
Abstract
Objective
Determine standards of referral and management of patients with venous leg ulceration in primary care after the release of the EVRA (A Randomized Trial of Early Endovenous Ablation in Venous Ulceration) study results.
Methods
An online questionnaire was disseminated over four months to professionals working within primary care.
Results
The survey received 643 responses. Of respondents, 90 (14%) had heard of the EVRA trial and 51 (8%) were familiar with the results. Of those who answered the following questions, 410 (69.1%) stated that referral to a vascular specialist must be made by the General Practitioner and 13 (2.2%) reported that they would always refer patients for secondary care assessment before the publication of EVRA. Considering the EVRA results, 128 (29%) reported that they would change practice regarding referral and would experience no barriers and 198 (45%) reported that they would like to refer earlier but is not their decision. Barriers to changing practice included local referral policies, training and time restrictions, 266 (59%) had heard of the NICE guideline (CG168) and 194 (43%) were aware of the recommendations for referral to a vascular service within two weeks for patients with an open or healed ulcer.
Conclusion
There is a considerable variation in local referral pathways for venous leg ulceration, and despite clinicians wanting to refer promptly, many primary care professionals are unable to. Unfortunately, the EVRA study alone may not change the overall practice, and work is needed to overcome barriers faced by primary care professionals.
Background
Venous leg ulceration (VLU) affects up to 2% of the population worldwide and accounts for 60–80% of all cases of ulceration. 1 It is defined by the National Institute for Health and Care Excellence (NICE) as loss of skin taking more than two weeks to heal as a result of sustained venous hypertension. 2 Affecting mostly the older adult population, the wound care and treatment associated with VLU consume over £2.7 billion per year of the NHS budget. 3 In addition to the financial burden, VLU has a profound effect on a patient quality of life due to prolonged pain, immobility and social isolation. 4 District and community nursing teams are primarily responsible for the long-term management of VLU and spend 25–50% of their time caring for this patient population. 1
VLU does not currently have a set of standalone NICE guidelines; however, it is outlined within the guidelines for the Diagnosis and Management of Varicose Veins (NICE CG168). Recommendations include referral to a vascular specialist within two weeks of ulcer presentation for assessment and management, in addition to compression bandaging. 2 In the absence of a specific NICE guideline, the Royal Society of Medicine’s Venous Forum developed a guideline titled ‘Management of Patients with Leg Ulcers’ to guide clinicians in 2017 (Royal Society of Medicine Venous Forum, 2017) 5 (online Appendix 1). However, despite publication of the guidelines in 2013, there has been little improvement in how quickly patients are referred. 6 Unfortunately, delays in referral and barriers accessing specialist treatment are a global issue. A study from the Netherlands found that the median referral time to specialist services was 14.7 months, with patients experiencing an average of 2.73 ulcers before referral. 7 Additionally, a survey of US practitioners found disparities in the care pathway for patients presenting with venous ulceration. The study concluded that practitioners who are first to assess venous disease do not provide care in a uniform way. 8
The landmark trial providing evidence to support early referral and treatment of venous reflux was the EVRA trial (A Randomized Trial of Early Endovenous Ablation in Venous Ulceration), which showed that early treatment of underlying venous incompetence leads to improved healing rate and greater ulcer-free time. 9 In addition to publication in medical journals and presentation at national and international conferences, the study was also disseminated via nursing periodicals such as Wounds UK and the Nursing Times. Following the publication, initiatives were outlined for the development of a national wound care strategy and an increase in the workforce of an additional 5000 district nurses. 10
Aims
This survey aimed to determine the standards of referral and management of patients with venous leg ulceration in primary care after the release of the EVRA results.
Methods
To explore standards of referral and the management for patients with venous leg ulceration, an online 11- question survey was created. A short, simple design was utilized, and through the use of the online platform ‘Qualtrics Survey’, a voluntary, opt-in consent by completion approach was taken, allowing all responses to be anonymous. The platform enabled respondents to review and change their answers via the ‘back’ button in addition to being equipped with a completeness check highlighting incomplete answers to before the questionnaire could be submitted, this could however be overruled. Cookies were used to assign a unique-user identifier to each respondent computer and set on each page.
