
Abstract
Vision impairment could have debilitating effects on patients’ mental, physical, and emotional health. Our study aims to understand the role of meditation and breathing exercises in the management of vision loss and its effects on patient’s disease progression. This study is designed as a systematic review and meta-analysis. Eligible studies were retrieved from MEDLINE, EMBASE, and CINAHL databases and gray literature. Covidence software was used to conduct the systematic review. Duplicate records were removed, and two independent reviewers screened records for relevance. After the screening, a risk-of-bias assessment was carried out. Data were extracted, and a meta-analysis was performed using STATA 14.0. Fixed-effect and random-effect models were computed based on heterogeneity. Our results indicate that meditation and breathing exercises significantly reduce intraocular pressure (IOP) (ES = −1.76, 95% CI = [−2.69, −0.83]) in glaucoma patients, mean deviation of Humphrey visual field testing (ES = −0.20, 95% CI = [−0.37, −0.03]), and biomarkers such as cortisol (ES = −0.73, 95% CI = [−0.25, −2.22]) and reactive oxygen species (ES = −2.45, 95% CI = [−4.20, −0.71]). In addition, our results demonstrated significant increases in beta-endorphins (ES = 28.60, 95% CI = [25.61, 31.59]) following breathing and meditation exercises. Furthermore, our study demonstrated that these exercises were associated with non-significant decreases in inflammatory markers, such as interleukin-6 levels (ES = −1.25, 95% CI = [−2.75, −0.24]), retinal nerve layer fiber thickness (ES = −0.20, 95% CI = [−0.53, −0.14]), and non-significant increase in brain-derived neurotrophic factor (ES = 28.24, 95% CI = [−25.24, 81.71]). Our systematic review also found improvements in quality of life, physical fitness, and mood for vision loss patients. Meditation and breathing exercises offer a range of benefits to patients with vision loss, including improvements in IOP, biomarkers, quality of life, physical fitness, and mood. Further research is needed to better understand the mechanisms underlying their effects and the means to apply them in practice.
Keywords
Introduction
Visual impairment and blindness is a major public health challenges, estimated to affect up to 359.1 million people worldwide (Flaxman et al., 2017). While there are many medical treatments available for various eye conditions, such as glaucoma and age-related macular degeneration, many patients still experience progressive vision loss despite conventional treatments. Vision loss is among the most debilitating impairments for individuals of any age group. The effects could be on the physical, mental, and emotional well-being of patients and caregivers, significantly diminishing their quality of life. The effects of vision loss extend beyond the physical inability to see, as it can lead to significant mental and emotional distress. For instance, patients can experience anxiety, depression, and even social isolation, which can further worsen the overall outcome of the condition (Demmin & Silverstein, 2020). Therefore, there is an urgent need to identify new and effective therapies that can improve the quality of life of vision loss patients.
As a result, there has been growing interest in complementary and alternative approaches to managing vision loss (Jaber et al., 2021). Conventional therapy, although effective, does present some flaws and limitations, leading to the need for complementary approaches (Samal, 2014). Meditation and breathing exercise approaches have gained popularity in recent years. Both practices are based on the principles of mindfulness and relaxation and have been shown to have numerous health benefits (Behan, 2020; Zaccaro et al., 2018). Meditation involves training the mind to focus on the present moment and to develop an awareness of one’s thoughts and emotions (Sharma, 2015). Breathing exercises, however, involve regulating the breath to calm the body and reduce stress (Zaccaro et al., 2018).
Studies have found that both practices can have a positive impact on a wide range of physical and mental health outcomes. For example, meditation has been shown to reduce symptoms of anxiety and depression, lower blood pressure, and improve immune function (Black & Slavich, 2016; Goldstein et al., 2012; Hofmann et al., 2010). Furthermore, research has found that meditation can improve quality of life by reducing stress levels (Levin et al., 2014). Stress is a common side effect of vision loss and can cause physical symptoms, such as headaches and muscle tension, and emotional symptoms, such as anxiety and depression (Sabel et al., 2018). By reducing stress, meditation may help vision loss patients to better cope with their condition and improve their overall quality of life.
Similarly, breathing exercises have been found to reduce symptoms of asthma and improve lung function (Santino et al., 2020). Moreover, both practices are generally safe and well tolerated, making them attractive options for patients who may be unable to tolerate more invasive treatments.
However, the potential role of meditation and breathing exercises in managing vision loss is not well understood. Meditation is well validated as a technique to normalize stress biomarkers (Kutz et al., 1985). As vision loss is associated with an increase in stress (Dada et al., 2020; Sabel et al., 2018), reducing stress could yield improvements in visual outcomes. A randomized controlled trial validated this mechanism as it found that daily breathing exercises reduced intraocular pressure (IOP) in patients with primary open-angle glaucoma (POAG) (Dada et al., 2021).
In this systematic review, we aim to examine the existing literature on the effects of meditation and breathing exercises on vision loss patients. Specifically, we will explore the effectiveness of these practices in improving visual acuity, reducing visual field loss, and alleviating associated symptoms, such as eye pain and fatigue. By synthesizing the available evidence, we hope to provide a comprehensive overview of the potential benefits of these complementary approaches for vision loss patients and to identify gaps in the current research. Ultimately, this information could inform the development of new interventions to support vision loss patients and improve disease progression and quality of life.
