
Abstract
Background:
Globally, mental health issues are becoming more prevalent, but stigma and obstacles to getting treatment are substantial. There is still a lack of community-based and region-specific research in India.
Methods:
This study examined patterns of mental health literacy (MHL) and help-seeking preferences among an urban non-clinical population in Ahmedabad, Gujarat, India. A community sample of 100 adults participated in semi-structured interviews and completed an adapted version of the General Help-Seeking Questionnaire (GHSQ). Qualitative manifest content analysis was used to analyze the interview results. Descriptive frequencies were used to map patterns of understanding and help-seeking preferences.
Results:
Although the individuals were aware of the term “mental health,” mental illness and abnormal behavior were the most prevalent conditions associated with mental health. The most common issues were anxiety and depression, and little knowledge of professional roles. The primary source of information about mental health was digital media. Even though the attitude toward seeking professional help was found to be positive, assistance was only considered as the last option for severe mental health issues such as schizophrenia and suicidal thoughts. Non-clinical concerns were mostly managed through informal support from trusted individuals or faith and motivation-based sources. Many participants also reported uncertainty about how to respond when others shared mental health concerns.
Conclusions:
The findings highlight a gap between awareness and appropriate help-seeking. Improving MHL must extend beyond awareness to strengthen understanding of professional roles, normalization of psychological help for non-clinical concerns, and promote community-level dialogue.
Question: What are the levels of mental health literacy (MHL), stigma, and help-seeking attitudes among urban Indians for non-clinical mental health issues? Findings: Gaps exist in MHL and help-seeking behaviors, also reflecting the influence of stigma and sociocultural factors. Meaning: Mental health programs in India should be rooted in local realities and reinforced through community-based awareness efforts.Key Messages:
Mental health concerns have become a growing global issue, with nearly 30% of the population experiencing mental health problems during their lifetime. 1 In India, approximately 197.3 million people were affected by mental disorders in 2016, a number expected to rise in the coming years, which may strain public healthcare systems, productivity, and the national economy. 2 Despite the increasing prevalence, the National Mental Health Survey (2015–2016) reported treatment gaps of 85.2% for depression and 86.3% for substance use disorders. 3 Contributing factors include limited psychiatric infrastructure, poor policy implementation, economic constraints, and pervasive stigma.4–7
Addressing stigma requires special considerations in the Indian context, where cultural and religious beliefs about mental health often diverge from biomedical models. Studies in India have consistently reported poor understanding of mental illness, widespread stigma, and a reluctance to seek professional help.8,9 These challenges have prompted a growing interest in mental health literacy (MHL), defined as “knowledge and beliefs about mental disorders which aid their recognition, management, and prevention.” 10 MHL includes awareness of symptoms and treatment options, maintaining positive mental health, reducing stigma, and encouraging help-seeking. 11 However, since awareness does not always translate into action, research distinguishes between help-seeking attitudes, which are an individual’s orientation toward seeking psychological help, and help-seeking intentions, which are the likelihood that they would actually seek help. 12 Both are influenced by multiple factors, including stigma, knowledge, social norms, trust in services, cost, and accessibility. 9
Some of the earliest Indian studies reported high levels of stigma, setting the foundation for subsequent work in this field.13,14 Over the past five decades, Indian researchers have explored mental health stigma, MHL, and help-seeking behaviors both within the general population,15–19 and among specific groups, including adolescents, 20 young adults, 21 college and school students,22,23 women, 24 medical professionals,25,26 Accredited Social Health Activists, 27 teachers,28,29 policymakers, 30 caregivers of people with mental health concern, 31 and patients with mental health concerns. 32
Despite this growing body of literature, findings remain highly inconsistent across studies. While some studies report improvements in MHL and help-seeking,33,34 others continue to show persistently high levels of stigma and low help-seeking.15,28,35 These inconsistencies highlight the need to examine the methodological approaches and context within which prior research has been conducted. Although understanding stigma, MHL, and help-seeking in India needs cultural sensitivity, most existing studies rely on quantitative tools such as brief vignettes and structured questionnaires, offering limited insight and failing to capture nuanced, culturally rooted understandings of mental health in everyday life, particularly among lay urban adults.
In a culturally and socio-linguistically diverse country such as India, qualitative research is essential to explore understanding, reasoning, experiences, and context-specific factors that may not be adequately reflected through quantitative measures alone. Furthermore, relatively few studies have been conducted in Gujarat,27,36–40 revealing a regional gap in the literature. There remains a need for descriptive, community-based qualitative research that explores MHL and help-seeking preferences within specific urban contexts. The present study seeks to address this gap by examining these patterns among the urban non-clinical population of Ahmedabad, Gujarat, India.
Aims and Objectives
The present study aimed to identify and describe patterns of MHL and help-seeking preferences among the urban non-clinical population of Ahmedabad, Gujarat. It focuses on categorizing understanding of people regarding mental health and common conditions, sources of mental health-related information, knowledge about mental health professionals (MHPs) and their roles, responses to mental health concerns of other people, and preferred sources of help for both clinical and non-clinical problems.
Methods
Following the study proposal, the institutional ethics committee reviewed and approved the study.
Participants
The study included 100 community-dwelling healthy urban adults from Ahmedabad, Gujarat. The sample size was determined practically to capture a wide range of perspectives within an urban setting. Data collection continued until responses began to show repetition across major categories of MHL and help-seeking, with no distinctly new categories emerging in later data. The final sample of 100 participants thus allowed for descriptive mapping of response patterns. Purposive and snowball sampling techniques were used to select participants. The participants included both females and males aged 18–50, and their educational qualifications were at least secondary (10th grade or higher). Based on their self-report, the participants were considered to be “healthy,” which implies that they had no known diagnosis of a serious mental illness at the time of data collection. Exclusion criteria included a self-reported history of major psychiatric illness, being a primary caregiver of a person with mental illness, or being an MHP.
