
Abstract
According to the UK Government, people with a disability or long-term health condition are more likely to experience chronic loneliness than the general population. However, government figures do not disaggregate data on loneliness among different types of health conditions or disabilities, and it remains unclear how this affects people with visual impairment (VI). This review examines experiences of loneliness and isolation among people with VI. Six databases (CINAHL, PubMed, Scopus, Sage, APA Psycharticles, and Psychology and Behavioural Sciences Collection) were searched using a Population, Interest and Outcome (PIO) framework, yielding a total of 2476 articles. A total of 29 articles were selected and appraised for quality using JBI appraisal tools. These articles represented studies from 14 countries. Relevant Government and voluntary sector organisation websites were also considered. Findings showed widespread experiences of isolation and exclusion among people with VI, but subjective experiences of loneliness did not necessarily align with this. Further research is needed to gain a better understanding of the relationship between VI and loneliness and experiences of loneliness for people with VI within both LGBTQ+ communities and within Black, Asian, and Ethnically Minoritised communities, where research remains notably scant. Studies about the impact of the COVID-19 pandemic showed its heightened effect on isolation and loneliness among the VI community. Further research is needed to understand the long-term effects of this. While technology holds promise in mitigating loneliness and isolation among individuals with VI, accessibility issues persist. Future research is needed to understand how technology-based interventions might address loneliness and isolation for individuals with VI and the accessibility barriers associated with the implementation of these. For loneliness and isolation to be minimised, recognising the diversity within the VI population is imperative for tailoring interventions and initiatives effectively.
Introduction
This review examines experiences of loneliness and isolation among people with visual impairment (VI). According to the UK Government, people with a disability or long-term health condition are more likely to experience chronic loneliness than the general population (UK Government, Department of Culture, Media & Sport, 2023a) However, government figures do not disaggregate data on loneliness among different types of health conditions or disabilities, and it remains unclear how this affects people with VI. Loneliness has been associated with adverse impacts on both physical and mental health. Physically, loneliness has been linked to conditions such as hypertension, strokes, coronary disease, and increased risk of premature mortality (Cacioppo & Capitanio, 2014). It has also been found to correlate with mental health issues such as depression, anxiety, and disturbances in sleep patterns (Cacioppo & Capitanio, 2014). Perlman and Peplau (1981), define loneliness as a subjective, painful feeling experienced by an individual when they recognise the quality of their relationships are not as they would wish them to be. Three distinct categories of loneliness have been identified. Social loneliness, which describes the condition in which people perceive an inadequacy in their desired relationships and an inability to foster such connections (De Jong Gierveld & Van Tilburg, 2006). Emotional loneliness, which pertains to the experience of lacking closeness or intimacy within one’s social network and the inability to establish such connections (De Jong Gierveld & Van Tilburg, 2006). Finally, existential loneliness that entails a profound sense of separation between oneself and the broader society (Campaign to End Loneliness, 2023).
Those experiencing isolation can be impacted both physically and mentally. Isolation is characterised by an objective, observable lack of relationships, contact, or social connection (Cudjoe et al., 2020). While there can be overlap between isolation and loneliness, the two are distinguishable and not causally related. An individual who is isolated may not feel lonely if they do not experience a painful feeling in response to this. Conversely, a person who has relationships and is highly socially active can feel lonely if these relationships do not contain the quality or intimacy that the individual seeks from them (Yang, 2019).
Little research has focussed specifically on the relationship between VI and loneliness and isolation and there is lack of empirical evidence as to whether people who live with VI are more likely to experience chronic loneliness and/or isolation. There is also a lack of information about how living with a VI contributes to experiences of loneliness and isolation and the impacts these have for people. In a previous literature review on this topic, Hodge and Eccles (2013) concluded there was modest evidence that people with VI were more likely to experience loneliness, although some studies in their review did not find any association. In addition, much of the literature explored loneliness and isolation as experienced by older people with VI. Recent data have identified that younger people are most likely to report feelings of chronic loneliness (UK Government, Department of Culture, Media & Sport, 2023a). This review examines the literature on loneliness and isolation in relation to people living with VI. It synthesises existing knowledge and identifies areas for future research.
