
Abstract
The World Health Organization created the International Classification of Functioning, Disability and Health (ICF) to provide a common framework to understand and describe functioning and disability. To make the ICF more applicable for everyday use, an ICF core set can be developed. We are going to reduce the entire ICF of 1400 categories to essential categories that can be used in a specific health context. These ICF core sets are created through a scientific process based on preparatory studies and the involvement of a multidisciplinary group of experts. The aim of this project is the development of an internationally accepted, evidence-based and valid ICF core set for irreversible vision loss. This article describes the process that is followed in detail and invites stakeholders to participate in the development.
Introduction
Vision accounts for about 80% of the function of all five senses combined. That is why vision plays an important role and leads to restrictions in all areas of life when impaired. In almost all activities related to participation in social life, such as religion, mobility, recreation, and daily living, intense visual tasks are commonly required (Yibekal et al., 2020). Individuals with visual impairment are at risk of disability, poor health, unemployment, low financial income, and adverse interpersonal events (Brunes et al., 2019). Persons with visual impairment experience difficulties with forming and maintaining social relationships. This difficulty challenges their psychosocial functioning and results in a sense of loneliness (Veerman et al., 2019). Research from K. Yang and Victor (2011) has shown that these problems are not only experienced by older adults but also by young people with vision loss.
From a global perspective, out of the 733 billion people alive in 2015, an estimated 36 million were blind, 2166 million people had a moderate to severe visual impairment, and 1885 million had mild visual impairment. Older adults (aged ⩾ 50 years) have the largest burden of vision impairment (Bourne et al., 2017). Looking at the geographical distribution, researchers have observed that 90% of the world’s individuals with visual impairment live in developing countries (Yibekal et al., 2020). The distribution of eye conditions varies across regions, income levels, and ages. Several eye disorders, including cataract, presbyopia, glaucoma, and age-related macular degeneration increase with age (World Health Organization [WHO], 2019).
The International Classification of Diseases divides visual impairment into two groups: distance and near. A distance visual impairment varies from mild (presenting visual acuity less than 6/18 in the better eye), moderate (less than 6/18 to 6/60 in the better eye), severe (less than 6/60 to 3/60) to blind (less than 3/60 or no light perception). For near vision, the definition is acuity worse than N6 or N8 at 40 cm and best-corrected visual acuity ⩾ 6/12.
The most common global causes of visual impairment are refractive errors, age-related causes, infectious causes, nutritional and metabolic causes, and trauma. Cataract and under-corrected refractive errors are the leading causes of blindness and moderate and severe visual impairment in all world regions in the age group of 50 years and older. The occurrence of glaucoma and age-related macular degeneration increases with age, while the contribution of diabetic retinopathy to blindness decreased with age (Bourne et al., 2017; Vision Loss Expert Group of the Global Burden of Disease Study, 2020; WHO, 2019).
Visual impairment is not only a problem for the individual; it is also a global public health problem which leads to a variety of public health, social, and economic problems. Common additional health problems in persons with vision loss are anxiety, depression (van der Aa et al., 2015), fatigue (Schakel et al., 2019), and bone fractures after a fall (de Boer et al., 2004; Hong et al., 2014).
Because of demographic changes and the aging population, the number of people with irreversible visual impairment is expected to rise in coming decades (Vision Loss Expert Group of the Global Burden of Disease Study, 2020). Population aging will impact the number of people with eye conditions significantly. By 2030, the number of people worldwide aged 60 years and over is estimated to increase from 962 million in 2017 to 1.4 billion, while numbers of those over 80 years of age will increase from 137 million in 2017 to 202 million. These population changes will lead to considerable increases in the numbers of people with major eye conditions that cause vision impairment (WHO, 2019).
Vision loss has been ranked third, behind arthritis and heart disease among the most common chronic conditions that require older adults to have assistance with activities of daily living. Visually impaired older adults participate less than their peers because of the restriction in activities such as mobility, reading, hobbies, and social interactions (Van Nispen, van der Aa, et al., 2019).
This implies increasing pressure on visual rehabilitation services (Condon et al., 2004; Keunen et al., 2011; Limburg, 2007).
Based on the rationale described above, to understand the full impact of a vision impairment it is important to use a holistic approach, because this has a lifelong influence on the patient and his or her environment. In the past years, many theoretical frameworks have been developed that describe human functioning.
We find this holistic approach within the International Classification of Functioning, Disability and Health (ICF). The ICF was endorsed in 2001 by the World Health Organization (WHO) for use as an international standard to describe and measure health and disability. ICF offers a theoretical framework by integrating the social model and the medical model into a bio-psycho-social model. The ICF is also a classification system, with alphanumerical categories that not only looks at the health condition, but recognizes the role of the environment in the creation of a disability. ICF is a bio-psycho-social model where there is an interaction between different components, as shown in Figure 1.
