
Abstract

Introduction
Venous leg ulcers (VLUs) represent the most severe clinical presentation in the spectrum of chronic venous disease. Referring to an open skin lesion of the leg or foot in areas affected by venous hypertension, it is the most common cause of all chronic lower limb wounds, accounting for 70% of all leg ulcers. 1 It contributes to significant personal, financial, and social burden. VLUs can impair patients’ quality of life to a similar degree as heart failure or chronic obstructive pulmonary disease 2 and can be a source of social embarrassment from the malodourous exudates that come from the wound. 2 This represents only part of the societal costs, with financial implications of diagnosing and managing the condition taking up to 1%–2% of the annual healthcare budget of Western societies. This can amount up to €600–€900 million per annum in certain European countries.
With this clinical and socioeconomic burden, provision of appropriate treatment of VLU is clearly of clinical importance. As recommended by multiple international and national guidelines,3,4 the management of VLUs involves a combination of wound care, compression therapy, and early treatment of venous insufficiency. Despite these recommendations, there are still patients who fail to receive adequate treatment when they present with VLUs, leading to failure of VLU healing. With appropriate treatment, most VLUs heal within 6 months of receiving treatment.
This article seeks to highlight the management recommendations of VLUs from the International Union of Phlebology (UIP). This is accompanied by a one-page summary of treatment options and an algorithm that can be followed by any clinician that may encounter patients with VLUs (Figure 1). It also highlights diagnostic steps that can help guide clinicians in accurately identifying VLUs to ensure treatment be appropriately targeted to the right population. The one-page guideline.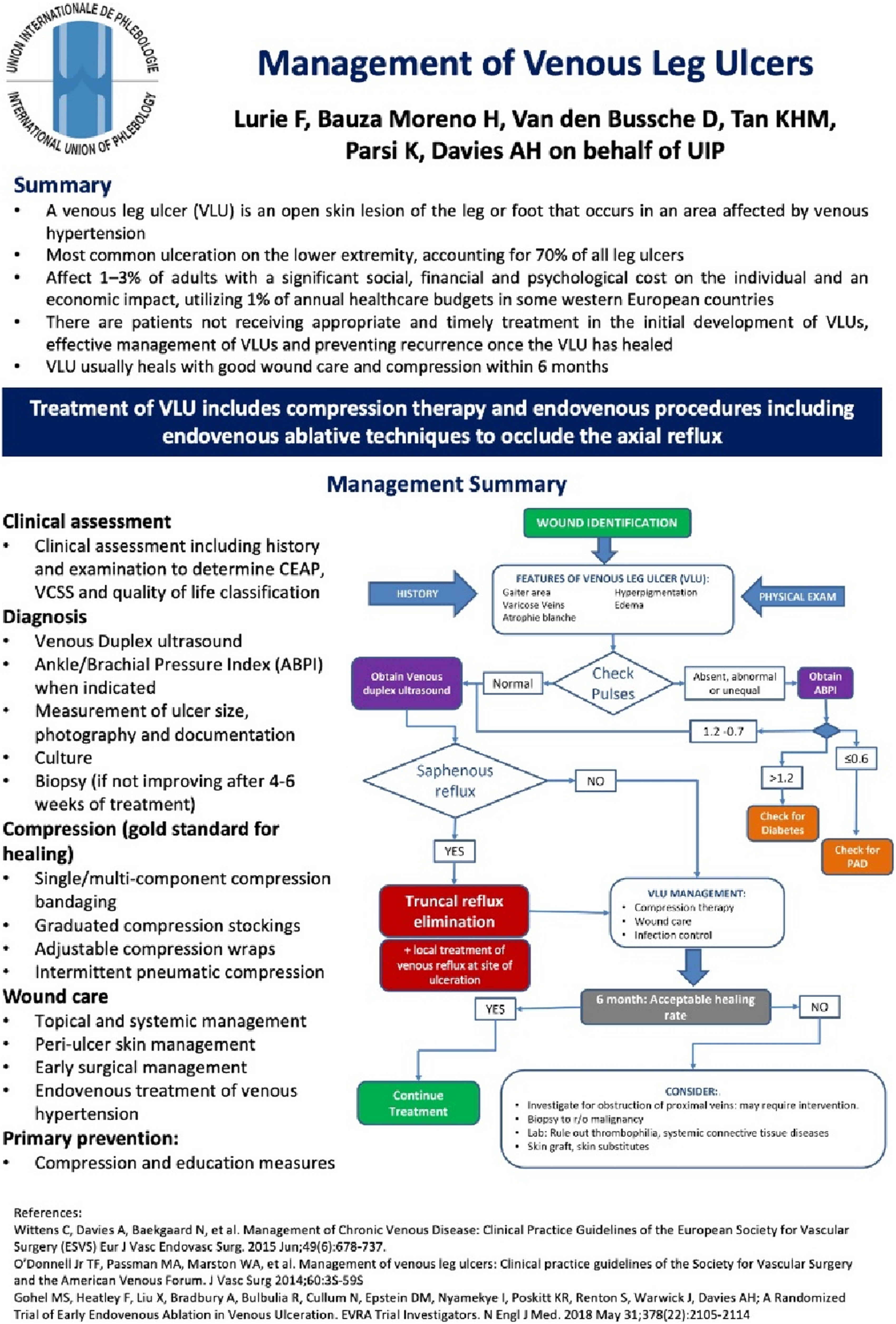
Management recommendations
All patients presenting with a lower limb ulcer should first undergo detailed clinical assessment. This should include a clinical history and physical examination, observing for features of VLUs. These include an ulcer in the gaiter region together with other clinical features of chronic venous disease (e.g. eczema, haemosiderin deposition, and varicose veins). During examination, the clinician should also check for lower limb pulses. If there are signs of absent, abnormal, or unequal foot pulses, it is recommended that the patient’s ankle brachial pressure index (ABPI) is measured. Should there be an abnormal ABPI, patients should be referred to a vascular specialist for further investigations. An ABPI of ≤0.8 warrants further workup and early management of concomitant peripheral arterial disease, and clinicians should check for diabetes mellitus if the patient’s ABPI is ≥ 1.2.
