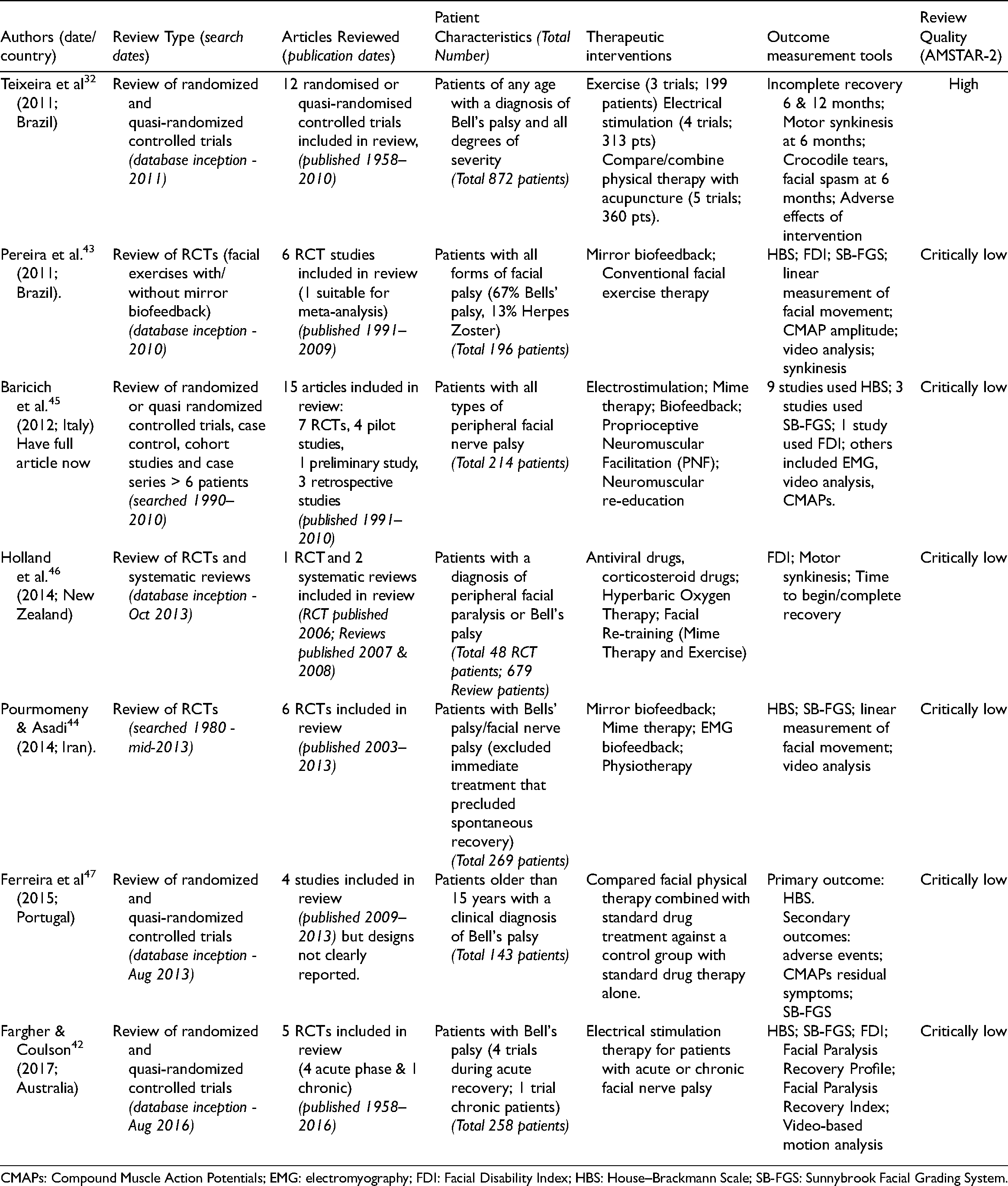
Summary table: Characteristics of included systematic reviews.
CMAPs: Compound Muscle Action Potentials; EMG: electromyography; FDI: Facial Disability Index; HBS: House–Brackmann Scale; SB-FGS: Sunnybrook Facial Grading System.
