
Abstract
Depression and anxiety are common in people with congenital and acquired vision impairment but often go unaddressed. Staff from a variety of professions and roles in the sight impairment sector are well-placed to identify mental health issues and signpost individuals for support. However, many of these individuals need training to do this competently. The aim of this project was to develop a mental health training curriculum for staff. We used a seven-step method involving staff and service users from national sight loss charities and local authorities, and university researchers. The result was a curriculum containing five modules covering an introduction to mental well-being, the use of a standardised depression and anxiety screening tool, referral and support options and implementation issues to consider. Future work involves developing the curriculum into an online training programme for wide dissemination across the sight loss sector.
Keywords
Background
Congenital and acquired sight impairment can have profound psychological consequences (Demmin & Silverstein, 2020; Thurston, 2010), and it is now widely evidenced that symptoms of depression and anxiety are highly prevalent in individuals with vision impairment (Nollett et al., 2016; Schuster et al., 2018; Zhong et al., 2022). These conditions can add to the disability caused by sight loss (Demmin & Silverstein, 2020; Egede, 2007; Sabel et al., 2018) and impede effective rehabilitation (Simon, 2001). Worryingly, high numbers of people with vision impairment are not provided with specific support to address these distressing symptoms (Nollett et al., 2016; van der Aa et al., 2015), partly due to the current lack of requirement for screening: in Wales, while the primary-care based, National Health Service funded Low Vision Service Wales has implemented depression screening and referral pathways into low vision assessments, there is no similar requirement the wide variety of staff working in charities and local authorities in the United Kingdom. This leaves a big gap which this project seeks to address.
National eye care guidelines (National Institute for Health and Care Excellence, 2018) and professional bodies (College of Optometrists, 2019) recommend identifying depression in individuals with vision impairment using a short validated questionnaire and managing suspected depression via referral to a suitable professional for further assessment (National Institute for Health and Care Excellence, 2018). Following evidence that eye care practitioners generally lack confidence to undertake such screening (Fenwick et al., 2009; Nollett et al., 2018), one of the authors (CN) and colleagues developed and evaluated a mental health training session for low vision practitioners in Wales (optometrists and dispensing opticians with further training in low vision) (Bartlett et al., 2021). It focused on identifying depression using a validated two-item questionnaire (‘Whooley questions’; Whooley et al., 1997) and referring positive cases to the GP. Six months after completing the training, practitioners reported an increase in their confidence and perceived less barriers to using the questionnaire and recorded more instances of suspected depression (Bartlett et al., 2021; Nollett et al., 2020). Similar results were found for eye health and rehabilitation professionals who participated in depression screening programmes in Australia (Rees et al., 2010, 2012).
While training programmes exist for eye health professionals working in the vision impairment sector, to our knowledge, there is currently no standardised guidance or training for the large number of different types of staff employed in the UK third sector (charities) or the local authority (council) services. Workers in these organisations are engaged in wide-ranging roles, including rehabilitation officers, mobility officers, employment advisors, telephone advisors, course facilitators and counsellors. Hence, this project aimed to develop an online training curriculum targeted at the staff in these (non-health care) roles.
The training programmes for eye care professionals cited above have focused solely on screening for depression, but with increasing evidence of the prevalence of anxiety in people with visual impairment, there is a need to screen for both depression and anxiety. The PHQ-4 (Kroenke et al., 2009) is a useful tool to open conversations about mental health and identify possible symptoms. It is a brief, validated four-item questionnaire which assesses the key symptoms of both depression and anxiety (Table 1) and has been previously used with people with vision impairment (Clancy et al., 2022; Elsman et al., 2022; Fitzgerald & Fitzgerald, 2014, 2015). Given the lack of staff confidence around using such questionnaires, we designed a curriculum for a depression and anxiety training programme for frontline staff in the sight loss sector, in particular, non-health care professionals working in charities and local authority organisations (around 2000 staff). Importantly, we involved staff and service users in designing the programme to ensure it met their needs.
Questions and scoring system for the PHQ-4.
