
Abstract
Our study aims to understand the impact of the Coronavirus Disease of 2019 (COVID-19) pandemic on mental health of individuals with vision impairment and to highlight the unique challenges faced due to social isolation and disruption in healthcare services. The study design is a systematic review and meta-analysis. A literature search was conducted using MEDLINE, EMBASE, and CINAHL databases. A total of 363 articles were screened, 18 studies were included for qualitative analysis and 12 were used for quantitative analysis. After screening, a risk of bias assessment was carried out. Data were extracted and a meta-analysis was performed using STATA 14.0. Fixed-effect and random-effect models were computed based on heterogeneity. Our meta-analysis encompassed 16 studies investigating the psychological impact of COVID-19 in 2317 vision loss patients. The meta-analysis indicated significant levels of loneliness (44%, 95% confidence interval [CI] = [0.24 to 0.64]); anxiety (45%, 95% CI = [–0.31 to 1.21]); depression (48% CI = [–0.05 to 1.01]); fear of vision loss (42% mild, 95% CI = [0.24 to 0.61]); fear of contracting COVID-19 (61%, 95% CI = [0.45 to 0.77]); and psychiatric disorders (28%, 95% CI = [0.07 to 0.50]) for patients with vision impairment. Vision loss patients experienced significant levels of loneliness, anxiety, depression, fear of vision loss, fear of contracting COVID-19, and psychiatric disorders during the pandemic. This psychological distress is attributable to poor access to health care, a lack of social support, and difficulties adhering to pandemic-related precautions such as physical distancing and avoiding contaminated surfaces.
Introduction
The Coronavirus Disease of 2019 (COVID-19) pandemic has significantly impacted both the physical and mental health of individuals worldwide (Tsamakis et al., 2021). Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) primarily causes respiratory symptoms such as cough and fever (Zhu et al., 2020). However, in severe instances, it can cause organ failure and death (Huang et al., 2020; Zhu et al., 2020). During the pandemic, a major concern for vision loss patients was the risk of COVID-19 infection. Patients with vision loss may have comorbid systemic or autoimmune conditions, which make them immunocompromised and susceptible to COVID-19 (Brewerton et al., 1973; Corse et al., 2020; Durrani et al., 2004; Foster et al., 1984; Herbort et al., 2009). In addition, many of these patients are older due to the prevalence of eye conditions such as age-related macular degeneration or glaucoma in that age group (Klein et al., 2011; Quigley & Broman, 2006). As a result, visually impaired patients are often at an increased risk of severe COVID-19 complications (Centers for Disease Control and Prevention, 2020). Fear of infection can lead to heightened anxiety and depression, which negatively impacts the overall well-being of these individuals (Serafini et al., 2020).
It is imperative to recognize the psychological effects of the COVID-19 pandemic on vision loss patients. It is well established that eye conditions can negatively influence mental health, leading to issues such as anxiety, depression, and sleep disturbances (Cimarolli et al., 2016; Sabel et al., 2018; van der Aa et al., 2015; Zheng et al., 2013). The social isolation caused by the pandemic has only worsened mental health issues for this population (Serafini et al., 2020). COVID-19 lockdown and quarantine measures has impacted the mental well-being of children, adults, and healthcare professionals (Brooks et al., 2020; McGinty et al., 2020; Razai et al., 2020). For vision loss patients, the measures implemented to stop the spread of the virus have led to significant social isolation and a diminished support network (Hwang et al., 2020).
During the COVID-19 pandemic, visually impaired patients faced significant disruptions in healthcare services (Pietrabissa & Simpson, 2020). A study showed an 81% decrease in patient volume for ophthalmological services during the months of April and March 2020, due to the lockdown (Strata Decision Technology, 2020). Following the implementation of clinic changes related to COVID-19, a study observed a fourfold reduction in patient encounters within their ophthalmology clinic (Berkenstock et al., 2021). Similarly, another study reported that while 82% of patients completed their scheduled visits before the pandemic, only 59.3% did so during COVID-19 (Brant et al., 2021). Many hospitals and clinics reduced or canceled non-emergency appointments to prioritize COVID-19 patients and reduce the spread of infection (Syriga et al., 2021). However, these decisions are not without consequences, as delays in essential eye care can lead to a deterioration of one’s eye condition and a decrease in quality of life (Leung et al., 2022). This disruption of healthcare services also led to increased anxiety and stress for eye disease patients, as they felt uncertain about their ability to access necessary care (Dar et al., 2021). Studies have shown that fear of blindness and loss of quality of life are major concerns for individuals with eye diseases (Scott et al., 2016).