Characteristics of included studies: The 19 individual studies shown in Table 2 included, seven randomised controlled trials (total no. of subjects = 354); one quasi-experimental study (n = 16 patients) 48 ; two pilot studies (n = 37 patients)49,50;and nine non-experimental observational studies (n = 447 patients). Observational studies varied in their design: three were cohort studies (n = 169 patients)51–53; two were retrospective studies (n = 101 patients)54,55; three used group comparisons (n = 164 patients)56–58; and one a small clinical study of 13 patients. 59 In total, the research studies identified reported the impact of physical therapy in a total 854 participants (age range 12–80 years old).
Methodological quality and risk of bias: Consensus ratings of the methodological quality of studies (GRADE) are shown in the final column of Table 2. Five of the 19 individual studies were rated as high quality; four of these were randomised controlled trials60–63; and one was a cohort study. 51 A further six studies were judged to be of moderate quality. Two were randomised controlled trials,64,65 and four were non-experimental observational studies.53,54,56,58 The remaining nine studies were rated as low methodological quality. Two were randomised trials,57,66 one was a quasi-experimental study, 48 and two were small pilot studies.49,50 In terms of methodological flaws all, except one study, 60 were at risk of bias for failing to blind participants when outcomes were based on patient-reported measures. One high-quality study failed to achieve the required sample size, with a significant number of severe facial palsy patients in the control group dropping out in order to access physical therapy which was shown to be improving outcomes. 62
Patient characteristics (diagnoses/conditions): There was a high level of heterogeneity in the characteristics of patients included in the studies as shown in Table 2. Where specified, there was considerable variation in time post-onset of facial palsy at study entry. Six studies focused on patients in the acute phase, ranging from 48 h, 63 five days, 66 ten days, 62 to one month since onset.48,51 One study recruited patients in the ‘sub-acute phase’, that is, 3–5 days after the acute onset subsided. 60 A further two studies focused on chronic stages of recovery, that is, 2–30 years since onset.55,64 The remaining 11 studies did not pre-specify time post-onset at study entry. Individual studies also varied in the types of facial palsy patient recruited. All studies included Bell's palsy patients. Three studies also recruited some Ramsay Hunt syndrome patients.45,53,66 Where specified, all patients had unilateral facial palsy, although some studies did not state the type. Some studies recorded patients’ level of facial synkinesis at entry.53,57,59 Others focused on the severity of facial palsy; this ranged from Grade II to VII.50,52,58,62,64
Therapies Evaluated: Only two studies evaluated the use of facial muscle strengthening exercises on their own.50,55 A further five studies evaluated facial exercise therapy combined with biofeedback (via mirror or other device)49,51–54; and one evaluated exercise with added facial taping. 66 One paper compared Western facial exercise therapy with or without the addition of a Korean variant of facial muscle exercises. 56 The remaining studies reported the effects of combining facial exercise therapy with another form of treatment. Two studies explored the use of laser treatment before or in conjunction with facial exercises,60,65 and two research teams assessed the addition of electrical stimulation to physical therapy.48,63 Three papers examined physical therapy with and without corticosteroids58,61,62; and three studies considered Botox added to facial therapy.57,59,64
Outcome measures reported: Individual studies used three main validated measurement tools (see Table 2). Further details about these and patterns of combined use are presented in Appendix 7. The House–Brackmann Scale (HBS) was the most common method used to record improvements in functional recovery following therapy (n = 9 studies). A further six studies incorporated the Sunnybrook Facial Grading Scale (SB-FGS) to measure the severity of facial paralysis symptoms. A patient-rated outcome measure of the disability resulting from facial palsy, the Facial Disability Index (FDI), was used in six studies; one study reported separate results for the physical elements (FDIP) and social elements (FDIS) of the FDI. 54 The five remaining studies utilised a different single measure; two used an alternative validated facial grading system,55,67 and three used another unvalidated measure.50,59,66 All these five studies were assessed to be of low quality. Outcome measures used and their timing varied in the four high-quality randomised controlled trials,60–63 meaning comparable data were not available for meta-analysis to be undertaken. 68 The choice of outcome measure(s) was not indicative of the final quality (GRADE rating) of studies, although highly rated studies tended to use a combination of measures. For the randomised controlled trials, domains in which GRADE identified critical flaws are identified in Table 3.
Results reported in individual research studies.
