
Abstract
During the development of the Core Sets for deafblindness, using the World Health Organization’s (WHOs) International Classification of Functioning, Disability, and Health (ICF), the last preparatory study consists of a multisite cross-sectional clinical assessment. Its purpose is to use standardized tests of functioning that have been identified during a systematic literature review, and that have been most frequently used with deafblind individuals. These measures need to be available at no cost, standardized and validated, and not interfere with protected professional acts. Here, we explore the administration of the Mini-Mental State Exam (MMSE), the Lawton-Brody Instrumental Activities of Daily Living Scale, and the Center for Epidemiological Studies Depression Scale for this purpose. Participants were 29 deafblind adults (14 men, 15 women), ranging in age from 20 to 74 (M = 47.29, SD = 16.31), with a wide range of severity and diagnostic criteria, and from 15 countries distributed across the six WHO regions. They were invited to a structured online clinical assessment based on the ICF Check List of assessment categories, in addition to the administration of the three identified standardized measures. Participants demonstrated varying levels of independence in daily tasks, with the highest independence in managing laundry and medications and greater dependency in financial management and transportation. Nearly half (48%) showed signs of clinical depression. MMSE completion rates were low (n = 6), with significant non-responses in visually demanding items; among those who completed it, 67% scored within the normal range. A positive correlation between cognitive status and functional independence was found. These findings underscore the heterogeneity of deafblind individuals. None of these most frequently used measures were designed to be administered to individuals living with combined vision and hearing difficulties, underscoring the importance of tailored assessment tools and interventions to support this population.
The International Classification of Functioning, Disability and Health (ICF) is a comprehensive framework developed by the World Health Organization (WHO) to describe health and functioning across disabilities (World Health Organization, 2001). Officially endorsed by all 191 WHO Member States in 2001, the ICF serves as the international standard for measuring health and disability. It provides a holistic and biopsychosocial model of (dis)ability, integrating both medical and social models, thereby capturing an individual’s functioning, and develops a common language to describe health (World Health Organization, 2001). Since its inception, the ICF has been utilized for various purposes, including statistical analysis, research, clinical practice, social policy development, and educational initiatives. For instance, at the policy level, the framework can help provide a consistent definition of the disability condition that can be used to develop eligibility criteria for disability pensions, regulations for assistive devices, and policies for communication accessibility and accommodation (Kostanjsek, 2011).
The structure of the ICF is organized hierarchically into two main parts: functioning and disability, and contextual factors. These parts are further categorized into four interactive components: body structures and functions, activities and participation, environmental factors, and personal factors (World Health Organization, 2001). This approach allows for a holistic understanding of an individual’s health status, considering their health condition, their ability to function in society and the environmental factors that affect their daily life. Each component, except for personal factors, is classified into chapters, categories, and subcategories in a hierarchical structure. The ICF Core Sets, which are subsets of ICF categories, have been developed for various health conditions to describe functioning and disability more specifically (Bickenbach et al., 2012). These Core Sets have been developed for more than 30 health conditions, spanning musculoskeletal, neurological, cardiovascular, and respiratory domains (ICF Research Branch, 2017). These specialized Core Sets significantly improve the assessment of functioning by providing tailored, comprehensive, and standardized tools to clinicians for specific health conditions (Selb et al., 2015).
Specifically related to sensory loss, both comprehensive and brief Core Sets have been established for hearing loss (Danermark et al., 2010, 2013). Meanwhile, the development of Core Sets for vision loss is currently in progress, led by a team from the Netherlands (Billiet et al., 2021, 2024). In the case of deafblindness, Core Set development and validation is ongoing as well (Wittich & Dumassais, 2025). Deafblindness, a unique sensory disability characterized by combined hearing and vision impairment that significantly affect an individual’s ability to access information, communicate, and engage socially (Dammeyer, 2014, 2015). This condition is often categorized into congenital, acquired, and age-related deafblindness (Heppe et al., 2025; Jaiswal et al., 2018). Individuals with deafblindness often cannot compensate for the loss of one sense with the other, presenting distinct challenges (Dammeyer, 2014; Wittich & Simcock, 2019). In addition, deafblindness often presents together with other disabilities, such as cognitive-, motor-, and/or communication impairments, as is the case in CHARGE syndrome or many other complex conditions (Hartshorne & Slavin, 2023). As it turns out, Core Set development for long-term multimorbidity (including vision and hearing difficulties) is currently ongoing elsewhere (Bickton et al., 2025); therefore, the present project focuses on deafblindness alone, without considering comorbidities. The prevalence of deafblindness is estimated between 0.2% and 2% globally, increasing with age (Koesters et al., 2025; World Federation of the Deafblind, 2018). Despite its significant consequence on functioning, the effects of deafblindness are frequently underestimated, and individuals living with deafblindness face inequalities in human rights and access to appropriate support (World Federation of the Deafblind, 2018, 2023a, 2023b).
The development of ICF Core Sets for deafblindness was initiated in 2021 to provide health care professionals and researchers with tools to assess and document the functioning of individuals with deafblindness more efficiently. This process requires four preparatory studies (Selb et al., 2015), three of these studies have been completed: a systematic literature review representing the perspective of researchers (Jaiswal et al., 2024; Paramasivam et al., 2023), a qualitative study with individuals living with deafblindness providing insights into priorities from the perspective of lived experience (Wittich, Dumassais, Prain, et al., 2024), and an expert survey representing the perspective of professionals working in the field (Wittich, Dumassais, Jaiswal, et al., 2024). The fourth study, the empirical multicentre study, identifies problems experienced by individuals with deafblindness that are documented in a clinical setting. Data from this study included intake assessments of adults living with deafblindness, using the ICF Checklist, the results of which are presented elsewhere (Ogedengbe et al., 2025). In addition, the ICF Core Set development guidelines recommend including health condition–specific measures that are most used by experts – as identified through the systematic literature review – to comprehensively capture the spectrum of functioning associated with the condition under study (Selb et al., 2015). Ideally, these measures are available free of charge, standardized and validated, and do not fall within a protected professional act, such as, for example refraction for best corrected visual acuity. In the case of deafblindness, the literature review indicated that the three measures that fulfilled these criteria assessed the domains of cognition, mental health, and daily functioning (Paramasivam et al., 2023). Here, we report on the outcomes of administering these measures to a heterogeneous group of deafblind individuals, exploring both the qualitative process of administration, and the quantitative results.