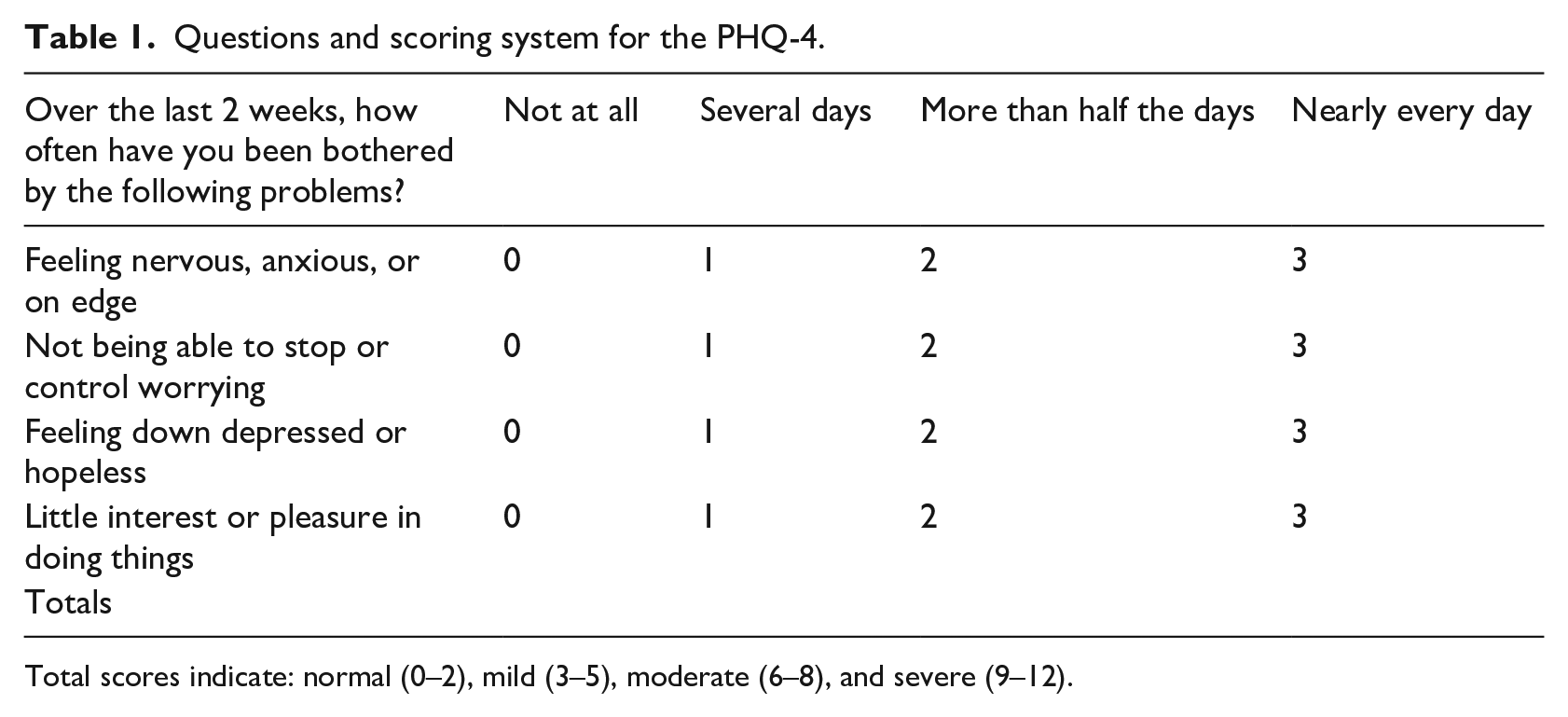
Total scores indicate: normal (0–2), mild (3–5), moderate (6–8), and severe (9–12).
Project procedures
This stakeholder consultation project was initiated by a collaboration called the UK Mental Health Screening Implementation Group. This group included staff experienced in working with people with sight loss: the lead for the Rehabilitation Workers Professional Network (2024, RWPN: the professional body for Vision Rehabilitation Specialists); representatives from three national vision impairment charities (Royal National Institute of Blind People [RNIB], Guide Dogs and Thomas Pocklington Trust) including the RNIB Head of Mental Health and Counselling; and academics from three universities (Cardiff, Abertay and Birmingham City) including a Senior Lecturer in Counselling (author MT) and researchers in the field of vision impairment and mental health (one also being qualified as Psychological Wellbeing Practitioner, author CN). We involved stakeholders in drafting a mental health awareness curriculum. We engaged with staff who would undertake the training (some of whom had visual impairment themselves) and service users who would be on the ‘receiving end’ of the training. We considered stakeholder involvement to be key in enhancing the relevance, usefulness, and sensitivity of the programme (Slattery et al., 2020).