Healthcare professionals and policymakers should recognize and address the emotional challenges experienced by eye disease during the pandemic. This meta-analysis hopes to provide a comprehensive understanding of the psychological effects of COVID-19 on vision loss patients, supplying crucial information for healthcare professionals, policymakers, and researchers. Such insights could guide interventions and policies to support the well-being of vision loss patients during future pandemics.
Methods
Search strategy
This protocol adheres to the preferred reporting items for systematic reviews and meta-analysis (PRISMA) guidelines. The PRISMA checklist can be found in Appendix I. The search for eligible studies was conducted across MEDLINE, EMBASE, and CINAHL databases, covering all available records up to 24 August 2022. The search strategy is detailed in Appendix II. Gray literature was obtained from sources such as ProQuest Dissertations, and Theses Global and ClinicalTrials.gov. Conference proceedings from Canadian Ophthalmological Society, American Academy of Ophthalmology, and The Association for Research in Vision and Ophthalmology were reviewed for relevant poster presentations and abstracts.
Inclusion criteria
The studies included in the protocol met the following criteria: they focused on human subjects 18 years or older with vision loss, regardless of the cause. The primary focus of the review was to evaluate the psychological effects of COVID-19 on individuals with vision loss, specifically looking at measures such as anxiety, depression, and stress. The review considered the inclusion of randomized control trials, clinical trials, multicenter studies, economic studies, observational studies, cohort studies, comparative studies, and case series.
Exclusion criteria
The studies excluded from the protocol include systematic reviews, meta-analyses, review articles, case reports, commentaries, and letters to the editor. However, conference abstracts were considered as long as sufficient details and data were provided. Only studies found in English were included. There were no limitations on the publication year or location of the studies.
