
Abstract
Introduction
Laser speckle imaging is used for noninvasive assessment of blood flow of cutaneous wounds. The aim of this study was to assess if laser speckle imaging can be used as a predictor of venous ulcer healing.
Methods
After generating the flux speckle images, three regions of interest (ROI) were identified to measure the flow. Sensitivity, specificity, negative predictive value, and positive predictive value for ulcer healing were calculated.
Results
In total, 17 limbs were included. A sensitivity of 92.3%, specificity of 75.0%, PPV of 80.0%, and NPV 75.0% were found in predicting wound healing based on laser speckle images. Mean flux values were lowest in the center (ROI I) and showed an increase at the wound edge (ROI II, p = 0.03).
Conclusion
Laser speckle imaging shows acceptable sensitivity and specificity rates in predicting venous ulcer healing. The wound edge proved to be the best probability for the prediction of wound healing.
Introduction
Venous ulcers are currently a considerable health care problem. It will be an even more challenging problem in the near future due to the aging population and the increasing incidence of obesity in Western society. The incidence of venous ulceration in the general population is 1–2% and even higher in the elderly patient (>65 years).1–4 These ulcers have great impact on quality of life, especially due to social isolation and induced pain.1,5
Normal stages of wound healing include hemostasis, inflammation, tissue proliferation, and tissue remodeling. All stages are characterized by specific pathways in which vascularization plays an important role. In contrast to the normal wound healing, venous ulceration is referred to as abnormal wound healing with typical venous skin changes like hyperpigmentation or redness. These skin changes develop due to chronic venous insufficiency or obstruction with poor venous drainage resulting in venous hypertension. As a consequence, the pressure in the post capillary vessels increases and gives rise to skin capillary damage, fluid exudation, and poor tissue nutrition favoring inflammation. These venous ulcers have been shown to be hard to heal. The long duration until wound closure and many recurrences make it a complex and unpredictable problem. 6
There are many factors, which affect the ulcer characteristics and ulcer healing time. Due to this variability of factors, it is difficult to predict the individual healing time. Currently, we are still searching for a simple, clinical, and diagnostic tool that can give more insight in this complex phenomenon.
Laser speckle imaging (LSI) analysis is a technique used for noninvasive assessment of tissue blood flow and therefore also applicable for cutaneous wounds. LSI maps the relative velocity of moving cells in the microcirculation and discriminates between slow and fast movement. Using near-infrared laser speckle contrast this analysis can be performed.7–10 Previous research has shown that LSI is a sensitive, reproducible, and reliable technique for detecting decreased blood perfusion. 11
The aim of this study was to analyze if LSI can be used as tool to predict the healing of venous ulcers. Likewise, whether LSI can help to select those patients that need more intensive treatment and follow up.
Material and methods
We analyzed prospectively gathered patient data from our tertiary referral care academic center. All consecutive patients who presented at the venous ulcer outpatient clinic between June 2013 and May 2016 were assessed. This study was approved by the medical ethical committee of Maastricht University (reference number METC 15-4-267).
Baseline characteristics were scored for all patients and included: age, gender, body mass index (BMI), medication use, venous history, and general medical history. Arterial insufficiency was excluded by measurement of the ankle-brachial index (ABI) combined with toe pressures whenever ABI was unreliable. All patients were examined for superficial and deep venous post thrombotic obstructive changes as well as venous insufficiency as a potential cause for the nonhealing tendency of the venous ulcer. These conditions were analyzed by duplex ultrasound and magnetic resonance venography to identify whether an additional intervention such as deep venous reconstruction, percutaneous transluminal angioplasty, or stenting were deemed necessary.
Of all the performed speckle images, those with accidental disturbance due to background factors (i.e. white fiber mats or ointment around the wounds) were excluded. Other exclusion criteria were: presence of mixed arterial and venous ulceration, and missing follow up data regarding wound closure.