The School of Medicine Research Ethics Committee (Cardiff University) assessed the project and confirmed that ethical review was not necessary, as the individuals involved were public representatives in a project and not participants in a research study. However, individuals did provide verbal consent to take part in the discussion groups, and the project was conducted in line with the principles of Declaration of Helsinki (World Medical Association, 2001).
To draft the curriculum, we conducted a number of steps in an iterative process (Figure 1).

The seven-step process.
In Step 1, we reviewed previous mental health awareness curriculums aimed at staff working with individuals with vision impairment (Bartlett et al., 2021; Rees et al., 2010, 2012). The main topics were collated in a spreadsheet and provided a starting point for the curriculum.
In Step 2, we held six discussion groups: one with staff and one with service users at RNIB, Guide Dogs, and Rehabilitation Workers Professional Network. The groups were run online to enable a geographical spread of attendees, and due to ongoing concerns about COVID-19, with the facility for individuals to dial in using the telephone if needed, thus reducing digital exclusion. An independent facilitator with experience in running public involvement activities (CN) led the groups with a member of staff from the organisation acting as co-facilitator to manage the logistics.
Members of the three organisations’ established staff and service user groups were invited to meetings (three staff meetings and three service user meetings). Each group comprised between 5 and 10 attendees and lasted for 2 hr (with a 15 min break). A standard set of questions developed for the project was used to guide the discussions around the perceived acceptance of mental health conversations, the acceptability of using the PHQ-4, the preferred support options and the desired length and format for delivery. The groups were audio recorded to aid note-taking, and the key points summarised and demonstrated with quotes, to inform the curriculum development. This was done at a high level, given the information collected was not research data. The written summary was sent to the group attendees to edit or to add further thoughts. The final summaries from each group were used to create a spreadsheet of key topics.
In Step 3, the curriculum writing team (including two counsellors and a psychological well-being practitioner) used the spreadsheet of previous course content and group summaries to create an initial outline of the proposed curriculum.
In Step 4, we sought input from staff and service users into this outline via two further discussion groups, one with staff (N = 5) and one with service users (N = 4) at RNIB. Due to resource limitations, we emailed the outline to staff and service users at Guide Dogs and RWPN to seek their input.
Following stakeholder input, the writing team revised the outline and added detailed content based on their expertise and the research evidence in this field (Step 5). It was then reviewed and edited by the wider project team, before being sent to staff and service users at the three organisations for further input and review (Step 6). In the final part of the process (Step 7), the curriculum content, format, and length were finalised.
Curriculum development
Step 1: List of potential course topics – Supplemental Appendix 1.
Step 2: Initial input from stakeholders – we report the feedback first from the three service user groups combined (part i), then from the three staff groups combined (part ii).
1. Four key themes from service users at RNIB, Guide Dogs and RWPN
Address mental health issues
The initial discussion groups with service users at the three organisations produced rich accounts of individual’s struggles with mental health.
I know whenever I first started losing sight it felt like a bereavement and you really had to grieve the loss of your sight and you got that low that the only way was up.
Individuals with vision impairment generally agreed that discussing mental health should be ‘part of the package’ provided by the third sector and local authorities, and staff should initiate conversations openly and confidently. The PHQ-4 was seen as acceptable and as providing a clear opportunity to discuss well-being.
I think it’s (PHQ-4) a great idea . . . It gives them the opportunity to say how they’re feeling and it’s then, it’s honestly being asked the question it gives them the opportunity to say I need help.
Building a trusting relationship
However, across all three organisations, individuals stressed the importance of building trust with the member of staff before they could answer honestly, particularly when it was feared that honest answers could lead to withholding of services or a guide dog.
