
Abstract

What is a venous leg ulcer (VLU)?
A venous leg ulcer (VLU) is a wound on the lower leg or foot that occurs due to chronic venous disease and venous hypertension. Blood is pumped away from the heart through the arteries and returned to the heart through the veins. The veins have one-way valves to keep blood flowing in one direction. When the valves do not close properly, the blood can flow back in the wrong direction, which is called venous reflux. Venous reflux can cause an increase in pressure in the venous system, which is referred to as venous hypertension. Prolonged venous hypertension causes tissue damage leading to VLUs. Chronic venous disease includes all manifestations of venous disease, including spider veins, varicose veins, leg swelling and skin changes, and VLUs. The term ‘chronic venous insufficiency’ is used for the more severe forms of chronic venous disease with skin changes and skin breakdown. VLU is the most advanced form of chronic venous insufficiency.
What are the symptoms of VLUs?
VLUs most often occur on the inside of the lower leg and above the ankle. The ulcer may have irregular borders with a red base (Figure 1). Patients with VLUs often have a history of chronic venous disease. Symptoms of chronic venous disease include leg swelling, aching, itching, fatigue, heaviness, throbbing, or cramps. These symptoms may be worse at the end of the day or after sitting or standing for long periods when the blood pools in the lower legs. The leg may turn a dark color when the iron in the blood leaks out and stains the skin (hemosiderin staining), and the skin may become hardened (lipodermatosclerosis).

Image of a venous leg ulcer (VLU) with associated hemosiderin staining (brown discoloration) and lipodermatosclerosis (skin hardening).
Who is at risk for VLUs?
VLUs are more common with older age because the vein valves can wear out over time. Being overweight can increase the pressure in the veins in the abdomen, making it more difficult for blood to return from the legs to the heart. Being sedentary, prolonged standing, and muscle weakness in the lower legs can also contribute. A history of venous reflux, varicose veins, or blood clots can increase pressure build-up in the veins, increasing the risk for VLUs.
Are there other causes of leg ulcers?
Other causes of leg ulcers include diabetic foot ulcers, pressure ulcers, and arterial ulcers. 1
Diabetic foot ulcers
Diabetic foot ulcers are due to a combination of foot deformity, peripheral neuropathy, decreased arterial blood flow, and pressure injury. Neuropathy causes decreased sensation leading to increased injuries or trauma to the feet. The ulcers are often found in areas that are difficult to see, including the bottom of the toes, foot, or heel. To heal these ulcers, the offending injury or pressure needs to be removed, and patients may require special shoes or other off-loading devices. Good glucose control is important, and any underlying arterial circulation issues (peripheral artery disease, or PAD) that may be slowing the healing process need to be addressed.
Pressure ulcers
Pressure ulcers most often occur in areas of bony prominence of the feet and require appropriate off-loading to relieve the pressure for healing.
Arterial ulcers
Arterial ulcers occur in patients with PAD, or blockages in the arteries that carry oxygen-rich blood to the legs and feet. When adequate blood flow is unable to reach tissues in the legs, a minor injury can lead to a prolonged ulcer. Arterial ulcers are often painful and usually located on the toes and feet.
What tests are used to diagnose VLUs?
The initial diagnosis of a VLU is made by a clinical evaluation by a health care provider. The patient will be asked questions about the wound (such as how it formed and duration) and may also be asked about physical activity, exercise habits, weight changes, occupation, and injuries. Body position is also important because sleeping in a chair or sitting for extended periods in a wheelchair can increase the pressure (venous hypertension) in the legs. Medical history includes reviewing medications (including antibiotics), prior or current blood clots, diabetes, PAD, connective tissue disease, autoimmune disorders, and any previous wounds. Next, a physical examination is performed, including assessment for swelling control, skin condition around the wound, skin infection (cellulitis), range of motion of the ankles, and leg or foot deformities.
An ultrasound of the leg veins can detect underlying venous disease in the entire leg and around the wound. For more information on ultrasounds, please see the Patient Information Page titled “Venous reflux testing”. 2 Occasionally, further imaging is necessary, such as a computed tomography (CT) scan to look for compression of the veins in the abdomen and pelvis.
How are VLUs treated?