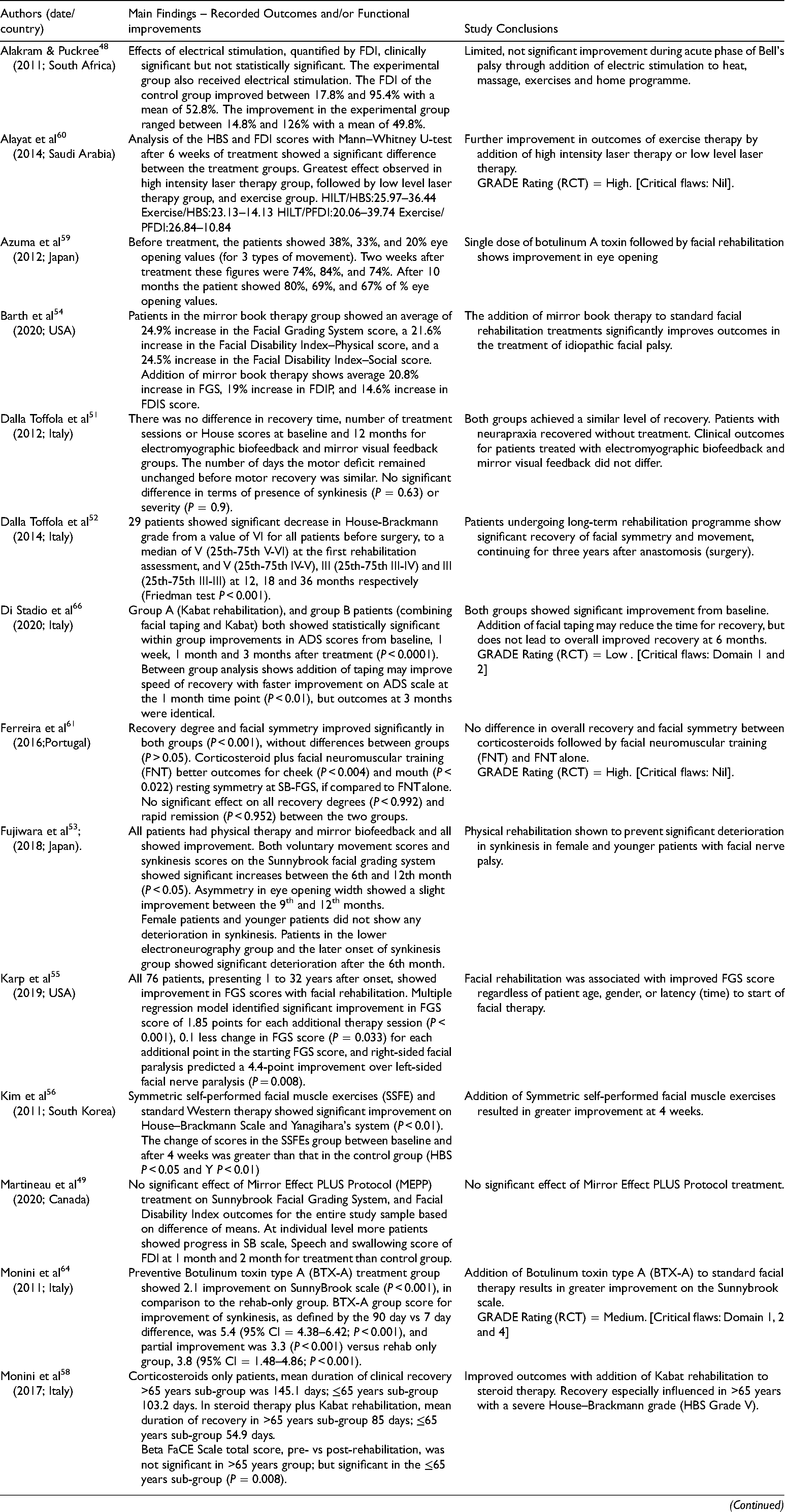
HBS: House–Brackmann Grading System; SB-FGS: SunnyBrook Grading Scale; FDI: Facial Disability Index; GRADE (RCT): 5 Critical Domains. [Domain 1: Risk of Bias; Domain 2: Inconsistency; Domain 3: Indirectness; Domain 4: Imprecision; Domain 5: Publication Bias (other considerations)].
Effectiveness of physical rehabilitation
Table 3 summarises the main findings and the conclusions drawn from the 19 new research studies identified. Of the 11 articles assessed to be of medium to high quality, all reported improvements following the use of physical rehabilitation for those with facial palsy.