Feeling heard and understood
Emphasis was placed on the manner of asking, so rather than being a ‘tick-box exercise’, the individual feels really heard and acknowledged; for example, positive responses be followed up with further questions so staff really understand a person’s position before moving on to offer support options. Service users conveyed the importance of staff developing ‘soft skills’ such as active listening, demonstrating empathy, and building trust to achieve this.
Offering support
Service users felt that organisations need to recognise staff are not trained counsellors and provide them with signposting options. The GP was considered a useful route for some, but others were concerned about long wait times for doctors and other National Health Service services. They advocated for self-help support options in the interim. Counselling, either through the third sector or privately, had been helpful for many, but could be unhelpful if the counsellor did not understand the impact of sight loss:
I felt counsellors outside maybe RNIB don’t acknowledge the true depth of what we consider to be a trauma, or to be a bereavement. They don’t almost acknowledge it like that. I think there’s definitely a gap there, with some counselling services.
Other useful forms of support included: Cognitive Behaviour Therapy (CBT), talking with an Eye Clinic Liaison Officer, peer support groups, self-help techniques, and engaging in hobbies: With regard to peer support groups: you’re not on your own and other people have gone through the same thing. It definitely lifts your spirits.
Service users thought staff should manage expectations when referring to services, particularly around waiting times. Support should be offered at all points of the sight loss journey and not just at diagnosis.
2. Eight key themes from staff at RNIB, Guide Dogs and RWPN
Assessing mental health
Staff at all three organisations recognised that people with vision impairment commonly experience mental health issues, and many try to identify if a service user is experiencing anxiety or depression. However, for most, it is not formally part of their role, and there is currently no standard assessment process:
It’s a very, very individual thing and everybody’s different. It comes out in a different way and I don’t have a standard way of doing things if you see what I mean?
Staff rely on assessing a service user’s demeanour, behaviour, and environment. They may also speak to family members or consult records. They believe emotional issues can be easily hidden, with anxiety in particular being difficult to detect. Therefore, training should cover the signs and symptoms of anxiety and depression, including the physical symptoms, and distinguish between symptoms which are ‘everyday’ and fleeting and those which become an issue and need addressing more fully. Practitioners currently make assessments about the appropriateness of addressing mental well-being with a particular individual and prefer to approach the topic ‘gently’.
Building trust
In agreement with service users, staff felt it was important to build trust and rapport before asking difficult questions:
It’s building that rapport, it’s building the trust. You tend to find like, as you say, it’s just a general conversation at first to get to know the person, and what are their likes and dislikes and then sometimes they will open up and it is like listening to that key word, and the body language is a great thing.
In some cases, they deal with high levels of distress including issues of abuse, alcohol addiction, and suicidal ideation.
. . . I’ve been dealing with three people who’ve attempted suicide recently.
Using the PHQ4
Staff agreed the PHQ-4 questions could be useful for opening a conversation about mental well-being, rather than trying to ‘pick up’ on signs. They liked the brevity of the measure and the standardised and validated assessment. However, they described concerns about it being a ‘blunt’ questionnaire which could damage rapport if not delivered sensitively:
Especially if you’re working with somebody whose anxiety is sky high and you just come in with a question straight like that (PHQ-4) . . . and sometimes you’ve took a while to build up that rapport, you can lose that relationship within seconds.
Acquiring skills
Staff expressed a desire for guidance on when and how to ‘weave them in’ to the assessment to avoid sounding robotic:
I still come back to the fact that you can introduce it, either introduce the questions in a different way or ask them at different intervals within your time with the person, and get out a credible and valid answer without suddenly saying, right I think you might be depressed, shall we just do this questionnaire and see what it comes up with?
They suggested follow-up questions were needed to really understand the person’s situation. Staff queried whether the wording of the questions could be adapted and whether the language might be leading, for example, to cause people to experience mental health issues. When informed this is not the case, practitioners suggested this should be noted in the curriculum.
Staff concerns
Staff shared service users concerns regarding dishonest answers if the individual feared being prevented from accessing services, or indeed if they wanted to avoid any intervention:
What would worry me is that people with anxiety and depression if they’re asked the same questions all the time will know the questionnaire and won’t answer them truthfully in the first place . . . you know, if they don’t want any intervention . . . .