Methods
Search strategy
This systematic review protocol follows the preferred reporting items for systematic reviews and meta-analysis (PRISMA) recommendations. The PRISMA checklist is detailed in Supplemental Appendix A.
MEDLINE, EMBASE, and CINAHL databases were performed from inception to August 24, 2022. Variations of natural language terminology, as shown in our detailed search strategy (Supplemental Appendix B), were used to retrieve eligible studies. Gray literature searches included ClinicalTrials.gov and ProQuest Dissertations and Theses Global (ProQuest). Conferences of the Association for Research in Vision and Ophthalmology, American Academy of Ophthalmology, and Canadian Ophthalmological Society were manually searched to identify any relevant poster presentations or abstracts.
Inclusion criteria
We included studies discussing the use of meditation or breathing exercises in vision loss patients. Examples of meditation and breathing exercises included but were not limited to mindfulness meditation, Buteyko breathing exercises, pranayama breathing exercises, alternative nose breathing, diaphragmatic breathing, yoga, and relaxation techniques. All causes of vision loss were considered in addition to varying levels of visual impairment. Examples include but are not limited to retinal disorders, corneal disorders, glaucoma, refractive error, and cataracts. The effects of meditation and breathing exercises on vision loss patients were evaluated by looking at any outcomes looking at eye health, including but not limited to, IOP, mean deviation of Humphrey’s visual field (HVF) testing, biomarkers, retinal nerve fiber layer (RNFL) thickness, motor strength and coordination, and quality of life. Economic studies, comparative studies, observational studies, cohort studies, randomized control trials, clinical trials, and multicenter studies were included.
Exclusion criteria
Exclusion criteria included review articles, systematic reviews, meta-analyses, case reports, letters to editors, and commentaries. Conference abstracts were included if adequate study details and data were provided. Any studies that did not have an English copy were omitted due to inconsistencies that could occur during the translation process of a non-English paper. There were no restrictions placed on publication year or geographical settings.
Study selection
All the compiled literature from the databases were imported into Covidence. Three levels of screening occurred (title, abstract, and full text), following automatic duplication checks conducted by Covidence and a manual duplicate check done by a reviewer (E.T.). Level 1 screening (title) and level 2 (abstract) screening were conducted using the inclusion and exclusion criteria.
Level 3 screening (full-text screening) included literature that evaluated the effects of meditation and breathing exercises on the health of vision loss patients. During each level of screening, three reviewers (E.T., M.A., and V.P.) independently assessed the literature and conflicts were resolved. If a consensus for conflict could not be reached between the two reviewers, then a third reviewer would mediate the conflict resolution. Cohen’s kappa (κ) coefficient was computed at each level of screening. The PRISMA flowchart (Figure 1) displays the number of studies included and excluded at each screening step.
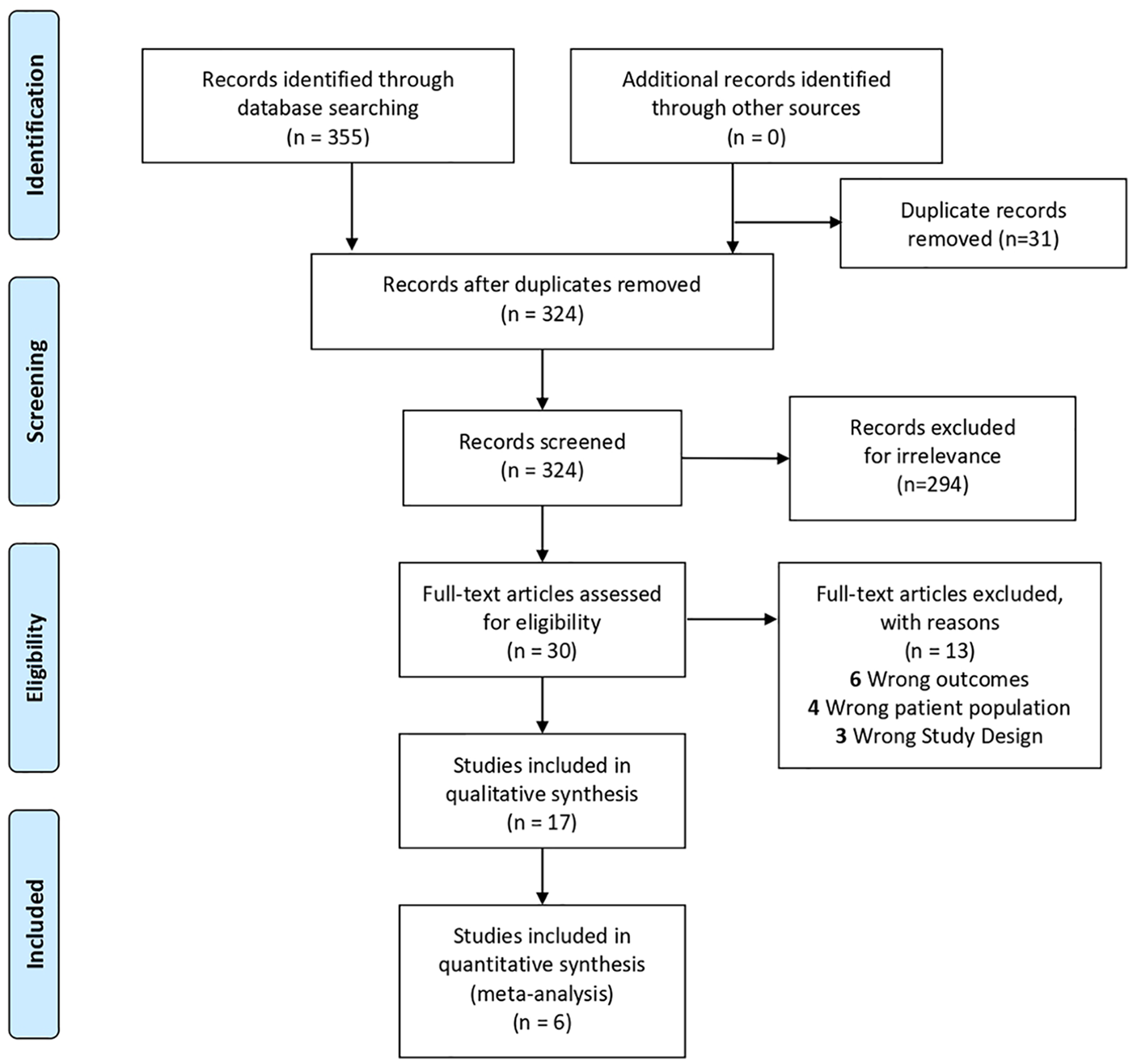
PRISMA flowchart summarizing the results of the literature search.
