
Abstract
The interpersonal process model of intimacy suggests that intimacy within dyads develops when open communication from one dyad member is met with validating, understanding and caring responses from the other dyad member. Little is known about interpersonal processes between informal caregivers and care recipients in different illness contexts (i.e., coping with neurological, physical or other impairments/comorbidities) and relationship types (i.e., spouses, adult children and others), and how interpersonal processes are linked to the caregivers’ wellbeing. In this cross-sectional study, caregivers (N = 882) from nine countries reported on their open communication with care recipients, care recipients’ responsiveness, and caregivers’ wellbeing (i.e., intimacy, burden and communal motivation to care). Although caregivers of care recipients with neurological impairments and adult child caregivers reported lower mean levels of open communication and perceived responsiveness, similar mediating effects of perceived responsiveness between open communication and intimacy (effect = 0.05; CI95 = [0.04, 0.06]), burden (effect = −0.42; CI95 = [−0.49, −0.35]), and communal motivation to care (effect = 0.28; CI95 = [0.21, 0.36]) were reported across different illness contexts and relationship types. Only the negative relationship between perceived responsiveness and burden was stronger for spouses (b = −0.23, CI95 = [-0.26, −0.19]) than for adult children and others. Results suggest the interpersonal process model of intimacy may be used to identify caregivers at risk of poor wellbeing in different illness contexts and with different relationships with their care recipients. Lack of open communication and caregivers’ misperceptions of care recipients’ responsiveness may represent opportunities to intervene to enhance caregivers’ intimacy to the care recipients, communal motivation to care, and to decrease caregiver burden.
Introduction
According to the interpersonal process model of intimacy, intimacy is likely to develop and increase within relationships when partners openly communicate feelings and stress to each other and, as a result of their partners’ responses, come to feel understood, validated, and cared for (i.e., perceived responsiveness) (Reis & Shaver, 1988; Laurenceau et al., 2004). Several studies among the general population provide support for the interpersonal process model of intimacy in romantic and spousal relationships (hereafter referred to as spouses) (Candel & Turliuc, 2021; Laurenceau et al., 1998; 2004; 2005; Lippert & Prager, 2001). The model has also applied to couples dealing with illness, specifically cancer, suggesting that open communication behaviours, such as constructive communication and emotional disclosure of cancer-related concerns, are associated with higher levels of intimacy via perceived responsiveness (Manne et al., 2004, 2014, 2018; Manne & Badr, 2010; Porter et al., 2009). Moreover, a limited number of studies have tested the interpersonal process model of intimacy linked to psychological wellbeing. For example, interpersonal processes have been found to be related to lower levels of distress and greater psychological adjustment in couples dealing with cancer (Manne & Badr, 2010; Lepore & Revenson, 2007). However, some studies suggest open communication is not always beneficial. For example, increased distress, burden and worsened physical wellbeing has been reported in partners after sharing illness-related concerns, potentially due to awareness-raising of concerns and a mismatch between one’s need to talk and the other’s ability to respond in a caring, understanding, and validating way (Hagedoorn et al., 2011; Manne et al., 2004; Porter et al., 2009; Hasson-Ohayon et al., 2022).
The number of studies suggesting how relational and psychological wellbeing develop from interpersonal processes (i.e., open communication and perceived responsiveness) is growing. However, research about these processes in illness contexts other than cancer, in non-spousal relationships, and specifically in caregiver and care recipient relationships, is scarce (Revenson et al., 2016). Caregivers are individuals caring for a relative or a friend facing illness, disability, or any care need (Gérain & Zech, 2019). The provision of care to a loved one can be an integral part of many close relationships, and is often associated with decreased relationship quality, increased burden, and poor motivation outcomes (Carboni-Jiménez et al., 2021). Caregivers may also face different challenges in different illness contexts (Pinquart & Sörensen, 2011). A focus on the diversity of the illness contexts is relevant to understand factors contributing not only to the caregiver’s relationship with the care recipient but to the caregiver’s wellbeing and motivation to care in different situations. In order to expand the current literature and inform the development of evidenced-based caregiver interventions, an understanding of interpersonal processes, considering different illness contexts and relationship types between caregivers and care recipients, is essential (Revenson et al., 2016). Considering a wide range of relationships including spousal but also adult-child parent dyads, siblings, other family members or friends, might provide a better understanding of caregiving, as care is almost equally directed towards spouses and other family members, mainly older parents (Colombo et al., 2011).
The first step to address this important knowledge gap, is to explore whether there are differences, based on care recipients’ illness and caregiving relationship type, in how caregivers communicate with care recipients and how caregivers perceive care recipients respond to them during an interaction. It is plausible that the type and severity of the care recipient’s illness may have an impact on the caregiver – care recipient interactions. For example, care recipients with cognitive impairments or mental health problems have more difficulties communicating or being responsive than care recipients without cognitive or mental health problems (Kimberlin et al., 2004). However, some studies demonstrated that in advanced diseases such as dementia, where communication processes are strongly impaired, aspects of communication and perceived responsiveness might still be important for both dyad members. For example, spousal caregivers of care recipients with dementia were found to benefit from positive verbal and non-verbal communication (e.g., problem discussion and humour) with their husbands (Braun et al., 2010; Bannon et al., 2022). It is unclear to what extent advanced neurologic diseases (e.g., dementia, stroke, neurologic injury) may complicate interactions or whether open communication and perceived responsiveness are always important for different caregiving relationships (Revenson et al., 2016).
Due to the unique nature of close relationships, differences may exist between spousal and adult-child caregivers (e.g., intensity of care, living arrangements, depression and burden, and psychosocial needs) (Dang et al., 2022; Pinquart & Sörensen, 2011). For example, evidence suggests perceived responsiveness might take different forms depending on relationship type, for example in spousal, filial, or other (Le et al., 2018). At the same time, open communication, collaboration, and congruent dyadic behavioral responses to care, usually considered beneficial for couples, were also found among adult daughter – older parent dyads (Ferraris et al., 2022). While research on adaptation to chronic illness has highlighted how open communication about stressors is fundamental for couples (Bodenmann, 2005), less attention has been given to communication in non-spousal dyads, limiting comparisons between different dyad types (Ferraris et al., 2022). Therefore, there is a need to explore potential differences in interpersonal processes, across different illnesses and relationships, to identify which caregivers may benefit more from interventions targeting communication.