Compression therapy
Compression therapies are used to treat leg swelling and to help the calf muscles return blood up the leg. There are two types of compression therapies: static compression and dynamic compression. Static compression refers to multilayer bandages that put pressure around the leg. The strength of this pressure varies depending on the wrap. Both inelastic and elastic compression bandages are used, but nonelastic bandages are usually more effective. With dynamic compression, a pumping device can apply pressure in segments in a massage-like movement on the leg for short periods of time, often in cycles. Dynamic compression systems are most effective when used for as many hours a day as possible. Overall, compression therapy helps the wound heal more quickly and reduces the risk of recurrence. One way to reduce swelling further is to elevate the legs above the heart level by lying down and propping the legs up with two pillows. Swelling control is essential for VLU healing.
Exercise
In cases of VLU in patients with weak calf muscles, which may not pump the blood effectively, exercise to strengthen the calf muscles can help with returning blood up the leg. Exercise programs can shorten the time it takes to heal VLUs.
Wound care treatments (cleaning, debridement, and dressings)
Ulcers should be kept clean and washed regularly with water and a mild soap that does not irritate the wound. A process called debridement promotes the healing of the ulcer. Debridement involves thorough cleaning of the wound and the removal of the dead, callused, or infected skin, the bacterial build-up, and any dead tissue or other debris on and around the wound.
Ulcers that are leaking fluid may need to be wrapped in a large bandage called a dressing. The dressing keeps the ulcer moist but absorbs the excess drainage from the wound. The VLU needs to stay moist to promote a healing environment, but too much moisture can prevent wound healing. Specialized ulcer dressings are used to keep the level of moisture at a proper level for wound healing and to reduce inflammation.
After trying initial treatments, including debridement, dressings, and compression therapies, advanced skin substitute products (usually stem cell products derived from animals or neonates) may be used if VLUs are slow to heal.
When are antibiotics needed for VLUs?
Wounds always have bacteria on the surface, but sometimes the bacteria can cause problems, resulting in an infection. Wounds may need to be swabbed to determine the kind of infection. If pathologic bacteria are present and the area is inflamed, oral antibiotics may be prescribed. Topical antibiotics can be used on wounds but are not effective if the infection has spread to the surrounding tissue or into the bloodstream.
When is invasive treatment required for VLUs, and what are the options?
Some wounds require a vein procedure if the patient’s underlying venous disease is causing excessive venous hypertension. Venous procedures (such as ablation or sclerotherapy to close veins or surgical vein removal) have been shown to speed up the healing of VLUs. For example, if one of the superficial veins in the lower leg is found to have venous reflux (leaky vein valves), the doctor may collapse the vein to re-route the blood through a healthy vein with functioning valves.
What are the complications of VLUs?
VLUs can affect quality of life. It can be difficult or dangerous to perform daily activities with an open wound on the leg. Frequent use of antibiotics increases the risk of developing resistant bacteria. Treatments, both at-home care and hospital visits, can be time-consuming and frustrating. The cost of treatment and the potential reduced work hours or even job loss can create a significant financial burden. 3 Having a VLU increases the risk of depression and anxiety, as well as frustration from needing the help of others. VLUs have a high recurrence rate, especially if not cared for properly.
What is the best way to care for the skin to prevent future VLUs?
Patients with VLUs and chronic venous disease benefit from following a special skin care regimen to keep skin moisturized and to minimize scaling and irritation. It is good practice to inspect the legs, feet, and in between toes daily to look for any cuts or sores, changes in color, or breaks in the skin that could lead to infection. A pH-balanced cleanser should be used for routine cleansing. Alkaline soaps should be avoided because they can increase water loss. Moisturizers and mild cleansers should be labeled ‘fragrance-free’ with no added colors. Emollients (e.g., petroleum jelly, mineral oils, lanolin, and ceramides) prevent water loss and are good for keeping the skin supple. Humectants (e.g., urea, glycerin, and alpha-hydroxy acids) pull water into the skin and work well for very dry skin. The best time to apply moisturizers is after a shower when the skin is clean and slightly damp. Moisturizers should not be used in between toes, an area that should be kept dry to prevent fungal infection. Table 1 shows how to address various skin problems that may contribute to VLUs.
Care of various skin types. Good skin care can help prevent recurrent venous leg ulcers.