Methodology
Search strategy
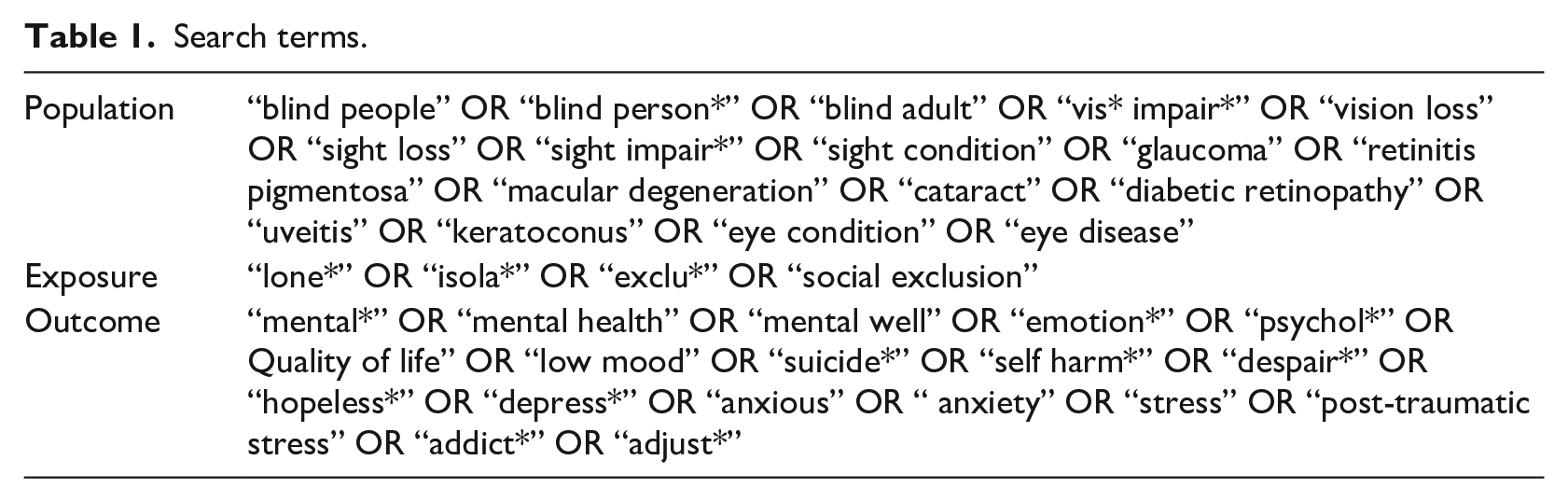
Six databases (CINAHL, PubMed, Scopus, Sage, APA Psycharticles, and Psychology and Behavioural Sciences Collection) were searched using a Population, Interest, and Outcome (PIO) framework to define the search criteria (Shaffril et al., 2021). A wide range of search terms were included to maximise the yield of articles. Table 1 below contains the search terms that were used within each PIO category.
Search terms.
Further inclusion criteria defined peer-reviewed journal articles in English language from 2016 until June 2023. These dates were chosen to cover a period of increased attention to loneliness and isolation as a health priority in the United Kingdom. Combined, these searches yielded a total of 2476 potential articles. Zotero 5.0 (Corporation for Digital Scholarship, 2022) was utilised to remove duplicate articles. Titles and abstracts were then screened and those not relevant to the study were excluded. Table 2 provides a breakdown of the reasons for exclusion by each database.
Exclusion of articles by database.
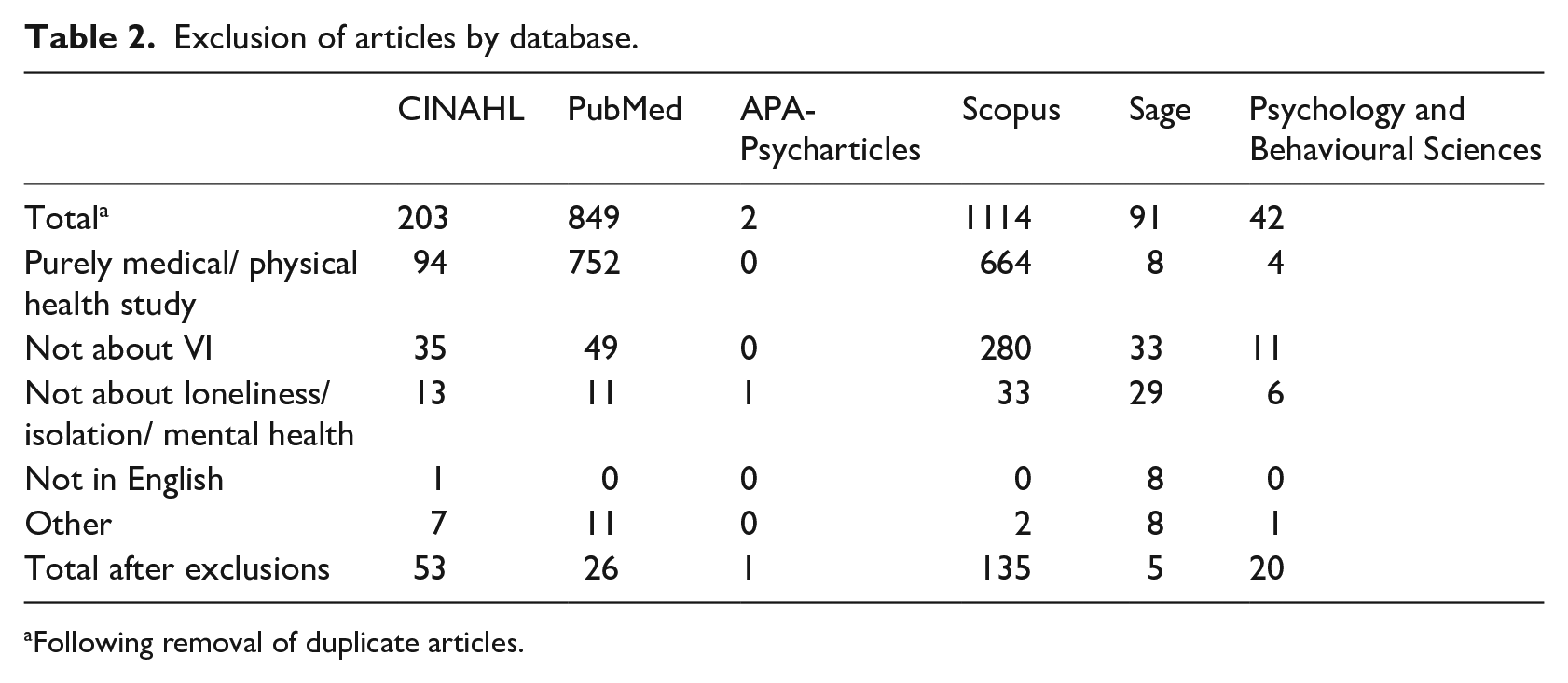
Following removal of duplicate articles.