Study selection
Studies were selected based on a two-tier system consisting of title/abstract screening and full-text screening. Each tier was performed by two independent verifiers (E.T. and M.A.), with disagreements between study selection resolved at a joint meeting. The PRISMA flowchart (see Figure 1) outlines the studies that were included/excluded at each phase of the screening process.
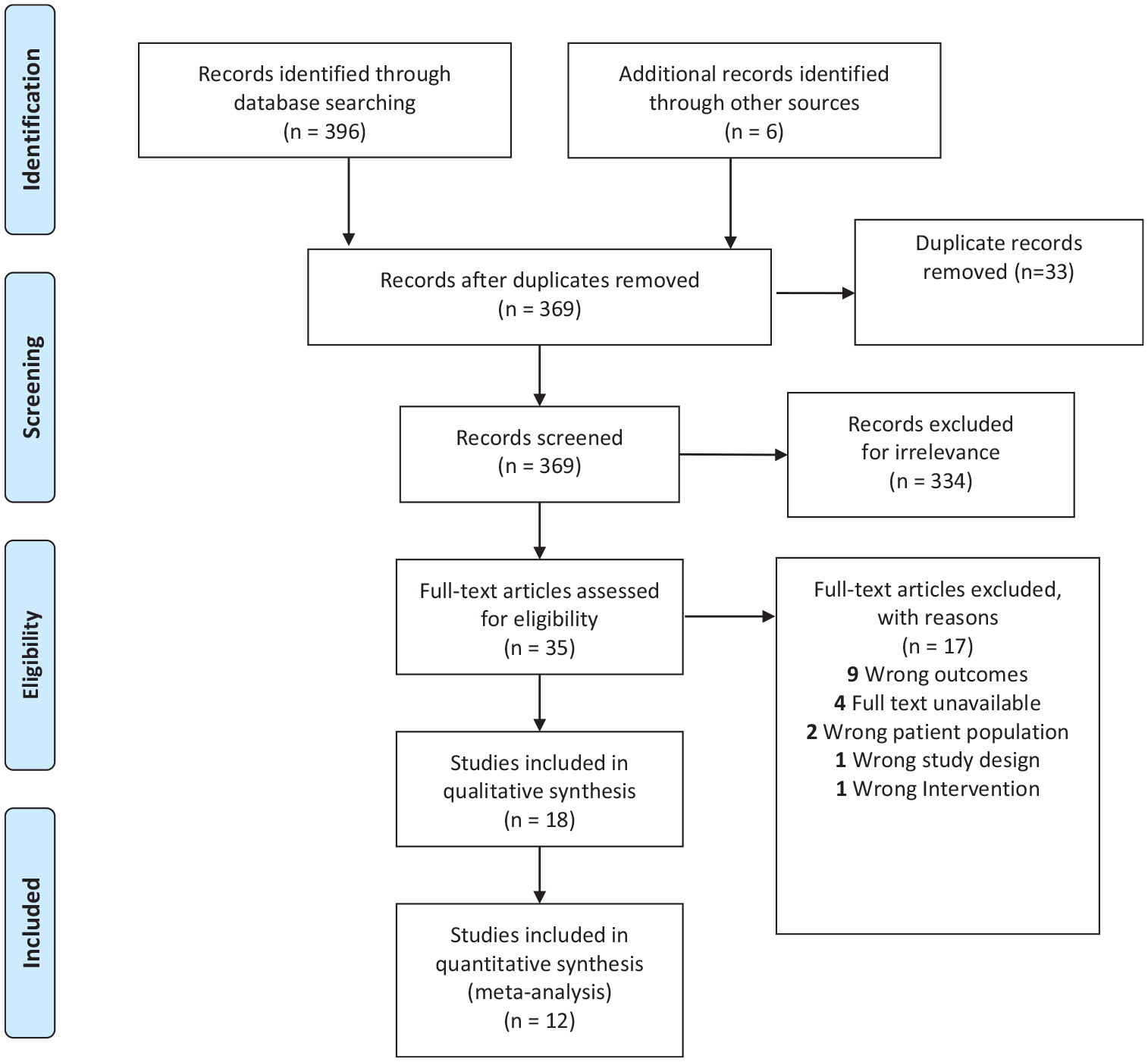
PRISMA flowchart illustrates the systematic review, including database searches, the number of abstracts screened, the evaluation of full-text articles for study eligibility, and the reasons for exclusion.
Risk of bias
Potential bias within the studies was assessed using a modified version of the Downs and Black (1998). Based on their scores, the studies were grouped into three categories: high quality for scores above 20, medium quality for scores ranging from 16 to 19, and low quality for scores below 15. A quality control check was conducted to ensure methodological accuracy and comprehensiveness. Due to the limited amount of evidence, studies categorized as low quality were not disregarded in the analysis. Detailed information on the bias risk evaluation is contained in Appendix III.
Data collection process
Following the quality-check process, we extracted the study characteristics of 12 articles (see Table 1). These details include the author, publication year, research methodology, study location, eye disease under investigation, as well as psychological outcomes such as concerns about vision loss, feelings of isolation, anxiety, depression, fear of COVID-19 infection, and the occurrence of mental health conditions. We looked at psychiatric disorders including bipolar disease and dementia. A total of 12 articles were used for quantitative synthesis and 18 for qualitative analysis.
Summary of included studies’ characteristics.