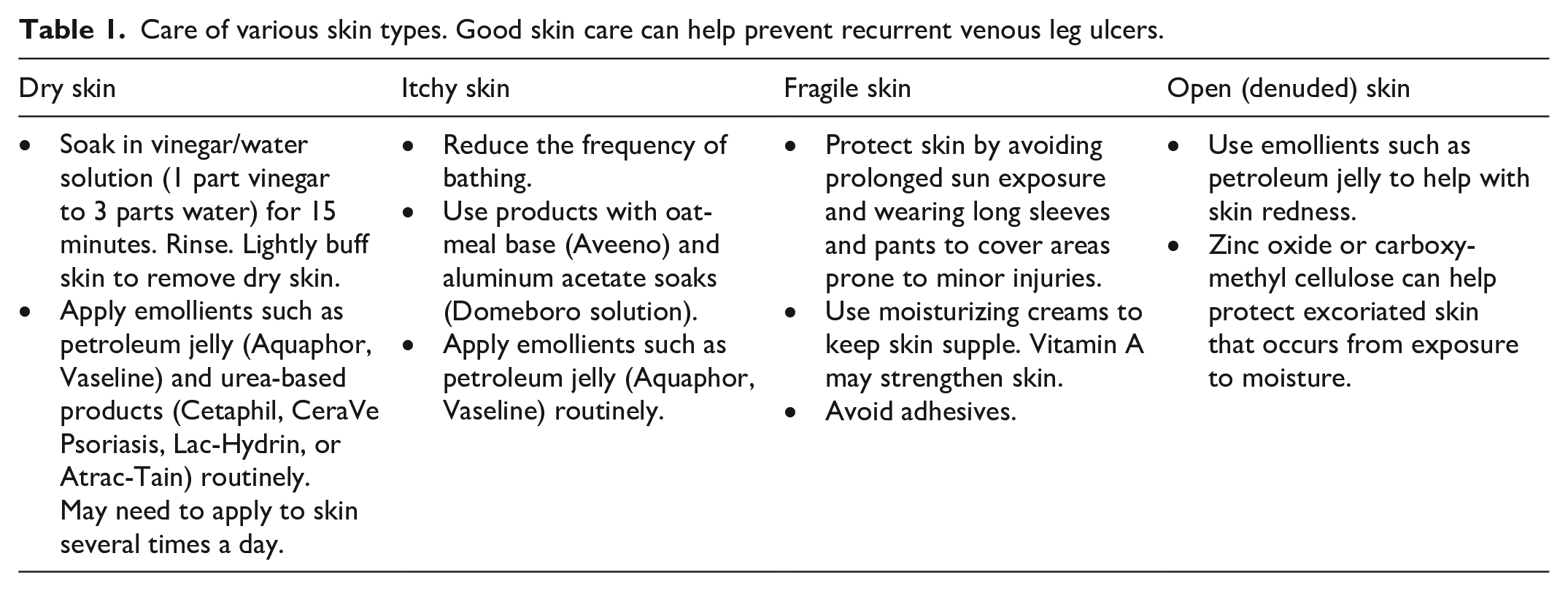
As aging occurs, the skin becomes more fragile from the loss of collagen and fat tissue. The sensory receptors in the skin decrease, and blood flow is reduced. Pressure, friction, and shearing can then increase the risk of skin breakdown. It is important to pay attention to relieving pressure in between the legs, especially in areas of bony prominence.
What else can be done to prevent VLUs?
To prevent VLUs from returning, the first step is to manage the leg swelling with compression and leg elevation. Wearing compression stockings or bandages will help the valves in the veins move blood back up to the heart. Maintaining a normal body weight is key, and getting 30 minutes per day of moderate-intensity exercise is important for overall cardiovascular health. For patients with vein problems, exercises should focus on strengthening the calf muscles. The calf muscles are vital because the contraction of the calf helps to pump the blood through the veins back to the heart (Figure 2). Exercises that promote this movement include walking and cycling. Repeated motions like rocking on the feet (alternating between heels and toes) and standing on tiptoes also help to strengthen the calf muscles.