Methods
This study received institutional review board approvals from the Comité d’éthique de la recherche Clinique of the Université de Montréal, Montreal, Canada (# 2023-4663) and the Instituto del Salud Carlos III (#CEI PI 44_2021-v3) in Madrid, Spain. The approvals ensured compliance with ethical standards for research involving human participants across all participating sites.
Participants
Participants in the study aged 18 and older, who experienced any form of deafblindness (congenital, adult-onset, age-related, or any combination thereof) were recruited to share their experiences related to functioning and disability. The study ensured representation from all six WHO regions – Africa, Americas, South-East Asia, Europe, Eastern Mediterranean, and Western Pacific – by including at least two participants from each area. This approach was designed to align with the WHO’s recommendations of global representation for developing the ICF Core Sets (Selb et al., 2015).
The study recruited individuals with deafblindness and/or their family members or caregivers, through the extensive global networks of Deafblind International and the European Deafblind Network. Various national organizations across Sweden, Spain, France, Argentina, Australia, New Zealand, India, Nepal, Tanzania, Uganda, Niger, Zambia, Egypt and the Netherlands further assisted in the recruitment of participants from their region. In Canada, recruitment was supported by partners providing services to people with deafblindness, including Deafblind Ontario Services, Canadian National Institute for the Blind Deafblind Community Services, and the Canadian Hellen Keller Centre. This comprehensive approach ensured wide-ranging global data collection, tapping into diverse resources and expertise in the field of deafblindness.
Materials
Twenty-nine participants with deafblindness were interviewed by one of two clinical researchers (an occupational therapist or a speech language pathologist). The interviews utilized three standardized assessment tools.
The Mini-Mental State Examination/MMSE (Folstein et al., 1975) is a widely used cognition screening tool, with subscales for orientation (0–10 points), registration (0–3 points), attention (0–5 points), recall (0–3 points), language (0–8 points) and copying (0–1 point). Scores on the MMSE range from 0 to 30, with higher scores indicating better cognitive function (Folstein et al., 1975; Lach et al., 2020). This tool has demonstrated a sensitivity coefficient of .87 and a specificity coefficient of .82 for detecting cognitive impairment (Parada et al., 2021). The MMSE language section evaluates various aspects of language ability, including naming objects, repeating phrases, following commands, obeying instructions, and writing a sentence.
The Lawton-Brody Instrumental Activities of Daily Living/IADL Scale (Lawton & Brody, 1969) was used to measure functional independence across various activities. This scale examines eight items: ability to use telephone, shopping, food preparation, housekeeping, laundry, mode of transportation, responsibility for own medications, ability to handle finance. It has a validity coefficient of .85 and reliability coefficients ranging from .87 to .91 (Carmona-Torres et al., 2019). For each category, participants’ highest functional ability is recorded as either 0 (dependent) or 1 (independent). In the traditional scoring method of this questionnaire, women receive a summary score ranging from 0 (low function, dependent) to 8 (high function, independent), while men receive a score ranging from 0 to 5. To minimize potential gender bias, which could arise from differences in tasks traditionally performed by men and women, all items on the scale were included for every participant in this study. Consequently, the total scores range from 0 (indicating complete dependence) to 8 (indicating full independence).
Depression symptoms were assessed using the 10-item Center for Epidemiologic Studies Depression Scale (CESD; Radloff, 1977), consisting of 20 items measuring the frequency of symptoms experienced over the past week. It has response options ranging from 0 to 3: 0 = rarely or none of the time (less than 1 day); 1 = some or a little of the time (1–2 days); 2 = occasionally or a moderate amount of the time (3–4 days); 3 = most or all the time (5–7 days). The total score ranges from 0 to 30, with higher scores indicating more severe depression symptoms. We used a cut-off point of ⩾16, suggesting the presence of depression symptoms (Parada et al., 2021; Rong et al., 2020).
These three specific measures were used because they emerged during the systematic literature review as the three most frequently used questionnaires in research with participants living with deafblindness that are validated and available at no cost (Paramasivam et al., 2023). The MMSE had been used in 15 studies with deafblind participants, the IADL in 17 studies, and the CESD in 24 reports (Paramasivam et al., 2023). Furthermore, they were selected for their reliability, validity, and widespread use in clinical and research settings. Quantitative analyses were conducted using Jeffreys’s Amazing Statistics Program (JASP Team computer software, Version 0.18.3).
Procedure
Informed consent was obtained from all participants, with special attention given to making the consent process accessible to individuals with deafblindness (Paramasivam, Jaiswal, Minhas, Wittich, & Spruyt-Rocks, 2021; Wittich et al., 2023). Accommodations were provided during the preparation for consent and during the consent itself, as well as during the study procedure. These included but were not limited to early provision of consent materials in plain language, accessible formats and alternate formats (e.g., interpreter assisted clarifications tailored to individual questions or procedural needs). Written, verbal or recorded consent were secured during the initial consultation interview, prior to the functional assessment. Participants self-reported any co-occurring diagnoses. To ensure confidentiality, all personal information was coded and stored on a secure server (OneDrive) at the Université de Montréal with restricted access to the immediate academic research team.