Secondly, given the above-mentioned potential differences, there is a need to explore whether the interpersonal process model of intimacy varies (or not) based on different illness contexts and relationship types. That is, testing and expanding the model of intimacy to explain how relational and psychological wellbeing develops during caregiver – care recipient interactions and when to provide support in different caregiving contexts. Currently, we do not know whether the same pathway occurs in other illness contexts (e.g., not only cancer) and for other relationship types (e.g., adult children and parents, other family relationships and friendships). It is plausible that different illness contexts and relationship types, might either strengthen or weaken intimacy processes. While exploring different illness contexts, existing research suggest that, similarly to couples in the cancer context (Laurenceau et al., 2005), couples coping with mild Parkinson’s disease (Champagne & Muise, 2022), and with physical disabilities (Zhaoyang et al., 2018; Hofsöe et al., 2018) benefit from interpersonal processes, in terms of enhanced intimacy and psychological wellbeing. At the same time, communication-responsiveness associations resulted strongly compromised in neurological diseases (e.g., dementia), undermining intimacy and wellbeing outcomes in spousal dyads (Poon, 2019). With regard to caregiving relationship types, spousal and non-spousal relationships might benefit differently from perceptions of responsiveness from the other dyad member. Extensive literature has highlighted the benefits of reciprocity and dyadic communication among spouses (Kuijer et al., 2001; Ybema et al., 2001; Bodenmann, 2005). However, in a different type of relationship (e.g., adult child-older parent) intimacy and communication processes might determine different patterns of wellbeing outcomes. Except for a limited number of studies that have provided evidence on the intimacy model in developing friendships in the general population (Laurenceau et al., 2005; Sanderson, 2004; Shelton et al., 2010), no other studies to date have applied the model to other non-spousal relationships within caregiving contexts. In the present study we seek to clarify whether and how different care recipients’ illness might moderate communication-responsiveness associations; and explore whether different types of relationship might moderate the associations between perceived responsiveness and wellbeing outcomes.
Thirdly, little is known about the impact of interpersonal processes on the caregivers’ wellbeing such as burden (Gérain & Zech, 2019) and motivation to care (Ferraris et al., 2022; Zarzycki & Morrison, 2021). If caregivers are overburdened and not sufficiently motivated to care, they might provide low quality of care and/or ineffective forms of support for their care recipients’ needs, resulting in risks for negative outcomes for both dyad members (Fenton et al., 2022). One specific type of motivation that develops within interpersonal relationships and still poorly investigated in the caregiving context, is communal motivation to care that is defined as “care and concern for the welfare of others” (Le et al., 2018). Evidence suggests communal motivation acts as a buffer against perceived stress of caring for others in high need (e.g., with illness) among nurses (VanYperen et al., 1992), among caregivers of cardiac patients (Thompson et al., 1995), and among caregivers of Alzheimer patients (Williamson & Schulz, 1990). However, interpersonal processes which may lead to different levels of communal motivation to care have remained largely unexplored among different illness contexts and caregiving relationship types (Mills et al., 2004). Therefore, in the present study we seek to explore whether the degree to which caregiver’s open communication with the care recipient is associated with burden and communal motivation to care, also depends on the mediating nature of the caregiver’s perceptions of care recipient’s responses (i.e., perceived responsiveness).
Aim of the Study
Based on the above knowledge gaps, the current study addresses these unexplored questions first by exploring potential differences in interpersonal processes (i.e., open communication and perceived responsiveness) based on (a) the illness context (e.g., care recipients’ physical, neurological, other impairments/comorbidities) and on (b) the caregiving relationship type (e.g., spouses, adult children and others); and second, by testing and expanding the interpersonal process model of intimacy in a multinational group of caregivers participating in the ENTWINE iCohort study taking into account diversity of illness contexts and relationship types. By doing so, we examine whether higher levels of caregivers’ open communication with the care recipients are associated with caregivers’ higher intimacy with the care recipients, lower burden, and higher communal motivation to care through the mediation of caregivers’ perceptions of care recipient’s responsiveness. We will also explore the moderating effects of illness contexts in the association between open communication and perceived responsiveness and of relationship types between perceived responsiveness and intimacy, burden, and communal motivation. See Figure 1 for the proposed moderated mediation model. The proposed moderated mediation model. Note. CG = caregiver; CR = care recipient.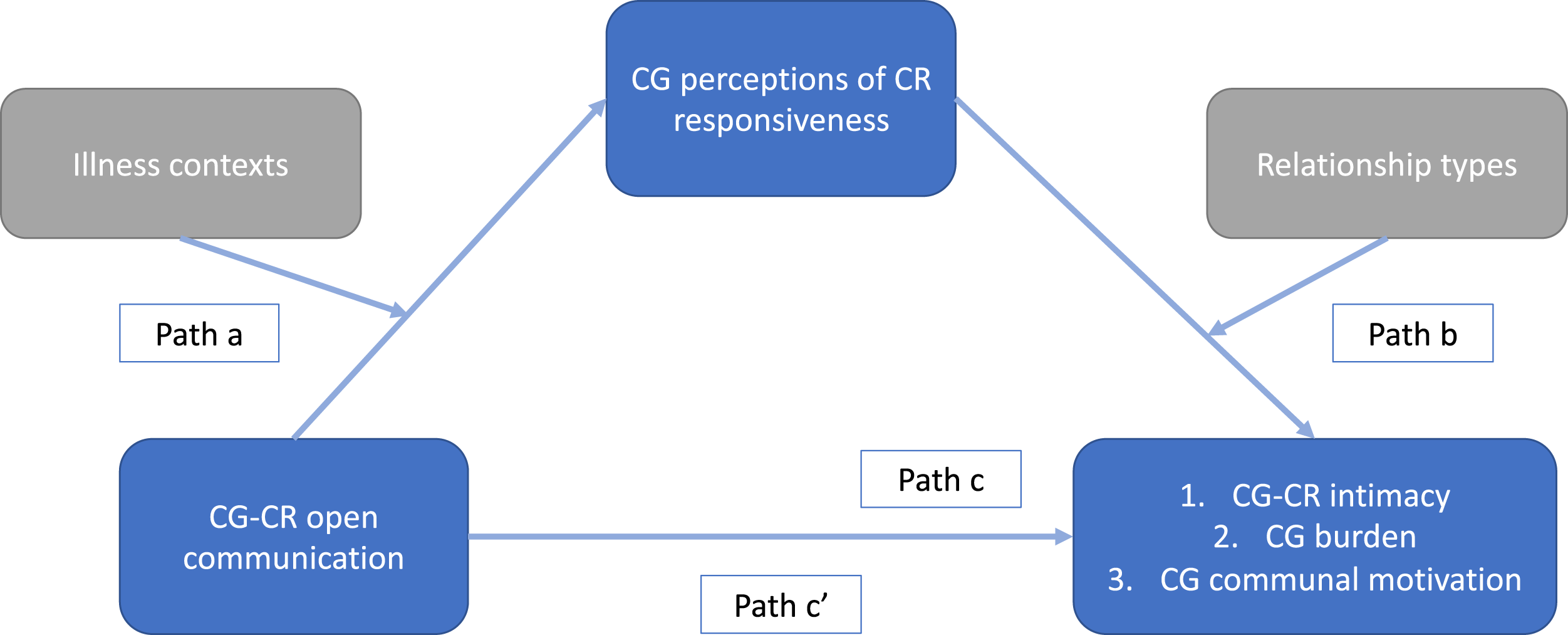
Method
Participants
This study uses baseline data from the ENTWINE iCohort, a multinational, transdisciplinary, longitudinal study incorporating intensive longitudinal methods (i.e., weekly repeated assessments for 6 months) to explore caregivers’ and care recipients’ experiences in the context of chronic health conditions. Additional information on the procedure and participants of the ENTWINE iCohort has been published in two other articles (Morrison et al., 2022; Elayan et al., 2022).