Speckle imaging
The Moor FLPI-2 (Moor instruments, Devon, UK), was used to perform LSI measurements. This is a commercially available system calibrated according to the manufacturer’s recommendations. This system can illuminate tissue up to a maximum of 1 mm in depth. The near-infrared laser beam (785 nm) illuminates tissue which gives a 16-color coded tissue perfusion image. This image is created based on the interaction between photons and moving red cells, which are therefore Doppler-shifted. Some of these shifted or nonshifted photons are diffusely scattered and lead to a dynamic speckle pattern. This pattern can be shown using a CCD camera (150x116 pixels at 25FPS) in which high perfusion gives rapid variation, and thereby, a low area of contrast. Low perfusion accounts for low variation in speckle pattern, and thus, a high contrast of speckles. This contrast is quantified and results in 16-color-coded perfusion images varying from blue (indicating low perfusion) to red (indicating high perfusion).
Experimental conditions and measurements
All speckle measurements were performed by one investigator. Factors, which could account for disturbances, were canceled out to gain good quality images. 8 All included patients were analyzed in a dedicated room with a constant room temperature (23.5 ± 0.5℃), with locked door and all lights off. A black fiber mat was placed under the patients’ legs to avoid influence of background reflection.
To reduce vibration or movement of the LSI devices’ measurement arm, the arm was fixed and the patient was asked to sit on the examination table with their legs in the horizontal position. It was explained to the patient that vibration or talking could influence the results and thus requested to sit still and remain quiet during the examination. The laser head of the LSI device was positioned, as perpendicular as possible, at the center of the venous ulcer. The red dots of the aiming lasers were centered as one point with a distance of 10–30 cm.
To measure the microcirculation during dynamic responses, we performed a venous stasis test in all patients. This test simulated venous hypertension (VHT) and was performed by placing a rapid deflatable pressure cuff around the upper leg. A baseline flux was measured for 1 min as a reference. The cuff was then inflated to 80 mmHg and maintained inflated for 2 min. Subsequently, the cuff was deflated and the VHT measurement was continued for 2 more minutes.
After generating the flux speckle images, three regions of interest (ROI) were selected, since flow rates were significantly diverse in those three areas of the wound. The first ROI was placed in the center of the wound, the second at the best definable edge of the wound and the third in the tissue around the wound specifically away from any skin changes (Figure 1). The ROIs were placed and flux values were measured with the moorFLPI analysis software package. The smallest wound was analyzed first, to ascertain reproducibility by defining the size of the ROIs.