Risk of bias
The risk of bias assessment was conducted using a modified Downs and Black (1998) checklist. Studies with a score more than 20 were of high quality, studies with a score between 16 and 19 were considered to be of medium quality, and studies with a score lower than 15 were of poor quality. A quality check was performed to ensure the completeness of our methodology. Due to limited evidence, none of the lesser-quality articles were excluded from the analysis. Appendix C provides details on the risk of bias assessment.
Data collection process
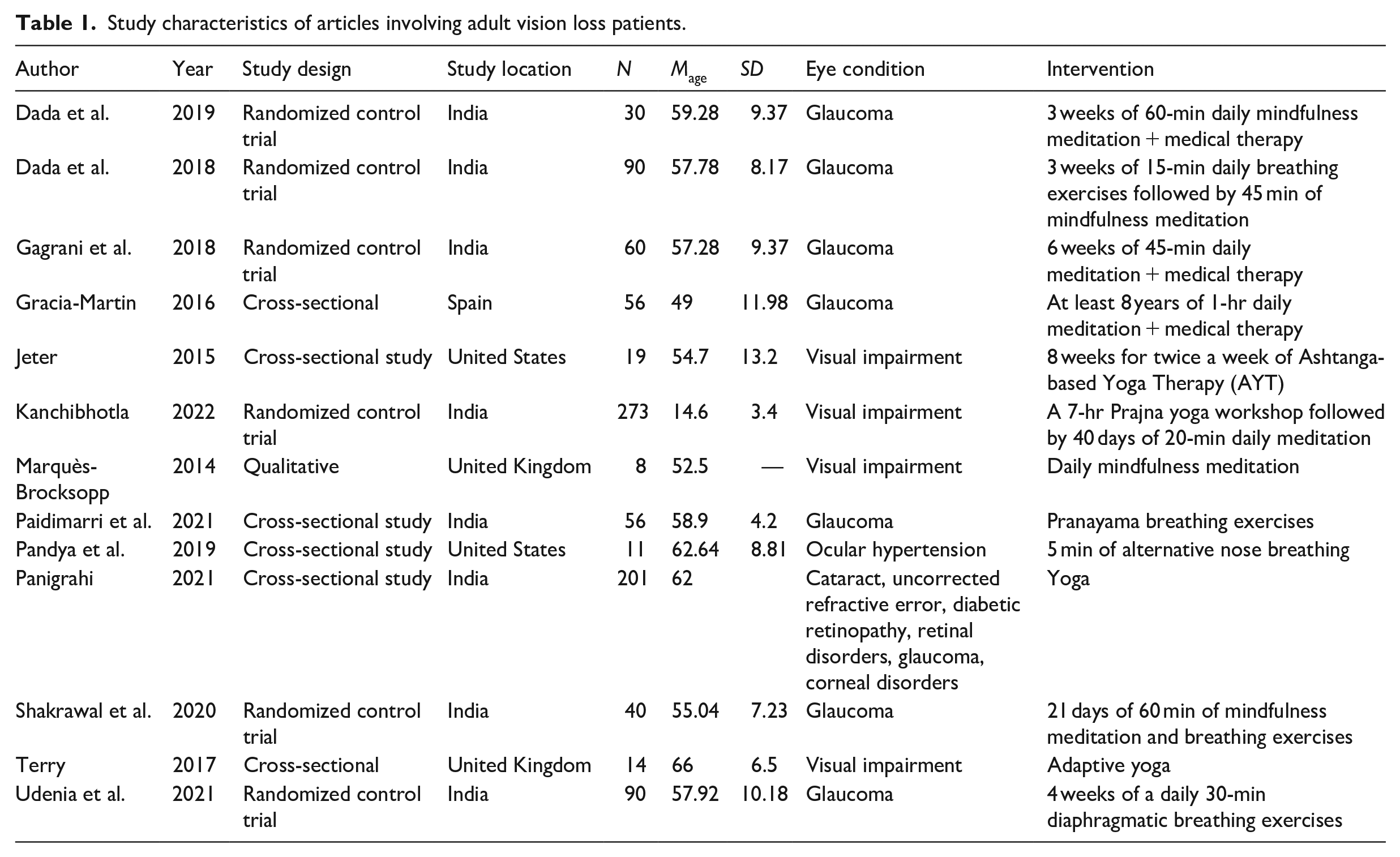
After the quality check process, the study characteristics of 17 articles were extracted (Table 1). This included author, year of publication, study design, study location, and sample size. A total of seven articles were used for quantitative synthesis.