Among the five high-quality articles, four were randomised controlled studies all of which reported a positive effect. Tuncay et al. 63 randomised patients with HBS scores of 2–4 into electrical stimulation with exercise or exercise-only treatment groups. They reported a statistically significant improvement in HBS scores at three months after onset in the combined treatment group but no difference in FDI scores between the groups. The exclusion of HBS grades 5 and 6 and the limited sensitivity of the HBS scale makes it difficult to draw any conclusions for these patients. Alayat et al. 60 found that high-intensity laser therapy, massage, and exercise three times a week for six weeks provided statistically significant improvements in HBS and FDI scores in those in the acute phase of unilateral Bell's Palsy when compared with low-intensity light therapy with massage and exercise or massage and exercise alone; the exercise-only group showed the lowest effect. Nicastri et al. 62 reported physical therapy produced a significant improvement in HBS grade, but time to recovery only improved in those with severe (HBS 5/6) facial palsy. Ferreira et al. 61 reported, with the exception of resting symmetry of the cheek and mouth on the SFGS, that neuromuscular retraining was as effective as acute provision of corticosteroids in improving static and dynamic symmetry in those with unilateral idiopathic facial palsy. The final, observational study, Dalla Toffola et al. 51 found no difference in the recovery in patients with idiopathic facial palsy and evidence of axonometric facial nerve injury when provided with EMG biofeedback compared to mirror biofeedback as a primary rehabilitation tool. Development of synkinesis, extent of motor recovery, and health resources used was included in their appraisal of recovery.
The six articles rated as medium quality included two randomised controlled trials and four non-experimental observational studies. All reported improvements Monini et al. 64 completed a small trial of 20 consecutive patients randomly allocated to pre-treatment with Botulinum toxin type-A prior to standard facial therapy. They found that both groups showed improved outcomes on the SunnyBrook scale, but pre-treated patients had significantly better outcomes. Ordahan and Karahan 65 randomized 46 patients with acute idiopathic palsy to physical exercise with or without low-level laser therapy. They reported that therapy alone showed a significant improvement in FDI score from baseline at week 6 but not at week 3. Laser therapy and exercise produced significant improvements from baseline FDI scores at both three weeks and six weeks post onset.
Among the four observational studies rated as medium quality, Barth et al. 54 reported a statistically significant increase in SFGS, FDIP and FDIS when mirror therapy was combined with standard facial rehabilitation. Standard rehabilitation was documented as including massage, stretching, neuromuscular re-education, myofascial release, and postural exercises. Monini et al. 58 found that treating all age groups with steroid therapy and physical rehabilitation resulted in a significantly quicker time to recovery than steroid therapy alone. They also highlighted the importance of physical therapy for older patients and those with more severe HBS grading at the onset of their palsy. This followed their previous trial showing standard facial therapy results were improved with the addition of preventive Botulinum toxin treatment. 64 Kim et al. 56 compared Western physical therapy with Korean symmetric self-performed facial muscle exercises, reporting that the addition of SSFE showed significant improvement in HBS at four weeks. 56 In a study by Fujiwara et al., 53 physical rehabilitation was shown to prevent significant deterioration in synkinesis in female and younger patients with Bell's palsy.
Eight of the 11 individual studies assessed to be of medium to high quality included the statistical significance of their results (P values). One reported a non-significant difference between two methods of biofeedback (electromyographic and mirror visual feedback), 51 while all others demonstrated a significant improvement.53,56,58,61–65 No studies attempted to calculate effect size, so there were insufficient data to assess imprecision or inconsistency as outlined in GRADE approach. 39
Among the remaining nine individual research studies that were assessed to be of low quality, three articles reported a statistically significant effect ranging from P < 0.05 to P < 0.001,52,55,57 Barth et al. 54 reported changes were ‘statistically significant’, one study (a small pilot trial) reported no significant effect, 49 and two studies simply reported percentage improvements.48,59 In the one poor quality randomised controlled trial, Di Stadio et al. 66 reported a significant improvement for Kabat rehabilitation with and without facial taping based on a new rating Arianna Disease Scale. 69
Timescale and sustainability of therapeutic effects
The timescales over which physical therapy was assessed differed widely and this limits any robust analysis of how sustainable the reported therapeutic effects were. Dalla Toffola et al. 52 compared the efficacy of EMG and mirror biofeedback over a 12-month period. Ferreira et al. 61 assessed the role of corticosteroids (prednisolone) and neuromuscular retraining in recovery from acute idiopathic palsy and so chose to perform their analyses at the entry to the study and six weeks later. Kim et al. 56 reviewed acute outcomes at four weeks post onset. Fujiwara et al. 53 appraising physical therapy in the treatment of synkinesis selected 6, 9 and 12-month intervals to assess the outcomes. Nicastri et al. 62 followed study participants up on a monthly basis for six months.