(a) Flux image, red flux indicating highest flow, blue flux indicating lowest flow. ROI I in the center of the wound, ROI II at the wound edge, ROI III at the surrounding. (b) Black and white image of venous ulcer indicating where ROIs were placed. (c) Color image of venous ulcer indicating where ROIs were placed. (d) The lines represent the microcirculation of different ROIs in time. Flux 1 corresponds to ROI I, flux 2 corresponds to ROI II, flux 3 corresponds to ROI III.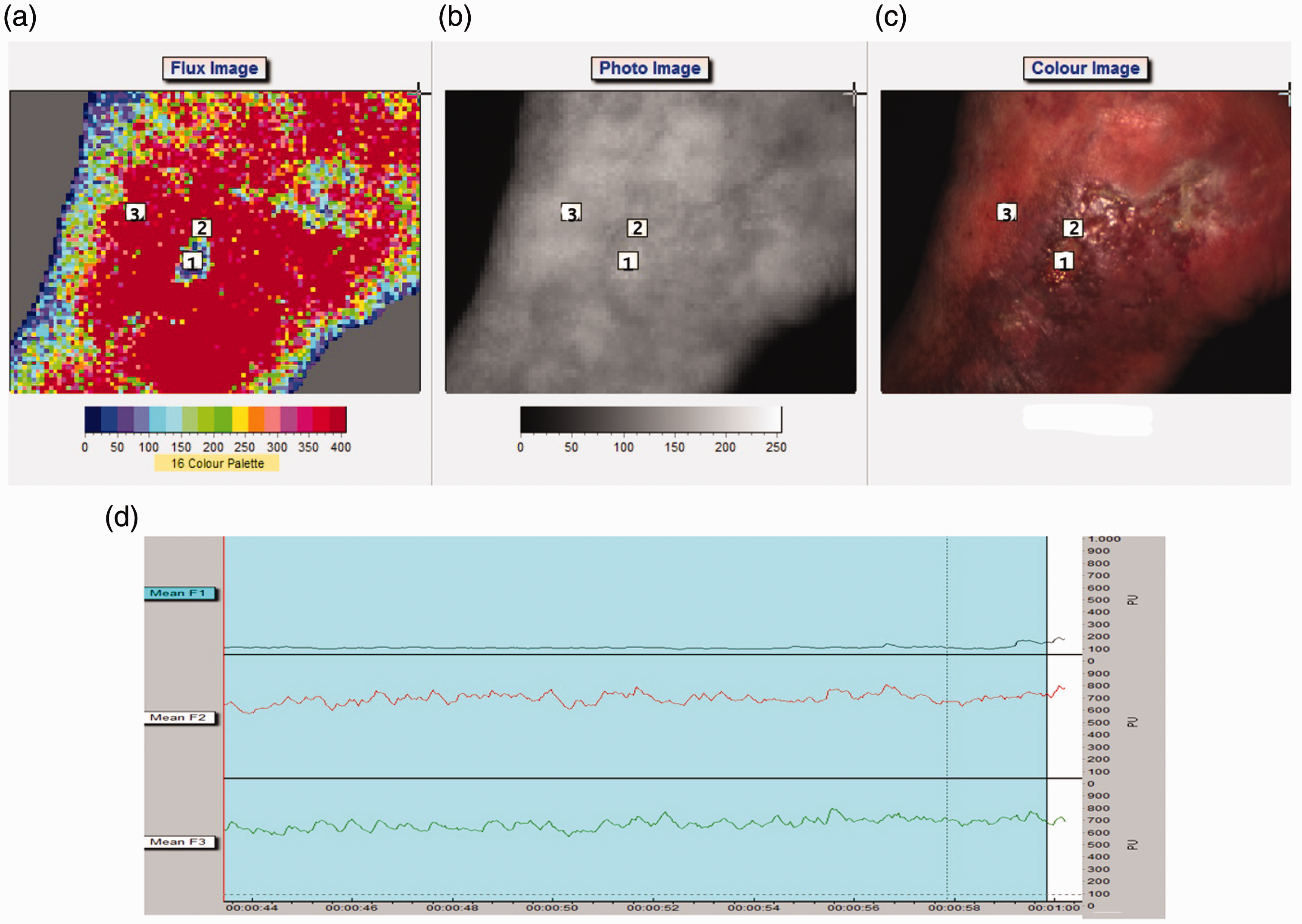
Mean flux was calculated, and the flow pattern was shown in a speckle image. A cut-off point at the mean of all flux values was used to subdivide ROIs into low and high flow. All of the ROI measurements were performed for the baseline flux and for the VHT flux.
Two independent researchers performed the assessment of the speckle images and films: one vascular surgeon and one vascular researcher. They were blinded for the healing or non-healing tendency of analyzed wounds. Based on the flux colors gathered in the movie they made a prediction on whether the wound would close or whether the wound would be hard to heal. Hard-to-heal wounds were defined as no healing tendency within 6 months of the first visit at the outpatient clinic.
After this analysis, the observed state of the wounds was compared with the predicted outcome. Based on the outcomes, sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) were calculated.
Analysis and statistics
All continuous data are presented as average with their standard deviation, except non-normally distributed data (these are presented as median with their inter quartile range). Categorical data are presented as frequencies and percentages. Comparisons of ROIs between wounds with and wounds without healing tendency were performed using a Student’s T-test. A α of ≤0.05 was considered to be statistically significant. Data were analyzed using IMB SPSS statistics v23.0 (IBM Corporation, Armonk, NY, USA).
Sensitivity and specificity, negative predictive value (NPV) and positive predictive value (PPV) of healing tendency based on flux images were calculated.
Results
Demographics
We analyzed 84 limbs in 78 patients at our outpatient venous ulcer clinic. Twenty-six of these limbs presented with totally or nearly healed wounds. Nearly healed wounds were defined as wounds having a surface area less than 1 mm. Twenty-two limbs of the total population could not be speckled due to the fact that the patient was unable to sit still or due to the circumferential shape of the ulcer. In eight limbs, the background conditions were not optimized, since in some cases a white background was used or wounds were not sufficiently cleaned from ointment. Since these conditions give background disturbance these patients were excluded for further analysis. Nine patients had mixed venous and arterial ulcers. Two patients did not wish to participate in this study and could not be included as there were no data regarding wound healing.
Patient demographics.
statistical significance.
Apart from the overrepresentation of diabetes in the hard-to-heal group (p = 0.002), there were no statistically significant differences in the baseline characteristics.
