
Abstract
Background:
There seems to be a relationship between barriers of distress-perception and stigma to consult a mental health professional (MHP), help-seeking inclination from MHP, help negation, and encouragement from significant others (SO) to consult MHP in bringing about a change in help-seeking behavior. However, these have not been studied in tandem. This study aimed to explore the relationship between factors influencing help-seeking behavior among distressed, non-treatment-seeking young adults (D-NTS) for common mental health concerns following the ReachOut intervention.
Methods:
A total of 109 D-NTS aged 20–35 engaged with ReachOut were recruited online using purposive and snowball sampling. ReachOut was aimed at enhancing professional help-seeking. Participants were assessed at baseline and one month post-intervention for help-seeking barriers, inclination, and encouragement from SO. Help-seeking behavior from MHP was evaluated at a two-month follow-up. Inferential statistics in the form of Spearman’s rho correlation, logistic regression, and path analysis were computed.
Results:
Regression analysis revealed a significant model (χ2 = 34.53, P < .001) with an R2 value of 0.52. Help-seeking inclination from MHP (B = 0.711, P = .037), help negation (B = −0.452, P = .039), and encouragement from SO to consult MHP (B = 1.942, P = .008) at post-assessment were significant predictors of help-seeking behavior, assessed at follow-up. The SEM hypothesized for path analysis with help-seeking behavior as the outcome was a good fit.
Conclusion:
Help-seeking decisions are complex processes influenced by an intricate interplay of internal and external factors. A comprehensive examination of these elements simultaneously provides valuable insights for tailoring interventions and strategies aimed at enhancing help-seeking behavior in D-NTS young adults.
Trial registration:
The intervention trial was registered in the ISRCTN registry (ISRCTN14504454).
Keywords
Help negation and encouragement from significant others predict help-seeking behavior. Stigma and encouragement from significant others moderate help-seeking behavior. The help-seeking decision is a multifaceted process influenced by the interplay of internal and external factors.Key Messages:
Young adults often show reluctance to seek professional support for their mental health, which can result in immediate and prolonged functional limitations, reduced education, career opportunities, and the possibility of comorbid conditions. 1 Despite the availability of effective interventions, there is a substantial treatment gap for common mental disorders globally, including in India. 2 High treatment gap indicates a significant disease burden and disability.
Numerous studies have examined factors behind the unwillingness to seek professional consultation. Perceived susceptibility and problem severity influence health-related behaviors. 3 Young adults often normalize their distress, shifting their threshold of “real” distress to extreme notions of normality. 4 Recognizing the need for treatment due to a mental health concern is the first step toward seeking help. 5
However, awareness alone may not be enough. Once the individual is aware and can express their distress and need for support, they must also be inclined to discuss their concerns with the source of help. 5 Individuals with positive views about service accessibility may have a higher inclination and are closer to seeking professional help than those in the pre-contemplation stage. 6 Intervention studies have confirmed that an initial inclination to seek professional help may facilitate positive outcomes. 7 Most help-seeking intervention studies target help-seeking inclination, especially from mental health professionals (MHPs), which is known to predict help-seeking behavior. 8
Furthermore, stigma is known to deter young adults from seeking professional help. 9 Among those with easy accessibility to services, self-stigma is an important barrier, 10 where individuals internalize negative societal attitudes, which significantly reduces their likelihood of seeking help. Perceptions of non-biological causes of mental illness, often influenced by cultural beliefs, increase the tendency toward self-blame and exacerbate stigma in Asian cultures.11,12 These perceptions, combined with stigma and cultural beliefs, decrease the likelihood of help-seeking among young adults.
Another major barrier to help-seeking is help negation, where individuals actively avoid seeking professional help despite recognizing the need for it. It is often reported in young adults experiencing distress and other mental health conditions. 13 However, the determinants underlying help-negation are not fully understood, and factors such as socio-demographics, treatment history, etc., do not fully explain the variance in help-negation.14–16
Social support is a key antecedent of help-seeking 17 and is known to predict help-seeking behavior. 18 Lynch et al. 19 identified informal helpers as supportive intermediaries or as obstructive forces. They noted informal networks to be dynamic and important agents in pathways to care that could hinder or support young individuals in accessing and engaging mental health facilities. Moreover, social support plays an essential part in combating the negative aspects of exclusive focus on self-reliance among young individuals seeking help. 20
There appears to be a relationship between barriers of distress-perception and stigma, help negation, help-seeking inclination, encouragement from significant others (SO), and help-seeking behavior. However, these have not been studied in unison. For instance, an increased possibility of endorsing self-stigmatizing beliefs and focusing on self-reliance when individuals anticipate that others may view them negatively for taking professional help has been noted. 21 Help-negation, which is also understood in terms of excessive preference for self-reliance, is related to reduced perceived social support and inclination to seek professional help. 20 Help-seeking inclination, subjective mental health condition, social support, and perceived need to seek help are known to be significant predictors of help-seeking behavior. 22
Drawing from the outlined observations, we propose a conceptual model that integrates the aforementioned variables to explain help-seeking behavior among distressed, non-treatment-seeking young adults (D-NTS; Figure 1). These interactions are crucial in understanding the complex pathways that lead to or obstruct professional help-seeking behavior. Specifically, we hypothesize that distress perception (i.e., the awareness and acknowledgment of mental health concerns), help negation (i.e., the refusal or avoidance to seek professional help), and the inclination to seek help from MHPs are key predictors of help-seeking behavior in D-NTS. We posit that help negation has a direct relationship with help-seeking behavior, as individuals who exhibit increased levels of self-reliance or fear of judgment from others are less inclined to seek professional help, even when it is readily available. Additionally, we propose that help-seeking inclination, encouragement from SO to consult MHP, and stigma act as moderating variables. By integrating these variables, our model seeks to offer a comprehensive understanding of the aspects that impact help-seeking behavior for mental health in distressed young adults, specifically in contexts where mental health services are accessible but underutilized.