Evidence from systematic reviews
Table 4 presents an overview of the six reviews shortlisted for examination in publication date order, with data from the original Cochrane review included for comparison. 32 The six new reviews were published over the period 2011–2017 and originated from research groups in Australia, 42 Brazil, 43 Iran, 44 Italy, 45 New Zealand, 46 and Portugal. 47 Apart from the 2011 Cochrane review by Teixeira et al., all systematic reviews were rated as ‘critically low’ using the AMSTAR-2 rating. 40
Table 5 summarises the main findings and conclusions drawn by the authors, and the weaknesses identified in these reviews. The one high-quality review remains that was undertaken by Teixeira et al. 32 This found low-quality evidence that tailored facial exercise could reduce sequelae in the acute phase, could improve facial function in those with moderate paralysis, and could produce improvements in the chronic stages. The authors concluded that further research evidence was required, as provided by individual studies listed in Tables 2 and 3, none of which are included in the Teixeira review.
Findings reported by included reviews.
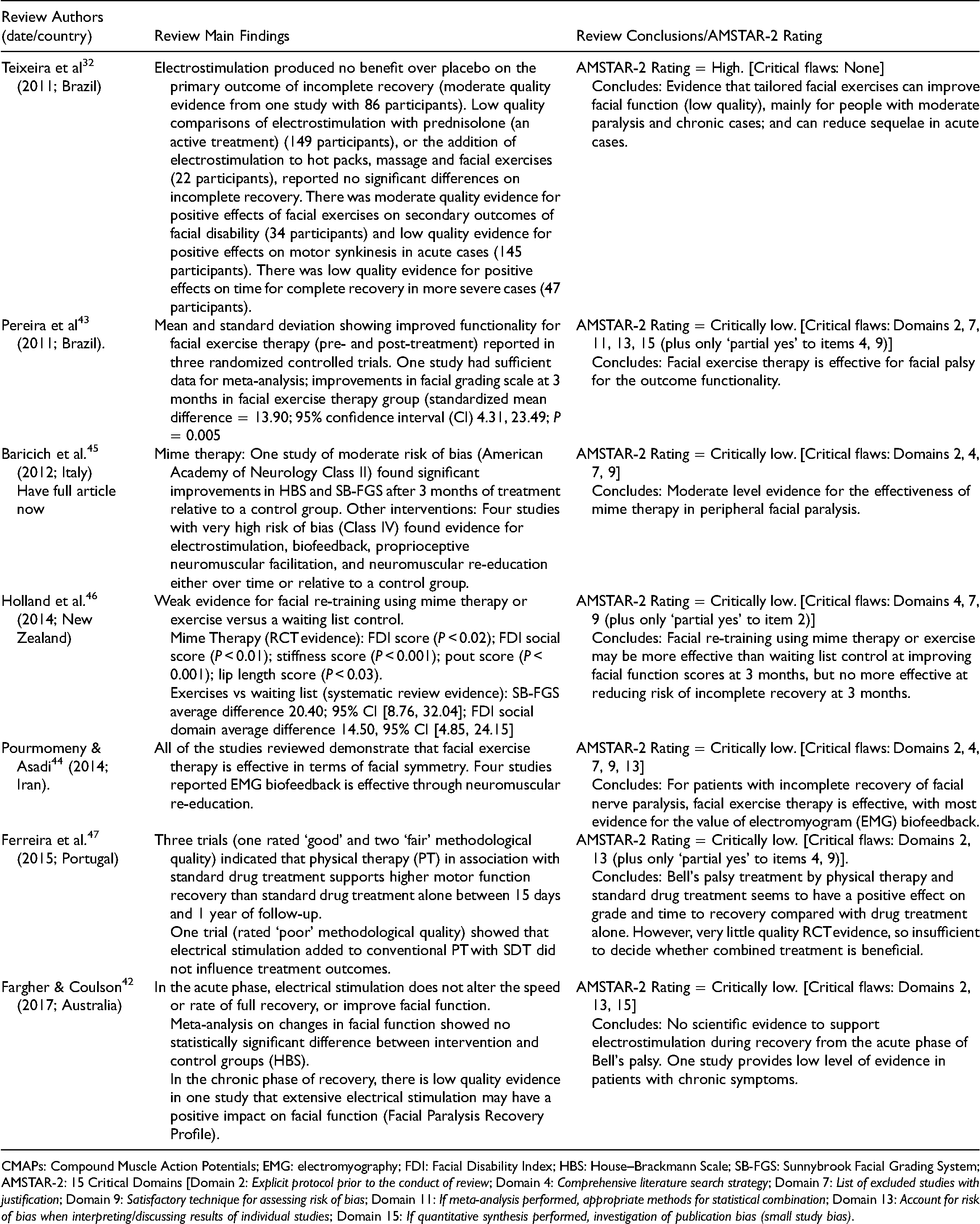
CMAPs: Compound Muscle Action Potentials; EMG: electromyography; FDI: Facial Disability Index; HBS: House–Brackmann Scale; SB-FGS: Sunnybrook Facial Grading System; AMSTAR-2: 15 Critical Domains [Domain 2: Explicit protocol prior to the conduct of review; Domain 4: Comprehensive literature search strategy; Domain 7: List of excluded studies with justification; Domain 9: Satisfactory technique for assessing risk of bias; Domain 11: If meta-analysis performed, appropriate methods for statistical combination; Domain 13: Account for risk of bias when interpreting/discussing results of individual studies; Domain 15: If quantitative synthesis performed, investigation of publication bias (small study bias).
The six more recent reviews all reach largely positive conclusions about the effectiveness of facial exercise therapy.42–47 But all have major methodological shortcomings resulting in critically low AMSTAR-2 quality ratings, so could not be included in our synthesis. Critical weaknesses include lack of clarity a priori about the review protocol; deviations from the original protocol; a lack of comprehensive description of search strategies, excluded studies, or risk of bias assessments; and no consideration of how bias might influence the interpretation of results. Equally important, the reviews did not include additional new evidence; only half