Semi-structured interviews using the standardized scales were conducted by trained team members: an occupational therapist (author AJ) or a speech language pathologist (author MP). Interviews took place either in person or via secure Zoom sessions, which were recorded using the platform’s built-in feature (Zoom Video Communications, San Jose, California, USA). All interviews were conducted in English, either directly with the participants, through a sign language interpreter who could speak English, and/or with a translator or family member who could translate to/from a local language, as needed to accommodate participants’ preferred communication modalities. Of the 13 interviews conducted with the help of interpreters, five used American Sign Language, one used Québec Sign Language (Langue des signes Québécoise), while the remaining interviews were conducted using professional trained sign language interpreters in local language of the country of the participant in countries within Africa and South-East Asia. The interpreters (sign language as well as local language) had work experience in the field of deafblindness and were professionally trained in their country along with knowledge of American Sign Language and/or their locally signed language. Local language signing was preferred and used to facilitate the communication with participants so that they would feel more comfortable and had a better understanding of the interview questions. Interviews were recorded for quality control, in case individual responses needed to be revisited after the interview. Participants, family members, and informal communication facilitators received $50 CAD compensation for their participation. Professional interpreters were compensated at their standard professional rates.
Results
A total of 29 participants, living with deafblindness, took part in the study, including 14 men and 15 women, with ages ranging from 20 to 74 years (M = 47.29, SD = 16.31). Thirteen interviews were conducted through interpreters, while 16 were conducted directly with participants. Other communication supports included sitting close to the ear with better hearing, ensuring a quiet environment and repeating some questions. Table 1 presents the demographic characteristics of the study sample. The results are presented in four main sections: the IADL scale, the CESD scale, the MMSE and the Correlation Analysis.
Baseline demographic characteristics (n = 29).
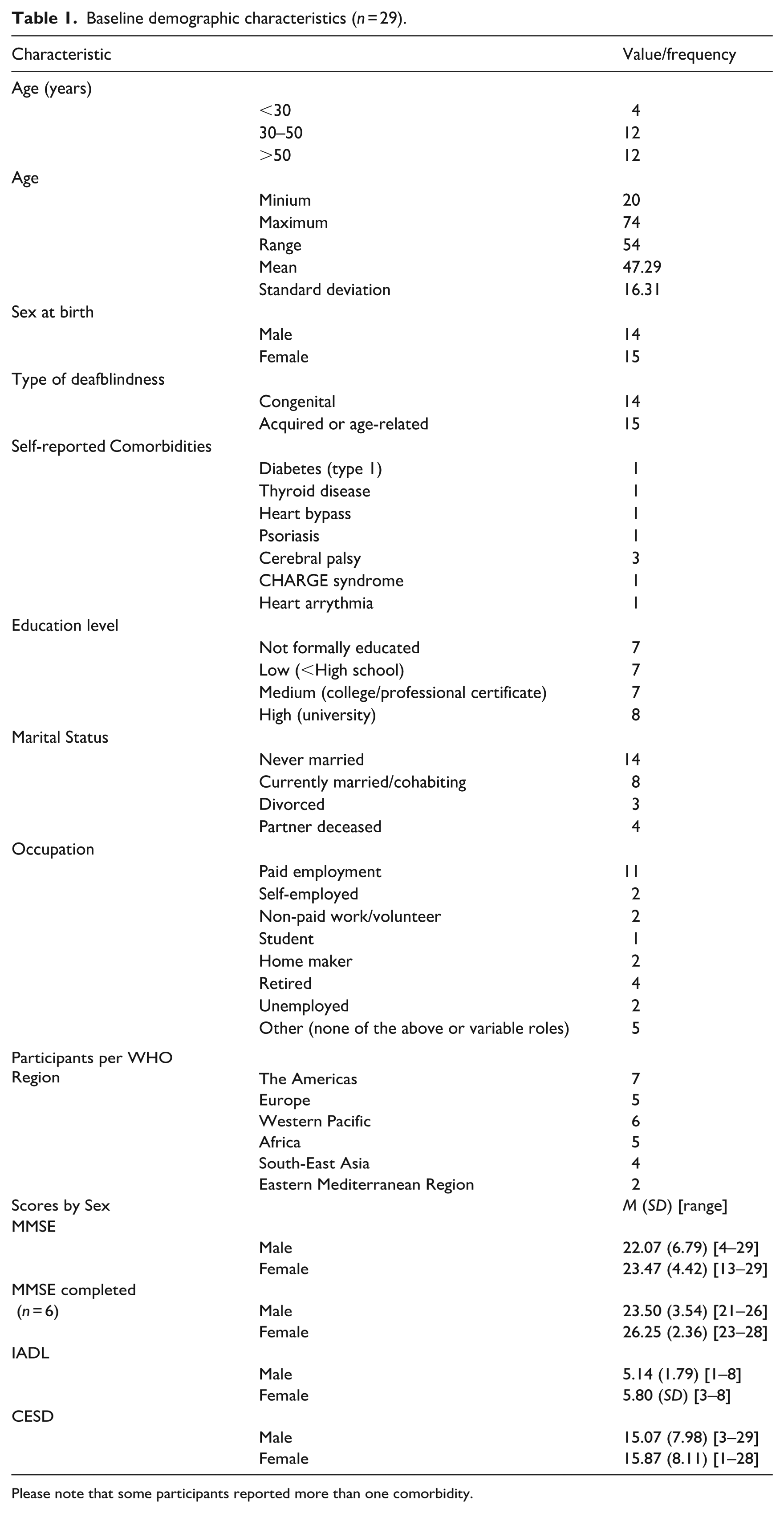
Please note that some participants reported more than one comorbidity.