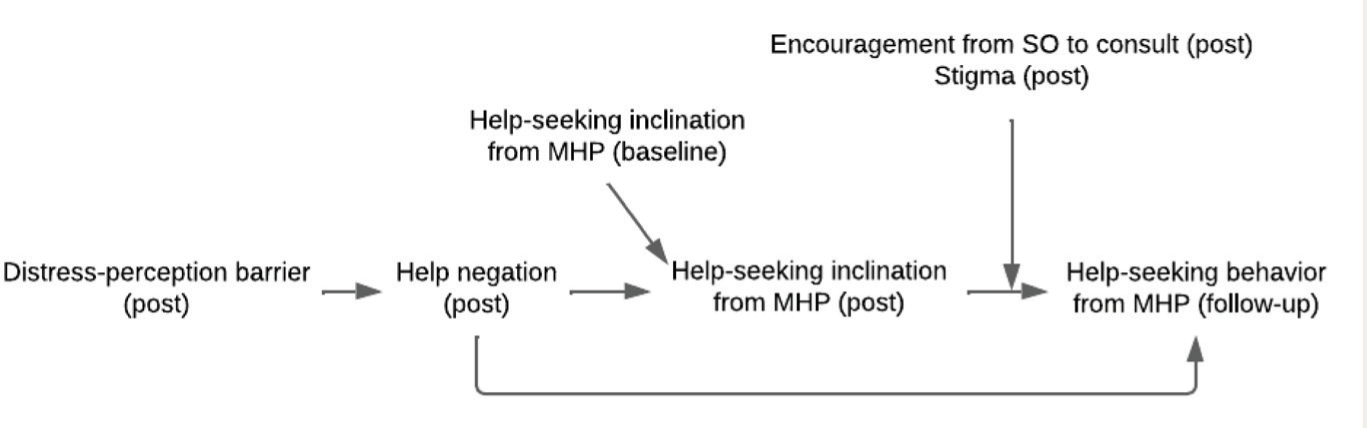
Although two moderators are presented together for clarity, they were tested separately.
Methods
Participants
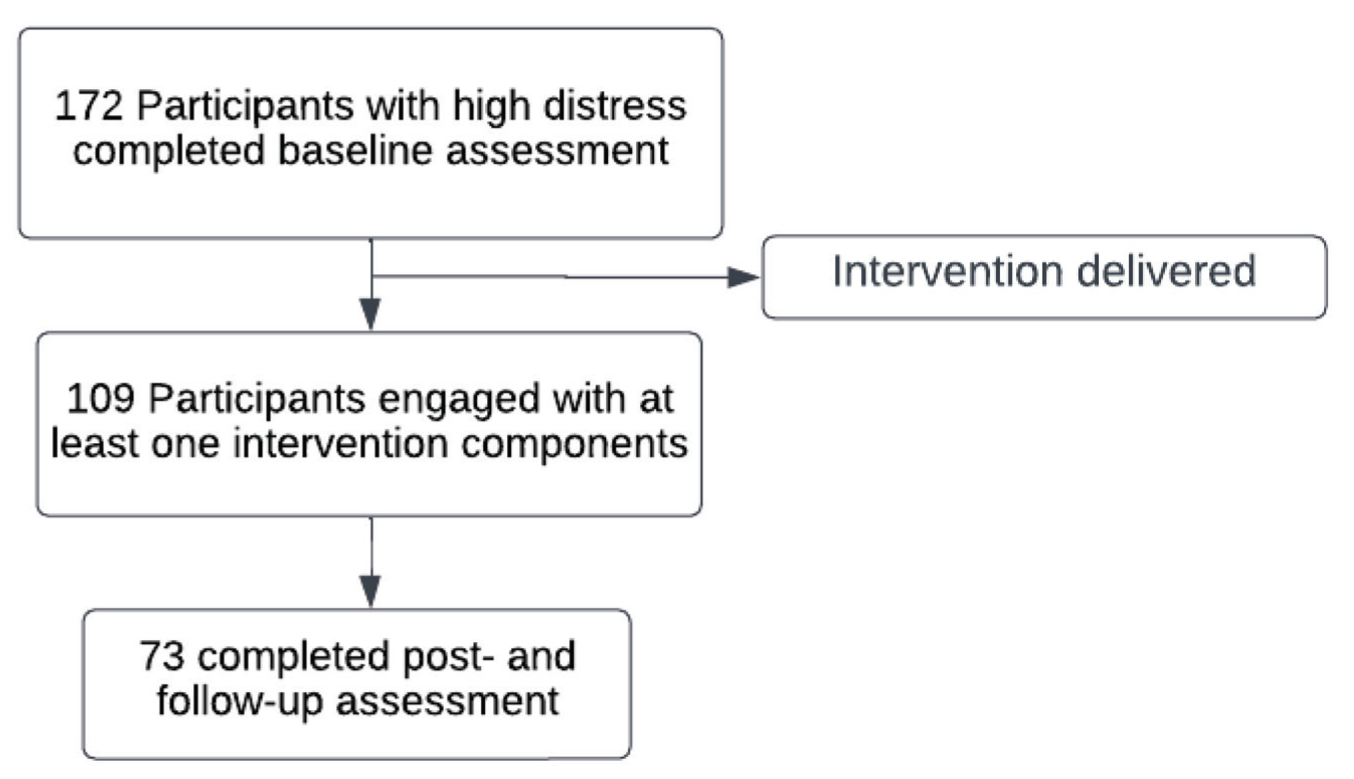
A single-group short-term prospective study design was used to identify factors influencing help-seeking behavior from MHPs among D-NTS following the ReachOut intervention through multi-point assessments. One hundred and seventy-two distressed non-treatment-seeking young adults (D-NTS) were recruited via purposive and snowball sampling using the following sample selection criteria mentioned in Box 1. Since this was a challenging-to-reach sample, snowball sampling, apart from purposive sampling, proved beneficial for recruiting distressed non-treatment seekers. Participants were asked to share the recruitment announcement with individuals they believed were in distress. They did not receive any compensation or incentives for participation. The sample size was calculated using G*Power software, version 3.1.9.7. Based on the research design, assuming 80% of the sample would exhibit help-seeking behavior during the intervention period and accounting for a 6% precision at a 95% confidence level, the minimum required sample size was calculated to be 171. Figure 2 illustrates the participant flow diagram throughout the study.
Participants Flow Throughout the Study.
Box 1. Sample Selection Criteria
Age range of 20–35 years
Formal education of at least 12 years
All genders
Self-reported psychological distress currently experienced for a minimum of two weeks.
A score above 20 on the Kessler Psychological Distress Scale (K10) 23 indicates psychological distress.
Not currently seeking professional help for the reported distress.
Proficient in the English language.
Access and comfort in using the internet
ReachOut (Help-seeking Intervention)
To improve professional help-seeking among distressed young adults, ReachOut was created as a WhatsApp-based intervention. It was developed and validated based on the literature review,24–26 relevant theoretical frameworks,4,9,27 preferences of young adults as assessed in an exploratory study, 28 and a priori guidelines. 25 The intervention incorporated eight core and one optional component, including personalized feedback, recognition of common mental health concerns, overcoming barriers to consulting an MHP, motivational interviewing, facilitating support mobilization from a nominated SO for professional help-seeking (optional), indirect social contact with mental health service consumers, socialization to the consultation