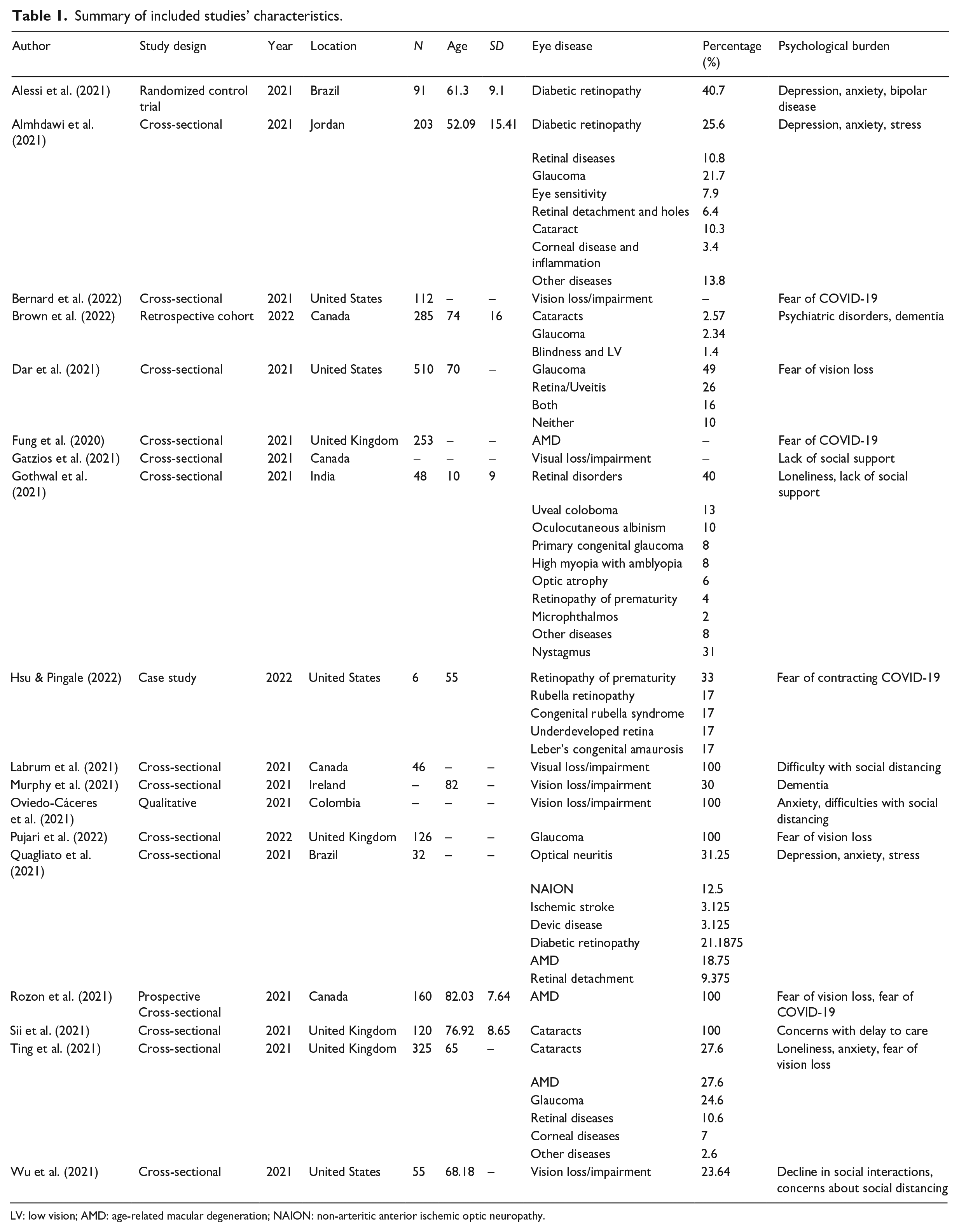
LV: low vision; AMD: age-related macular degeneration; NAION: non-arteritic anterior ischemic optic neuropathy.
Main outcome
The primary outcome assessed by data extraction was to quantify the psychological impact of the COVID-19 pandemic on patients suffering from vision loss. The prevalence of mental illnesses such as anxiety, depression, and other psychiatric disorders was analyzed. More general metrics such as loneliness and fear of both vision loss and contracting COVID-19 were also assessed.
Statistical analysis
The meta-analysis utilized STATA 15.0 software (STATA Corporation, College Station, TX) for data analysis. The effect size (ES) or treatment effect was represented by the proportion. To assess the heterogeneity among the studies, the I2 value was employed, indicating the proportion of variation across studies attributed to heterogeneity rather than chance. The chi-square test was used to determine whether the observed differences between studies were likely due to chance alone. The presence of heterogeneity was indicated by a low p-value and a large chi-square statistic in relation to its degree of freedom. Depending on the level of heterogeneity, fixed-effect or random-effect models were utilized. Forest plots and funnel plots were generated to visually present the results and evaluate for potential publication bias.
Results
Search results
The database search identified 396 articles, including 33 duplicates, which were subsequently removed, and the remaining 369 articles were screened. After the two independent verifiers (E.T. and M.A.) completed abstract and title screening, 35 articles proceeded to full-text screening. Of the 18 articles that proceeded to data extraction, 12 were included in the meta-analysis. The other six articles provided data not synonymous with other studies or were qualitative studies. Cohen’s kappa (κ) coefficient for the abstract and title screening and full-text screening were 37% and 8%, respectively, suggesting a moderate level of agreement between screeners.