MMSE
Thirty-eight percent of participants did not perform the object-naming task related to naming objects, 10% of participants did not perform the tasks related to repeating phrases, following commands, and obeying instructions, and 69% of participants did not perform the sentence-writing task. These findings indicate that the highest non-response rate was for the sentence writing task, with 69% of participants failing to perform the task. Conversely, tasks such as repeating phrases, following commands, and obeying instructions had the lowest non-response rate, at 10%. Ultimately, only six participants were able to complete all the items in this measure. The distribution of MMSE scores among the six participants who completed the questionnaire was as follows: 67% (n = 4) (scores > 24) exhibited normal cognitive function, 33% (n = 2) had scores suggesting mild cognitive impairment (scores 19–23), none had scores suggesting moderate cognitive impairment or severe cognitive impairment (scores 0–18).
Lawton-Brody IADL Scale
The data distribution for men and women did not demonstrate a significant deviation from normality (Shapiro–Wilks’ test) and did not violate the assumption of equality of variance (Brown-Forsythe test). The Mann–Whitney test did not reveal any statistically significant difference between men and women on the Layton-Brody IADL total scores, U = 86.5, p < . rpb = –.176. The wide variability of raw scores is presented in Figure 1, with men represented in black and women in white. Regarding the frequency of answered questions, several findings emerged (Figure 2). The participants displayed a range of capabilities in managing their finances. Five participants (17%) were incapable of handling money, while the majority managed day-to-day purchases but required assistance with banking and major purchases (n = 14, 48%). Notably, 10 participants (34%) managed their financial matters independently, including budgeting and paying bills. Medication management showed a higher level of independence among participants compared with other categories. Only one participant (3%) was unable to dispense their medication, while the majority (n = 18, 62%) were responsible for taking their medication. In terms of transportation, most participants required some form of assistance; 14 participants (48%) travelled with assistance, seven arranged travelled independently, seven (24%) arranged their own travel via taxi, and four participants (14%) travelled independently on public transportation or drove their own car. Laundry tasks were predominantly handled independently by participants. Only three participants (10%) required others to do all their laundry, and a substantial majority (20 participants, 69%) did their personal laundry completely independently. Housekeeping abilities varied among participants. A considerable number (n = 10, 34%) performed light tasks such as dishwashing and bed making, while another ten participants (34%) maintained the house alone with occasional assistance for heavy work. Food preparation abilities also showed variability. Eleven participants (38%) prepared meals independently, eight (28%) needed ingredients provided. Shopping independence was limited among participants, whereby 16 (55%) needed assistance, and 10 (34%) shopped independently for small items. Finally, 20 (69%) of participants used the telephone independently.
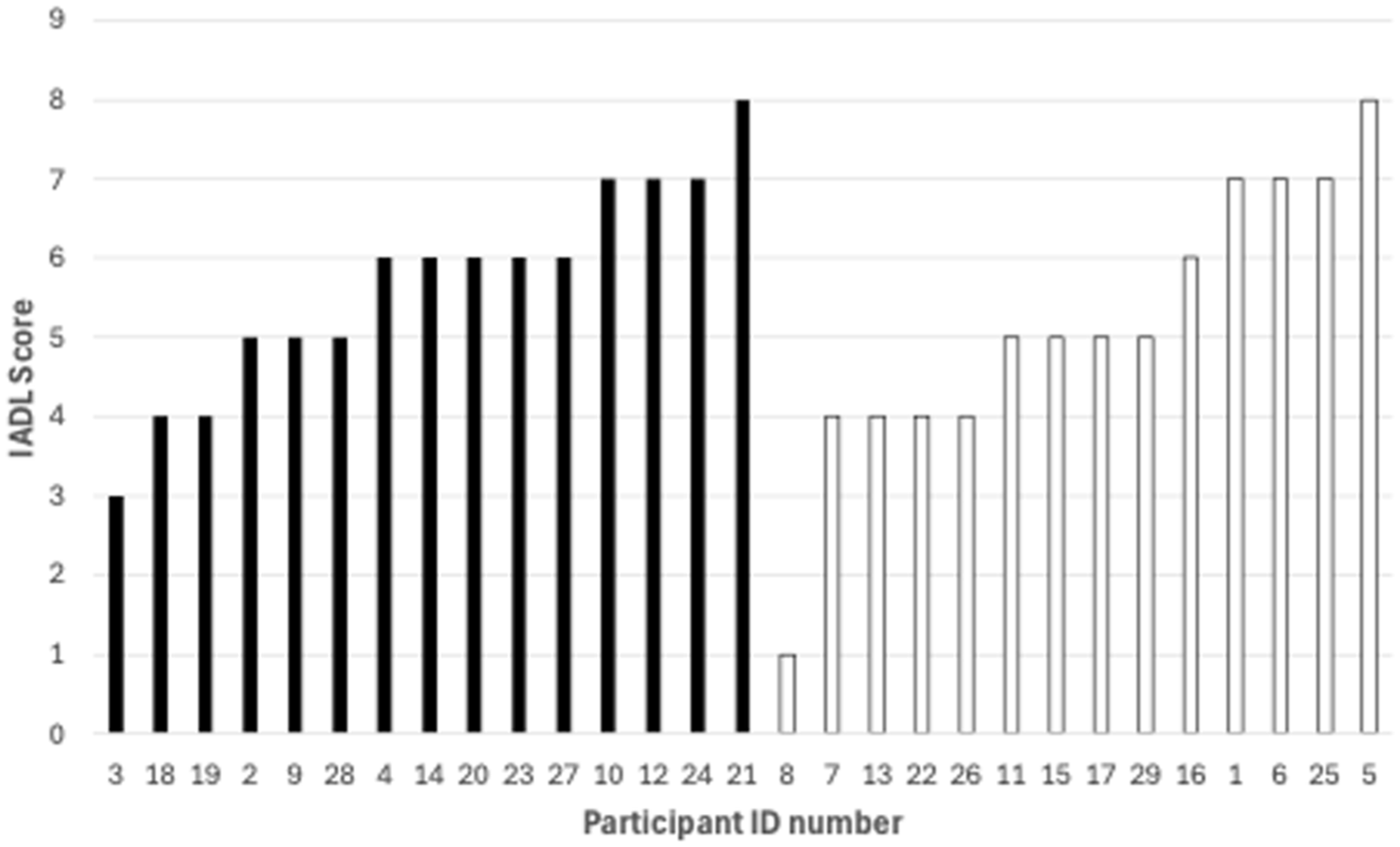
Total Lawton Browdy Questionnaire Scores for 29 participants: the x-axis represents participants grouped by gender, while the y-axis shows the scores ranging from 1 to 8. Women (black bars) represented on the left and men (white bars) on the right. Scores range from 1 to 8 for all participants, indicating varying levels of independence in daily living activities.