Baseline data collection took place from August 2020 until May 2021 in the following countries: Ireland, UK, Poland, and Italy; from October 2020 to May 2021 in The Netherlands, Sweden, and Greece; and from February 2021 to August 2021 in Israel and Germany. Caregivers were recruited online via multi-language advertisements, flyers, and informative videos with the survey link placed on different social media. Online advertisements were also shared by relevant caregivers’ organizations.
Eligible caregivers were 18 years or older and provided care for a family member or a friend with a chronic health condition, disability, or any other care need (i.e., Do you provide care for a family member or a friend with a chronic health condition or disability?
Procedure
Eligible participants accessed the online information letter, provided electronic informed consent, and completed the online survey anonymously. The study was submitted for ethical approvals in all countries where the study was conducted (Morrison et al., 2022). Measures included in the survey are reported in the study protocol (Morrison et al., 2022) and baseline measures used in the current analyses are described below.
Measures
Socio-demographic variables. Self-reported caregiver age, gender, level of education, relationship status, country of residence, employment, health status, care recipient’s age, gender, type and duration of health conditions, and relationship with the care recipient. The relationship between caregivers and care recipients was re-categorized into the three most common typologies: spouses, adult children (including children in-law) and others (including parents, siblings, and friends). Caregivers were asked to complete the measures with respect to their care recipients (referred to as loved one).
Caregiving context. Caregiving context variables included: (1) the length of the caregiving period in months; (2) whether the participant was the primary caregiver; (3) the health conditions of the care recipient which were re-categorized into physical impairments, (including: cardio-vascular diseases, cancer, diabetes, kidney diseases, lung disease), neurological impairments (including: stroke, cognitive or memory impairment, mental health conditions) and other impairments/comorbidities; (4) living in the same household; (5) intensity of care (total number of hours per week spent on general caregiving tasks and on specific tasks such as household activities, personal care, practical support, and emotional support); and (6) and the ability of the care recipients to perform Activities of Daily Living (ADL) independently using the Katz Index (Katz, 1983), which demonstrates good internal consistency (Cronbach’s α = .87).
Open Communication. Open communication between caregiver and care recipient was measured by the communication subscale (8 items) of the Dyadic Coping Inventory (DCI; Bodenmann, 2005). Based on the Systemic Transactional Model of Dyadic Coping, the DCI is designed to measure dyadic coping in close relationships when one or both dyad members are stressed. For this study, we selected the communication dimension of dyadic coping, to explore how caregivers and care recipients openly communicate stress verbally and/or nonverbally to each other. One difference from the original interpersonal process model of intimacy, which commonly analyzes self and other communication behaviours of dyad members separately, was to assess caregivers’ open communication using one scale including items measuring how stress is communicated by the caregiver (4 items, e.g., I let my loved one know that I appreciate his/her practical support, advice, or help) and perceptions of how stress is communicated by the care recipient (4 items, e.g., My loved one lets me know that he/she appreciates my practical support, advice, or help). Given high correlation between the two sub-scales (r = .87) and previous research using these two subscales as one indicator of communication (Bodenmann, 2005), we chose to use it as one scale representing open communication. Responses were scored on a 5-point Likert scale from 1 (very rarely) to 5 (very often). Scores are the sum of the included items with higher scores indicating a good ability to communicate own stress to the other and positive perceptions of the other’s ability to communicate their own stress. For the current sample, the internal consistency was satisfactory (Cronbach’s α = .78).
Perceived Responsiveness. Caregivers’ perceptions of care recipient responsiveness were measured by the 12-item Perceived Partner Responsiveness Scale (PPRS; Reis et al., 2018). The PPRS measures the degree to which people feel their loved ones are responsive to them. It measures two dimensions of perceived responsiveness in close relationships: (1) understanding (7 items, e.g., My loved one gets the facts right about me; My loved one knows me well) and (2) validation (5 items, e.g., My loved one values and respects the whole package that is the real me; My loved one seems interested in what I am thinking and feeling). Responses were scored on a 9-point Likert scale ranging from 1 (not at all true) to 9 (completely true). A total score is calculated by summing of all items (Reis et al., 2018), with scores indicating greater perceptions of other’s responsiveness. Internal consistency was very strong for the current sample (Cronbach’s α = .96).