Study characteristics
Table 1 details the demographic characteristics of the 18 eligible studies included in the review. The majority of studies were cross-sectional studies (n = 16), whereas the rest were randomized controlled trials, qualitative studies, retrospective cohort studies, and case studies. The locations of the studies spanned globally, including Brazil, Colombia, and Jordan. However, there was a high prevalence of high-income countries such as the United Kingdom, the United States, and Canada. Therefore, the generalizability of the findings of this review is limited in the case of low-income countries, specifically vision loss patients in low-income countries may lack social support and have specific experiences not currently captured. Selected studies consisted of a total of 4656 patients. The most common eye diseases that were investigated were vision loss or impairment (n = 10), glaucoma (n = 6), cataracts (n = 4), and diabetic retinopathy (n = 3). Several studies did not detail the cause of vision loss or impairment diagnosis.
Assessment of study quality and publication bias
Based on the Modified Downs and Black Checklist (Downs & Black, 1998), the majority of studies (n = 17) obtained a score of 15 or higher, indicating “fair” or “good” quality. A smaller subset of studies (n = 4) achieved a score ranging from 11 to 14, indicating poor quality. Despite the lower quality of these articles, they were not excluded from the analysis due to limited availability of evidence. It should be noted that funnel plot asymmetry does not necessarily imply publication bias as there could be other plausible explanations. Appendix III provides comprehensive information regarding the assessment of risk of bias and potential publication bias.
Impact of loneliness
The forest plot, Figure 2(a), indicates significant heterogeneity between studies examining the impact of loneliness (I2 = 93.8%, p = .000). Studies reported significant rates of loneliness (ES = 0.44, 95% confidence interval [CI] = [0.24, 0.64]) among vision loss patients during the COVID-19 pandemic. Therefore, our results indicate that rates of loneliness among vision loss patients could be higher during the COVID-19 pandemic.
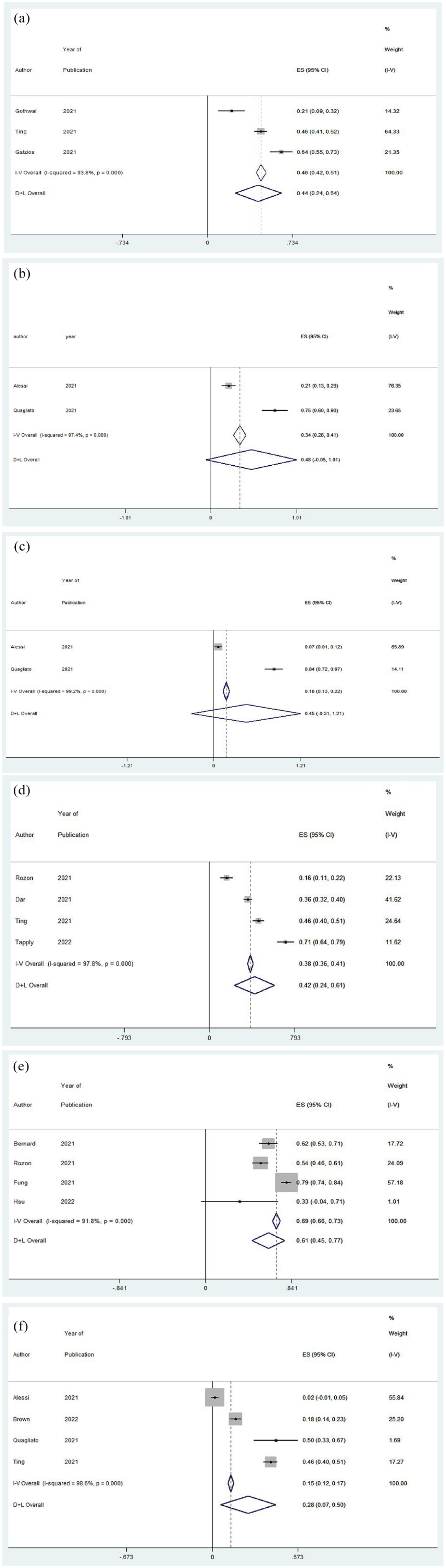
Forest plots for effect size (ES) of the percentage of vision loss patients experiencing (a) loneliness, (b) depression, (c) anxiety, (d) concerns about vision loss, (e) fear of contracting COVID-19, and (f) psychiatric disorders during the COVID-19 pandemic. Positive ES denotes that vision loss patients are experiencing that specified psychological effect.