As part of the clinical workup, clinicians should also consider assessing clinical severity using validated scores including the Venous Clinical Severity Score and quality of life using both generic (e.g. EuroQoL-5 domains) and disease-specific instruments (e.g. VEINES-QOL/Sym questionnaire). The size of the ulcer should be measured, and photographs taken for documentation. If there are local or systemic features (e.g. increasing pain, discharge from ulcer, worsening erythema, and fever) that lead to clinician suspicion of infection, a wound swab should be taken for microbiological culture to identify any bacterial species that may put the VLU at risk of infection.
Venous duplex ultrasound is recommended as the gold standard imaging modality to determine the presence of venous reflux and obstruction, including assessment of patients’ proximal veins (e.g. iliac veins). Patients with identified truncal reflux (defined as reflux in the great saphenous, small saphenous, and/or anterior accessory saphenous veins) should undergo procedures to eliminate this reflux, including endovenous ablative techniques such as radiofrequency ablation or endovenous laser ablation. Additionally, local treatment of reflux at the site of ulceration should be performed. All patients with VLUs should receive good wound care, infection control, and compression therapies, which is the gold standard for healing. Compression treatments include bandaging, stockings, wraps, and intermittent pneumatic compression.
It is recommended that patients be followed up regularly to monitor the healing rate of the VLU. If there is acceptable healing at follow-up, the patient should continue their regular treatment. However, if the VLU is not showing signs of improvement or has deteriorated, further investigations and treatment options are warranted. Clinicians should consider performing biopsies to rule out malignancy and blood tests to rule out thrombophilia and systemic connective tissue diseases. Clinicians may also consider applying skin grafts or other skin substitutes that provide a scaffold for epithelialisation of the wound to help with poor healing.
Discussion
This article provides a one-page clinical practice guideline summarising the clinical management of VLUs. It is part of a series of publications for the International Union of Phlebology (UIP) One-Page Guidelines which are aimed at ensuring that patients with venous disease receive timely and appropriate care based on current best evidence and expert consensus.
VLUs represent the most severe form of CVD and lead to significant impairments in patients’ quality of life. Despite this, patients still often fail to receive acceptable levels of treatment, leading to a prolonged course of healing and high rates of recurrence of up to 70% at 5-year follow-up. 5 The one-page guideline from the UIP reiterates the importance of patients receiving the gold standards of VLU management, which includes treatment of venous reflux. This is in line with landmark clinical trials including ESCHAR 6 and EVRA 7 which showed improved wound healing and reduced recurrence rates following venous treatment. The EVRA trial also showed the timing of such procedures to be important, with earlier ablation showing clear benefits in VLU healing compared to deferred treatment. 7 However, there are still a good proportion of patients not receiving timely and appropriate treatment due to delayed recognition of venous hypertension by frontline healthcare providers, leading to increased healthcare resource utilisation. 8 This one-page summary may improve this by highlighting signs consistent with venous hypertension for frontline staff members, improving identification and timely referrals.
While the effectiveness of wound care, compression, and venous treatment in VLU healing has been clearly shown, the efficacy of adjuncts treatments in VLU healing, including systemic medications and procedures such as graft application, has yet to be studied in detail. One such oral therapy is pentoxifylline, which has been shown to be a useful adjunct in VLU healing. 9 Skin grafts for VLU healing has been the subject of a previous Cochrane review, with 17 studies only showing evidence for improved healing with bilayer artificial skin. Insufficient evidence was seen for other types of skin grafts (e.g. porcine xenografts and autografts). 10 Improving VLU healing should be a clinical priority, and with little change in treatment algorithms over the last decade, more focus should be given to trials studying these promising adjunctive treatment modalities.
For healthcare providers, this article and summary document should highlight the severity of VLUs and the impact of VLUs on both physical and mental wellbeing of their patients. Primary care physicians and other healthcare staff members such as tissue viability nurses should be reminded to refer the patient urgently to be seen by a vascular specialist for further evaluation and management. From there, vascular specialists are advised to assess each patient carefully and tailor management to each individual case. This is in line with multiple national and international guidelines and reinforced by this one-page guideline. This will facilitate the urgent assessment and interventions indicated in this population of patients to improve VLU healing and reduce burden of disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
Professor Alun Davies on behalf of the UIP.
Contributorship
K.P. and A.H.D. conceptualised the design of the short report and one-page guideline. F.L., H.B.M., and D.V.d.B. contributed to the literature review and formulation of the recommendations. M.T. contributed to the formatting and layout of the one-page guideline (![]() ) and wrote the initial draft of the short report. All authors reviewed the short report prior to submission.
) and wrote the initial draft of the short report. All authors reviewed the short report prior to submission.