identified any studies published since the 2011 Teixeira review. Pourmomeny and Asadi 44 identified two new randomised controlled trials; Ferreira et al. 47 included one new study; and the 2017 review by Fargher and Coulson 42 identified two randomised controlled trials. Only three of these five studies met our inclusion criteria and they had already been included in our review51,62,63; the other two did not focus on facial exercise therapy.70,71
Discussion
The primary aim of this study was to update the evidence base on the effectiveness of physical therapy for facial palsy rehabilitation, 32 focusing on tailored facial exercise therapy. The review identified nineteen new research studies, including eight randomised controlled trials, four quasi-experimental or pilot studies, and seven observational studies. These studies provide evidence on the effectiveness of facial exercise therapy in 839 patients with ages ranging from 12 to 80 years old. Although, six reviews published after the Cochrane review were also identified all were rated as being of critically low quality. They also identified only three new studies which met our inclusion criteria, and all these were already included in our review. This article therefore adds significantly to previously available evidence on the effectiveness of facial exercise therapy for the recovery of people diagnosed with facial palsy.
The 19 new studies included in this review vary in their research design. Seven incorporated a randomised controlled trial, nine used a non-experimental observational design, and the remainder were quasi-experimental or pilot studies. Overall, four out of seven trials were rated as high quality and all described a positive impact. Among the nine observational studies, three were rated as high or moderate quality, all cohort studies. Two of these studies reported a significantly better outcome for those receiving facial exercise therapy, especially among younger patients.53,58
The effectiveness of facial exercise therapy on its own was evaluated in only two studies; both reported that patients performing facial exercises achieved greater functional recovery than those who did not.50,55 Six studies assessed physical therapy combined with biofeedback, either via a mirror or other means; all reported positive improvements.49,51–54,66
The remaining 10 studies evaluated the effectiveness of combining facial exercise therapy with corticosteroids,58,61,62 botulinum toxin,57,59,64 electrical stimulation,48,63 or laser treatment.60,65 Nine reported a positive improvement.