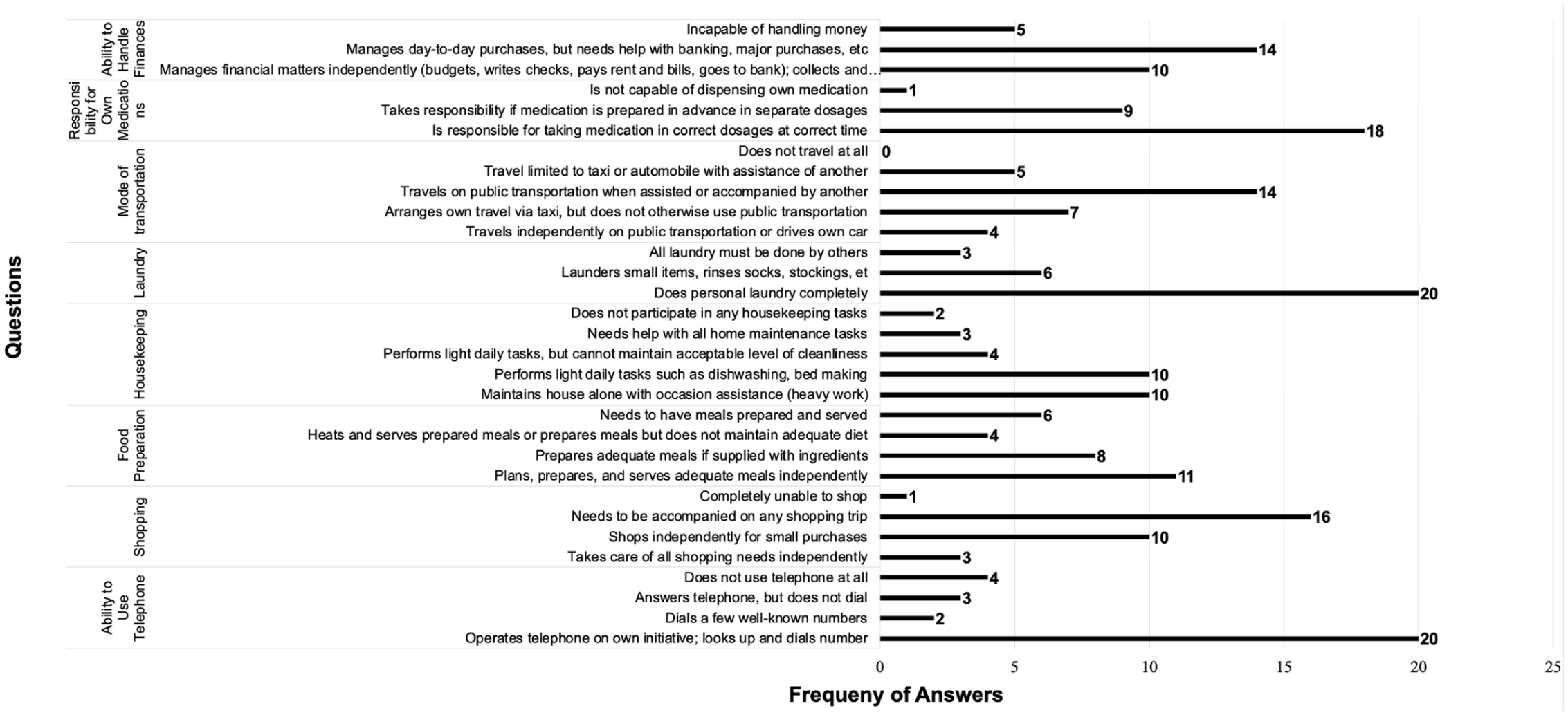
Bar chart depicting the distribution of responses to IADL-related questions, highlighting varying levels of independence among participants in tasks such as managing finances, transportation, housekeeping, and food preparation.
CESD Scale
The data revealed that 48% of participants, equally split between men and women, had scores of 16 or higher, indicating that they may be at risk for clinical depression.
Correlation analysis
Pearson’s correlation coefficients were calculated to examine the relationships among the questionnaire variables and the age of the participants (Table 2). There was a significant positive correlation between IADL scores and MMSE scores using all available data (n = 29), even when some MMSE items were missing (r = .585, p < .001), whereby higher IADL scores were associated with higher MMSE scores. When reducing the data set to the n = 6 individuals who were able to complete all MMSE items, this correlation remained significant (r = .821, p < .05). There were no significant correlations identified among IADL, CESD, MMSE, completed MMSE, and age.
Pearson correlation coefficients among age, IADL, CESD, and the MMSE (partial and complete) scores.