To ensure the appropriateness of questions, the survey was reviewed by several experts in the field of venous leg ulceration, who also have expertise in research methodology. Using the Health Research Authority (HRA) development tool, the survey was classed as a service evaluation and therefore was deemed not to require HRA/ethical approval.
The questions aimed to determine whether respondents were familiar with the EVRA trial, whether they could refer patients with venous leg ulceration directly to a vascular service and, if not, who was responsible for this. The questions also probed what proportion of patients with open and healed ulceration were referred to specialised vascular centres and their anticipated waiting times. Opinions were sought on the guideline recommendation that all patients with venous leg ulceration should be referred to a vascular service. The survey is detailed in online Appendix 2.
Survey distribution
Responses were collected over four months (September 2018–December 2018). The survey was circulated via local and national networks, such as the Tissue Viability Network and the Wounds Research Network (WREN) by attaching it to the monthly email bulletin forwarded to the regular mailing list. At the time, WREN had approximately UK 300 subscribers on their mailing list and 500 subscribed to the Tissue Viability Network mailing list. To increase awareness of the survey, it was also circulated via the RCN District and Community Nursing Facebook forum, which had approximately 5500 members that time. Therefore, the total distribution of the survey was to approximately 6000 health care professionals with an interest in wound care.
Data analysis
Continuous variables that followed a normal distribution were summarised using mean and standard deviation. Skewed continuous variables were summarised using median and interquartile range (IQR). The free text was categorised by common themes for the ease of interpretation.
Results
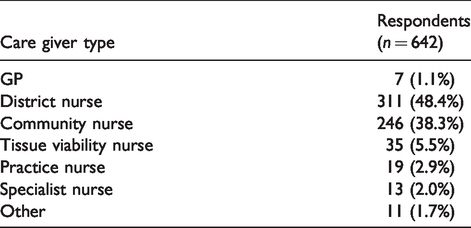
With a response rate of approximately 10% the survey received 643 responses in total, however, some participants did not answer all the questions. For clarity, the total number of responses are detailed for each question. The professions of respondents are outlined in Table 1, of all 643 respondents, only 90 (14%) had heard of the EVRA trial and 51 (8%) were familiar with the results.
Referring professional
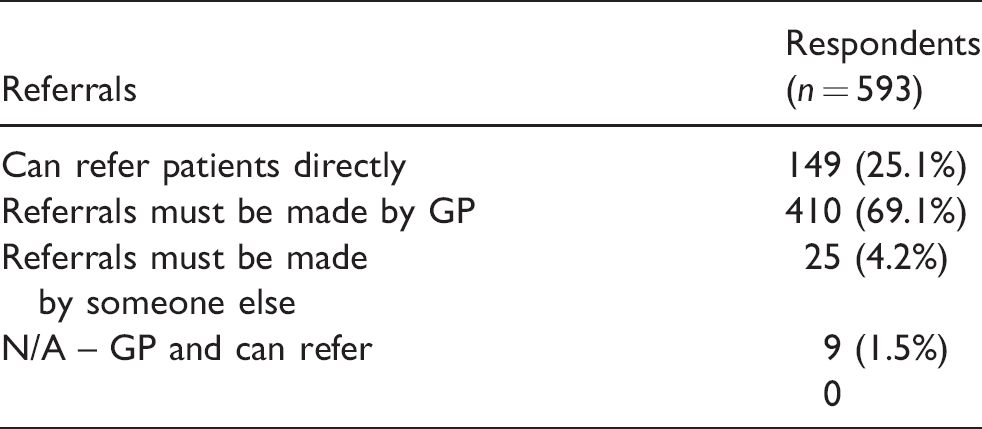
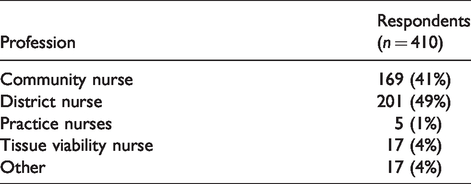
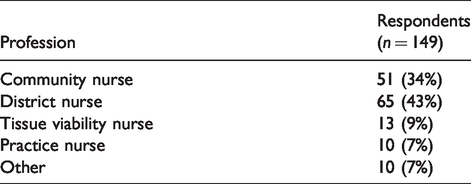
The vast majority of participants stated that referrals to specialist care had to be made by the GP (69%). Only 25% could refer patients directly. Details regarding the referral pathways are presented in Tables 2 to 5.