This review considerably strengthens the evidence base in support of facial exercise therapy, but information on the specific benefits of therapy at different timepoints post-onset of facial palsy or for patients living with different levels of severity is difficult to disentangle with certainty. In studies where the stage of recovery was specified, six studies concentrated on the acute phase, recruiting patients from 48 h to one month since onset of facial paralysis.48,51,60,62,63,66 A further 12 studies focused on chronic cases including patients from 2 to 30 years post onset.55,64 These studies strengthen previous Cochrane review evidence on the value of physical therapy early in recovery, and also add to the previously limited evidence in support of its use for chronic cases. 32 Evidence of the specific benefits with increased clinical severity is less clear. Five research studies selected patients based on the severity of their facial palsy, with cut-offs ranging from Grade II to VII,50,52,58,62,64 and a further three reported selecting patients based on the presence of facial synkinesis.53,57,59 However, it is not possible to draw any conclusions on the impact of physical therapy depending on the clinical severity of facial palsy from these studies.
The review findings also demonstrate an increase in the use of validated outcome measures, compared to research identified in the earlier Cochrane review. 32 A clinician facial grading system (House–Brackmann or Sunnybrook) was used in 12 studies, and a patient-rated outcome measure (Facial Disability Index) was included in six studies. The use of both a clinician and patient outcome measure was observed in the highly rated studies. A recent systematic review has recommended the adoption of Sunnybrook for reporting outcomes of facial nerve disorders. 72 Only three studies included in the review used a single, non-validated outcome measure; all were rated low quality. No study defined ex ante what would represent a clinically significant change. A similar finding has been reported in the service setting when monitoring patient recovery. 20 No study included cost-effectiveness as an outcome or incorporated a health-utility outcome measure (e.g. EQ-5D) that would enable economic modelling. 73 Finally, because the point at which outcomes were measured ranged from 4 weeks to 12 months post-treatment, evidence on the sustainability of any improvements following therapy is difficult to gauge. Arguably, a comprehensive analysis of the impact of therapy on the evolution of facial palsy, including synkinesis, should be performed over a minimum of a 24-month period. 74
Conclusions and future influence on clinical practice
This review provides new evidence from high-quality studies to support the use of facial exercise therapy in patients with facial palsy. Limitations of the evidence include differences in research design, the interventions evaluated, and patients included in studies. This heterogeneity makes it impossible to pool data from individual studies to increase the power and precision of estimates of treatment effects. 68 The heterogeneous nature of the current evidence base also limits the ability to draw any clear correlation between the effectiveness of facial exercise therapy and time since onset of facial palsy, clinical severity, or other patient demographics. The use of both a clinician grading system and patient-rated outcome measure, as identified in high-quality studies, is recommended.
Looking to the future, further improvements to the evidence-base will become even more important if reports emerging of a link to COVID-19 are substantiated. These include a tripling of cases in patients who have had COVID-19, 75 as well as possible links to vaccines,76,77 with safety concerns already officially recorded for the latter, 78 and a recent call for surveillance following use of particular vaccines. 79 Large-scale COVID-19 vaccine programmes could lead to a rise internationally in the future number of facial palsy cases. Our review demonstrates widespread international interest in evaluation of physical therapy for facial palsy, with studies originating from 10 different countries. This provides a good foundation for future collaborative research, moving away from a previous pattern of studies almost exclusively undertaken in the United States. 31 International collaborations are already leading to standardisation of outcome measures, and development of value-based reimbursement strategies. 80 A future move to digitally enabled facial palsy rehabilitation at home is also likely to be catalysed.20,34 Pre-pandemic, a review of telerehabilitation could identify no facial palsy studies. 81 This situation is likely to change as a consequence of an accelerated worldwide move to digitally enable services due to COVID-19, 82 new routes for commissioning home-based digital services,83,84 and the development of new wearable technologies. 33
This review has concentrated on peripheral facial nerve paralysis. A similar evidence base for facial palsy following stroke is currently lacking. 85 Because this form of central facial palsy is clinically distinct, 86 current review findings are not directly transferrable. But, the lessons learned here might be applied to improve the evidence base for these patients.
Clinical messages
RCTs of facial exercise therapy confirm improved facial functioning and patient-reported outcomes.
Therapy is effective in early cases, when combined with other treatments, and potentially in chronic cases.
Multi-centre collaboration is needed, particularly given emerging evidence of links with COVID vaccination.
Specialist facial therapy should be integrated fully into treatment pathways.
Footnotes
Authors’ note
Data and other materials are available from the corresponding author.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the National Institute for Health Research (NIHR) as part of FRAME project (Reference Number II-LA-0814-20008).