Measures
A socio-demographic information sheet was used to collect basic demographic information from the participants. The researcher developed a semi-structured interview schedule including the following key questions to understand participants’ MHL and help-seeking preferences: (a) What do you know about mental health? (b) What are the most common mental health issues that you have heard of or observed? What all do you know about it? (c) What is the source of the mental health-related information or content you just shared? Any other common sources from which you get such information? This is a different question. (d) Do you know about various types of MHPs? Can you talk more about the nature of their work? (e) Have people shared their mental health-related concerns with you ever? What did you tell or suggest to them? (f) What are your views on consulting an MHP? Have you ever recommended someone to consult an MHP?
The General Help-Seeking Questionnaire (GHSQ) was used to identify participants’ likelihood of seeking help for various psychological concerns. 41 This tool is designed to be adaptable based on the specific requirements of a study and is found to be reliable and valid. 41 The questionnaire was used to complement the qualitative interview data by systematically mapping commonly preferred sources of help rather than using it as a psychometric assessment tool.
Participants were required to indicate their likelihood of seeking help from different sources for a range of psychological concerns by marking “yes” or “no” in the corresponding box. For the present study, the questionnaire included both non-clinical concerns (e.g., stress, anger issues, overthinking, career guidance, relationship difficulties, family problems, self-confidence issues, body image concerns, sleep disturbances, and over-perfectionism) and clinical concerns (e.g., anxiety, depression, suicidal ideation, psychotic disorders, and addiction).
For the current study, the GHSQ was adapted for contextual relevance and administered in Gujarati. The adaptation involved translation and back-translation procedures, followed by expert review to ensure linguistic accuracy and face validity. As the questionnaire was meant for descriptive use, no proper psychometric validation was undertaken.
Help-seeking sources were categorized into three broad groups: Trusted personal contacts (partner, friend, colleague, parent, close relative, family doctor), MHPs (psychiatrist, counselor, therapist), faith- and motivation-based sources (motivational speaker, life coach, astrologer, priest, religious guru, or leader). Participants were also given the option to indicate that they would not seek help at all or to specify any additional sources not listed in the questionnaire. Multiple responses were permitted to capture a comprehensive understanding of help-seeking preferences.
Procedure
The researchers developed a pool of questions through a prior literature review and field experience in mental health. A semi-structured interview schedule aligned with the study’s aims was developed. Two clinical psychologists and a psychiatrist reviewed both the interview schedule and the adapted GHSQ. Their feedback was incorporated to enhance relevance and appropriateness. Once shortlisted, the questions were translated into Gujarati and back-translated with expert review. After finalizing the translated questionnaire and interview schedule, a feasibility study with six participants was conducted to identify challenges and refine the interview process for the final data collection.
The first author conducted all interviews. Participants were recruited through purposive and snowball sampling using community networks. Informed consent was obtained from each participant, outlining the study’s objectives, procedures, voluntary nature, and confidentiality. No monetary incentives were offered, and participants were assured of no associated risks. The semi-structured interview lasted approximately 15–45 minutes, followed by a GHSQ that took about 2–5 minutes. Depending on the participant’s comfort, setting, and consent, interviews were either audio-recorded or documented via detailed field notes.
To avoid influencing participants’ responses, no mental health education was provided before or during data collection. Once the interview was over, each participant received a researcher-developed informational booklet on mental health conditions, help-seeking options, and self-care strategies. Participants who expressed significant distress, shared concerns, or asked for professional support were guided further using the contact details of local MHPs.
Given that participants were selected through community networks and that the researcher shared a similar sociocultural background with them, the researcher’s positionality cannot be ruled out as a potential influence. Therefore, reflexive awareness was maintained throughout the data collection process, and care was taken to conduct interviews in a neutral, non-directive manner. Consequently, findings are carefully evaluated, keeping in mind the study’s exploratory nature.
Data Analysis
Qualitative manifest content analysis was used to analyze the qualitative data collected through the semi-structured interviews. 42 The analysis focused on the explicit content of responses given by the participants about categories derived from the aims of the study. To become acquainted with the data, the researchers read through detailed field notes and interview transcripts several times. Based on their manifest meaning, relevant statements were identified and classified into the respective content categories. A descriptive overview of participants’ preferred patterns was obtained by counting the frequency of responses within each category. Furthermore, data from the adapted GHSQ were summarized descriptively by counting frequencies to map participants’ reported help-seeking preferences across each category (i.e., trusted personal contacts, MHPs, and faith- or motivation-based sources) and to complement the qualitative findings.
Results
The socio-demographic profile of the sample reflected a diverse mix of ages, education levels, marital statuses, and background characteristics. For the present research, 100 participants were interviewed. Of these, 45 participants were aged 18–25, 24 were aged 26–35, and 31 were aged 36–50. Thus, the age range of participants was 18–50 years (M = 32 years, SD = 12). Since participants had an average of 15 years of formal education (SD = 2), their educational qualifications were high. Of these participants, 13 had 10–12 years of formal education, 54 had 12–15 years, and 33 had more than 15 years. In terms of gender, 39 were male, while 61 participants were female. Regarding marital status, 41 participants were unmarried, 57 were married, and two were widowed. The sample comprised 25 homemakers, 39 employed individuals, and 36 students. Regarding the participants’ socio-economic status, 16 belonged to the lower-middle class, 30 to the middle class, and 54 to the higher socio-economic class.