One solution offered is to directly address this when introducing the questions, stating that honest answers would not affect the service they receive. Building trust was seen as crucial and staff suggested that listening and empathy skills should be covered. Concerns were also raised about ‘opening a can of worms’ and pushing a person into an emotional state in a time-limited conversation. A desire to leave them on a ‘positive note’ led to requests for guidance on how to sensitively close a conversation. One of the main issues shared in the groups was if a person’s scores indicate possible issues, ‘then what?’:
For me the thing is the response, what are you going to do with that information . . . I think it’s what are you going to do if they answer yes to those questions.
Support and signposting
Currently, some staff feel if emotional difficulties are related to sight loss they will offer support in the form of practical solutions. If they feel it is unrelated, they are more likely to refer to other professionals including the GP, mental health nurse, or counsellor, although they acknowledged that long waiting times were an issue:
If it is around the visual impairment then I would feel fairly confident to deal with some of those issues because I may have some of the solutions that that person actually wants or needs. If it’s a general depression I would want to be looking at the support that that individual gets professionally outside of our service.
Others take a ‘softer’ approach and signpost to peer support groups, courses, online CBT, or activities. They noted that it can be time-consuming to find the right support. Staff requested clear guidelines on what support to offer but were reluctant to take specific actions based on a particular score. They also wanted help to manage service user expectations and to deal with suicidal ideation.
Staff self-care
Another frequently discussed issue was the impact of addressing mental health on their own well-being and how to look after themselves. Options included having formal supervision and establishing clear protocols in each organisation. Talking about mental health was perceived as being scary for some staff, and they suggested the training should explain why it is important, why it is part of their role and how they can seek support and further guidance.
Training requirements
Staff suggested devoting at least a day to the training, as it is a complex topic with a lot to learn. The general preference was for face-to-face learning or live virtual learning, or for online learning, an interactive style with role plays, videos, and knowledge checkers. Live virtual follow-up meetings were requested once they had put the learning into practice, so they could problem solve with colleagues. They also recommended that organisations consider how to record the service user responses in their databases, so that people were not repeatedly questioned by different staff.
Steps 3–6: Development of and feedback on the curriculum (discussion groups and email)
Based on the previous course review and initial input from staff and service users, a draft curriculum was written, including six modules, each intended to take 45–60 min to complete.
Feedback on the draft curriculum from staff and service users was mainly received in relation to Module 5 which outlined the proposed framework of support options. It was seen as a useful ‘toolbox’ which staff could access but concerns were expressed over how staff would determine the level of support appropriate. Due to waiting times, one service user was keen to promote alternatives to the GP such as peer support and social prescribing. Conversely, another was concerned that the draft framework did not provide for people with more difficulty. It was revised to reflect these comments.
For Module 4 outlining the PHQ-4, staff asked for videos demonstrating asking the questions in a natural way and iterating the confidentiality of responses, and examples of how to integrate the PHQ-4 with other safeguarding questions. Staff suggested there could be less emphasis on dealing with suicidal ideation, covered in other training, and more on supporting someone who has received bad news, although it was acknowledged that this might be outside the scope. Staff were keen that training was not a ‘one-off’ course and that ongoing resources should be provided, for example, via a Teams space or forum.
The feedback was incorporated into draft 2 of the curriculum where possible, and further content developed. The curriculum was reduced to five modules and additional resources for post-training were added. In a second round of feedback, advice from one service user was given to be mindful of language around distinguishing everyday symptoms from a clinical disorder, subsyndromal depression, acquired sight loss, sight impairment, and disability. Suggestions to highlight the positive element of anxiety and to include examples of people from diverse backgrounds were made by service users, who also shared concerns about the current wording around closing a conversation. These comments informed the final draft.