Study characteristics of articles involving adult vision loss patients.
Statistical analysis
The meta-analysis was conducted using STATA 14.0 software (STATA Corporation, College Station, TX). The proportion was the effect size or the treatment effect. The degree of heterogeneity among studies was determined using the I2 value, which indicates the proportion of variation across studies that is due to heterogeneity rather than chance. The chi-square test was used to assess whether the observed differences between studies were likely due to chance alone. A low p-value and a large chi-square statistic relative to its degree of freedom indicated the presence of heterogeneity. Based on the level of heterogeneity, fixed-effect or random-effect models were applied. Forest plots and funnel plots were generated to visualize the results and check for publication bias.
Results
Search results
Searches of online databases and gray literature yielded 324 results after 31 duplicates were removed. After title and abstract screening, 294 articles were deemed irrelevant and 30 articles proceeded to full-text screening. After full-text screening, 17 articles proceeded to data extraction. A total of 17 studies were included in the meta-analysis, 6 were included in the quantitative analysis, and 9 studies did not provide data synonymous with other papers. Studies that were excluded were deemed to be irrelevant or failed to proceed past the screening levels. The Cohen’s kappa (k) coefficient for the abstract and title screening, and full-text screening was 0.64 and 0.65, respectively.
Study characteristics
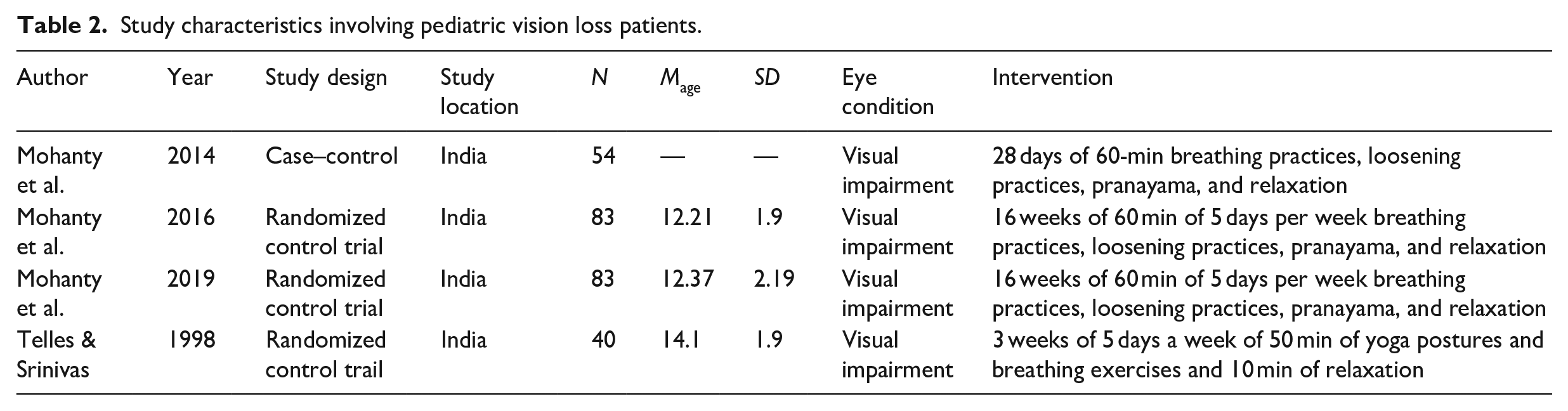
Table 1 details the demographic characteristics of the 17 eligible studies included in the review, consisting of 9 randomized control trials and 6 cross-sectional studies. The locations of the studies were primarily within India with the rest of the studies taking place in the United States, United Kingdom, and Spain. The population size of the studies ranged from 8 to 273 (Kanchibhotla et al., 2022; Marquès-Brocksopp, 2014). Studies reported a mean age ranging from 12.21 to 66 years (Mohanty et al., 2016; Terry et al., 2017) indicating that this meta-analysis captures a diverse range of age groups affected by vision loss (Tables 1 and 2).
Study characteristics involving pediatric vision loss patients.
Assessment of study quality and publication bias
Using the Modified Downs and Black (1998) Checklist, most studies scored 15 or above, indicating “fair” or “good” quality (n = 15). One study achieved a score between 11 and 14 (n = 2), indicating poor quality. Due to the limited availability of evidence, the lesser-quality articles were not excluded from the analysis. Publication bias could not be concluded given it is only one of the numerous possible explanations for funnel plot asymmetry. Appendix C provides details on the risk of bias assessment and publication bias.
Physical fitness in vision loss children
Three studies have investigated the relationship between physical fitness and vision loss in children, with results indicating improvements in upper extremity strength and motor speed (Mohanty et al., 2016), improved physical fitness (Mohanty et al., 2019), and improvements in proprioception (Mohanty et al., 2014).