Intimacy. Caregivers’ degree of intimacy with the care recipient was measured using the Inclusion of the Other in the Self Scale (IOS; Aron et al., 1992). The IOS consists of seven pairs of circles representing the self (i.e., caregiver) and the loved one (i.e., care recipient), which are drawn to show varying levels of overlap, indicating the degree of intimacy in the relationship. The less the circles overlap, lower degrees of intimacy exist between the two; the more two circles overlap, higher degrees of intimacy are perceived. A 7-point scale is used to score the degree of overall intimacy. Convergent validity among the IOS and the Relationship Closeness Inventory and the Intimacy Scale (Aron et., 1992) demonstrate high reliability of the scale.
Burden. Caregiver burden was measured with the Short Form Zarit Burden Interview (ZBI-12; Bédard et al., 2001). The ZBI-12 has been used to evaluate burden in different caregiving contexts with a 5-point Likert scale ranging from 0 (never) to 4 (always) (e.g., Do you feel that because of the time you spend with your loved one that you don’t have enough time for yourself? Overall, how burdened do you feel in caring for your loved one?). Items were summed into a total score (ranging from 0 to 48), with higher scores indicating greater caregiver burden and distress. The internal consistency was strong (Cronbach’s α = .87)
Communal motivation to care. Communal motivation was assessed with the 10-item Partner-Specific Communal Motivation Scale (Lemay & Neal, 2013). Caregivers were asked to assess to what extent they were communally motivated to care for the wellbeing of their care recipients. Responses were scored on a 9-point Likert scale ranging from 1 (not at all) to 9 (extremely). Example items are: Helping my loved one is a high priority for me; I would sacrifice very much to help my loved one; I would be reluctant to sacrifice for my loved one. The total score is given by the sum of the items, after reversing items 2, 5, 10, and indicates higher levels of communal motivation. For the current sample, the internal consistency was strong (Cronbach’s α = .82).
Data Analysis
Statistical analyses were conducted with SPSS (version 28). Missing data were assumed to be missing at random (based on Little’s test of missing completely at random and logistic regressions for the potential predictors of missingness) and constituted less than 10% of the sample. Therefore, complete case analyses were performed (Schafer & Graham, 2002). Although scores on some scales were not normally distributed (e.g., communal motivation), parametric analyses were performed for all scales according to the central limit theorem, as consequences of violating the assumptions of normality are considered to be trivial given the large sample size. Where appropriate, bootstrapping was applied as a useful alternative to parametric estimates (Lumley et al., 2002).
Descriptive analyses were performed (i.e., means and standard deviations for continuous variables, and frequencies and percentages for categorical variables) to describe the sample. One-way analysis of variance (ANOVAs) examined group differences in open communication and perceived responsiveness between different illness contexts and different relationship types. Pearson correlations examined associations between the main variables. Identification of covariates was informed by previous research (e.g., caregivers’ and care recipients’ gender and age) and by significant associations between categorical demographic variables (e.g., relationship type, living arrangements) and continuous demographic variables (e.g., intensity of care, Katz Index) and outcome variables (see Supplementary table).
To test whether perceived responsiveness mediates the relationship between open communication (independent variable) and intimacy, burden, and communal motivation (outcome variables) three separate mediation analyses were conducted using model 4 in the PROCESS macro created by Preacher and Hayes (2007), controlling for the variables of caregivers’ and care recipients’ age, gender, living arrangements, relationship type, caregivers’ intensity of care, and care recipients’ physical impairments. Full mediation occurs if the indirect effect (path a*b, the relationship between the independent variable and the outcome variable via the mediator) is significant (the confidence interval does not cross zero), the direct effect (path c’, the relationship between the independent variable and the outcome variable) is non-significant, and the total effect (path c, the sum of the direct and indirect effect) is significant. Partial mediation occurs if the direct effect is also significant. Next, moderated mediation analyses were performed using model 21 in the PROCESS macro, to examine whether the effect of open communication on the perceived responsiveness varied based on the illness context (first moderator: physical, neurological, or other impairments/comorbidities), and whether the effect of the perceived responsiveness on intimacy, burden, and communal motivation varied based on the relationship type between caregivers and care recipients (second moderator: spouses, adult children, and others). The significance of indirect effects was examined using the bootstrap estimations for 5000 samples and 95% confidence intervals based on Preacher and Hayes’ recommendations (Preacher et al., 2007).
Results
Sample Characteristics
Sample Characteristics and Descriptive of Caregivers (N = 882).
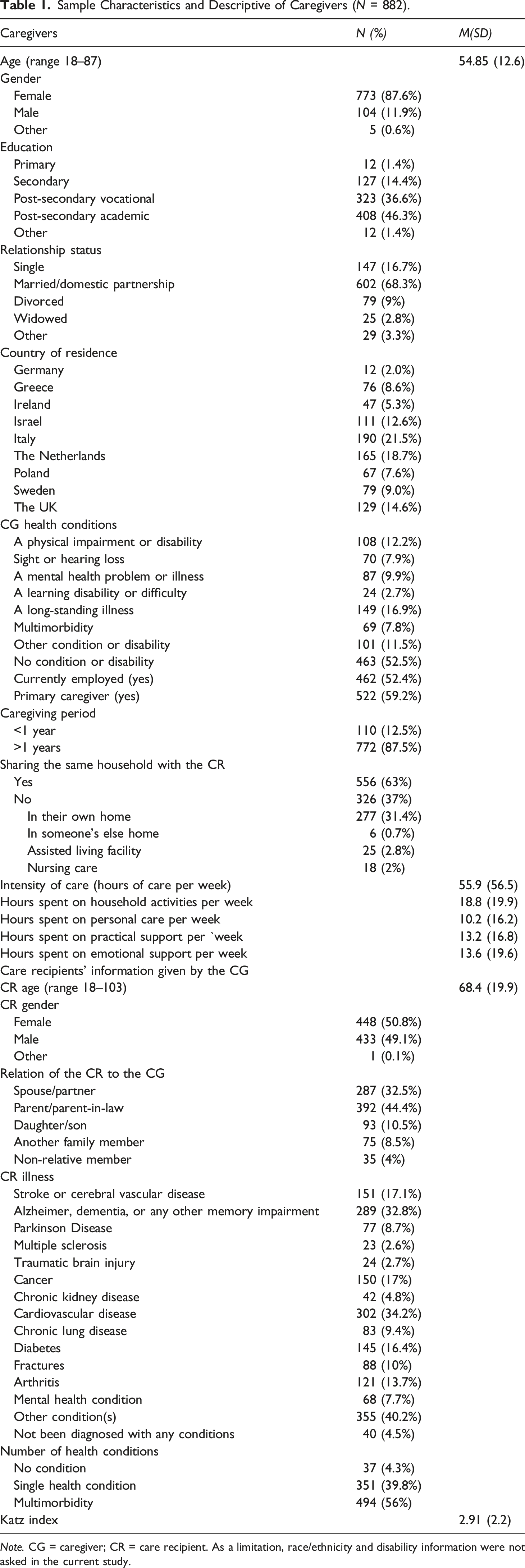
Note. CG = caregiver; CR = care recipient. As a limitation, race/ethnicity and disability information were not asked in the current study.