Respondent primary caregiver type.
Overall response to how leg ulcer referrals must be made to a specialised leg ulcer service.
Professionals stating referral to a specialised leg ulcer service must be made be a GP.
Professions of respondents who can refer directly to a specialist leg ulcer service.
Professions of respondents stating referral must be made by another member of staff.
Referral practices pre-EVRA publication
Respondents were questioned regarding how often they would refer patients with open venous leg ulceration to a specialist vascular centre before the EVRA results were published. Of the 589 respondents, 227 (47%) reported referring sometimes, 165 (28%) reported referring rarely, 119 (20.2%) reported referring frequently, 15 (2.6%) reported never referring and only 13 (2.2%) reported they would always refer.
When asked how often they would have referred patients with healed venous leg ulceration to specialist vascular centre before the EVRA publication, of 588 responses, we received the following responses: 278 (47.3%) would rarely refer (25% of the time), 225 (38.3%) would never refer, 67 (11.4%) would sometimes refer (50% of the time), 13 (2.2%) would frequently refer (75% of the time) and 5 (0.9%) would always refer.
Estimated waiting times
Respondents were asked how long they felt it would take for a patient to be seen by a vascular specialist after a referral had been made. The overall estimated median waiting time from community review to outpatient clinic assessment was eight weeks (IQR 4–12). Of 444 respondents, 304 (68.5%) assumed that patients waited six weeks to six months, 130 (29.3%) assumed that they waited less than six weeks and 10 (2.3%) assumed that they waited more than six months.
Change in practice post-EVRA publication
Respondents were asked if they will change their practice with respect to the referral of patients based on the EVRA study results. Of the 444 responses, only 53 (12%) reported that they already refer promptly. However, 128 (29%) reported that they will change their practice and face no barriers to do so; 198 (45%) reported that they would like to refer earlier but the decision is made by someone else. A further 48 (11%) reported that although they would like to change practice, they face certain barriers stopping them from doing so (Figure 1). Of respondents reporting that it was someone else’s decision (n = 198), 169 (85%) recorded that it was the GP’s decision, 10 (5%) the tissue viability nurse, 16 (8%) other and 4 (2%) not stated.