A total of 240 titles and abstracts were screened by the lead researcher and research assistant. Those focussed solely on mental health, without any reference to loneliness or isolation, were excluded, leaving 29 articles, which were read in full and are the main subject of this review (see Figure 1).
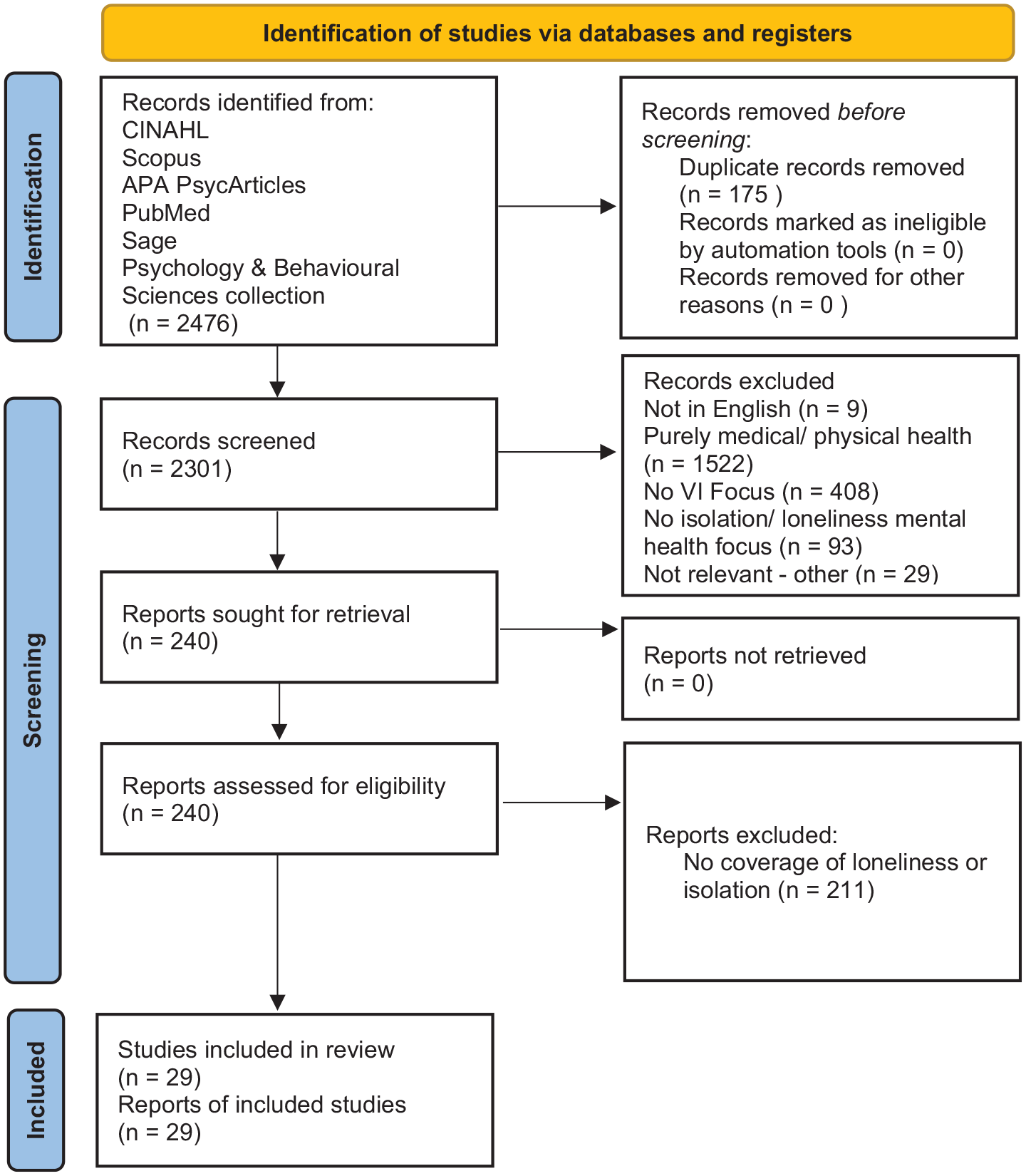
PRISMA Flow Diagram for review process. (Page et al., 2021).
Search results
A full list of articles included is provided in Table 3.
Peer-reviewed academic articles included in the review.