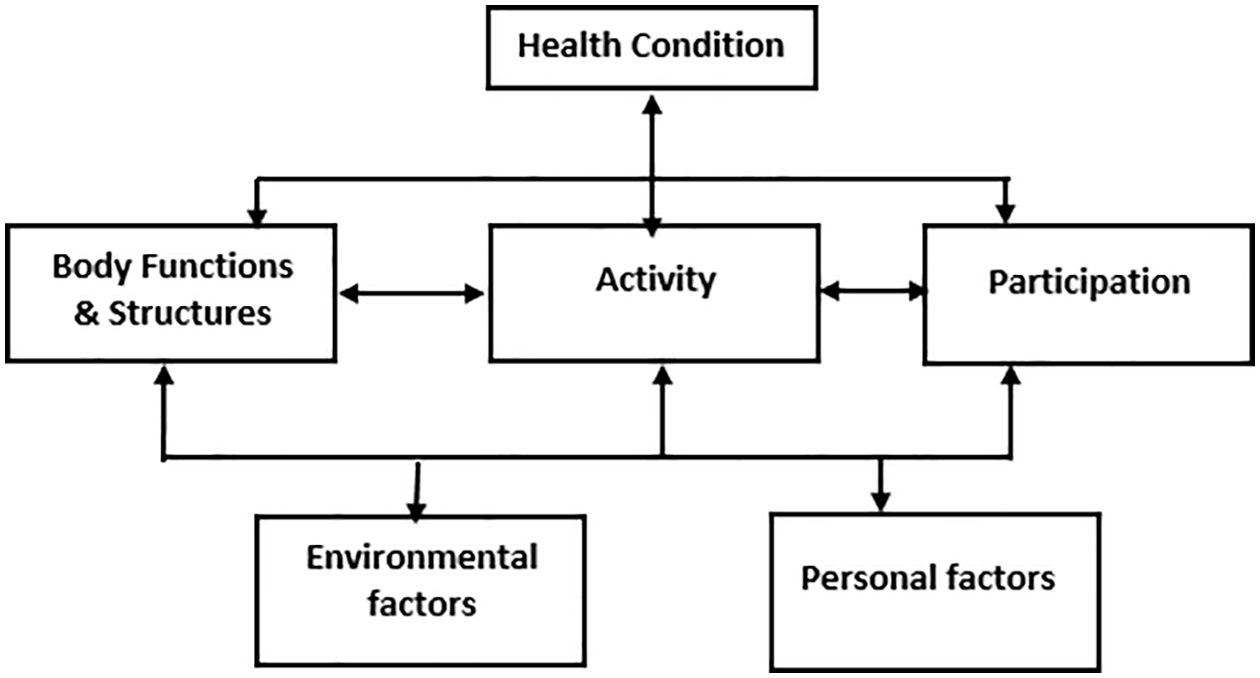
Illustration of the ICF domains.
The ICF components have multiple hierarchical domains: body functions (b), body structures (s), activities and participation (d) and environmental factors (e), organized by over 1400 categories (WHO, 2001).
The first domain is focused on the anatomical parts of the body and the physiological functions and systems. Where activities focus on the execution of a task or action by an individual, participation focuses on one’s involvement in a life situation. Contextual factors are also important as they focus on the personal and physical and the social and attitudinal environment.
This is a widely used model in rehabilitation medicine and paramedical care. The expertise centers for people with visual impairment in the Netherlands and Belgium make frequent use of the ICF for adults to map out requests for help and classify interventions (Van Nispen, Van der Ham, et al., 2019).
The objective of this discussion paper is to outline the process to develop the ICF core set for vision loss and to invite experts from all over the world to participate in this process.
Aim
The aim of this project is the development of an internationally accepted, evidence-based, reliable, and valid ICF core set for vision loss in (older) adults which is both comprehensive and brief. In the development of the core set, the focus is on irreversible eye conditions such as age-related macular degeneration, glaucoma, diabetic retinopathy, and hereditary eye diseases.