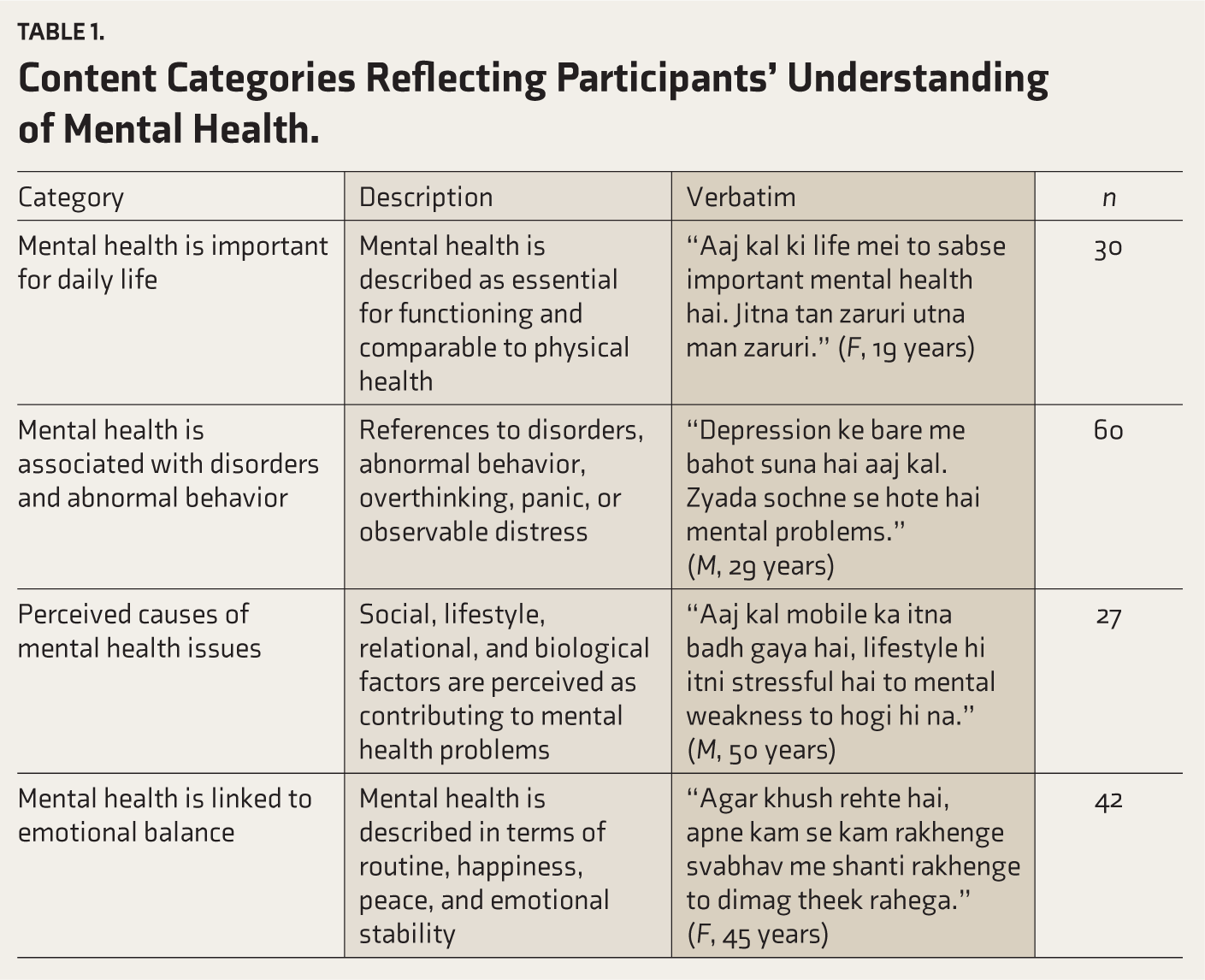
When asked about their understanding of the term mental health, most participants described it in relation to mental health disorders, abnormal behaviors, and severe psychological conditions (Table 1). Many participants referred to individuals they had observed with severe mental health illnesses when explaining their understanding. A smaller number of participants mentioned perceived causes of mental health issues, with social or lifestyle-related factors being reported more frequently than biological ones. Some participants also described mental health as increasingly important in contemporary life. In addition, a proportion of participants noted positive aspects of mental health, such as emotional balance, resilience, strength, happiness, confidence, and healthy daily routines, recognizing them as integral components of mental well-being. In response to the second question on knowledge about mental health concerns, most participants mentioned depression and anxiety. Very few participants referred to other conditions such as psychosis, Attention Deficit Hyperactivity Disorder (ADHD), phobias, or bipolar disorder. Similarly, only a small number of participants were able to describe specific symptoms associated with depression.
Content Categories Reflecting Participants’ Understanding of Mental Health.