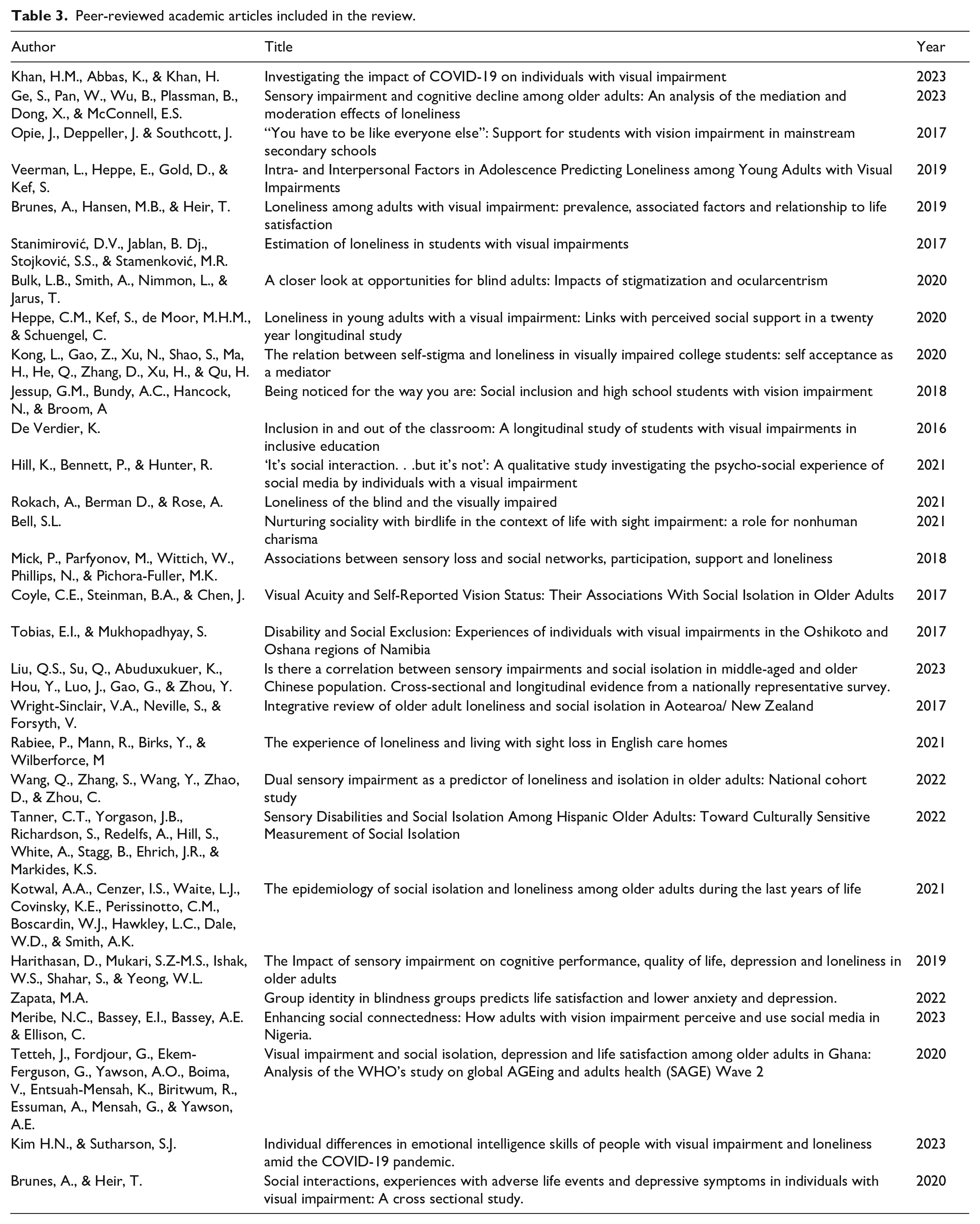
These 29 articles represented studies from 14 countries over five continents. About 34.5% (10) were qualitative studies and 31% (9) were cross-sectional studies. The remaining articles were cohort studies, 20.7% (6); prevalence studies, 6.9% (2); and a further 6.9% (2) systematic reviews.
Using the JBI Critical Appraisal Tools (Joanna Briggs Institute, 2023) to assess the rigour of the studies, 69% (20) were assessed as being of high quality, 24.1% (7) were of moderate quality, and 6.9% (2) were of low quality. Further articles identified from references within the articles as being potentially relevant were added to the report. Further contextual information was gathered from articles identified in library searches and Google Scholar. Government and voluntary sector organisation websites were also searched, including the UK Government and the devolved administrations of Scotland, Wales, and Northern Ireland. The voluntary sector searches focussed on national organisations in the VI sector; Royal National Institute of Blind People (RNIB; 2020), Guide Dogs UK, Thomas Pocklington Trust, Bravo Victor and some bodies with an interest in loneliness including the Campaign to End Loneliness, Jo Cox Foundation, the NHS, and the Mental Health Foundation. All searches took place in May and June 2023.
During the analysis, themes were identified and knowledge was synthesised by categorising the literature into clusters around specific issues, in relation to the research question. Verification of the themes was established through discussion among the researchers, until consensus was reached.
Results and discussion
Prevalence of loneliness and isolation among people with VI
There is little consistent research evidence about whether VI, is a predisposing risk factor for loneliness, with very few studies establishing a clear link between VI and loneliness. However, there is a broader body of evidence, across academic and other literature, suggesting isolation and exclusion are widespread for people with VI. This is experienced in different ways and across various life stages and cultures and, in some instances, it is associated with loneliness (Bulk et al., 2020; Hill et al., 2021; Kotwal et al., 2021; Mick et al., 2018; RNIB et al., 2022; Tetteh et al., 2020).
Consistent with Hodge and Eccles (2013), a greater number of studies examined loneliness and isolation experienced by older people. There appears to be much less attention to studying loneliness and isolation among younger and middle-aged adults. A study of loneliness among 736 adults (over 18 years) with VI in Norway found that people with VI were significantly more likely to experience loneliness across all age groups (Brunes et al., 2019). Loneliness was associated with elevated risks in connection to other life factors such as being younger, having other impairments, being unemployed, and having experience of bullying or abuse. Furthermore, loneliness was more prevalent among those who were severely sight impaired (blind) in comparison to those who were sight impaired (partially sighted). A longitudinal study of people with VI in the Netherlands examined the impact of different types of social support available as people made the transition from adolescence to adulthood. It found the availability of different forms of support at different stages were important in predicting whether people would experience loneliness as they aged (Heppe et al., 2020). The influence of peer support in the transition from adolescence to adulthood was found to be predictive of loneliness. Although these relationships have also been found with participants without VI, the researchers concluded specific challenges faced by participants with VI in being able to access social networks and peer support may contribute to increased vulnerability to loneliness in later life.