A comprehensive ICF core set is a list of ICF categories that includes as concisely as possible the typical spectrum of problems in functioning for persons with irreversible vision loss. A brief ICF core set is a list of ICF categories that serves as a minimal data set that can be collected and reported in any clinical study and which provides a standardized description of an individual’s experience with a certain disease or disability. The ICF core set for vision loss in (older) adults can provide an overview of the aspects of functioning that should be assessed to get a complete picture of the level of functioning of an individual with vision loss. This overview can be translated into various assessment instruments, such as questionnaires, rating systems, structured interviews, and observation scales, depending on the needs and wishes of the user. Because the assessments are based on the core set, it will be possible to translate them back to the ICF categories. It is expected that the ICF core set for vision loss will allow comparison of data across disciplines and countries.
Methods
An ICF core set is a purpose-tailored shortlist of ICF categories that describe the functioning and disabilities of a specific group of people. There is a selection of essential categories from the full ICF classification that are considered most relevant for describing the functioning of a person in a specific health care context. In this way, the ICF core set can be a useful tool to increase supply-driven rehabilitation and not just by demand.
At present, 34 ICF core sets have been developed, including only one with a focus on the sensory aspect of the eyes (Danermark et al., 2013). The most current overview of the core sets already developed can be found on the website of the ICF Research Branch https://www.icf-core-sets.org (International Classification of Functioning, Disability and Health Branch, 2017).
The core set will be developed in a three-phase process that is predefined by the WHO: (1) preparatory phase, (2) an international consensus conference, and (3) the validation phase where we validate and test the ICF Core set (see Figure 2).
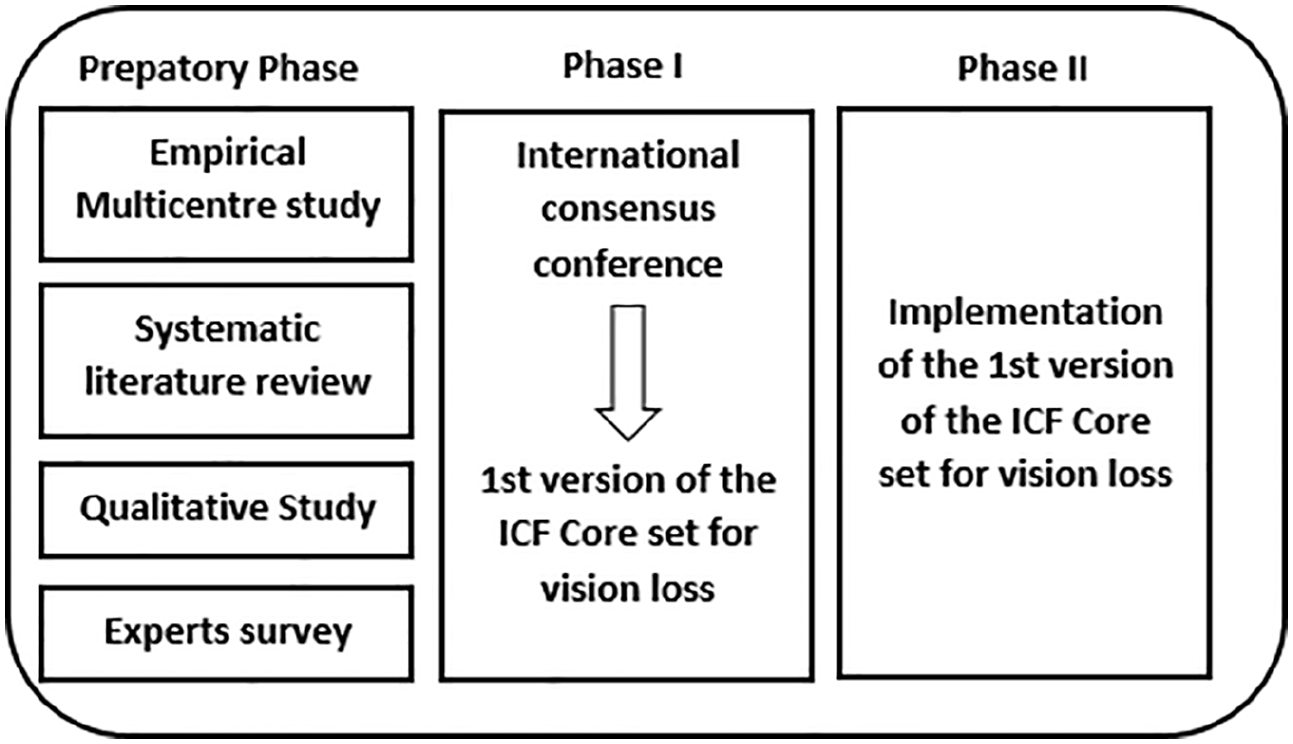
Phases of the project (Selb et al., 2015).