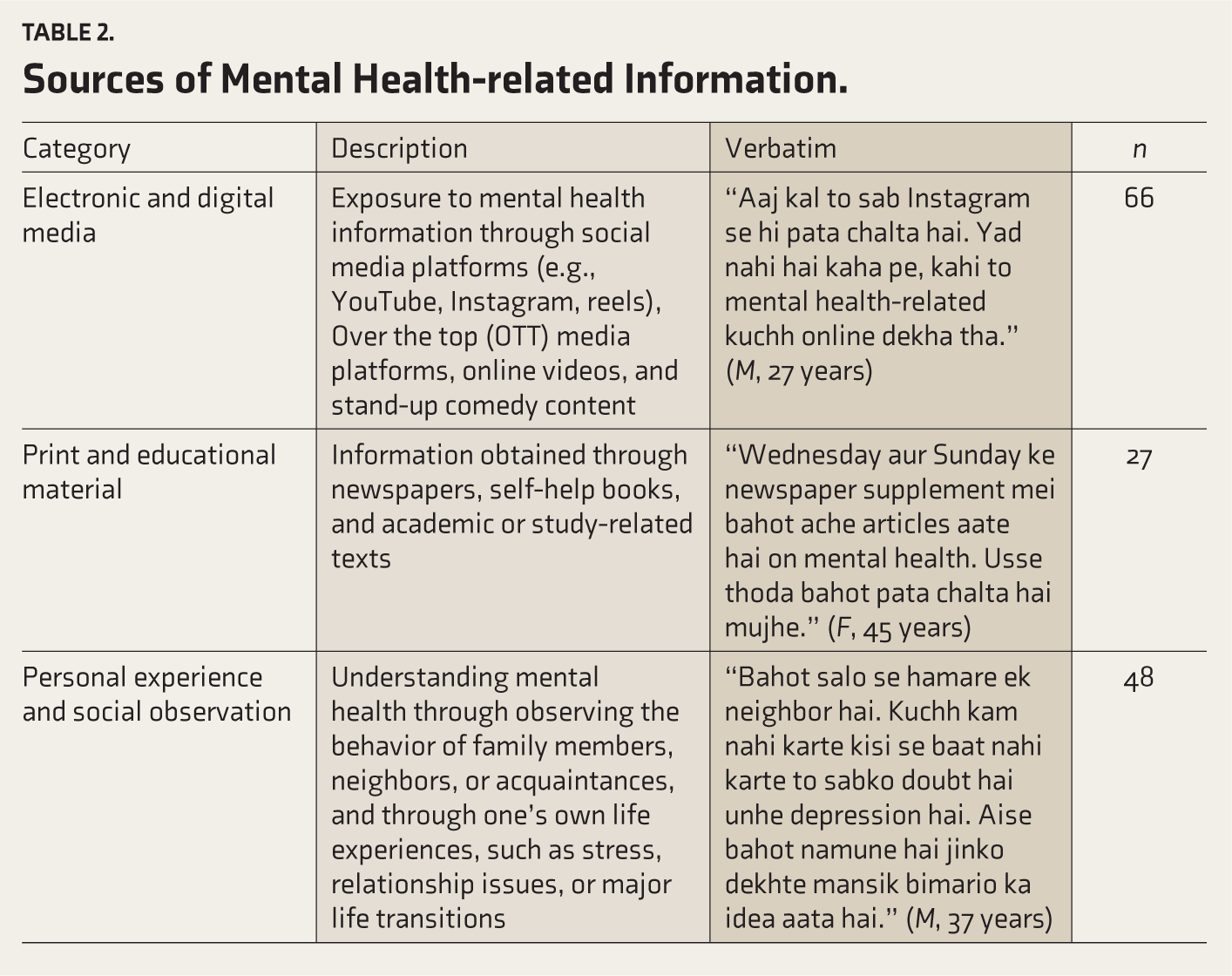
Another key aspect explored through the interviews was the participants’ sources of mental health-related information (Table 2). Most participants reported encountering such information through various forms of electronic and digital media, including YouTube, Instagram, WhatsApp stories, social media posts, Over the top (OTT) media platforms, and stand-up comedy, often describing this exposure as incidental or unplanned. Several participants mentioned developing an understanding of mental health through personal experiences or by observing others in challenging life situations, such as stressful family environments, significant life changes (e.g., job loss, menopause, or periods of high stress), and problematic behaviors in themselves or people around them. Participants also referred to conversations with friends or observing mental health issues within their friends’ families as important sources of awareness. A smaller proportion of participants identified print media, such as newspaper articles and supplement features, as a source of mental health-related information.
Sources of Mental Health-related Information.
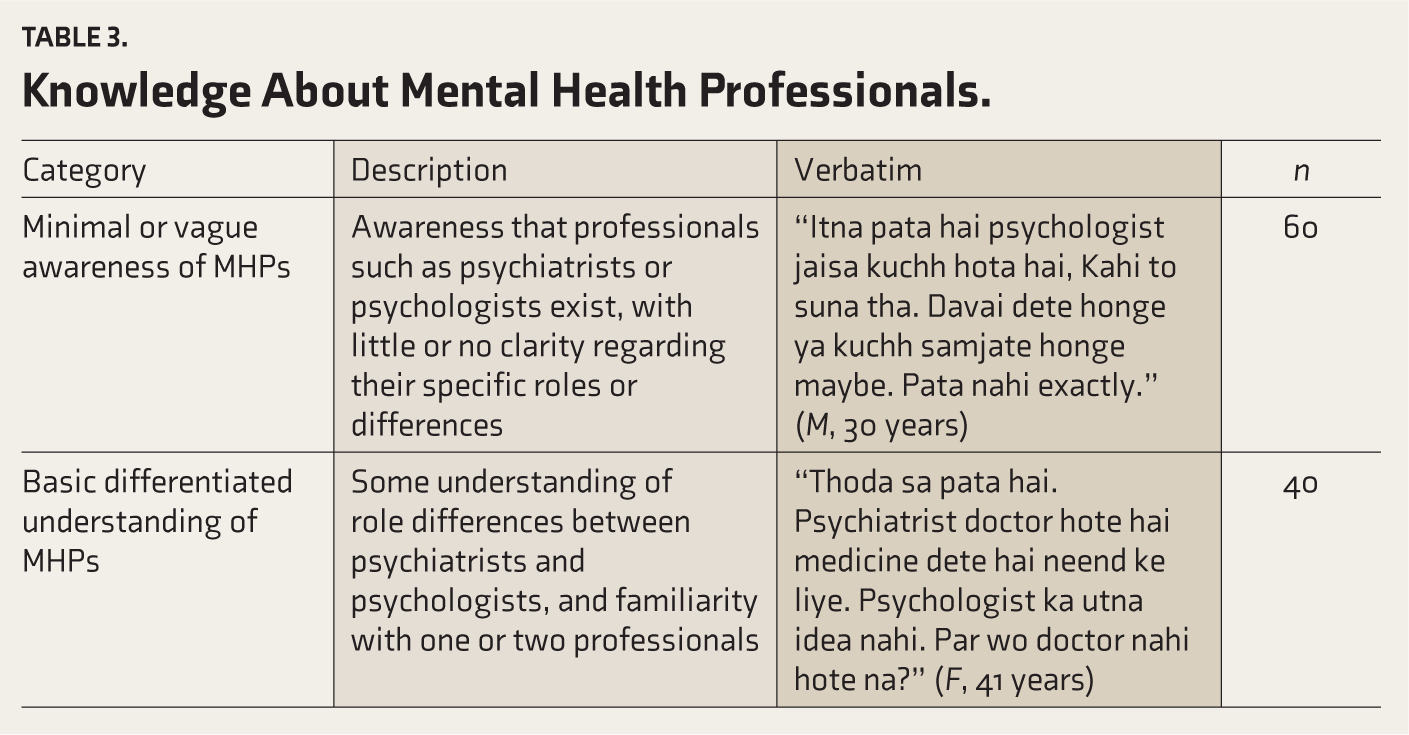
Participants’ knowledge about MHPs was also explored (Table 3). Most participants demonstrated minimal or vague awareness of MHPs, commonly referring to psychiatrists or psychologists without clear differentiation of their roles. A smaller group of participants showed a basic understanding of role differences, with psychiatrists typically associated with prescribing medication and psychologists with talk-based interventions. Very few participants demonstrated more detailed knowledge, such as educational qualifications of these professionals or the ability to name specific MHPs in their city whom they would consider consulting.