In other studies, loneliness among participants with VI was associated with emotional intelligence among people experiencing loneliness during the COVID-19 pandemic (Kim & Sutharson, 2023); higher emotional stability and social competence during adolescence were shown to predict lower loneliness among participants with VI in later life (Veerman et al., 2019); and Kong et al. (2021) found self-stigma and self-acceptance to be associated with levels of loneliness among Chinese college students with VI. These studies suggest, while some populations may be more prone to loneliness, there are a range of other factors, operating on the individual level that are likely to influence the subjective experience.
Qualitative experience of loneliness
Rokach et al. (2021) sought to explore differences in qualitative experiences of loneliness between people with VI and people without VI. The latter scored significantly higher than the participants with VI on measures of emotional distress, feelings of social inadequacy, social isolation, and self-alienation. The authors speculate in making sense of their experiences, people living with VI may not attribute difficult emotional experiences to loneliness but interpret these as being related to the impacts and effects of their VI.
Loneliness among further education students with VI
Two studies examined the prevalence of loneliness among college students with markedly different results. Stanimirović et al. (2017), found significantly lower levels of general loneliness in a sample of students with VI in comparison to sighted students. In further measures used to examine different types of loneliness (social, emotional, and romantic), the researchers found no significant differences between the sighted and VI groups. In their discussion, the researchers speculate their findings may have been influenced by contextual factors. There were significantly more females than males in the sighted control group, which could reflect gender differences in the prevalence of loneliness. Students with VI who volunteer for a study may be more open, communicative, and therefore, less likely to be lonely than those who declined to participate. Also, students with VI taking part in research, they speculate, may not want to be perceived as different or impaired. Furthermore, the provision of support available to students with VI in the university setting may have resulted in their forming relationships with support providers that guard against loneliness. However, the researchers were confident enough in their findings to conclude that VI alone was not a crucial factor in loneliness in students.
The other study looked specifically at aspects of loneliness among students in China. A total of 78 students completed a series of questionnaires measuring loneliness, self-acceptance, and self-stigma (Kong et al., 2021). This study found much higher rates of overall loneliness among the research participants with VI than those in sighted populations. Within the reasons outlined as being potential contributors to this, there are some factors of the student experience, which may be relevant and raise questions about the generalisability of the findings to other settings. For example, the students with VI who participated in this survey were accommodated and taught separately from other students and had limited access to a full range of educational options. The authors describe these as contributing to reduced opportunities to connect with others both within the college community and society in general.
Isolation and contributing factors
Although research on the prevalence and experience of loneliness appears to be inconsistent and evidence suggests a wide range of factors moderate and mediate the experience of loneliness among people with VI, there is a much clearer picture in relation to the experience of isolation, which is represented throughout both the academic and non-academic literature included in this review.
Communication
Communication issues appear to be a significant contributor to isolation for people living with VI. For example, in social settings, people with VI report sighted people regularly avoid communication with them, due to their feeling uncomfortable in not being able to use regular eye contact or other visual cues to initiate interaction. In living with VI, some people report higher instances of communication difficulties as they are unable to perceive non-verbal communicative signals (Bulk et al., 2020; Coyle et al., 2017). These difficulties can be particularly impactful for young people with VI who may not be able to use feedback from non-verbal communication or visual cues as a moderator or influence on their own behaviour. Research among adolescents with VI has found smaller social networks and a higher level of dissatisfaction with the amount of social contact (Veerman et al., 2019).
In combination, and over time, these communication difficulties and social challenges can contribute towards people with VI being ignored, overlooked, and left out of social activities, and contribute towards anxiety and avoidance of social situations.
Challenges in daily living
Steinman and Allen (2012) assert one of the most disabling aspects of VI, particularly for those who acquire sight loss, is in adjustment to daily living. This can lead to people developing feelings of dependence and reduce their sense of autonomy and control over their life, which people with VI can experience as distressing, leading to a loss of confidence and further withdrawal and isolation.
One of the most important of these, identified by people with VI, is the lack of opportunities for engaging in physical activity and sport. Physical exercise is widely recognised as being important for physical and mental health and the inability of people with VI to participate may be a driver of exclusion and isolation. For people with VI who are experiencing emotional or psychological difficulties, this also prohibits engagement in potentially therapeutic activities (RNIB et al., 2022).
Accessibility and transport issues
Access to transport is consistently identified in surveys as being the biggest factor inhibiting the social inclusion of people living with VI and improving this could facilitate major improvements in reducing exclusion and isolation. Research indicates that 25% of people with VI do not get out as much as they would like, rising to more than a third of people with moderate or severe VI and 43% of people with VI over the age of 75. (RNIB et al., 2022). Further challenges to getting out and about relate to street clutter, which affects people’s ability to safely navigate their environment. A third of respondents in the report said they had been injured within the previous 12 months through collisions with items in cluttered streets.