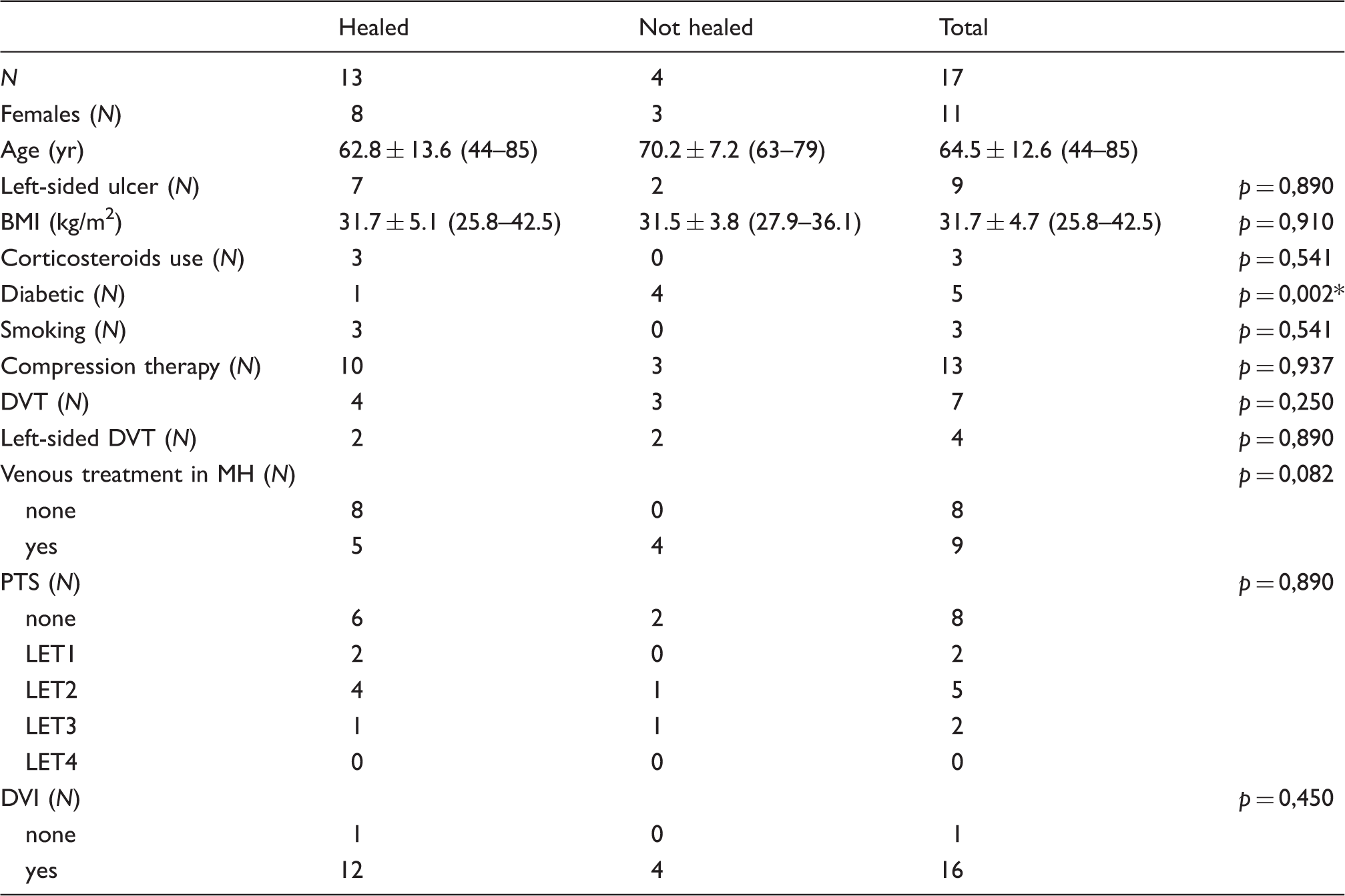
Overall, 13 wounds healed within a mean period of 184 days and 4 wounds did not show a healing tendency. Figures 2 and 3 show differences in the flow characteristics of a healed and a hard-to-heal wounds.