Intercorrelation Coefficients and Mean and Standard Deviations for Main Variables in the Study.
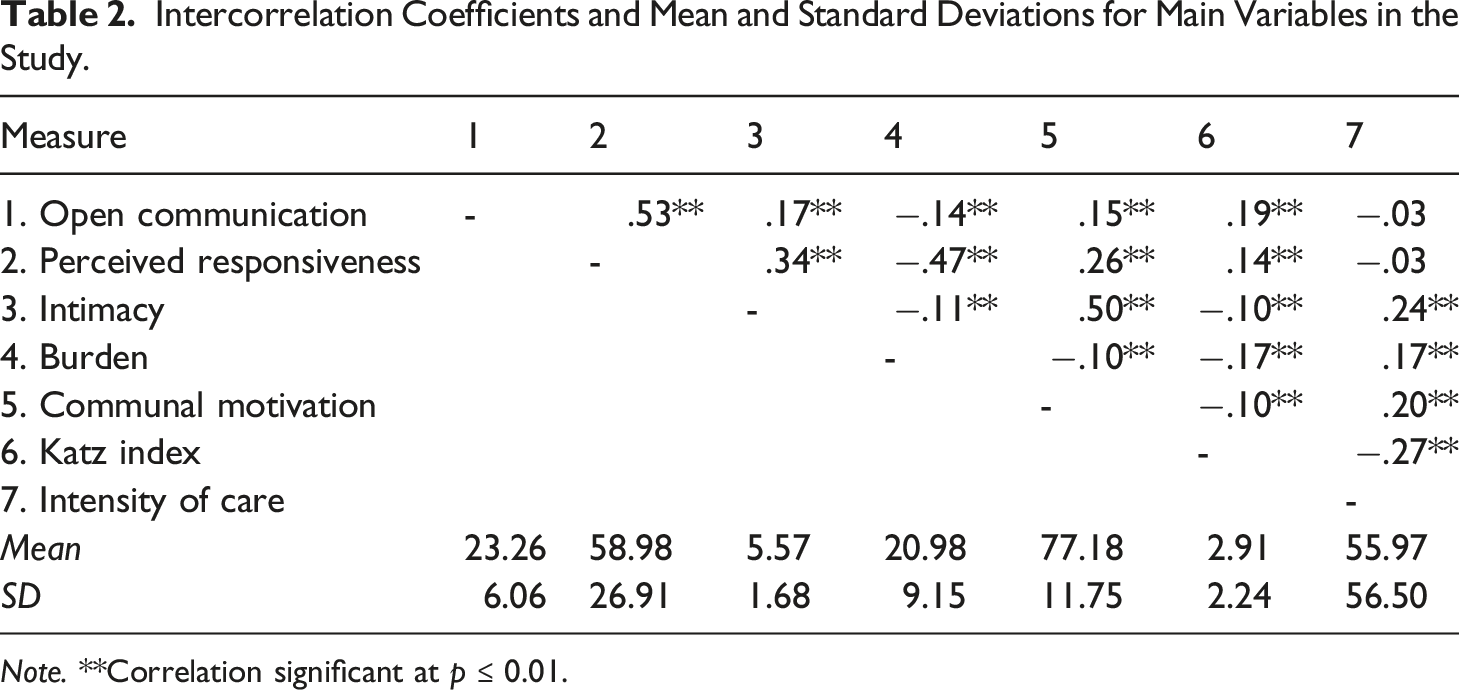
Note. **Correlation significant at p ≤ 0.01.
Group Differences in Open Communication and Perceived Responsiveness
Description of Group Differences and ANOVAs’ Tests.