Improvements in quality of life and mood for adults
Marques found that yoga was associated with self-perceived improvements in emotional, social, and physical health in patients with various medical conditions, including vision loss patients (Marquès-Brocksopp, 2014). Studies reported better quality of life in vision loss patients who practiced yoga compared to those who did not (Gagrani et al., 2018; Panigrahi et al., 2021). In addition, Jeter et al. (2015) found that yoga interventions may negative psychosocial states, such as anxiety, depression, and stress, by providing postural stability and minimizing the fear of fallling.
Impact on IOP
Figure 2(a) indicates there was significant heterogeneity between studies examining the impact of IOP in glaucoma patients who underwent medical therapy (I2 = 97.2, p = .00) and glaucoma patients who underwent meditation and breathing exercises in combination with medical therapy (I2 = 94.8, p = .00). Studies reported a significant reduction in IOP in glaucoma patients who underwent both meditation and medical therapy (effect size [ES] = −1.76, 95% CI = [−2.69, −0.83]) compared to those who only had medical therapy (ES = −1.09, 95% CI = [−1.71, −0.47]). There was a greater reduction in IOP in glaucoma patients who underwent meditation compared to a matched control. Given that four studies investigated IOP, more studies are required to draw definitive conclusions.
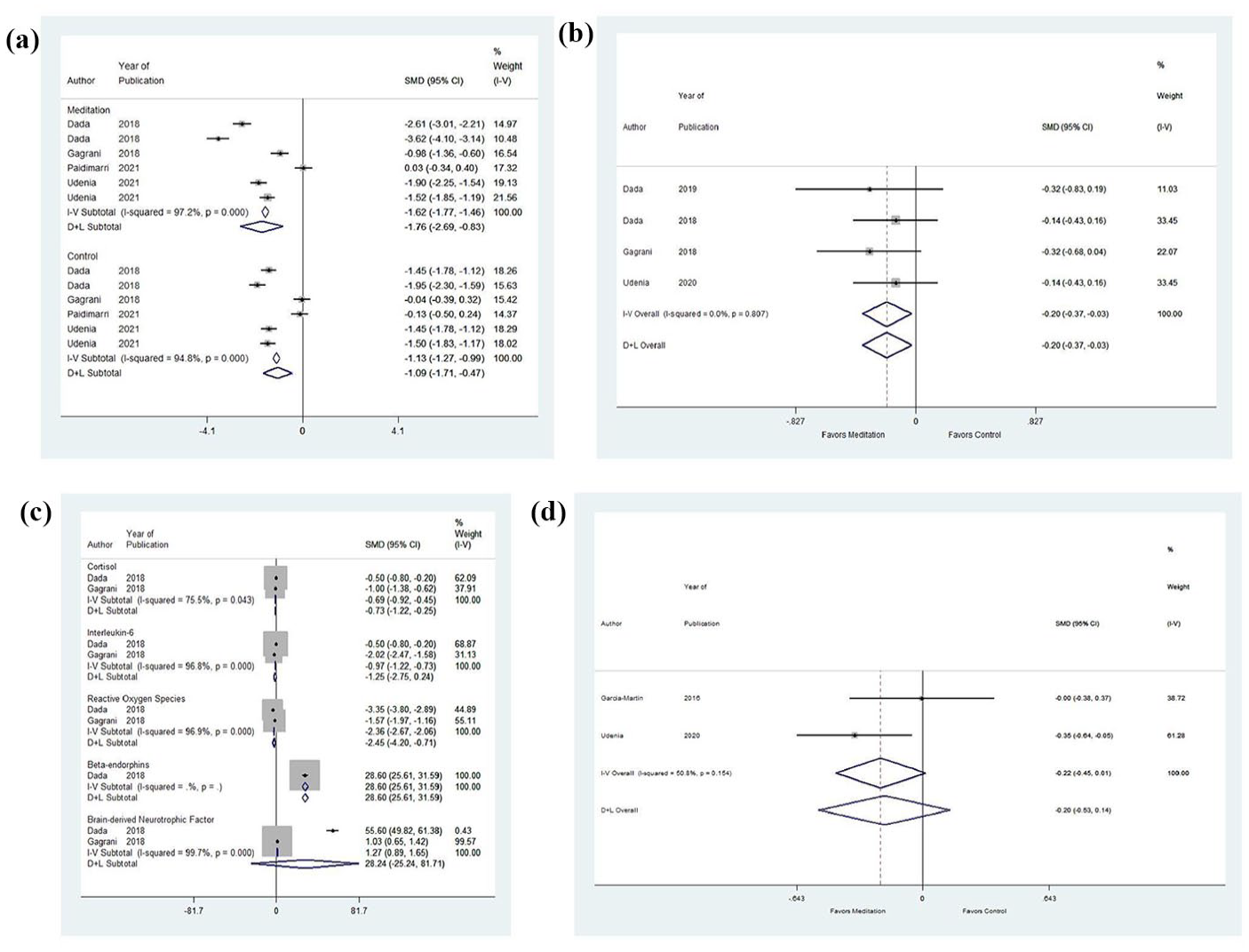
Forest plot for effect size (ES) of (a) intraocular pressure (IOP), (b) mean deviation Humphrey’s visual field, (c) biomarkers, and (d) retinal nerve fiber layers (RNFL) thickness in glaucoma patients who underwent meditation and breathing exercises. Negative ES denotes that the outcome is less predominant in the glaucoma patient.