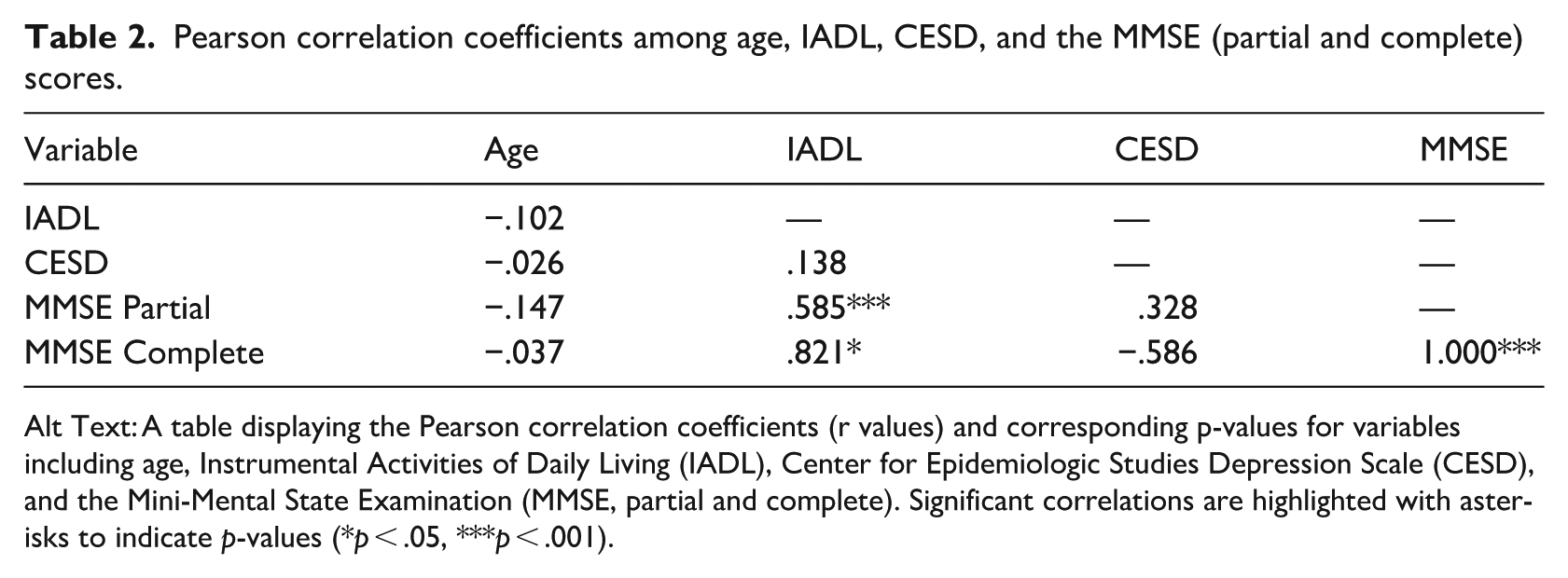
Alt Text: A table displaying the Pearson correlation coefficients (r values) and corresponding p-values for variables including age, Instrumental Activities of Daily Living (IADL), Center for Epidemiologic Studies Depression Scale (CESD), and the Mini-Mental State Examination (MMSE, partial and complete). Significant correlations are highlighted with asterisks to indicate p-values (*p < .05, ***p < .001).
Finally, independent samples t-tests compared men and women on the questionnaire scores of the IADL, CESD and MMSE (both those with missing scores, and those with all items completed). However, there were no statistically significant differences.
Discussion
The purpose of this study was to conduct an empirical multisite assessment using the most frequently used and freely available standardized clinical tools that have been utilized in research to date to evaluate adults with deafblindness. As the final step towards the development of the ICF Core Sets for deafblindness, these assessments inform the consensus process when the final selection of eligible categories occurs (Wittich & Dumassais, 2025). The domains assessed by these tools were functional independence, depression, and cognitive status. The study sample of individuals with deafblindness shows a diverse demographic and functional profile. Educational backgrounds varied widely, and this international group of participants spanned multiple WHO regions. These demographic insights are crucial for contextualizing the study’s findings and understanding the varied experiences of individuals living with deafblindness. Importantly, this diversity is not only a feature but a core strength of the study, especially in the context of ICF Core Set development. While the level of diversity and number of participants might be considered a limitation in conventional studies, in the present context, they align with the study’s primary goal – capturing a broad range of clinical experiences to inform inclusive and representative Core Set development.
An important consideration when interpreting the results is that the three measures that emerged from the systematic literature review, to be included in the Core Set development process, were not specifically developed to be administered to deafblind individuals. This aspect is important because none of these scales specifically consider the presence of a single or combined sensory impairment, neither during the administration (e.g., for accessibility reasons), nor for content (e.g., to contain items that consider the presence of sensory difficulties), nor during scoring (e.g., adjustments according to severity of sensory difficulty). Measures such as the IADL scale or the GDS require responses on a Likert-type scale; however, conceptually, such a scale is at times difficult to understand for individuals who communicate using a signed language. A scale from 0 to 10 does not easily make sense, and sign language responses cannot easily be converted into such a scale format (Bosch-Baliarda et al., 2019).
MMSE
More difficult, however, was the administration of the MMSE. While this screening tool is widely used in geriatric and neurological assessments, it was originally developed for sighted and hearing individuals. Its use with participants who are deafblind presented multiple methodological challenges. Tasks such as sentence completion, object-naming, and written responses inherently require sensory input that may not be accessible to individuals with combined vision and hearing loss. This mismatch likely led to elevated non-response rates on certain items, potentially underestimating participants’ cognitive abilities and misrepresenting their true capacities. Moreover, the MMSE may fail to capture the full spectrum of cognitive strategies and compensatory mechanisms used by individuals with deafblindness. This barrier highlights the urgent need for the development and validation of cognitive assessment tools that can be adapted when needed and accommodate the heterogeneity of the deafblind community.