Knowledge About Mental Health Professionals.
Another aspect explored was how participants reported responding when someone shared a mental health concern, as well as how they would respond if they themselves experienced such concerns (Table 4). A substantial number of participants reported difficulty in articulating specific ways of dealing with mental health concerns. Among those who responded, the most commonly mentioned approaches were recommending self-help and coping strategies, such as staying occupied, engaging in hobbies, spending time with family or friends, and practicing activities such as meditation or yoga. Some participants also described offering emotional support by actively listening, showing empathy, and encouraging open conversations. On the other hand, some participants reported advising people to reduce their worries by stopping to think about the issues, leaving the problem, and continuing with their daily activities despite the challenges they face. Participants’ views on professional mental health services were also explored. A smaller group of participants reported recommending professional help to others. The majority of participants had a generally positive attitude toward mental health services, admitting that it is appropriate and helpful to talk to a professional when asked about consulting an MHP, and whether they had ever recommended it to others. Furthermore, they admitted they would consider expert help only as a last resort, usually when the problem is serious and persistent. Only a few participants had actually recommended consulting an MHP, and these were done with obvious hesitation.
Knowledge of Strategies for Helping Self and Others.
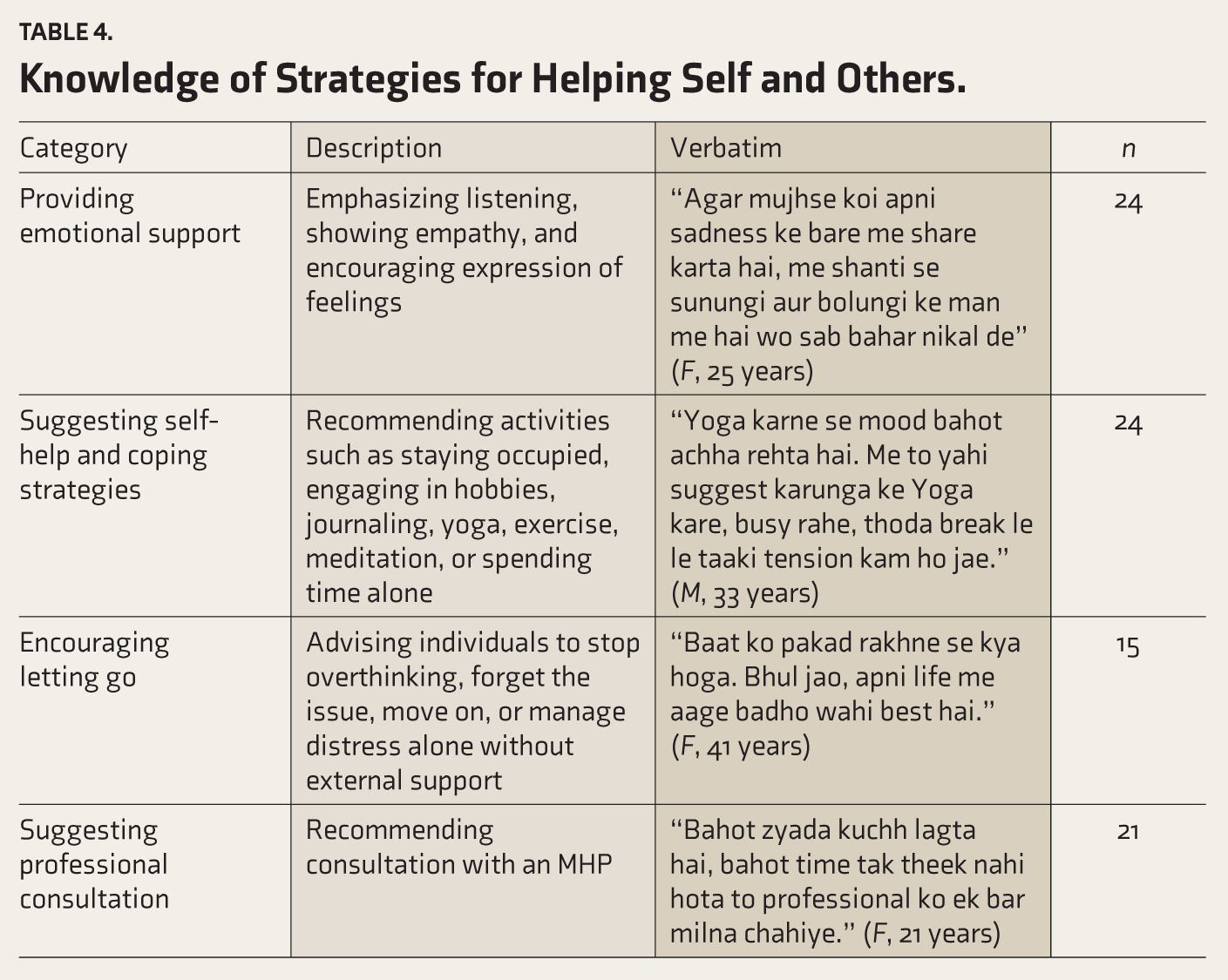
Table 5 presents an overview of individuals’ reported help-seeking preferences for various mental health-related and everyday life concerns. For concerns commonly perceived as clinical in nature, such as schizophrenia, depression, and suicidal thoughts, many participants preferred seeking help from MHPs. At the same time, faith-based or motivational sources were mentioned less frequently. At the same time, several participants reported that they would seek support from trusted personal contacts such as friends, relatives, or partners, even for clinical concerns. However, this pattern was less evident for concerns related to smoking or drinking. In these cases, a small number of participants reported considering professional help, and a considerable number indicated that they would not seek help from any source.
Reported Help-seeking Preferences for Different Mental Health Concerns.
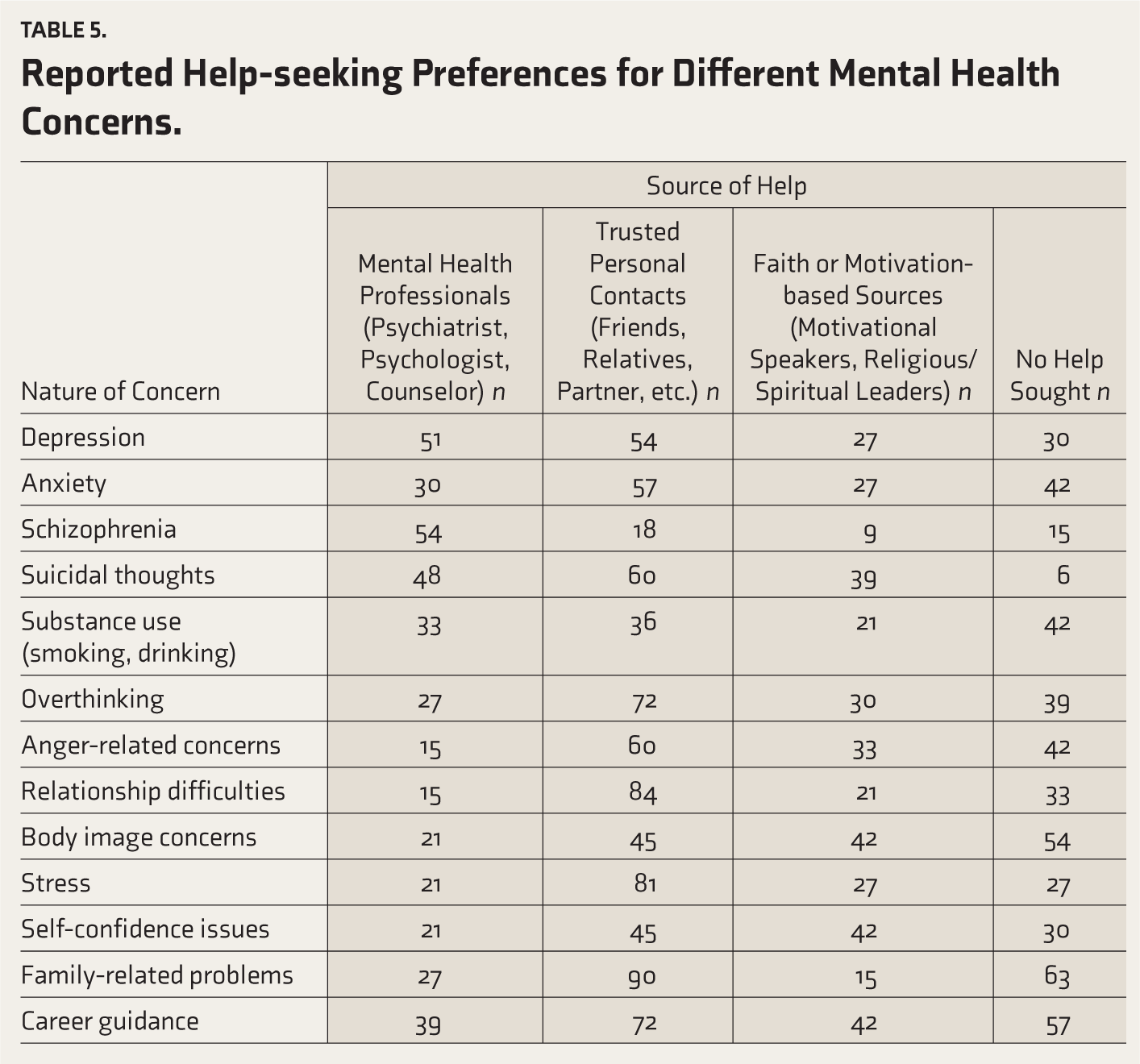
For concerns perceived as non-clinical, such as anger-related issues, relationship difficulties, and body image concerns, fewer participants reported a preference for consulting MHPs. Instead, participants most commonly indicated a preference for support from trusted personal contacts or faith-based or motivational sources. Across several concerns, such as body image issues, family-related problems, career guidance, anger management, overthinking, and anxiety, a substantial number of participants reported that they would not seek help from any source.