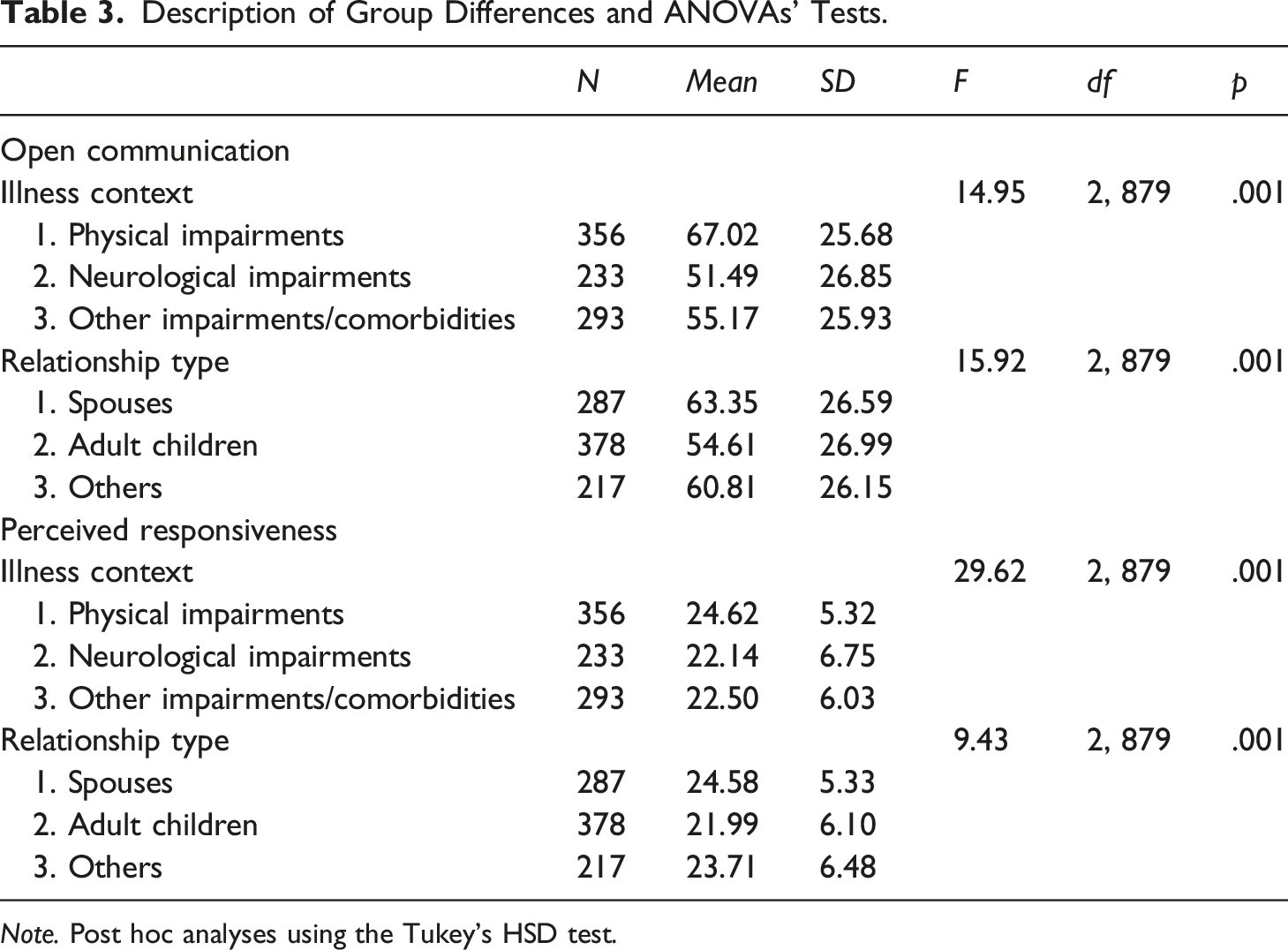
Note. Post hoc analyses using the Tukey’s HSD test.
Mediation Analyses
Results of Mediation Effects of Caregivers’ Perceptions of Care Recipients’ Responsiveness on Intimacy, Burden and Communal Motivation.
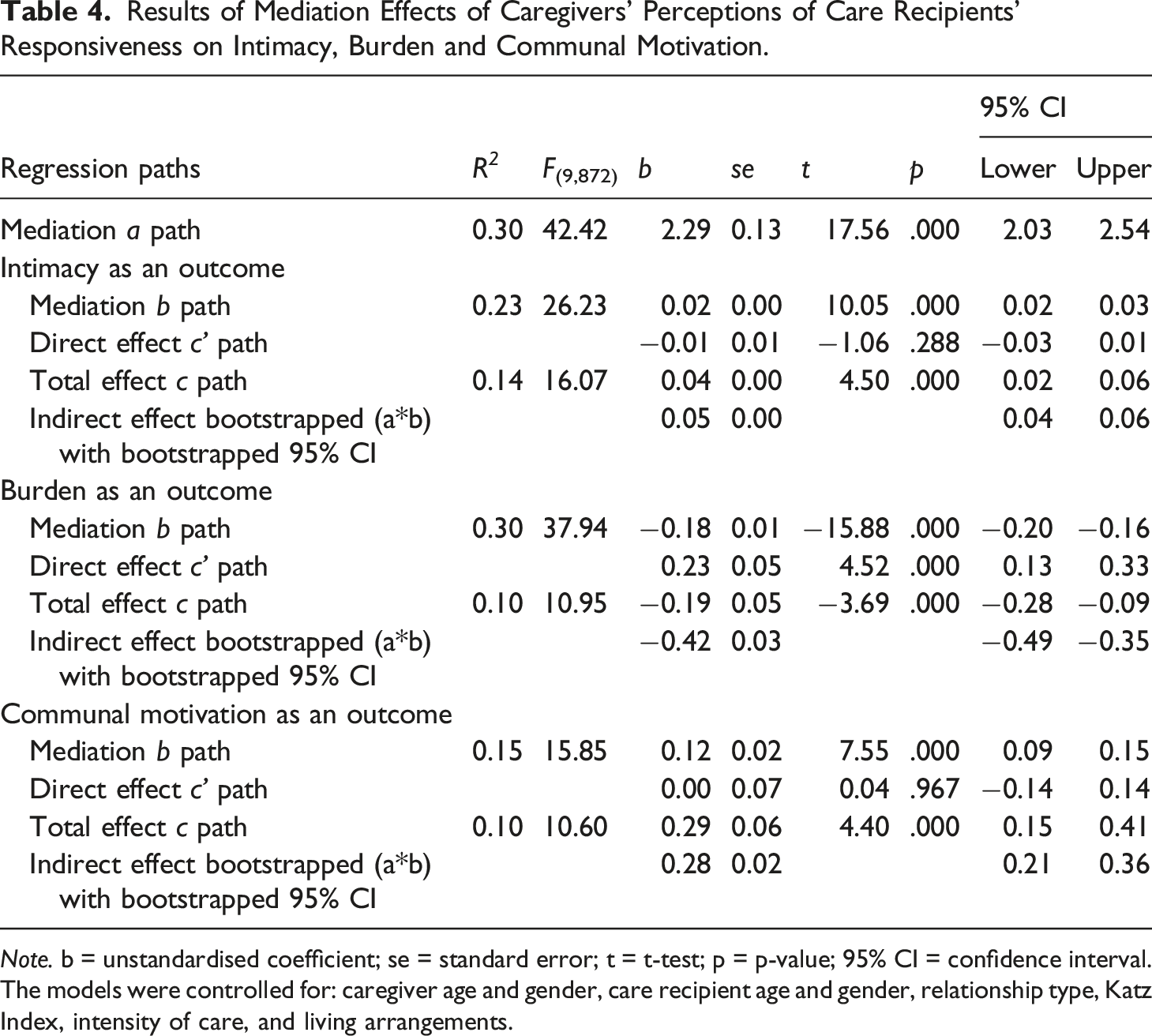
Note. b = unstandardised coefficient; se = standard error; t = t-test; p = p-value; 95% CI = confidence interval.