(a) Flux image of venous ulcer with healing tendency, red flux indicating highest flow, blue flux indicating lowest flow. ROI I in the center of the wound, ROI II at the wound edge, ROI III at the surrounding. (b) Black and white image of venous ulcer with healing tendency indicating where ROIs were placed. (c) Color image of venous ulcer with healing tendency indicating where ROIs were placed. (a) Flux image of venous ulcer without healing tendency, red flux indicating highest flow, blue flux indicating lowest flow. ROI I in the center of the wound, ROI II at the wound edge, ROI III at the surrounding. (b) Black and white image of venous ulcer without healing tendency indicating where ROIs were placed. (c) Color image of venous ulcer without healing tendency indicating where ROIs were placed.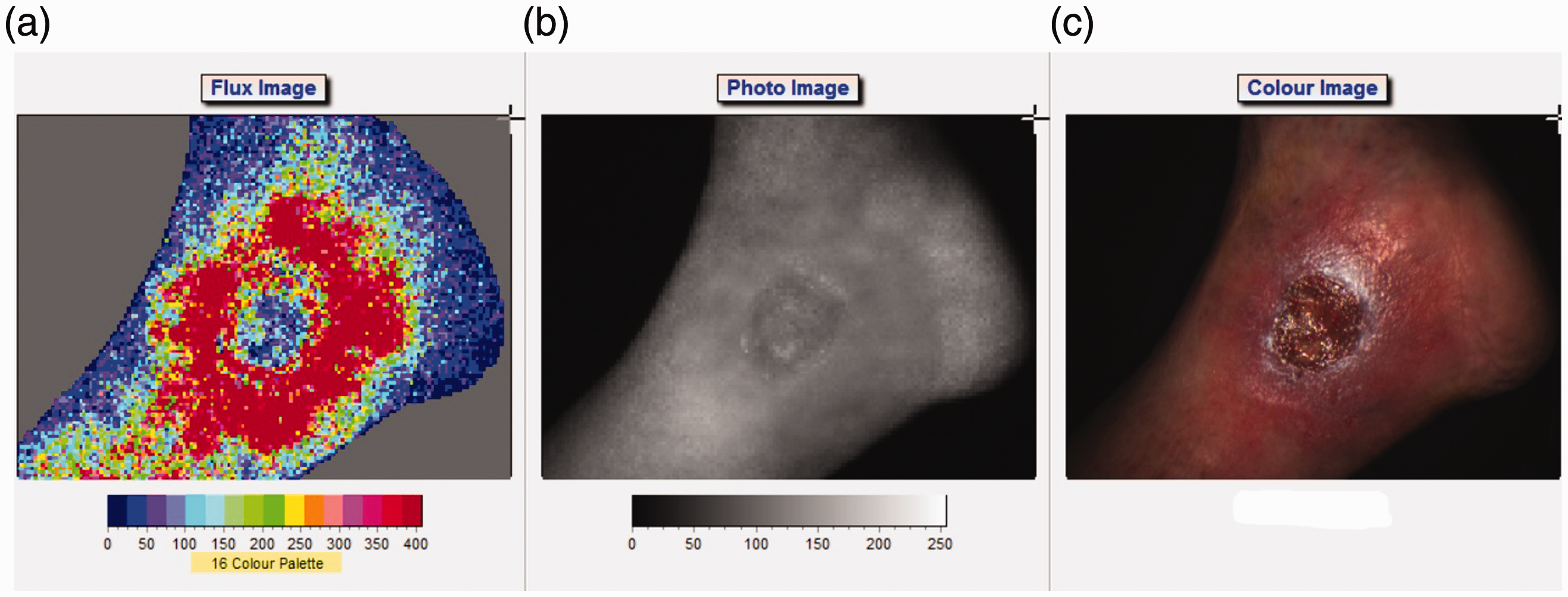
There were nine patients with post thrombotic changes shown on duplex imaging or MRV. In two of them, the post thrombotic changes were visible in the deep venous system i.e. iliac or common femoral tract. Both of these patients had hard-to-heal wounds. All of the patients with hard-to-heal wounds had a medical history of superficial venous treatment. Based on the clinical and radiological assessments, two of them needed additional superficial treatment to optimize the blood flow.
Analysis of observed and predicted wound healing based on flux colors in speckle imaging, yielded a sensitivity of 92.3%, specificity of 75.0%, PPV of 80.0%, and NPV 75.0%.