Step 7: The final curriculum
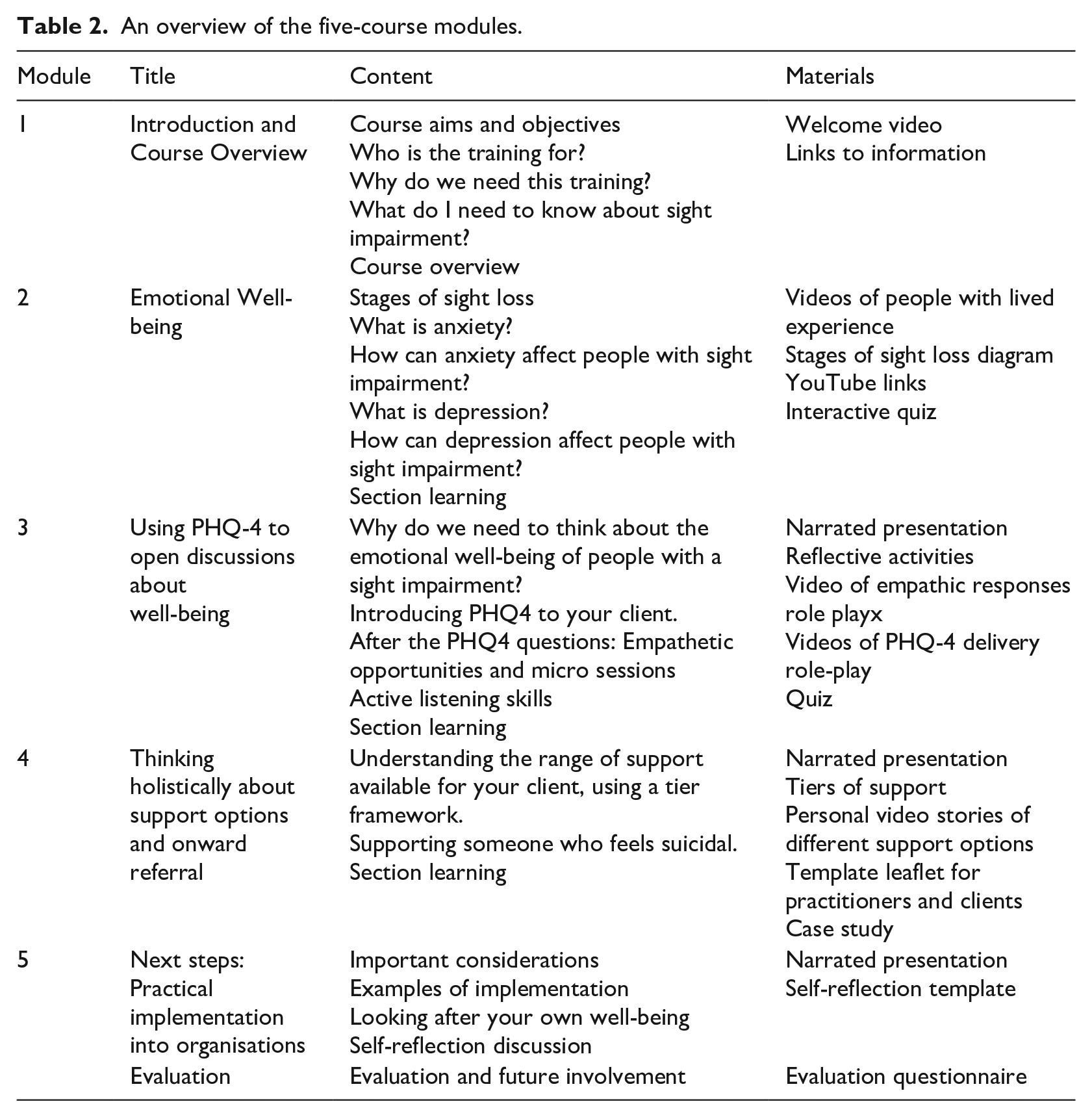
An overview of the curriculum content is presented in Table 2. While the preference of staff was to have real-time face-to-face or virtual training, this was not deemed feasible by the organisations involved due to the sheer number of staff requiring training and the lack of resources to deliver it. Instead, the plan is to develop the curriculum into an accessible online, on-demand training programme. However, to address staff preferences, we have developed additional materials which can be used in small group real-time sessions to reflect on learnings from the training and subsequent practice.
An overview of the five-course modules.