Discussion
To the best of our knowledge, this is the first published study in Gujarat, India, to examine public understanding of mental health and help-seeking preferences for both clinical and non-clinical concerns through in-depth interviews. Results indicated that participants generally demonstrated familiarity with the term “mental health” and were able to articulate personal interpretations or associations. However, mental health was most commonly equated with mental illness, described using idioms such as “stress,” “tension,” and “overthinking,” expressions frequently observed in Indian contexts to convey psychological distress. 43 Depression emerged as the most widely recognized condition, while only a few participants mentioned disorders such as psychosis, bipolar disorder, phobias, or ADHD. This mirrors national trends, indicating depression and anxiety as the leading contributors to India’s mental health burden, followed by schizophrenia and bipolar disorder. 44
The prominence of depression in public discourse may reflect its increasing representation in media and awareness campaigns. It is also more readily identified, not only by the public but also by primary care physicians. In contrast, more complex conditions such as personality and substance use disorders often remain under-recognized. 25 Similar findings have been reported among women 8 and older adults. 45 Anxiety was referenced by some participants, but with limited clarity, consistent with another study where it was observed that tension-related symptoms were often seen as untreatable and distinct from formally recognized mental illness. 46
Participants also identified a range of psychosocial and lifestyle-related stressors as perceived causes of mental health issues, reflecting existing literature that emphasizes the role of social determinants. 47 In contrast, biological or genetic causes were rarely mentioned, suggesting a gap in understanding mental illness as a medical condition potentially requiring pharmacological treatment. Notably, participants did not refer to supernatural explanations, such as possession or black magic, diverging from older studies that reported frequent reliance on non-biomedical explanatory models.48,49 Additionally, participants did not use stigmatizing terms (e.g., “pagal,” “sanki”) explicitly during interviews, in contrast to earlier Indian studies indicating a possible shift in attitudes. 50 Nevertheless, the possibility that social desirability bias influenced the responses cannot be ruled out, given that participants may have avoided certain culturally stigmatized beliefs or terminology during the interview.
A subset of participants also discussed the positive aspects of mental health, including happiness, confidence, inner peace, and emotional stability. This indicated their understanding of mental health beyond the usual illness-focused definitions. Such mentions may suggest that the general public is becoming more aware of the concepts associated with positive psychology due to the overall exposure in the media, educational institutions, and digital platforms. The importance of mental health in today’s fast-paced life was also emphasized by several participants, who equated it with physical health. A similar finding regarding the prevalent use of electronic media as the primary source of mental health information was noted, which is consistent with the international literature highlighting the role of digital platforms for spreading psychological information and support. 51 Prior research suggests that digital media can facilitate mental health awareness, bust myths, and enable contact-based anti-stigma interventions. 52 While participants’ preference for digital sources reflects growing accessibility, it also underscores the need for quality control, user-centered design, and integration within broader mental health strategies. 53
Print media was mentioned less frequently, whereas many participants reported learning about mental health by observing or hearing stories from people around them. This highlights the role of interpersonal narratives in shaping MHL. Existing research suggests that personal disclosures and direct conversations can help reduce stigma. 54 Fostering empathy and social support through online or digitally mediated interpersonal interactions is also found to be useful in recent times. 55
When individuals do share their concerns, it is equally important that listeners know how to respond, what may be termed emotional first aid. 56 Only a small proportion of participants demonstrated awareness of coping strategies, self-help techniques, or basic emotional support skills, highlighting the difficulty of accessing peer support as a resource in India. 57 Although some of the strategies described were broadly consistent with evidence-based practices for promoting well-being 58 such advice may inadvertently come across as judgmental or poorly timed, for example, suggesting rigorous routines or exercise to someone with functional impairment due to depression. Participants did not indicate awareness of when such suggestions might be unhelpful, underscoring the need to promote basic MHL skills, including empathic listening, and appropriate support. 59
Relatively few participants reported willingness to seek or recommend professional help, typically framing such help as a last resort when issues became persistent or unmanageable. Consistent with this, a limited understanding of the roles and qualifications of MHPs was evident. This indicates a persistent gap in knowledge about professional roles and qualifications, as reported over the past two decades. 10 Such misunderstandings may also be shaped by negative perceptions toward MHPs. For instance, researchers found persistent stigma toward psychiatrists even in metropolitan India, 60 potentially contributing to delays in accessing appropriate mental health care.
This study further qualitatively explored help-seeking preferences for both clinical and non-clinical concerns. A considerable proportion of participants indicated that they would consider seeking professional help for core clinical issues such as schizophrenia, depression, anxiety, and suicidal ideation. This aligns with prior findings among Indian university students, where professional help-seeking was favored for severe concerns such as suicidal ideation. 61 Similarly, a substantial proportion identified MHPs as preferred support for depression and schizophrenia.
However, attention must be given to the considerable number of participants who reported not preferring professional support. Recent Indian studies highlight persistent limited awareness of mental illnesses and available help as key barriers. 62 Notably, professional help-seeking was particularly low for addiction-related issues such as smoking and alcohol use, with only a few participants considering clinical intervention. Prior research similarly underscores that “tension” or “distress” is frequently perceived as everyday social suffering rather than warranting medical or psychological intervention. 63 Such interpretations may contribute to the normalization and trivialization of certain mental health problems, delaying or preventing engagement with formal care.