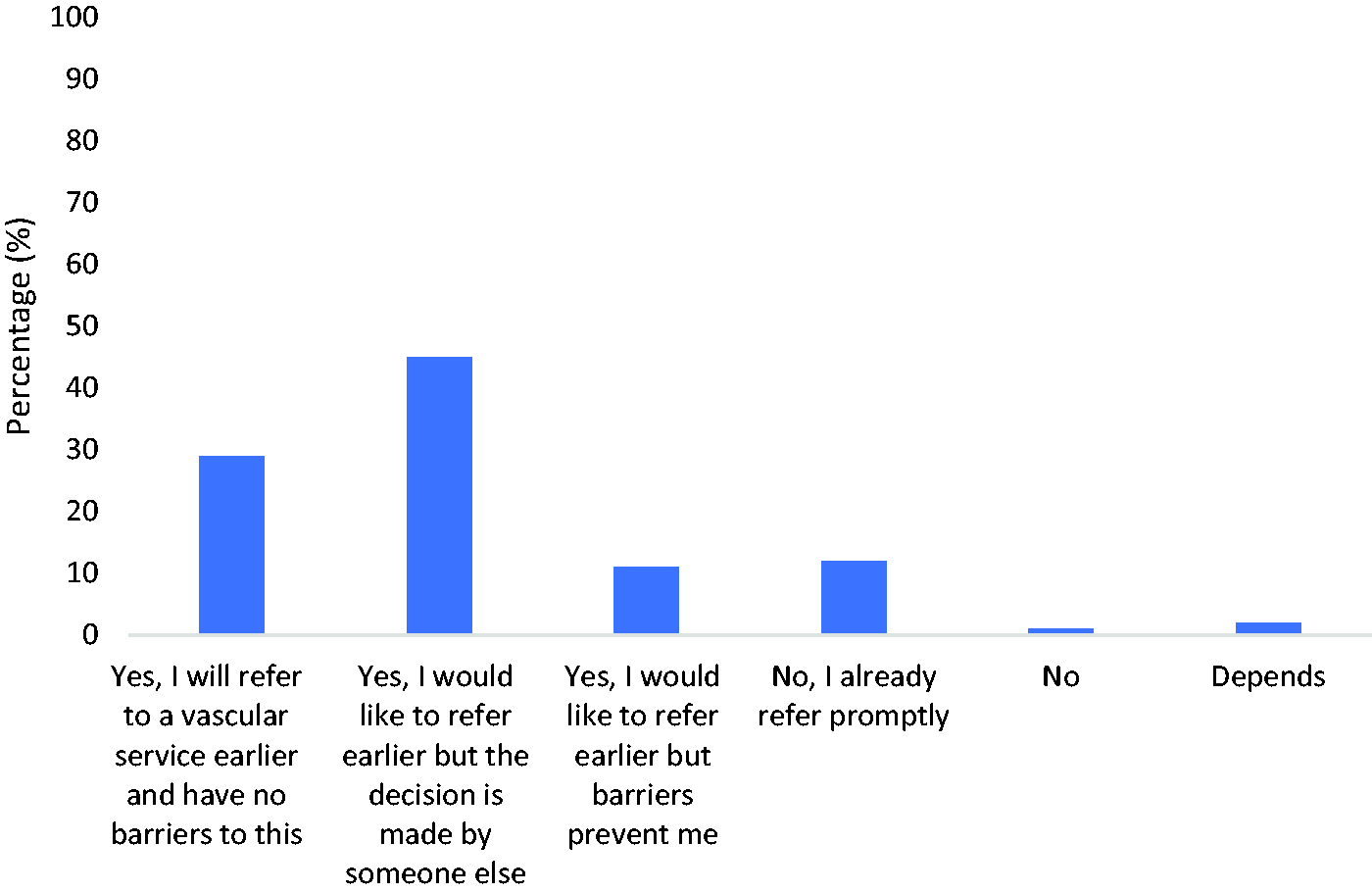
Practice change with respect to referral timing based on the EVRA results.
Using free text comments, the main barriers stated for changing practice were local referral pathway and policies, the capacity of vascular clinics and waiting times, training/confidence of the primary care professionals, availability of equipment such as Dopplers and time restrictions to perform the ABPI.
Guidelines
Of 450 respondents, 266 (59%) had heard of the NICE CG168 guideline, and 194 (43%) were aware of the guideline recommendation regarding referral to a vascular service. Respondents were then asked for their views on the recommendation that all venous leg ulcers should be referred to a vascular service for assessment and treatment. Of 449 respondents, 85 (19%) ranked the recommendation to refer all leg ulcer patients from zero to four (i.e. strongly disagree to disagree), 63 (14%) ranked the recommendation as five (neither agree nor disagree) and 301 (67%) gave a score of 6–10 (i.e. agree to strongly agree), including 60 (20%) of respondents who agreed strongly with the recommendation.
Discussion
Only a quarter of respondents reported that they could refer patients with a leg ulcer directly to a specialised vascular service with the remaining 75% requiring that referrals must be made by a GP, indicating a level of complexity in the referral pathway. It appears that some district, community and tissue viability nurses can refer directly, whereas some must refer via the GP, so the ability is not role-dependent and appears to be determined by local referral pathways. It is clear that GPs, therefore, act as the gatekeepers for the referral of patients into secondary care. GPs were not represented in this survey, and therefore their views and referral criteria have not been explored, which is a limitation of this survey.