Impact of anxiety
Figure 2(b) shows the forest plot for the studies evaluating anxiety among vision loss patients during the pandemic. There was significant heterogeneity between studies examining the impact of anxiety (I2 = 99.2%, p = .000). Studies reported significant rates of anxiety (ES = 0.45, 95% CI = [–0.31, 1.21]) among vision loss patients during the COVID-19 pandemic. Given two studies investigated anxiety, more good quality studies are required to make strong conclusions.
Impact of depression
The forest plot, Figure 2(c), shows the forest plot of prevalence of depression in vision loss patients during the COVID-19 pandemic. There was significant heterogeneity between studies examining the impact of depression (I2 = 97.4%, p = .000). Studies reported significant rates of depression (ES = 0.48, 95% CI = [–0.05, 1.01]) among vision loss patients during the COVID-19 pandemic. Because two studies investigated loneliness, more studies are required to draw definitive conclusions.
Impact of fear of vision loss
Figure 2(d) shows the forest plot for the fear of vision loss among vision loss patients during the COVID-19 pandemic. There was significant heterogeneity between studies examining the fear of vision loss (I2 = 97.8%, p = .000). Studies reported significant fear of vision loss (ES = 0.42, 95% CI = [0.24, 0.61]) among vision loss patients during the COVID-19 pandemic. Our results indicate that vision loss patients had an increased fear of vision loss during the COVID-19 pandemic.
Impact of fear of contracting COVID-19
Figure 2(e) demonstrates that there was significant heterogeneity between studies examining the fear of contracting COVID-19 (I2 = 91.8%, p = .000). Studies reported significant fear of COVID-19 (ES = 0.61, 95% CI = [0.45, 0.77]) among vision loss patients during the COVID-19 pandemic. Our results indicate that vision loss patients had an increased fear of contracting the COVID-19 pandemic.
Impact of psychiatric disorders
Figure 2(f) shows the forest plot for the prevalence of psychiatric disorders on vision loss patients during the COVID-19 pandemic. There was significant heterogeneity between studies examining the prevalence of psychiatric disorders (I2 = 98.6%, p = .000). Studies reported a significant prevalence of psychiatric disorders (ES = 0.28, 95% CI = [0.07, 0.50]) among vision loss patients during the COVID-19 pandemic. Our results indicate an increased prevalence of psychiatric disorders such as schizophrenia or bipolar disease for vision loss patients during the COVID-19 pandemic.
Publication bias
Figure 3 depicts funnel plots examining various factors among the included studies: (a) loneliness, (b) depression, (c) anxiety, (d) concerns about vision loss, (e) fear of contracting COVID-19, and (f) psychiatric disorders in vision loss patients during the COVID-19 pandemic. The scatter of studies on the plot extends from the top left to the bottom right. The funnel plot exhibits a smaller number of studies at the bottom, suggesting that smaller studies with non-significant results may not have been published. Upon visual examination, no asymmetry was detected in the funnel plot.