Impact on mean deviation of HVF
Figure 2(b) indicates there was no significant heterogeneity between studies examining the impact on the mean deviation of HVF in glaucoma patients who underwent meditation and breathing exercises (I2 = 0.0, p = .807). Studies reported a significant increase in the mean deviation of HVF of glaucoma patients who underwent meditation and breathing exercises (ES = −0.20, 95% CI = [−0.37, −0.03]). Given that two studies investigated the mean deviation of HVF, more studies are required to draw definitive conclusions.
Impact on biomarkers
Figure 2(c) indicates there was significant heterogeneity between studies examining the impact of meditation on biomarkers in glaucoma patients, such as cortisol (I2 = 75.7, p = .043), interleukin-6 (I2 = 96.8, p = .000), reactive oxygen species (I2 = 96.9, p = .000), and brain-derived neurotrophic factor (I2 = 99.7, p = .000). Studies reported a non-significant reduction in interleukin-6 (ES = −1.25, 95% CI = [−2.75, −0.24]) and a significant reduction in cortisol (ES = −0.73, 95% CI = [−0.25, −2.22]) and reactive oxygen species (ES = −2.45, 95% CI = [−4.20, −0.71]. Studies reported a non-significant increase in brain-derived neurotrophic factor (ES = 28.24, 95% CI = [−25.24, 81.71]) and a significant increase in beta-endorphins (ES = 28.60, 95% CI = [25.61, 31.59]. Given that two studies investigated biomarkers, more studies are required to draw definitive conclusions.
Impact on RNFL thickness
Figure 2(d) indicates there was no significant heterogeneity between studies examining the impact on RNFL thickness in glaucoma patients who underwent meditation and breathing exercises (I2 = 50.8, p = .154). Studies reported a non-significant increase in the RNFL thickness of glaucoma patients who underwent meditation and breathing exercises (ES = −0.20, 95% CI = [−0.53, −0.14]). Given that two studies investigated the mean deviation of RNFL thickness, more studies are required to draw definitive conclusions.
Publication bias
Figure 3 represents funnel plots for IOP (Figure 3[a]), mean deviation of Humphrey’s visual field (Figure 3[b]), biomarkers (Figure 3[c]), and RNFLs (Figure 3[d]) among vision loss patients. The funnel plot has few studies at the bottom of the plot which implies that small studies with non-significant results may not be published. Visual inspection of the funnel plot did not reveal any asymmetry.
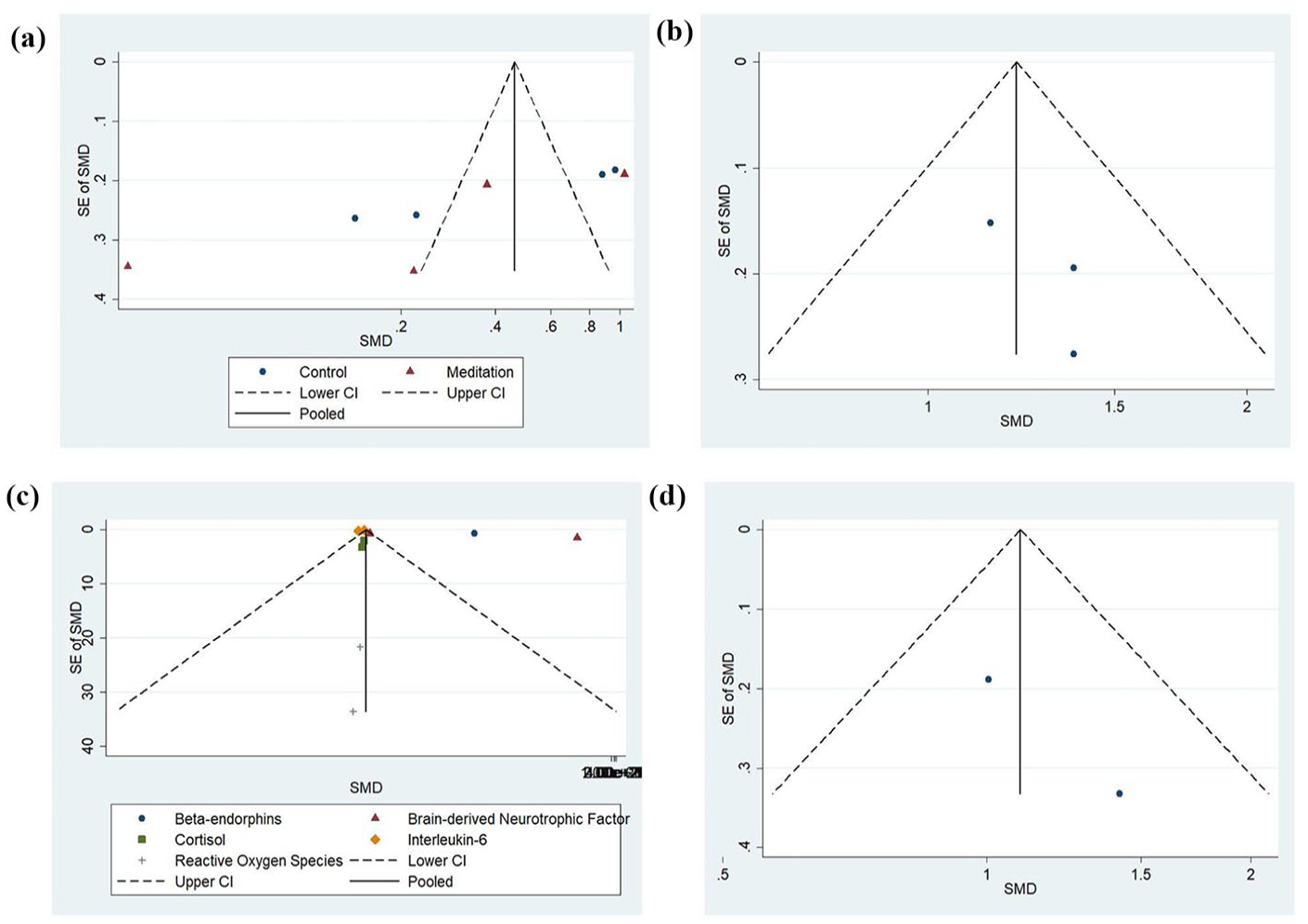
Funnel plot for the included studies evaluating (a) intraocular pressure (IOP), (b) mean deviation Humphrey’s visual field, (c) biomarkers, and (d) retinal nerve fiber layers (RNFL) thickness in glaucoma patients who underwent meditation and breathing exercises.