This makes it possible to follow a sufficiently evidence-based process that not only includes the point of view of health workers, but also that of the target group for which the ICF core set is being developed. The end result must be culture- and context-neutral so that it can be implemented within the different WHO regions (Selb et al., 2015).
Preparatory phase
The first phase consists of a systematic review and a qualitative in-depth study to map patients’ and experts’ perspectives.
Systematic review
The objective of the systematic review is to identify variables that are important for persons with a visual impairment and map them to the conceptual framework of the ICF. To start the systematic review, we followed the established procedure that has been used in the development of previous core sets.
To identify all relevant publications, we conducted a systematic search in different bibliographic databases: PubMed, Embase.com, CINAHL, APA PsycInfo, and Web of Science, from 2001 up to 2020. The following terms were used (including synonyms and closely related words) as index terms or free-text words: “Visually impaired persons,” “Low vision,” “Quality of life,” “Questionnaires,” “Surveys,” and “Adults.”
The second step is screening the abstracts to determine if they meet the inclusion criteria. The first 10% of all articles will be read by two independent investigators. In the last step of the systematic review, all articles will be read and linked to the ICF categories by using standardized linking rules (Cieza et al., 2005).
Qualitative study
To identify ICF relevant concepts for persons with a visual impairment, it is important to include the perspective of clients. Personal values will vary over time, between and within individuals.
First, information will be collected from focus groups in Belgium and the Netherlands. A varied set of questions will be set up to cover the components of the biopsychosocial model to guide the discussion in groups of 4–6 persons under the supervision of a moderator. To compose the focus groups, we will follow the maximum variation strategy based on the following criteria: age, sex, and degree of vision loss. Participants will be included in the focus groups until saturation is reached. The written transcription of the focus group discussion will be analyzed to identify important concepts for clients.
If some individuals are unable to take part in a focus group due to the severity of their condition, individual interviews will be carried out. To enrich the qualitative study with information from other WHO regions, an online survey will be set up.
Expert surveys
To investigate the opinions regarding aspects of visual functioning, activities, and participation, an international pool of experts will be invited to participate in an Internet-based survey. The pool will include experts from various disciplines (ophthalmologist, teachers, occupational therapists, low vision therapist, psychologists, occupational therapist, and social workers) who have experience in working with people with vision loss and from each of the six WHO regions (Europe, The Americas, Africa, Eastern-Mediterranean, South-East Asia, and Western Pacific).
Cross-sectional study
For the cross-sectional study, participants will be recruited from various regions of the world to incorporate an international perspective.
Phase I: consensus conference
This phase of the project involves the organization of an international consensus conference to present the information collected during the preparatory phase. The aim of this conference is to reach a consensus on an internationally accepted ICF core set for vision loss in adults and older people. The group will be composed in a way that the whole group of participants is representative with a view to expertise and international representation. It will be a group of 21–25 experts in the field of vision loss. To be sure everyone use the same terminology, the participants will receive training in the ICF philosophy and methodology followed by an iterative decision-making process. The decision-making and consensus process will use the nominal group technique.
Phase II: validation
The logical next step is bringing the core set into practice. Over the past few years, operationalization of ICF Core Sets for use in clinical practice occurred in different domains. Examples are the Brief Core Set Questionnaire of Breast Cancer for Screening in cancer care (E. J. Yang et al., 2014), the Work Rehabilitation Questionnaire for vocational rehabilitation (Finger et al., 2014), and the health index for patients with ankylosing spondylitis (Kiltz et al., 2015).
Ethics
The procedure will be conducted in conformity with the ethical principles of the Declaration of Helsinki. All documents will be presented to the corresponding Ethics Committees and informed consent will be collected from participants in the study.
Discussion
This paper describes the methodology we will follow to develop an ICF core set vision loss by (older) adults. The core set should allow clinicians and researchers to classify and describe an individual’s structure, functioning, activity, and participation using the most relevant ICF codes. It is a tailored ICF that can be useful for dealing with patients with vision loss. A brief ICF core set for vision loss will facilitate international studies, and a comprehensive core set could be used in the clinic as a checklist to assess individual needs, formulate rehabilitation goals, evaluate the progress of rehabilitation or assess progress. The complex problem of vision loss requires a multidisciplinary and multilevel assessment and intervention approach to improve function and quality of life. The developed ICF core set for vision loss can meet this need by providing a common basis for communication. It will give direction to what we measure instead of how, to reach this the implementation phase will be an important phase.
Invitation to participate
The development of the ICF core set for vision loss is an inclusive and open process. We would like to invite you to participate in the expert or the stakeholders survey. Anyone who wants to be involved during the development process can contact us. Individuals, institutions, and associations can be formally associated as project partners.