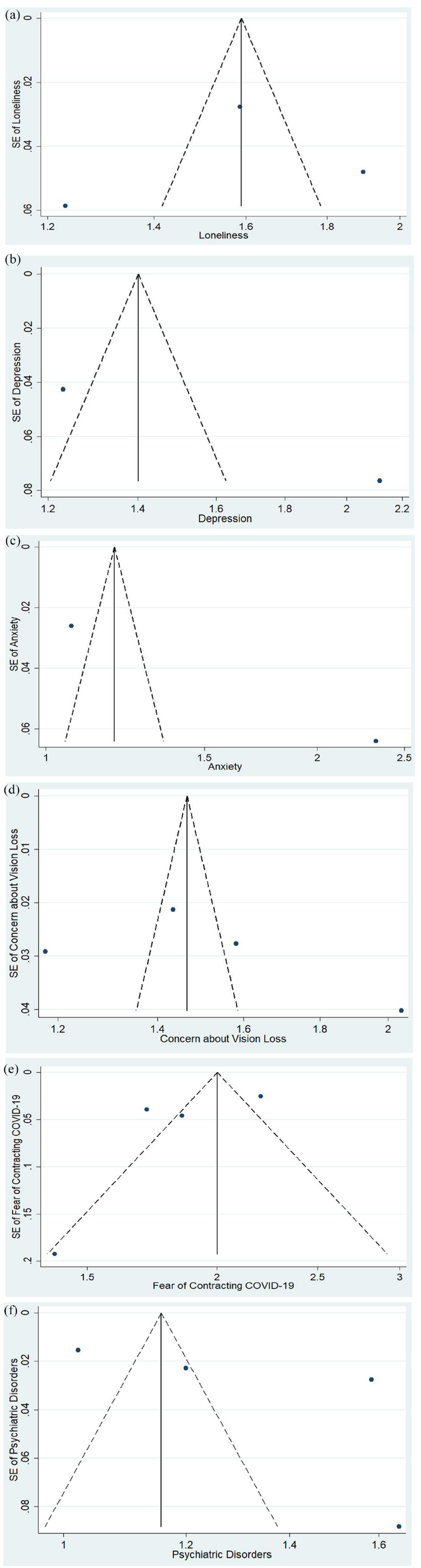
Funnel plots for the included studies evaluating (a) loneliness, (b) depression, (c) anxiety, (d) concerns about vision loss, (e) fear of contracting COVID-19, and (f) psychiatric disorders among vision loss patients during COVID-19 pandemic.
Discussion
Our systematic review and meta-analysis encompassed 16 studies investigating the psychological impact of COVID-19 in 2317 vision loss patients. Our meta-analysis indicated increased high rates of depression, anxiety, loneliness, and psychiatric disorders among vision loss patients during the pandemic. We also found high rates of fear regarding vision loss and fear of contracting COVID-19. These findings emphasize the importance of addressing the psychological effects of vision loss, particularly during the COVID-19 pandemic, and develop policies that properly accommodate for vision loss patients.
Among the general population, the COVID-19 pandemic has led to relatively high rates of mental health issues across various countries. These include symptoms of anxiety, depression, post-traumatic stress disorder (PTSD), psychological distress, and stress. Specifically, anxiety rates ranged from 6.33% to 50.9%, depression from 14.6% to 48.3%, PTSD from 7% to 53.8%, psychological distress from 34.43% to 38%, and stress from 8.1% to 81.9%; this was reported in studies conducted in China, Spain, Italy, Iran, the United States, Turkey, Nepal, and Denmark during the pandemic (MacDonald et al., 2021; Wang, Kala, & Jafar, 2020; Wang, Pan, et al., 2020) COVID-19 pandemic has led to widespread mental and physical health challenges in the general population due to factors such as prolonged social isolation, economic downturn, and fear of contracting the virus (Holmes et al., 2020; Nicola et al., 2020; Pfefferbaum & North, 2020; Pujari et al., 2022; Rajkumar, 2020). Given the high incidence of mental health challenges, such as depression, anxiety, loneliness and psychiatric disorders, in vision loss patients, there are valid concerns that this vulnerable population was harshly affected by the COVID-19 pandemic.
The disruption of healthcare services during the pandemic had a significant impact on patients with vision loss. This was particularly pronounced in ophthalmology, which was disproportionately affected by regulations intended to prevent the virus’s spread (Quagliato et al., 2021). Many ophthalmology clinics have to close or reduce their services, hindering patients’ access to routine eye exams and treatments (Rozon et al., 2021). For individuals already struggling with visual impairments, this added stressors only amplified the fear of vision loss. During the first 2 months of the pandemic, a study showed significant decreases in ophthalmological procedures across Europe: 85%–100% in cataract surgery, 57%–100% in glaucoma treatment, 50%–90% in retinal detachment treatment, 35%–90% in intravitreal injections, 63%–100% in corneal transplants, and 60% in emergency eye care (Sii et al., 2021). This disruption can be explained by the need to prioritize other medical emergencies, the challenges with accessing hospitals, and the fear of nosocomial infections. Due to the physical nature of eye exams, many ophthalmic services cannot be substituted with online consultations (Ting et al., 2021). Less frequent appointments can lead to delayed diagnosis and treatment, which can lead to further vision loss (56). Postponing eye care treatment for 2 days up to 5.5 years could result in a permanent vision loss for 72% of individuals (Holmes et al., 2020; Nicola et al., 2020; Pfefferbaum & North, 2020). The fear of vision loss from limited eye care may have increased the prevalence of mental health issues, especially depression and anxiety, among these patients.