The findings from the current study highlight some critical issues regarding participant’s ability to perform tasks and response rates, particularly in tasks requiring written responses. The high non-response rates in naming objects and sentence-writing tasks are a clear reflection of issues that stem from sensory limitations rather than cognitive problems, raising concerns about the MMSE’s effectiveness in fully measuring participants’ abilities. Aligned with this study, Hong et al. (2016) also found no significant link between sensory impairment and a decline in MMSE scores after adjusting for age, sex, and other factors. The MMSE was not designed to effectively detect cognitive decline in this population. Be that as it may, the mechanisms linking sensory loss to cognitive decline are not well understood (Ge et al., 2021) and reduced cognitive function and sensory impairment may coexist without a clear causal relationship (Ge et al., 2021; Hong et al., 2016). Both vision and hearing impairment have been identified as potentially modifiable risk factors for dementia, highlighting the importance of sensory status for cognition (Ge et al., 2021; Livingston et al., 2024). Therefore, the assessment of cognition in persons with deafblindness remains an important research priority.
IADL
The results indicate a diverse range of independence levels among participants highlighting the heterogeneity of experiences among individuals with deafblindness. These findings also propose that, while certain tasks remain manageable (e.g., medication and laundry) others, such as handling finances, transportation and shopping present significant challenges. Previous research has demonstrated that maintaining independence is a top priority for this population (Mueller-Schotte et al, 2019). A decline in IADL such as handling finances, grocery shopping, or walking can therefore jeopardize this independence and lead to difficulties in self-care tasks like toileting or bathing (Mueller-Schotte et al., 2019). The IADL assessment provided a comprehensive overview of a variation in functional abilities of individuals with deafblindness, highlighting the importance of providing tailored support and interventions to meet the unique needs of each person with deafblindness, rather than relying on a one-size-fits-all approach. Targeted support in areas where participants showed lower independence, such as handling finances and transportation, could significantly improve their overall quality of life (Heine et al., 2019). The successful completion of most individual IADLs requires adequate visual (e.g., meal preparation) and auditory abilities (e.g., using the telephone, travelling) (Mueller-Schotte et al., 2019). Hearing and vision difficulties can limit access to environmental information and hinder communication, possibly contributing to financial and mobility difficulties and ultimately social isolation, thereby placing an individual’s independence and overall well-being at risk (Viljanen et al., 2014). For instance, given that adults with deafblindness often face communication difficulties that lead to poor psychosocial functioning and social isolation, rehabilitation efforts should include communication training for both individuals with deafblindness and their caregivers (Kiely et al., 2013). Effective communication training programmes should focus on identifying and addressing the personal, situational, and environmental factors that contribute to communication breakdowns (Heine et al., 2019).
CESD
The data collected with the CESD highlight a concerning proportion of study participants with symptoms of depression. Previous research has shown that depressive symptoms in those with deafblindness are nearly twice as common compared with those with hearing loss alone, indicating that deafblindness significantly increases the mental health burden (Kiely et al., 2013). Moreover, depressive symptoms tend to rise more sharply over time following the onset of deafblindness and hearing loss, compared with those with vision loss or no sensory loss (Kiely et al., 2013; Rong et al., 2020). However, research has yet to explore the long-term changes in depression as vision and hearing loss progress, considering clinical measures of sensory function and contextual factors (Kiely et al., 2013; Xie et al., 2021). Therefore, this finding underscores the importance of regular mental health assessments in identifying individuals at risk and highlights the need for targeted interventions to address and mitigate depression symptoms. In addition, this finding aligns with other studies, which showed that men with deafblindness were more likely to be depressed than men without sensory impairments, while there was no significant difference in depression risk between women with deafblindness and women without any sensory impairment (Lyu & Kim, 2018). In comparison, another study showed that depression prevalence increased with multimorbidity, rising from 25.2% to 31.2% among older men and from 30.4% to 34.5% among older women (Ansari et al., 2022). Consequently, both studies suggest a significant link between deafblindness and increased depression risk, particularly among men.
Correlation analysis
The significant positive correlation between IADL and MMSE scores supports that cognitive function is somewhat related to the ability to perform daily activities independently. The absence of significant correlations involving age suggests that functional and cognitive abilities may be more critical determinants of independence than age alone in this population, especially given the heterogeneity in the age of onset of deafblindness. The link between higher IADL scores and higher MMSE scores highlights the crucial role cognitive function plays in maintaining independence in daily activities (Guthrie et al., 2018). Sensory impairments, such as vision and hearing loss are prevalent among older adults (65 + years) and are closely tied to difficulties in communication, mood, functional ability, and social engagement (Wittich & Dumassais, 2025). Previous research indicated that sensory impairments were significantly correlated with both depression and cognitive decline (Ansari et al., 2022; Lyu & Kim, 2018), and lower levels of social participation were found to be associated with greater limitations in daily functioning (Cimarolli & Jopp, 2014). However, we need to be mindful when relating these findings to the present study, given the limited range of cognitive scores among our participants.
Limitations
This study has several limitations that should be acknowledged to contextualize the findings and guide future research. One key limitation is the small sample size (e.g., uneven and small numbers across WHO regions) and some missing information (e.g., age of onset of the sensory difficulties, qualifications and experience of sign language interpreters, ability of formal and information communication support to translate/interpret research questions from English into local spoken and/or signed languages). These variables introduce unknown variability into the data, and may limit the generalizability of the findings. The multiple communication modalities as well as the varied languages are specifically crucial to consider, given the importance of accurate communication for the purpose of data collection and interpretation. The diverse demographic and geographic characteristics of the sample highlight the heterogeneity of individuals with deafblindness, but a larger sample would provide more robust conclusions and allow for subgroup analyses across different populations. In addition, the reliance on self-reported measures for IADL and depressive symptoms introduces the potential for recall bias or misreporting, which may not accurately reflect the true extent of participants’ functional limitations or mental health challenges. At the same time, self-report also facilitated data collection by giving us direct access to the subjective experience, and to empower participants in their research participation, while creating some methodological flexibility in the administration of the measures. Either way, the pragmatic decision to administer standardized measures that were developed in English to international participants, some of whom relied on formal and informal translation and interpretation raises concerns about the potential accuracy of such communication accommodations. Unfortunately, ensuring this aspect of data quality went beyond the resources of our study. The cross-sectional design of this study is another limitation, as it prevents the establishment of causal relationships between sensory impairments, cognitive function, and functional independence. Longitudinal studies are needed to better understand how these factors interact and evolve over time, particularly as sensory impairments worsen.