Summary
In this stakeholder consultation project, we involved service users and staff at charity and local authority organisations in developing a mental health awareness curriculum for front-line staff in the sight loss sector. Their involvement shaped the content and delivery format.
Staff in these organisations expressed similar concerns to those presented by eye care and rehabilitation professionals, including difficulties in identifying conditions, how to include the PHQ-4 in an assessment, the potential for ‘opening a can of worms’ and what support to offer (Elsman et al., 2022; Nollett et al., 2018, 2020). In addition, they worried that service users might not be honest if they thought sharing mental health issues would prevent them from accessing services. Staff shared concerns about the impact of discussing mental health on their own well-being, a burden also identified by occupational therapists working with people with depression (King et al., 2022), but acknowledged the importance of doing so and liked the structure and brevity of the PHQ-4. As in other studies, service users felt the PHQ-4 was an appropriate tool to open conversations (Elsman et al., 2022; Holloway et al., 2014) but stressed that staff need to build trust and have appropriate ‘soft skills’ to make them feel truly heard. They would like to see a range of support options offered and have staff manage expectations around waiting times.
If staff in charities and the local authority feel more confident and prepared to refer service users for support with anxiety and depression, there may be potential benefits for individuals with vision impairment such as increased motivation to attend rehabilitation services (Overbury & Wittich, 2011) and participate in society (Cimarolli et al., 2016), as well as reduced burden on their caregivers (Kuriakose et al., 2017). Being appropriately trained may also prevent ‘compassion fatigue’ in staff (Collins & Long, 2003).
A strength of the project was the strong stakeholder involvement. Online groups allowed a geographical spread of attendees, and using MS Teams facilitated telephone dial-in for those without internet access. A limitation was that the groups were held during the day, possibly excluding those in full-time employment. We did not capture formal feedback on people’s experiences of being involved, which may have been useful for shaping future projects.
The proposed curriculum builds goes beyond previous courses for staff working with vision impairment. First, we have expanded the remit to include anxiety screening. Second, input from staff and service users has helped us to expand the content of previous programmes (Bartlett et al., 2021; Rees et al., 2010, 2012) by (1) placing more emphasis on developing ‘soft skills’, (2) addressing how to manage one’s own well-being, (3) including interactive material such as videos, role plays, and material for discussion.
Conclusion
In this project, to the best of our knowledge, we developed the first mental health training curriculum specifically for non-health care frontline staff working with people with vision impairment in third sector and local authority organisations. Staff and service users were involved in drafting the content and format in an iterative seven-step process to ensure it meets their needs. The next step is to develop the curriculum into an online training programme which can be shared with the sight loss sector.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196241250210 – Supplemental material for Involving stakeholders in designing a mental health curriculum for staff in the vision impairment sector
Supplemental material, sj-docx-1-jvi-10.1177_02646196241250210 for Involving stakeholders in designing a mental health curriculum for staff in the vision impairment sector by Claire Nollett, Peter Cooke, Simon Labbett, Tom Margrain and Mhairi Thurston in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196241250210 – Supplemental material for Involving stakeholders in designing a mental health curriculum for staff in the vision impairment sector
Supplemental material, sj-docx-2-jvi-10.1177_02646196241250210 for Involving stakeholders in designing a mental health curriculum for staff in the vision impairment sector by Claire Nollett, Peter Cooke, Simon Labbett, Tom Margrain and Mhairi Thurston in British Journal of Visual Impairment
Footnotes
Acknowledgements
We wish to thank staff at the following organisations: RNIB – Harminder Kaur and Harriet Bird for their assistance in facilitating the stakeholder groups and Amanda Hawkins for her input into the curriculum; Guide Dogs – Helen Vaterlaws Whiteside and Sarah Baverstock for organising the stakeholder meetings. Dorothy Miller and Chris Roach for their input from a safeguarding perspective and help with compiling previous courses; Martin Walls for his overall guidance; Thomas Pocklington Trust–Eamon Dunne for his curriculum contributions. Many thanks also to the staff and service users who took part, to whom we are very grateful for their time, insights, and direction.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Wales Innovation Fund – Innovation for All – Impact Stream [grant number JA1112IF50] through Cardiff University.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.