Another challenged faced by vision loss patients during the COVID-19 pandemic was the lack of support from caregivers. Due to social distancing, they were unable to receive support, which not only reduced their emotional well-being but also impacted their autonomy (Senjam, 2020). Many with vision loss depend on caregivers for daily activities such as navigating spaces, using public transport, and shopping (Gombas & Csakvari, 2021). However, due to COVID-19 concerns, they often sought less assistance, leading to increased isolation and limited access to essential services (Gombas & Csakvari, 2021). The lack of available caregivers can lead to increased social isolation and poor access essential services (Wu et al., 2021). This issue likely contributed to the increased rates of depression, anxiety, and loneliness among vision loss patients.
Amid the global pandemic, the fear of COVID-19 infection has become a widespread and pressing anxiety for many. A major concern for visually impaired patients is the fear of touching contaminated surfaces. They depend on their tactile senses to navigate their environment and might struggle to identify clean surfaces (Wu, 2020). This fear can lead to increased anxiety and a reluctance to leave their homes, which significantly impacts their mental well-being (Murphy et al., 2021).
A study examining people with vision impairment during the pandemic revealed that the negative effects of lockdown could be mitigated. Recommendations included connecting with loved ones online, exercising at home, and purchasing essential items online (Rajkumar, 2020). Technological solutions were also suggested to help with mobility such as smartphone apps or sonar equipped canes (60). Policies for future pandemics should prioritize tailored mental health support for vision-impaired patients, embrace telehealth and other remote care models, integrate assistive technology into clinical practice, ensure accessible healthcare, and foster community-based support networks to enhance their well-being and independence.
Overall, the COVID-19 pandemic has presented unique challenges for vision loss patients. The fear of touching contaminated surfaces, the lack of available caregivers, and the disruption of healthcare services all had a significant impact on the mental well-being of vision-loss patients. We have identified a need for campaigns to highlight the challenges faced by this group and for policies that support if a future pandemic were to arise.
Limitations
The generalizability of the findings of this review is limited in the case of low-income countries as most of the articles came from developed countries. Specifically, vision loss patients in low-income countries may lack additional social support and have specific experiences not currently captured in the literature.
While we provided a broad overview of the psychological impact of COVID-19 on individuals with vision loss, we included a wide assortment of different causes of visual impairments. This broad approach was intentional to capture a general understanding of the community at large. However, it is important to recognize that each eye condition brings its own set of challenges and experiences that may not be captured within this meta-analysis.
It is also important to note that this study did not investigate burnout. Burnout is an important public health issue during the COVID-19 pandemic. Burnout is associated with increased risk of depression and anxiety, the use of a COVID-19 Burnout Views Scale could provide valuable insight into the prevalence of burnout and its impact on mental health in vision loss patients during the pandemic (Mistry et al., 2022).
Supplemental Material
sj-docx-1-jvi-10.1177_02646196241235283 – Supplemental material for Psychological effects of the pandemic on vision impairment patients
Supplemental material, sj-docx-1-jvi-10.1177_02646196241235283 for Psychological effects of the pandemic on vision impairment patients by Edward Tran, Nirmit Shah, Mohamed Aly, Vivian Phu and Monali S Malvankar-Mehta in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196241235283 – Supplemental material for Psychological effects of the pandemic on vision impairment patients
Supplemental material, sj-docx-2-jvi-10.1177_02646196241235283 for Psychological effects of the pandemic on vision impairment patients by Edward Tran, Nirmit Shah, Mohamed Aly, Vivian Phu and Monali S Malvankar-Mehta in British Journal of Visual Impairment
Supplemental Material
sj-docx-3-jvi-10.1177_02646196241235283 – Supplemental material for Psychological effects of the pandemic on vision impairment patients
Supplemental material, sj-docx-3-jvi-10.1177_02646196241235283 for Psychological effects of the pandemic on vision impairment patients by Edward Tran, Nirmit Shah, Mohamed Aly, Vivian Phu and Monali S Malvankar-Mehta in British Journal of Visual Impairment
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We are funded by the Glaucoma Research Society of Canada.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.