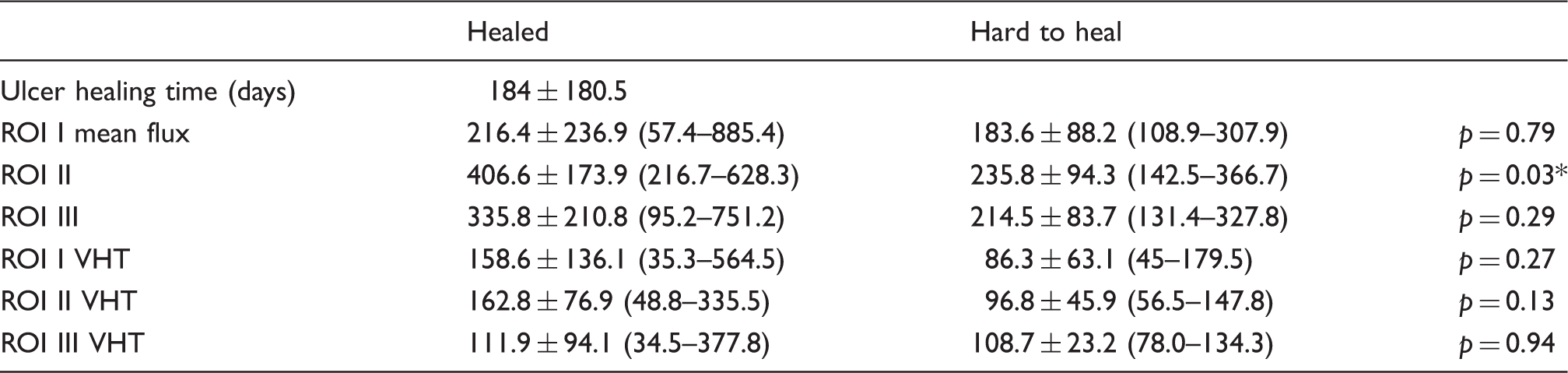
Mean flux values in all analyzed wounds were lowest in the center (ROI I; 216.4 (57.4–885.4) healed versus 183.6 (108.9–307.9) hard to heal) and showed an increase towards the wound edges (ROI II; 406.6 (216.7–628.3) healed versus 235.8 (142.5–366.7) hard to heal). The tissue around the wound (ROI III) showed a decrease in flux compared to ROI II (335.8 (95.2–751.2) versus 214.5 (131.4–327.8)). Baseline measurement of ROI II showed a statistically significant difference between healed and hard-to-heal wounds (p = 0.03). This indicates that the wound edge flux may be of greatest value in the prognosis of wound healing.
ROI measurements.
statistical significance.
Discussion
This study shows that LSI may be a useful tool to predict wound healing in venous ulcers with a high sensitivity of 92.3%, a good specificity of 75% and an acceptable positive predictive value (80%). The higher sensitivity percentages are at the expense of specificity percentages resulting in referral of patients who might not need additional wound care. In contrast, higher specificity levels would result in lower health care cost since this would provide less over-referral. In this setting, adequate sensitivity is of greater importance than high specificity, as overestimation of wounds that are hard to heal is to be preferred over underestimation.
To our knowledge, this is the first study that assessed the diagnostic properties of LSI for ulcer healing in venous ulceration. Although the researchers, who performed the assessments, were not familiar with LSI, acceptable prediction results after flux measurements were shown. Furthermore, if compared to previously used techniques such as laser Doppler, LSI has the advantage that it is possible to analyze the complete wound surface12,13 and therefore to retrieve flow information about every wound region of interest. This is a great advantage in guiding wound care and could help physicians to concentrate on specific parts of the wound.
The importance of hemodynamic changes during wound healing was simulated using the VHT model. Huisman et al. 10 could not find any significant changes in blood flow measurements when inducing venous hypertension (applying a pressure of 60 mmHg). These negative findings could be explained by the fact that 80 mmHg is the cut off value at which the venous flow is blocked.14,15 Subsequently, we decided to simulate our VHT model with the application of a pressure of 80 mmHg. The fact that VHT showed statistically significant changes (p < 0.01) in all three ROIs, strongly suggests that venous hypertension decreases the flow rate in venous ulcers. This finding can be extrapolated to demonstrate that patients with higher venous pressure have worse outcomes. As a related finding, all patients with hard-to-heal ulcers in this study had a medical history of superficial venous treatment and needed additional superficial and/or deep venous treatment.