The models were controlled for: caregiver age and gender, care recipient age and gender, relationship type, Katz Index, intensity of care, and living arrangements.
Moderated mediation analyses
Results of Moderated Mediation Effects of Care Recipients’ Health Condition on Caregivers’ Perceptions of Care Recipients’ Responsiveness and of Relationship Type on Intimacy, Burden and Communal Motivation.
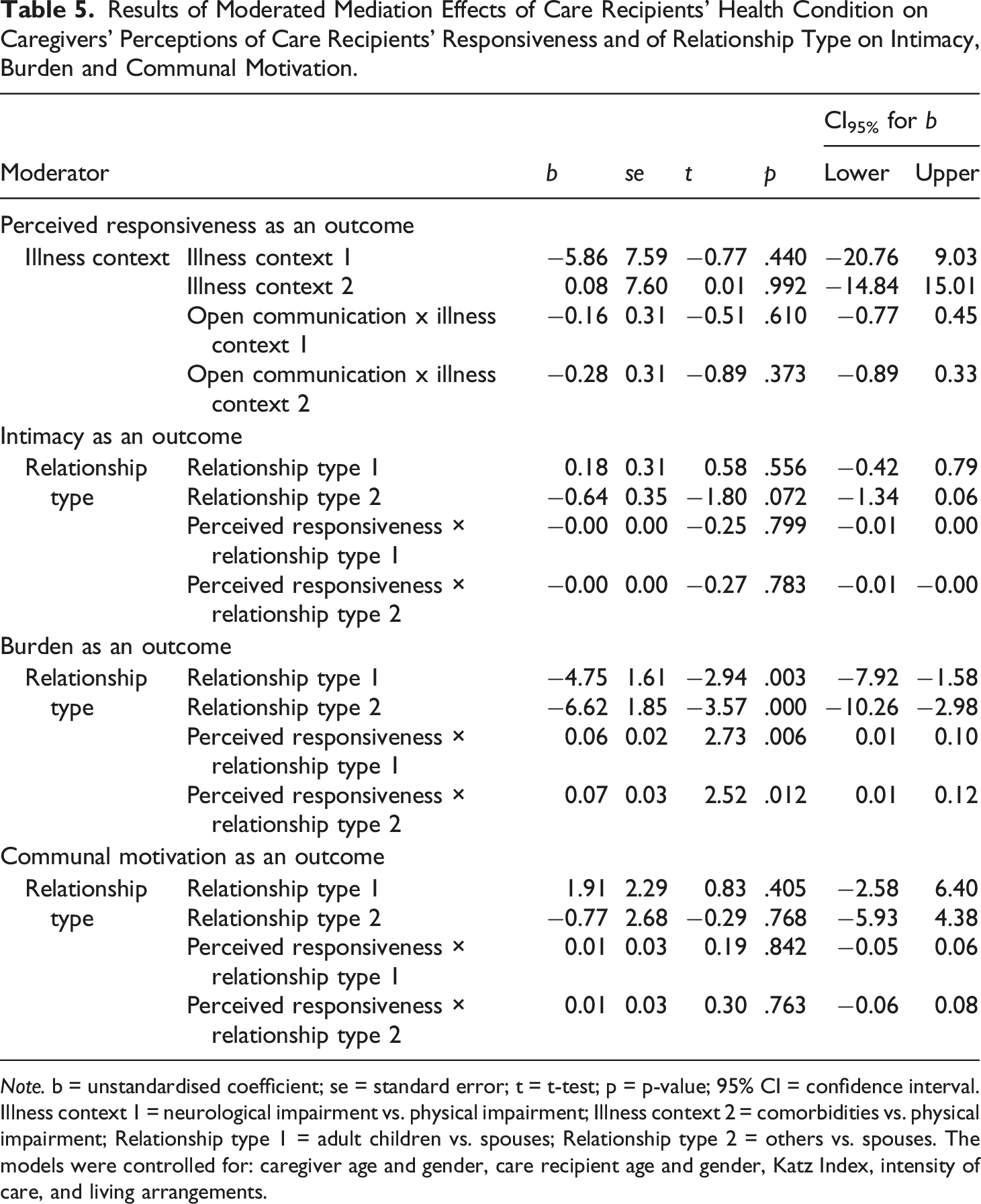
Note. b = unstandardised coefficient; se = standard error; t = t-test; p = p-value; 95% CI = confidence interval. Illness context 1 = neurological impairment vs. physical impairment; Illness context 2 = comorbidities vs. physical impairment; Relationship type 1 = adult children vs. spouses; Relationship type 2 = others vs. spouses. The models were controlled for: caregiver age and gender, care recipient age and gender, Katz Index, intensity of care, and living arrangements.
Discussion
The current study showed that, although there were differences in caregivers’ interpersonal processes with care recipients (i.e., levels of open communication and perceived responsiveness) depending on the illness contexts and relationship types, associations between open communication, perceived responsiveness, and both caregivers’ relational (i.e., intimacy) and psychological wellbeing (i.e., burden and communal motivation to care) were confirmed in the different illness contexts and caregiving relationship types.
The current study offers two important suggestions for better understanding these complex associations. Firstly, results support previous findings (Reis & Shaver, 1988; Manne et al., 2004) on perceptions of partner responsiveness as a key mediator component of effective communication. Additionally, perceived responsiveness might constitute a basis for the maintenance and development of both caregivers’ relational and psychological wellbeing. In line with the interpersonal process model of intimacy, when caregivers’ - care recipients’ open communication was met with care recipients’ understanding and validating responses (i.e., perceived responsiveness), caregivers reported higher intimacy with the care recipient, less burden, and higher communal motivation to care. In line with wider research, caregivers report greater wellbeing when caregiving is valued and acknowledged by the care recipient, the whole family, and broader society (Ransmayr, 2021). Even when a care recipient is ill and unable to reciprocate with tangible support, there is evidence that perceptions of being supported, acknowledged, and validated by care recipients, are of importance in terms of relationship satisfaction and positive aspects of caring role (Kuijer et al., 2001; Ybema et al., 2001).