Stigma and discrimination
Across the literature, there are examples of people with VI being subjected to and impacted by stigma and discrimination, both directly and indirectly and through different stages of life. Bulk et al. (2020) interviewed adults with VI in Canada on the impact of stigmatisation and the effect of living in a society generally designed for people with sight. All participants were able to describe situations of being discriminated against within a range of societal and interpersonal contexts, which shaped their opportunities in life. The effects of discrimination as it impacts on people with VI and contributes to isolation and exclusion can be seen and inferred through research on a wide range of issues. These include employment, with only 25% of working-age people who are registered as sight impaired or severely sight impaired being in work (RNIB, 2017); social activities (Hill et al., 2021; Mick et al., 2018; RNIB et al., 2022), housing with figures showing that people with a VI are over-represented in social rented housing and less likely to own their own home (RNIB, 2024), which is associated with a higher tendency towards experiencing loneliness (Office for National Statistics, 2019) and research in the Netherlands shows people with VI being routinely discriminated against when trying to access private rented housing (Verhaeghe et al., 2016); relationships, with research suggesting people with VI are later than their sighted peers in entering into romantic relationships and starting families of their own (Heppe et al., 2020); and finance, with people having VI facing higher costs of living related to their disability and being disproportionately affected by inflationary increases (RNIB, 2022). Internalised discrimination and self-stigma have also been identified in research with people living with VI. Self-stigma is said to occur when negative attitudes or beliefs that are held about a particular group, such as people with a disability, are adopted by individual members of that group themselves. In interviews with adults with VI in Canada, this was expressed through people not accepting their disability and attempting to reject or deny aspects of their VI, desiring to not be perceived or treated as different (Bulk et al., 2020). For some, this resulted in rejecting the use of mobility aids, such as a white cane or a guide dog, which would identify them to others as being a person with VI. This pattern of people rejecting, denying, or hiding their VI or aspects of it, appears to be consistent in a number of contexts and is often described when people are dealing with sight loss within their experiences of social exclusion in communal settings such as schools (de Verdier, 2016; Jessup et al., 2018), colleges (Kong et al., 2021), care homes (Rabiee et al., 2021), and social and community settings (Bulk et al., 2020; Hill et al., 2021).
Loneliness and isolation among older people with VI
There is still a significant focus within the research on VI and loneliness in older adults. As people become older, one of the most common health issues experienced is a deterioration in vision, which can result in sight loss of varying degrees of severity (Coyle et al., 2017; Harithasan et al., 2019; Tanner et al., 2022). This can be accompanied by other potentially debilitating health conditions, leading to loss of independence and mobility. In addition, it may impact on people’s ability to engage with social and recreational opportunities. This may result in people becoming isolated and, coupled with the loss of partners or friend networks through retirement or bereavement, there can be an increased vulnerability to loneliness (Liu et al., 2023; Yang, 2019). However, it is only among the ‘oldest old’ that levels of loneliness are higher than general population norms (Rabiee et al., 2021). The most recent UK data suggest that loneliness is most common among young people (UK Government, Department of Culture, Media & Sport, 2023b). Although this may reflect a genuine shift in the prevalence of loneliness at different life stages, there is also the possibility that wider cultural changes have occurred, which make talking about emotions and disclosing difficult feelings, such as loneliness, easier for younger people than it is for older people.
Loneliness in combination with VI in older adults has been associated with low net worth (Kotwal et al., 2021); cultural factors (Tanner et al., 2022; Tobias & Mukhopadhyay, 2017; Wright-SinClair et al., 2017) such as whether people live in rural or urban communities (Wang et al., 2022), marital status and other supportive relationships and networks (Mick et al., 2018), as well as having an accelerant effect on cognitive decline (Ge et al., 2023). However, Harithasan et al. (2019) found no association found between VI and loneliness in a study investigating sensory loss and the interaction with outcomes associated with older people, such as cognitive decline, depression, and quality of life. Kotwal et al. (2021) examined loneliness among older people during the last years of life and VI was found to be associated with loneliness, but not with isolation. 19% of participants were socially isolated and 18% were frequently lonely but only 5% experienced both. There is discrepancy between this and other studies, which have more clearly identified isolation among people with VI. Coyle et al. (2017) found that VI was consistently associated with isolation across a range of social and emotional measures. Tanner et al. (2022) also found that VI was also a strong predictor of social isolation in a longitudinal study of older adults in the United States. This research suggested measures of isolation need to be more culturally sensitive. When an adapted questionnaire was used for Hispanic research participants, different findings were discovered, noting that the more familial culture within this group appeared to provide a protective effect against isolation. Wright-Sinclair et al. (2017), in a systematic review of empirical studies examining loneliness among older people in Aotearoa/New Zealand, found VI was the only physical health factor significantly related to loneliness. In addition, they highlighted a relationship between loneliness and social isolation among older people with VI who live alone, positing social policy, which encourages and supports older people to continue to live within their own homes, while well intentioned, may be contributing to experiences of loneliness. In relation to the differences between living independently and communally and contrasting with the arguments of Wright-Sinclair et al. (2017), one article examined the experiences of older people with VI living in care homes in England (Rabiee et al., 2021). These researchers referred to a previous study (Victor, 2012), indicating that loneliness among care home residents is thought to be twice as prevalent as that among older people in the community. This is attributed to the experience of entering the care home environment, which interrupts established networks of support and social contact. Indeed, residents with VI, in this study, described widespread experiences of exclusion, isolation, and loneliness within the care home setting. People spoke of communication difficulties arising because they were often unaware of who they were sitting with in communal areas and unable to pick up on visual cues that might have initiated social interaction; that information regarding activities and opportunities for socialising were not communicated in accessible formats and that support was not available for accompanying people to potential social or cultural opportunities within the community. Where efforts at inclusion in activities were made in the care homes, these were often experienced as tokenistic and even patronising rather than as meaningful engagement. However, the findings of this report indicate that the residents were often accepting of their situation and satisfied with their quality of life, finding meaning and engagement in other ways.