This research was performed in a specialized ulcer care clinic with all facilities to treat and analyze venous ulcers. Speckle analysis as such can, however, also be performed in a regular outpatient clinic room as long as the door can be closed and the lights can be dimmed. Correctly executed speckle analysis in primary care might result in timelier referral to centralized wound care with broad knowledge in the treatment of venous wounds.
Although we showed some favorable outcomes, some limitations of the current study should be mentioned.
Laser speckle imaging is strongly affected by experimental confounding conditions. 8 In order to have reliable results one should eliminate confounding factors as much as possible. Previous research discussed artifacts in measurements due to the environmental factors. 10 We eliminated all possible disturbing conditions to get valid results. As long as these conditions are met, the flux values can be interpreted reliably to make fair predictions.
Besides, there are some patient-related factors, which contribute to disturbance. It is difficult to perform a speckle analysis in patients who are unable to sit on an examination table as movement will disturb the speckle pattern. Furthermore, in patients with a circumferential venous ulcer it is not possible to visualize the center of the wound in one image. Although the speckle technique can be used in these patients, multiple images need to be combined to make a prediction on the healing tendency of these circular venous ulcers. In our study, patient factors like these resulted in exclusion of 22 patients and we could therefore only yield data for a small proportion of patients.
The laser speckle image technique has previously been shown to be reliable in displaying flux up to 1 mm depth. 7 Since all wounds showed some signs of alteration in the wound healing process, there was a varying thickness all around the wound surface. We did not anticipate on measuring wound thickness and therefore variations in wound edge thickness may have confounded our results. This shortcoming can be overcome in future trials by selecting ROIs during the actual measurements. In this setting, wound edges can be measured and ROIs can be placed more accurately to represent the most reliable area.
Even so, wounds may contain crusts, severe exudates and fibrotic tissue thicker than 1 mm, which may influence the flow values. In order to solve this problem, the wound needs to be cleaned as much as possible before the speckle analysis. In this way, LSI can be performed in a cleaned and artifact-free area to get the most reliable results. LSI might in this case become a tool to guide a wound care specialist how to conduct wound care in the best way.
In some of the analyzed wounds, it was difficult to select a correct region of interest. The difficult wound shape with small wound surfaces mainly caused this. This is, however, a characteristic that could not have been prevented as it shows the normal nature of the wound.
Most importantly, due to the strict inclusion criteria resulting into a small sample size, no definite conclusion can be drawn yet. Conclusively, the results in this article could be interpreted as a first pilot study. We did, however, see a clear trend towards higher flow rates in patients with healed wounds compared to hard-to-heal wounds. Furthermore, a preferred area for predicting wound healing, which was shown to be at the wound edge (ROI II, p = 0.03) could be identified.
After these promising results, we will try to improve feasibility in all patients like the ones with large ulcers and healed ulcers, the latter to predict recurrence. A prospective trial has been started to overcome all abovementioned limitations. A larger group of patients will be included to ensure enough power. Follow-up speckle images will be used before and after a treatment to show the effect of decreasing the venous hypertension. Whenever significant changes can be proved, the LSI can be used to evaluate wound treatment, and it might also give an indication as to which part of the local wound needs more attention to improve healing.
Conclusion
Laser speckle imaging is, under standardized conditions, a clinically useful technique for the assessment of flow in venous ulceration, and shows acceptable sensitivity and specificity rates in predicting venous ulcer healing. The wound edge (ROI II) proved to be the best location to predict healing.
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Cees Wittens – Consultancy agreement with Angiocare; Consultancy agreement with BoMedical; Consultancy agreement with Med; Consultancy agreement with Optimed Gmb; Consultancy agreement with Vascular Insights; Research funds BTG; Research funds EKOS; Research funds Sapheon.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author contributions
TV and SD: Study design, data analysis, writing; CZ and RK: start study design, ethical approval, data collection, critical review in writing; IZ: critical review in data analysis and writing; AT and CW: study design, data collection, critical review data analysis in writing. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Ethical approval
This study was approved by the medical ethical committee of Maastricht University (reference number METC 15-4-267).