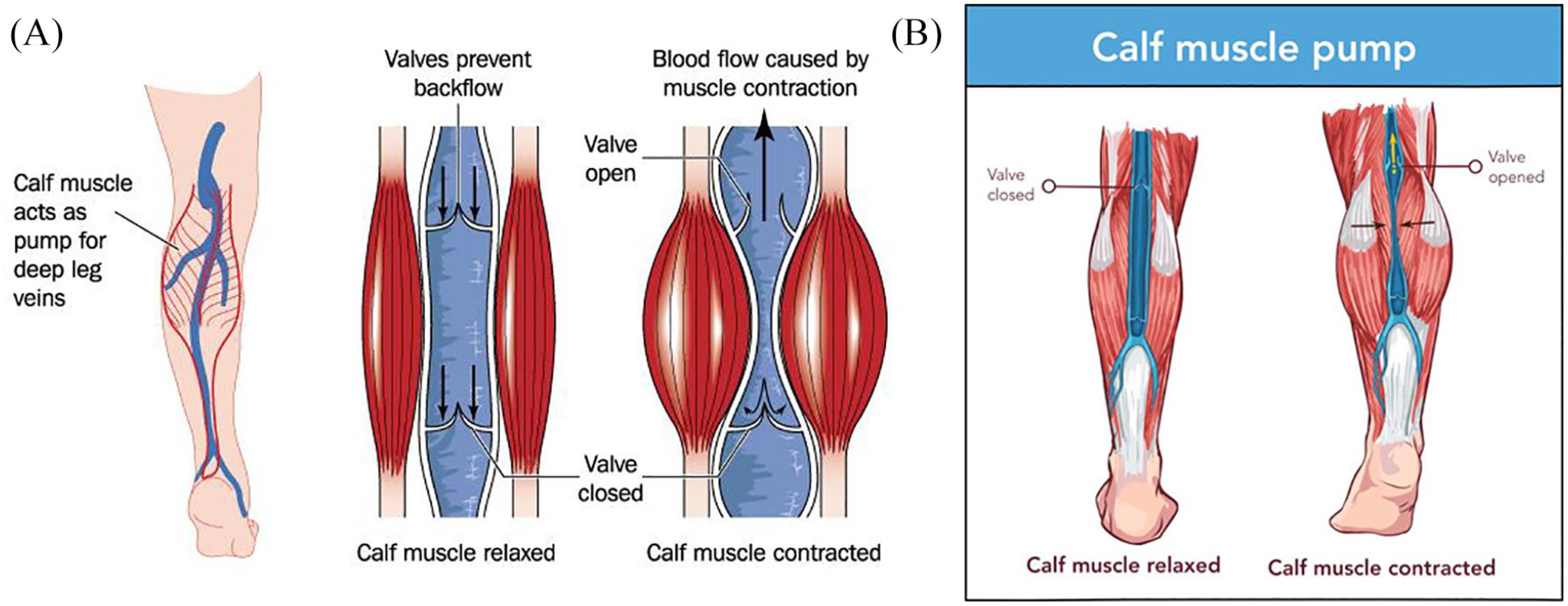
Function of the calf muscle pump. The calf muscle pump helps to return venous blood from the legs to the heart and reduce venous hypertension. By performing calf exercises, such as walking or ankle pumps, the calf muscle contracts to squeeze the blood through the valves to move blood back up to the heart.
Regularly wearing compression stockings, even after VLUs have healed, will reduce the pressure in the venous system of the lower legs. For more information on compression, refer to the Vascular Disease Patient Information Page “Compression therapy”. 4
Summary
VLUs are wounds of the lower leg that are caused by venous hypertension and chronic venous disease. These ulcers are often found on the inside of the lower leg and can be painful or irritating. Other symptoms of chronic venous disease include swelling of the leg, leg muscle fatigue, leg cramping or throbbing, and discoloration of the skin. Standard treatments for VLUs include cleaning and debridement of the wound, wound dressing, and compression therapies. Some patients with VLUs may require antibiotics or vein procedures. Most wounds close in a few weeks to a few months, depending on the size of the wound. However, VLUs that last longer, or show no signs of improvement, should undergo further evaluation and testing. VLUs often recur, but compression therapies and good skin care significantly reduce this risk.
The ‘Vascular Disease Patient Information Page’ is a regular feature of Vascular Medicine. All articles in the collection are available for free online at http://journals.sagepub.com/vmjpatientpage.
The Vascular Disease Patient Information Page is provided for educational purposes only and is not a substitute for medical advice.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Dr Elizabeth Ratchford’s work was supported in part by the generosity of David Kotick (1926–2021).