Despite 43% of respondents reporting that they were aware of the NICE recommendations for referral, only 2% of respondents stated that patients with open leg ulceration were always referred to a vascular centre. A further 20% were frequently referred, and about half sometimes referred. Over one-third of patients were rarely and never referred which may be a reflection of the referral pathways. Additionally, despite evidence from the ESCHAR trial showing that surgical intervention can reduce the rate of ulcer recurrence, 85% reported that ulcer-healed patients were reported as rarely or never being referred. 11 Perhaps, another factor affecting referrals is the estimated waiting time for patients to be seen in clinic, which was a median of eight weeks.
Just under one-third of respondents reported that they would change practice with respect to referral timing and had no barriers to this, although 45% of respondents reported that they would like to change practice, but the decision was made by someone else, with 85% reporting that this was the GP’s decision. To encourage changes in practice, the publication of NHS England’s Commissioning for Quality and Innovation CCG indicator specifications for 2020–2021 now includes the need for a comprehensive wound assessment and referral to a vascular specialist. 12
When detailing barriers, it was apparent that guideline awareness is a problem; this is evident considering 41% of respondents were not aware of the NICE guidance. Of the respondents who were aware of the guidance, less than half stated being aware of what the guideline recommends for referral. In spite of the gaps in knowledge, the majority of respondents thought that referring all patients with a leg ulcer to a specialist vascular service was a good policy, with less than one-fifth disagreeing.
Although this survey provides some insight into venous leg ulcer care, it only provides an overview of the barriers faced by a proportion of healthcare professionals. More detailed and in-depth work is needed to understand the experience of all staff involved in the pathway, such as general practitioners, in addition to patients and their careers.
Conclusion
It is evident that there is variation across the board when it comes to local referral pathways for patients with venous leg ulceration. There is evidence that in many cases, local referral pathways restrict the referral of these patients to secondary care. Additionally, it is also clear that the publication of the EVRA trial alone may not change overall practice, and work is needed to overcome the various barriers faced by primary care professionals to implement best practice.
Limitations
The numbers of community and district nurse respondents were 246 and 311, respectively, which is approximately 1% of the community nurse population and about 8% of the district nurse population. Although the overall number of responses to this survey (n = 643) was encouraging, with nurses being the primary caregiver for venous leg ulcer patients, it still only represents a small number of a large community of professionals.
General practitioners were underrepresented in the survey. The survey did, however, provide good evidence that, in most cases, the GP decides whether or not to make a referral. More work is needed to understand the reasons why GPs do not refer to a vascular service when a patient presents with venous leg ulceration.
Supplemental Material
sj-pdf-1-phl-10.1177_0268355520944102 - Supplemental material for UK primary care survey of venous leg ulceration management and referral – Post-EVRA trial
Supplemental material, sj-pdf-1-phl-10.1177_0268355520944102 for UK primary care survey of venous leg ulceration management and referral – Post-EVRA trial by Francine Heatley, Layla B Saghdaoui, Safa Salim, Sarah Onida, Manj S Gohel and Alun H Davies in Phlebology
Footnotes
Acknowledgements
Wounds Research Network, Tissue Viability Network and Royal College of Nursing District and Community Nursing Group.
CONSORT reporting guidelines
This study has been reported in accordance with the EQUATOR guidelines. The CHERRIES checklist was used as it was the most appropriate for a survey-type service evaluation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Using the HRA development tool, the survey was classed as a service evaluation and therefore was deemed not to require HRA/ethical approval.
Guarantor
AHD
Contributorship
FH – Principle investigator of research and made substantial contribution to concept and deign of work; LBS – Drafted article; SS – Drafted article; SO – Drafted article and approved version to be published; MSG – Approved version to be published; AHD– Concept, design, drafted article and approved version to be published.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.