Children and adolescents
Three articles specifically focussed on the experiences of children with VI in mainstream school education. Two of these were qualitative studies from Australia and one longitudinal study from Sweden. In the study by Opie et al. (2017), children, parents, and teachers report that despite legislative requirements for adjustments to be made for children with disabilities (including VI) to be included in an equitable way in education, this was rarely translated into practice. Children described a range of VI-related difficulties they routinely encountered within the school system, which were not adequately addressed. This gave rise to a sense of isolation, a heightened sense of being different or ‘othered’ in their experiences within the school setting. Some instances of being excluded through discrimination and preconceived attitudes towards what the children might be able to achieve or participate in were also described. Jessup et al. (2018) identified five themes affecting the inclusion of students in schools through interviews with 12 children in mainstream Australian high schools. These were ‘putting myself forward’, describing the strategies children would use to develop and enhance their personal relations and inclusion; ‘Knowing me’ where the young people spoke about the importance of their treatment from other people and their experiences of having their needs as individuals met, or not met, across a range of support and personal domains; ‘Having Control’, where the participants felt less excluded when they were appropriately supported to be able to access the full range of educational and other opportunities available within the schools setting; ‘Having a place to shine’ where opportunities for the children to be able to engage in activities they enjoyed or were good at and being acknowledged by others in these and ‘peer exclusion and rejection’, which the interviewees described as being the most difficult and hurtful part of their school experience. The study concluded that while some of the participants had good relationships within school, around a third were struggling and all the children had experienced social difficulties. The authors raise concern regarding the impact this might have on these children’s mental health and well-being in the long term.
de Verdier (2016), in a longitudinal study of students with VI, parents, and teachers throughout their school years, identified many of the same issues. The students found it difficult to be accepted by their sighted peers in social groups, and although it was possible for the adults in the school environment to manage group dynamics and ensure inclusion when the children were younger, as they progressed into adolescence it became harder for this influence to be effective. Most students spent their break times alone as they got older and this was experienced as painful rejection. One student left mainstream education to attend a specialist school for blind children and subsequently described feeling included for the first time. The students in this study consistently described increases in their exclusion over time in their educational journey. This led students to reject potentially useful aids, as these became symbols of their VI, which were visible to their sighted peers, marking them out as different. The rejection of potentially useful tools and strategies had consequences for their ability to engage as fully or as successfully as they might otherwise have done. Another coping strategy was for children to equate academic achievement with personal success and immerse themselves in their studies. Schools which prioritised the social relations within the class were found to have the most successful students in relation to overall well-being.
These studies indicate that social inclusion for VI students in mainstream schools is not something that happens by merely having children with VI included in the classroom and playground. To make true inclusion a reality, knowledge about the social and emotional needs of young people with VI is needed in school settings along with continuous effort for these needs to be met.
Impact of the COVID-19 pandemic
During the COVID-19 pandemic, the number of people describing themselves as lonely rose by over 2% nationwide which equates to around a million additional individuals experiencing chronic loneliness (UK Government, Department of Culture, Media & Sport, 2022). In a systematic review of studies conducted into the impact of the pandemic, Khan et al. (2023) concluded there was substantial evidence that emotional distress and social isolation were considerably higher for people living with VI throughout the pandemic. Unique difficulties were experienced about being able to adhere to the rules around keeping distant from people, as this requires visual awareness of where other people are in relation to oneself. Other requirements related to vision included signage to guide people, inconsistent directions in shops, transport hubs, and other public spaces. These requirements were generally inaccessible to people with VI, who could not read them. Guide dogs were not able to react to these new circumstances, having not been trained for them and concerns existed about using human guides, due to physical proximity, raising anxiety about the spread of the virus. People with VI are also more reliant on touch (either of surfaces or other people) than the general population to be able to gain information and interact with the environment, and again touch was a means through which the virus could be spread and was therefore discouraged. These factors contributed to increased anxiety for people with VI in attempting to engage in any type of public activity, both through the increased risk of catching or transmitting the virus and by being exposed to criticism and hostility from other people due to being unable to follow the prescribed rules on social distancing. In a UK survey of individuals with eye diseases resulting in various levels of VI, Ting et al. (2021) found those with moderate or severe VI were three times more likely to have experienced loneliness during the pandemic than those with mild or no VI.
In a US-based study, participants with VI also reported experiencing some degree of loneliness while living through the pandemic restrictions (Kim & Sutharson, 2023). The people in this study experienced a range of difficult emotions, including feeling isolated, left out, being ignored, pessimistic, unhappy, upset, and uncomfortable. In measuring the emotional intelligence of those who took part, the researchers found those who were able to manage difficult emotions were less affected by loneliness. Reduced physical exercise has also been linked to loneliness and people living with VI may have experienced increased loneliness as opportunities for exercise and physical activity, which are already areas where difficulties exist for people with VI (RNIB et al., 2022) and were further diminished during the pandemic period. Heinze et al. (2021) examined how levels of loneliness changed with different levels of restrictions. Results showed levels of loneliness were highest among participants with disabilities and people with VI compared to people with no disabilities. Gori et al. (2022) examined how the pandemic was experienced by people with VI in Italy. They found that those with less severe VI were more affected by the emotional impact of the social restrictions, while participants with more severe VI experienced more problems in practical matters, such as being able to shop for food or being able to organise regular home cleaning or maintenance. Participants with severe VI also reported more concerns about their loss of autonomy than others. Being more affected by practical challenges than emotional ones during the pandemic may be reflective of the unique difficulties faced by people with VI in having to navigate a new physical environment and the potential loss of regularly available assistance in doing so. Were people then to be unable to reliably obtain such essential resources as food, it is inevitable this might be the focus of concern since survival depends on it. UK research also found significant difficulties among people with VI ensuring they had access to food during the pandemic (RNIB, 2020).
There is compelling evidence across the studies that a range of factors combined to make this a uniquely difficult experience for many people living with VI and increased isolation and loneliness were common. It remains unclear what the long-term impact of this experience will be for many people who have VI.