Secondly, our findings suggest that, despite caregivers of care recipients with neurological impairments reporting lower levels of open communication and perceiving care recipients as less responsive than care recipients with physical impairments, perceived responsiveness remained a crucial pathway through which open communication might be related to the caregivers’ overall wellbeing. High-quality communication with the care recipient might still be a desired need for different caregivers (Fried et al., 2005). This is in line with existing literature highlighting the crucial role of communication and other dyadic coping behaviours in advanced neurological diseases (Bannon et al., 2022).
Thirdly, no moderating effect of relationship type was detected between perceived responsiveness and intimacy and between perceived responsiveness and communal motivation to care. Only the negative relationship between perceived responsiveness and burden was found to be stronger for spouses than for adult children and other caregivers. Perhaps, given research suggesting spousal caregivers are the most burdened caregiving group (Oldenkamp et al., 2016), spousal caregivers might benefit more by perceiving their partners as more responsive. Perceived responsiveness reflects a sense of partnership and togetherness that is typical of spousal relationships (Laurenceau et al., 2005). In our study, caregiving spouses and other relatives reported higher levels of open communication and higher care recipients’ responsiveness than adult children. Interactions between dyad members might depend on the family/dyad-specific patterns of communication (Herbst et al., 2020). In spousal relationships, often characterized by mutual noncontingent responsiveness to needs, people tend to express themselves and their vulnerabilities more (Clark & Finkel, 2005), and engage in more frequent interactions given they are more likely living with care recipients (Pinquart & Sörensen, 2011). In filial caregiving relationships, there may be less tendency to share thoughts and feelings resulting in limited open communication (Fenton et al., 2022). Furthermore, 37% of caregivers in our sample did not live in the same household as the care recipient, meaning they may have less frequent interactions. In any case, despite differences in interpersonal processes between spousal and filial caregiving relationships, validity of the interpersonal process model of intimacy was confirmed in each relationship type. This adds to the existing literature suggesting the model may be generalizable to dyads other than spouses. Moreover, interventions targeting interpersonal processes such as communication and perceived responsiveness might be particularly beneficial for spouses but still important for adult child and other caregivers (Khalifian & Barry, 2020).
Additionally, our study opens avenues for many novel questions about interpersonal processes in the caregiving context. First, few studies have examined adult children or other non-spousal caregivers’ interpersonal processes compared with spousal caregivers (Ferraris et al., 2022), therefore more research on caregiving dyads other than spouses is needed. Moreover, communication processes should be investigated further in association with other wellbeing outcomes such as burden, preparedness, and motivation for caregiving (Fenton et al., 2022; Fried et al., 2005; Otto et al., 2021). Caregiver - care recipient communication has not been examined linked to caregiver burden, although it appears to be a promising area for research in light of existing results (Otto et al., 2021). Moreover, our findings suggest the more caregivers perceive care recipient responsiveness, the more they might be communally motivated to provide care. Further dyadic examination of communal motivation will shed light on the reciprocal benefits of communal care among caregivers and care recipients (Mills et al., 2004). Perceived responsiveness can develop from the accumulation of repeated interactions over time, therefore longitudinal research and intensive longitudinal designs (i.e., diary studies) might be optimal to broaden our knowledge of this concept (Laurenceau et al., 2005). Lastly but importantly, future research can extend our findings from a methodological point of view by conducting dyadic designs including both caregivers and care recipients.
Our study has important clinical implications. Existing dyadic interventions developed for spouses to reduce emotional distress and preserve relationship intimacy (Braun et al., 2010; Poon, 2019) could be adapted to promote positive outcomes (e.g., psychological wellbeing) for a diverse range of illness contexts and caregiving relationships (e.g., non-spousal relationships). Findings suggest a valuable opportunity to involve both dyad members, regardless of relationship type, in psychosocial programs seeking to increase relational and psychological wellbeing by reducing burden and stimulating motivation to care. Such psychosocial programs could target improvements in caregivers’ interpersonal processes with care recipients (open communication about individual and shared stressors and perceptions of responsiveness) also in situations where communication is impaired, like dementia (Poon, 2019).
One major strength of this study is its large, multinational and heterogeneous sample of caregivers. Recruiting caregivers from nine countries with differing long-term care systems and cultural norms and beliefs around informal care is an added value to enhance the generalizability of the results. Another strength is that we controlled for potential covariates (i.e., socio-demographics) increasing the validity of findings. Moreover, this study represents an important step forward in testing and expanding the intimacy model in the caregiving context.
In addition to these strengths, our study should be interpreted in light of some limitations. First, we only included caregivers in our study, however the interpersonal components of the psychological processes we investigated could have benefitted from also including the care recipients’ perspective. Difficulties in recruiting dyads, especially when one dyad member is seriously ill, is acknowledged in the dyadic literature (Dagan & Hagedoorn, 2014). The cross-sectional design limits conclusions about directionality of effects. Finally, females were overrepresented in our sample (87.6%), although best efforts were made to recruit diverse samples in order to capture the caregiving experiences of participants with different characteristics and care situations. However, this is consistent with the existing caregiving literature identifying women as the predominant caregiving group (Colombo et al., 2011).
Conclusion
This study provided empirical support for the interpersonal process model of intimacy. Open communication and perceived responsiveness are fundamental components of the intimacy process and an important step in the prevention of burden and lack of communal motivation to care among caregivers, either spouses, adult children, or other family members or friends taking care of care recipients with neurological or physical impairments. As such, the interpersonal process model could be used as a valuable guide to understand and to tailor psychosocial interventions targeted to caregivers’ relational and psychological wellbeing in many caregiving contexts and relationships.
Supplemental Material
Supplemental Material - The interpersonal process model of intimacy, burden and communal motivation to care in a multinational group of informal caregivers
Supplemental Material for The interpersonal process model of intimacy, burden and communal motivation to care in a multinational group of informal caregivers by Giulia Ferraris, Eva Bei, Chelsea Coumoundouros, Joanne Woodford, Emanuela Saita, Robbert Sanderman, and Mariët Hagedoorn in Journal of Social and Personal Relationships
Footnotes
Acknowledgements
We gratefully acknowledge “ENTWINE Informal Care”.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Union’s Horizon 2020 research and innovation programme under the Marie Skłodowska-Curie grant agreement No 814072.
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.