Moreover, the analysis did not account for contextual and environmental factors, such as access to assistive technologies, environmental barriers, or the quality of social support, all of which could significantly influence functional and cognitive outcomes. To address the limitation of not accounting for contextual and environmental factors, future studies could incorporate a more comprehensive data collection framework. In addition, the international nature of the sample introduces cultural and regional differences in health care systems and social norms, which may influence participants’ responses and outcomes. These differences were not explicitly analyzed or adjusted for, which limits the study’s ability to draw global inferences. Finally, for the purpose of simplification, this study did not differentiate between congenital and acquired forms of deafblindness. While this decision allowed for a broader initial analysis, future research should consider these subgroups separately to better capture variations in lived experiences and support needs. Despite these limitations, this study provides valuable insights into the functional, cognitive, and psychosocial challenges faced by individuals with deafblindness. Addressing these limitations in future research will enhance our understanding and inform the development of tailored interventions to improve the quality of life for this vulnerable population.
Implications
Future research should prioritize longitudinal studies to investigate the causal relationships between sensory impairments, cognitive decline, and functional limitations over time. This approach would allow for a better understanding of the progression and interplay of these factors. In addition, in-depth assessments conducted by professionals such as neuropsychologists, social workers, or occupational therapists should be integrated to provide a comprehensive evaluation of participants’ cognitive, emotional, and functional status. These specialized assessments would have clinical implications and thereby enhance the accuracy of findings and inform targeted interventions to address the unique challenges faced by individuals with sensory impairments. As other studies have illustrated, future research should focus on the severity of deafblindness, the use of assistive technology, contextual factors, coping strategies, and IADL capacity to develop tailored support and interventions for this community (Mueller-Schotte et al., 2019). In addition, investigating the clinical impact of targeted interventions, such as vision and hearing (re)habilitation, on enhancing independence and overall well-being will be essential for informing best practices in the care of individuals with deafblindness. This holistic approach can foster greater autonomy, improved mental health, and better quality of life for this vulnerable population.
Importantly, these findings have contributed to the development of the ICF Core Sets for Deafblindness, particularly by informing the voting process during the consensus conference held in October 2024 in Spain (Wittich & Dumassais, 2025). Insights gained from research on deafblindness severity, assistive technology, and targeted interventions directly influenced the selection of priority items for inclusion in the Comprehensive Core Set (Wittich et al., 2025b), designed to include all aspects relevant to inform decision makers and policy, the Intermediate Core Set (Wittich et al., 2025c), intended to facilitate inter-professional communication and service coordination, and the Brief Core Set (Wittich et al., 2025a), designed for one-on-one clinical assessment priorities. This study, together with previous publications (Jaiswal et al., 2024; Ogedengbe et al., 2025; Paramasivam et al., 2023; Paramasivam, Jaiswal, Minhas, Holzhey, et al., 2021; Wittich & Dumassais, 2025; Wittich, Dumassais, Jaiswal, et al., 2024) required for the development of the comprehensive Core Set marks a critical step in establishing a standardized framework to address the complex needs of individuals with deafblindness. The next step will be to transform these items into a clinically useful measure, similar to the format of the ICF Checklist (World Health Organization, 2003).
Conclusion
This study provides critical insights into the functional, cognitive, and psychosocial challenges faced by deafblind adults, emphasizing the importance of individualized and multidisciplinary interventions. The findings highlight significant variations in functional independence, with notable limitations in specific tasks such as handling finances and transportation, underscoring the need for tailored support to enhance quality of life. Furthermore, the prevalence of depressive symptoms in this population points to the urgent need for mental health interventions, including strategies to address social isolation and communication barriers. The study also underscores the complex interplay between sensory impairments and cognitive function. Current assessment tools, such as the MMSE, may not fully capture the cognitive challenges in this population as they are not accessible, indicating a need for the development of more adaptable evaluative measures. These findings advocate for comprehensive rehabilitation programmes that address sensory, cognitive, and psychosocial dimensions, including interventions such as communication training, sensory aids, and socially engaging activities to mitigate the risks of depression and cognitive decline.
Footnotes
Acknowledgements
We extend heartfelt gratitude to the global network of Deafblind International and the European Deafblind Network for their invaluable support in participant recruitment. This study’s global reach was made possible through the collaborative efforts of numerous organizations across continents. We express sincere thanks to the National Knowledge Center for Deafblind Issues in Sweden, Associació Catalana Pro Persones amb Sordceguesa and Federación Española de Sordoceguera in Spain, CRESAM in France, Institución Fátima in Argentina, the School of Health Sciences at Örebro University, SensesWA and Deafblind West Australians in Australia, Deafblind Association New Zealand, Royal Dutch Kentalis in the Netherlands, Sense India in India, Sense Nepal in Nepal, Hope City Foundation for Development and Training in Egypt, DeafBlind Zambia in Zambia, Sense Tanzania in Tanzania, National Association of the Deafblind in Uganda, and Inclusion Sans Frontière-Multi Handicap in Niger. Special appreciation goes to our Canadian partners–DeafBlind Ontario Services, CNIB Deafblind Community Services, and the Canadian Hellen Keller Center –whose in-kind contributions were instrumental in facilitating recruitment across Canadian provinces. The collective effort of these organizations has been crucial in ensuring diverse global representation in our research.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study has been financially supported by Deafblind International, the Quebec Vision Health Research Network, and Canadian Hearing Services.