Discussion
This systematic review and meta-analysis looked at the incorporation of meditation and breathing exercises as a potential management option in vision loss patients. Studies showed improved physical fitness for pediatric vision loss patients following meditation and breathing exercises (Mohanty et al., 2014, 2016, 2019). The stimulation of skeletal muscles during isometric contraction and maintenance of proper posture and spinal alignment during yoga may help with muscular strength and flexibility (Bhavanani et al., 2011). Improvements in joint proprioception in children with vision impairment may compensate for poor vision; sensory systems have a wide range of plasticity, so early intervention may be beneficial (Prechtl et al., 2001). Improved muscular strength, flexibility, and proprioception may aid in the daily activities of children with vision loss. These findings suggest that interventions involving meditation, breathing exercises, and yoga may play an important role in improving the physical health and functionality of children with vision loss.
Studies on meditation and breathing exercises demonstrated self-perceived improvements in emotional, social, and physical health, a better quality of life, and improved negative psychosocial states, including depression, anxiety, and stress in adult vision loss patients (Gagrani et al., 2018; Jeter et al., 2015; Marquès-Brocksopp, 2014; Panigrahi et al., 2021). Falling is a significant concern for patients with vision loss; however, the improved postural stability from yoga and meditation exercises can help improve these negative psychological states (Roach et al. 2014). It is suggested that cultivating a sense of mindfulness and well-being can provide individuals with a sense of purpose and meaning, particularly when trying to navigate difficult life experiences, such as vision loss (Lindstrom & Eriksson, 2010; Whitford & Olver, 2011). Emotional acceptance of visual impairment is often critical for long-term adaptation to the condition (Fenwick et al., 2012; Wang & Chan, 2009; Weber & Wong, 2010). Meditation has been shown to improve mental health and well-being by reducing stress and negative emotions, such as anxiety and depression (Goyal et al., 2014; Jeter et al., 2015). This is an important finding due to the high correlation between stress and quality of life (Levin et al., 2014). Therefore, meditation and breathing exercises may play a role in improving the quality of life for vision loss patients by reducing stress, promoting emotional well-being, and enhancing overall well-being. This also has other important implications for health outcomes in individuals with visual impairment, as negative emotions can exacerbate existing health conditions.
By reducing stress levels and promoting emotional well-being, meditation may improve health outcomes in this population. It is believed that meditation achieves these effects by reducing the physiological responses to stress, including changes in heart rate, blood pressure, and cortisol levels (Tang et al., 2015). This reduction in physiological stress responses due to meditation may have particular relevance for individuals with glaucoma, a condition associated with increased IOP and a higher risk of cardiovascular disease (Emami et al., 2022).