When professional help is not sought, people easily turn to alternative sources such as faith-based or motivational practitioners and trusted individuals. As shown in multiple studies in India and across the globe, people often rely on general physicians, spiritual healers, or motivational speakers,64,65 which may often lead to discontinuity or abandonment of care. The study found that for serious issues such as suicidal ideation, anxiety, and depression, many participants endorsed faith-based practitioners or religious figures as potential support, consistent with literature highlighting religion’s central role in India. 66
For severe conditions such as schizophrenia, only a minority of participants preferred faith-based sources over professional help, echoing findings from North India, where psychiatrists were the primary contact, followed by general physicians, and faith healers. 67 Among all help sources, trusted individuals such as friends, partners, colleagues, and family members were most preferred across concerns. This aligns with India’s collectivistic culture and prior research showing a greater tendency to seek support from close relations over MHPs.61,68 The cultural emphasis on interpersonal support may lead individuals to initially seek informal help before considering professional care.
In contrast, for non-clinical concerns such as anger, relationship problems, or body image dissatisfaction, professional help-seeking was notably low. Most participants preferred confiding in trusted individuals or seeking spiritual or motivational guidance, describing professional consultation as a “last resort,” consistent with previous findings. 48 When help-seeking is limited even for diagnosable conditions, individuals distressed by non-clinical concerns are even less likely to be studied or to seek support. This gap, noted in recent reviews, points to an urgent need for research and outreach focused on preventive and subclinical mental health needs. 9
A key strength of the present study lies in its qualitative design, which foregrounds participant perspectives and enables a nuanced understanding of help-seeking preferences. Nevertheless, certain limitations have to be considered. The sample was skewed toward urban and relatively well-educated individuals who may have greater exposure to mental health resources. This limits the generalizability of the findings to rural or less educated populations, where hindrances related to literacy and access may differ markedly. Also, this is a pilot study that primarily aims to improve the methodological approaches and identify the salient categories. Future research should incorporate a larger, more diverse, and representative sample across rural and urban settings, socio-economic strata, and educational levels to better assess the socio-demographic influences on MHL and help-seeking in India.
Conclusion
This study highlights findings that differ from previous literature, particularly in the context of the urban population of Gujarat, where awareness of mental health conditions tends to be on the higher side. Social media’s role in spreading information might have contributed to a moderate increase in MHL, particularly regarding conditions such as depression and anxiety. This may also be attributed to the predominance of younger participants and those from higher socio-economic strata in the sample. Despite this awareness, the inclination to seek professional help was found to be limited. Professional psychological care was largely viewed as appropriate only for severe mental illnesses, such as suicidal thoughts or schizophrenia. This was found to be in line with an illness-centered understanding of mental health rather than a preventive or wellness-oriented perspective. For non-clinical problems and everyday psychological distress, reliance on informal support systems or self-management strategies continued to be the norm.
These findings suggest that to promote timely or effective help-seeking behavior, future interventions should go beyond information dissemination and be structured, with a focus on policy and practice, because information dissemination alone might not be effective. Mental health interventions at the national level could focus more on distinguishing the roles of psychologists and psychiatrists to improve public understanding of these issues. There should be equal emphasis on promoting psychological interventions for non-clinical issues, such as relationship issues, anger management, and issues of self-confidence as well. At the local level, it could be crucial in developing MHL through empathy and personal experience that safe spaces are developed for people to talk about their experiences. This could be crucial for building trust and reducing the stigma around seeking professional help. At the same time, there must be greater responsibility in disseminating information on mental health issues through digital media, with a focus on expert-developed information and appropriate representations of counseling and treatment in movies and entertainment. Last, this information can be implemented through existing support practices, including community outreach programs such as street plays, awareness programs, and support communications. Although this study is specific to the urban population of Ahmedabad, it can be extended to other cities in India based on their sociocultural and demographic characteristics. This can be done by using the trends that were identified in this study to develop region-specific mental health awareness programs.
Considering all the above factors, this will help to develop a more enlightened, empathetic, and ethical mental health environment that balances awareness, accessibility, and authenticity in India’s emerging mental health care landscape.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
We are grateful to each and every participant for their contribution.
Appropriate Permissions from the Concerned Authorities
None.
Data Sharing Statements
Deidentified individual participant data (including data dictionaries) can be made available, in addition to study protocols, the statistical analysis plan, and the informed consent form if required. The data will be made available upon publication to researchers who provide a methodologically sound proposal to achieve the goals of the approved proposal. Proposals should be submitted to Rupangi Shah at
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
ChatGPT was used to refine the language and check grammar across all sections of the manuscript. The authors take full responsibility for the accuracy and originality of the content, including any text revised using an AI tool.
Ethical Statement
Name of the Institutional Ethics Committee/Independent Review Board: Institutional Ethics Committee of National Forensic Sciences University. Approval Reference Number: NFSU/SDR/IEC/Certificate/495/2023. Date of Approval: 4 December 2023
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
All the study participants were above the age of 18. A written consent form signed by each participant for participation and publication of the findings.
Prior Presentations
Presented some part of the findings from the initial sample taken in a national conference held at the National Forensic Sciences University on 13th March 2024.
PROSPERO/CTRI Details
NA.
Registration
The study is not of an interventional nature. Hence, this is not applicable.
Trial registry name: URL: Registration number:
Simultaneous Submission to Another Journal or Resource
None.
Status of Your Study (for Study Protocol)
NA.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.