Factors influencing vulnerability and resilience
Although the literature in this review does not always support the view that there is an increased level of loneliness among people who live with VI, it does consistently identify multiple ways in which they experience isolation and exclusion. A range of variables are identified as influencing the relationships between isolation, loneliness, and VI and these can provide information about factors, which may promote resilience and conversely, vulnerability in indicating whether an individual with a VI experiences loneliness. Individual psychosocial factors potentially play a pivotal role in how someone responds to the challenges of living with VI (Bulk et al., 2020; Kim & Sutharson, 2023). Zapata (2022) highlights the importance of people’s acceptance towards their VI and being able to incorporate it as a part of their life experience and identity. The concept of positive group identity (PGI) describes this idea of a person having a non-judgemental attitude towards all aspects of their life, including their VI and being able to embrace their experience and find value, which is not qualitatively better or worse than the life experience of sighted people, just different. In research, Zapata found that a more positive group identity in research participants with VI predicted increased life satisfaction as well as lower anxiety and depression (Zapata, 2022). In the report, VI lives (RNIB et al., 2022) evidence is presented that ‘mind-set is key’ as to how well people can respond to the challenges of living with VI both practically and emotionally. While people experiencing sight loss are likely to face difficulties in coming to terms with their condition, this report suggests how people adjust to these challenges is associated with their resilience, attitudes to life, and how open they are to the challenges they face. This points to the importance of the emotional journey people embark on in coming to terms with VI and the importance of the availability and accessibility of appropriate forms of support and counselling, where necessary, for people to be able to process their emotional responses and make that transition to a more resilient and accepting outlook (Kong et al., 2021; Thurston et al., 2010).
Veerman et al. (2019), in a longitudinal study of young adults with VI, explored whether differences in the social competence of participants could be a factor in predicting whether they would experience loneliness later in life. They found participants who exhibited lower social competence went on to have a higher incidence of loneliness at a follow-up study 6 years later, which was mediated by the level of emotional stability participants had. Lower emotional stability was theorised as being a contributor to increased social anxiety, leading to decreased social competence and subsequent loneliness. The impact of internalised self-stigma, described previously in the report, may also play a part in reducing the ability of people with VI to be able to make this transition towards acceptance and may be an important part of preventing or alleviating a tendency towards chronic loneliness (Bulk et al., 2020; Kong et al., 2021).
The use of technology and social media has been studied as a potential means of reducing loneliness and isolation for people with VI. Hill et al. (2021), in interviews with 10 individuals with VI who regularly used social media, found this was helpful for making and maintaining contacts with other people and being able to feel more in control of their social experience. However, there were issues with the quality of those relationships in relation to their authenticity. A further drawback of social media use was the high prevalence of visual image–based material making up the content of many platforms, which was not accessible and contributed to experiences of feeling excluded and isolated. Some participants reported it allowed them to connect with other people with VI and receive forms of practical and emotional support, which they were unable to receive from sighted people who did not understand the experience of living with VI. Similar results were found in a qualitative study of people who had acquired sight loss in Nigeria, with participants noting the benefits of social media in allowing them to remain connected with social networks, access sources of information and support, and develop new relationships. However, this research also found frustration among participants whose VI had resulted in them being no longer able to access social media and highlighted the importance of assistive technology being available in allowing people with VI to access online materials (Meribe et al., 2023).
Research by RNIB et al. (2022), also highlights the importance of technology in being a key enabler for people with VI in a range of domains including navigating journeys and employment. It notes there are wide disparities in the use of technology among people with VI due to awareness of the available products and differing abilities in being able to access it.
Related to the resilience of individuals is the ability to be able to make connections and find meaning in alternative ways. Connections with nature are widely believed to be particularly nourishing for people in providing emotional support and being effective in assisting recovery from and preventing the occurrence of a wide range of physical, emotional, and psychological difficulties. An example of this comes from a qualitative study on the interactions with wild birds, from which people with VI were able to cultivate and gain significant value and pleasure (Bell, 2021). This article further highlights the importance of mind-set and the value in being able to cultivate meaning and connection from a wide variety of potential sources.
Conclusion
Consistent with Hodge and Eccles (2013), this review finds the correlation between VI and loneliness is inconsistently demonstrated across the studies. Although reports of isolation and exclusion were prevalent among people with VI, subjective experiences of loneliness did not necessarily align with this. The relationship between VI and loneliness is influenced by numerous moderating and mediating factors. Some life circumstances can heighten vulnerability to loneliness, such as being single, living by oneself, being unemployed, being in a financially unstable situation, or having low disposable income, all of which disproportionately affect the VI community compared to the general population (RNIB, 2017; RNIB et al., 2022). Research has yet to fully understand the interplay of these and experiences of loneliness and isolation for people with VI within LGBTQ+ communities and within Black, Asian, and Ethnically Minoritised communities, where research remains notably scant (Heinze et al., 2023). Studies about the impact of the COVID-19 pandemic showed its heightened effect on isolation and loneliness among the VI community. Further research is needed to understand the long-term effects of this. While technology holds promise in mitigating loneliness and isolation among individuals with VI, accessibility issues persist. Future research is needed to understand how technology-based interventions might address loneliness and isolation for individuals with VI and the accessibility barriers associated with the implementation of these. Finally, people with VI are not a homogeneous group and, like any other population, they have a wide range of likes, dislikes, interests, priorities, and passions. For loneliness and isolation to be minimised, recognising the diversity within the VI population is imperative for tailoring interventions and initiatives effectively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Vision Foundation/Fight for Sight.