Our meta-analysis showed that the addition of meditation and breathing exercises alongside conventional medical therapy significantly decreases IOP and reduction in stress biomarkers in glaucoma patients. IOP reduction is a major risk factor for the development of POAG (Gordon et al., 2002). It has been demonstrated that a reduction in IOP can significantly delay or prevent the progression of the disease (Heijl et al., 2002). Meditation and breathing exercises can lower blood pressure (Goldstein et al., 2012). As a result, it is possible that these practices could lead to reductions in IOP. The reduction in IOP may be mediated by the reduction of stress markers, such as cortisol (Dada et al., 2020), and inflammatory markers, such as interleukin-6 (Borkenstein et al., 2013). Meditation and breathing exercises decrease stress biomarkers, such as cortisol, proinflammatory cytokines, and catecholamines (Pascoe et al., 2017). Studies have validated the use of meditation and breathing exercises into one’s daily routine as a means of reducing stress levels, and the physiological markers associated with stress (Kutz et al., 1985). It has been observed that excessive levels of cortisol in the body can lead to an increase in blood pressure, but regulating the production of cortisol can lead to a reduction in blood pressure. (Whitworth et al., 2005). Increased blood pressure is related to increased IOP which can subsequently lead to increased risk and incidence of POAG (Nislawati et al., 2021). In addition, stress has been shown to induce endothelial dysfunction (Resch et al., 2009), elevate oxidative stress (Kimura et al., 2017), and increase IOP (Abe et al. 2020, which are all risk factors of POAG. Endothelial dysfunction in glaucoma can involve endothelial cells of the vasculature of the eye, channels of the trabecular meshwork, and Schlemm’s canal (Resch et al., 2009). The downregulation of brain-derived neurotrophic factor may also explain the progression of vision loss despite the reduction in IOP (Lambuk et al., 2022). Consequently, reduction in stress may play a direct role in mitigating the risk factors of glaucoma and therefore delay/prevent disease progression. By reducing stress, meditation and breathing exercises may lead to a decrease in IOP and improve vascular function, both of which are crucial for the prevention of glaucoma progression. Therefore, in combination with conventional medical and surgical therapy, meditation and breathing exercises could be explored as an adjuvant therapy to delay progression of glaucoma. Our meta-analysis also showed increases in the mean deviation of HVF and non-significant increase in RNFL thickness in glaucoma patients. This finding is in contrast to Garcia-Martin et al. (2016) who found that while meditation improved visual acuity, it had no effect on RNFL thickness. Mean deviation of HVF and RNFL thickness are two important measures for evaluating the severity and progression of glaucoma (Abu et al., 2020; Chang & Budenz, 2008). HVF test assesses visual function in individuals with glaucoma as the disease affects peripheral vision, and RNFL thickness indicates damage to the retinal fibers due to glaucoma (Chang & Budenz, 2008; Mashige & Oduntan, 2016). This implies that meditation and breathing exercises may reduce severity of glaucoma or delay progression of the disease.
This systematic review aimed to assess the effectiveness of meditation and breathing exercises on vision loss patients. Our results suggest that these practices may have some potential benefits for visual function and associated symptoms. However, the evidence base is limited, and the quality of the studies included in our review was generally low. Nonetheless, the available evidence suggests that meditation may have some potential benefits.
Breathing exercises also showed some promise in reducing IOP and improving visual function in patients with POAG, although the evidence is limited. In general, the studies included in our review were small and of poor quality, with high risk of bias and inadequate reporting of study design and outcomes. However, a significant strength of this analysis stems from the fact that all the included studies had coherent results of improvement in IOP and the visual function in patients with POAG due to breathing exercises.
The limitations of the current evidence base highlight the need for further research on the effects of meditation and breathing exercises on vision loss patients. Future studies should use rigorous designs, such as randomized controlled trials with larger sample sizes, to provide more definitive evidence. In addition, more research is needed to explore the mechanisms underlying the potential benefits of these practices. It is possible that meditation and breathing exercises may improve visual function by reducing stress and promoting relaxation, or by improving blood flow and oxygenation to the eyes.
Despite the limitations of the current evidence, our review suggests that meditation and breathing exercises may have the potential to improve the IOP, biomarkers, quality of life, physical fitness, and mood for vision loss patients. Stress is a common side effect of vision loss and can cause physical and emotional symptoms that can significantly diminish a patient’s quality of life. By reducing stress and promoting relaxation, meditation and breathing exercises may help patients to better cope with their condition and improve their overall well-being. In conclusion, incorporating meditation into the treatment plan for glaucoma patients may improve disease outcomes and enhance the overall quality of life.
Largely, our findings provide insight into the management of vision loss in patients. It is crucial for clinicians to recognize the benefits of non-medical/surgical therapies in managing vision loss. Ophthalmologists could counsel their patients about the possible benefits of meditation and breathing exercises in managing their vision conditions to empower patients in managing their health and improve disease outcomes and quality of life.
Supplemental Material
sj-docx-1-jvi-10.1177_02646196231201773 – Supplemental material for Benefits of meditation and breathing exercises in vision loss patients
Supplemental material, sj-docx-1-jvi-10.1177_02646196231201773 for Benefits of meditation and breathing exercises in vision loss patients by Edward Tran, Mohamed Aly, Nirmit Shah, Vivian Phu and Monali S. Malvankar-Mehta in British Journal of Visual Impairment
Supplemental Material
sj-docx-2-jvi-10.1177_02646196231201773 – Supplemental material for Benefits of meditation and breathing exercises in vision loss patients
Supplemental material, sj-docx-2-jvi-10.1177_02646196231201773 for Benefits of meditation and breathing exercises in vision loss patients by Edward Tran, Mohamed Aly, Nirmit Shah, Vivian Phu and Monali S. Malvankar-Mehta in British Journal of Visual Impairment
Supplemental Material
sj-xlsx-3-jvi-10.1177_02646196231201773 – Supplemental material for Benefits of meditation and breathing exercises in vision loss patients
Supplemental material, sj-xlsx-3-jvi-10.1177_02646196231201773 for Benefits of meditation and breathing exercises in vision loss patients by Edward Tran, Mohamed Aly, Nirmit Shah, Vivian Phu and Monali S. Malvankar-Mehta in British Journal of Visual Impairment
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by the Academic Medical Organization of Southwestern Ontario (AMOSO) Innovation Fund-2019, Ref number: #INN20-020.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.