process, experts’ views on mental health consultation and coordinated referral. A detailed procedure for delivering ReachOut is outlined in supplementary file 1. This intervention is intended for delivery by psychologists, counselors, health professionals, and trainers who have engaged in thorough preparation of the intervention’s themes. It aims to improve help-seeking in distressed young adults in community, educational, or workplace settings who are not currently seeking treatment. Individuals with formal training in psychiatry, psychology, social work, health education, counseling, or youth development may find it easier to deliver the intervention. The intervention was found to be successful in lowering professional help-seeking barriers and enhancing help-seeking inclination and behavior from MHPs. 29
Measures
The socio-demographic data sheet elicited details on age, gender, education, occupation, individual annual income, marital status, current living arrangement, and place of residence. It also contained an item to capture encouragement from SO to consult MHP for current distress with two options (“yes” or “no/can’t say”), which was also elicited at post-assessment.
Kessler Psychological Distress Scale (K10). 23 K10 is a self-report tool consisting of 10 items designed to assess distress stemming from anxiety and depressive symptoms experienced over the last four weeks. Participants rated their answers on a five-point Likert scale. Scores of 20 and below are indicative of a likely state of well-being, while scores above 20 indicate the presence of psychological distress. K10 has proven to be a valuable screening tool and was utilized in the WHO-WMH survey initiative across 28 countries.30,31 It has good psychometric properties in varied samples,32,33 including screening adolescents in India. 34 This measure was used to document the participants’ psychological distress levels at baseline to offer help-seeking intervention for those with high distress.
General Help-Seeking Questionnaire (GHSQ). 35 GHSQ measures current intention to seek help from various sources for various problems on a seven-point Likert scale from “extremely unlikely” to “extremely likely.” Instructions and help sources can be modified in this questionnaire to match the target population. The measure has been used in previous studies and found to have good convergent validity. 36 In the present study, the participants responded to the likelihood of seeking help from various sources, including help negation, keeping in view their current levels of distress at baseline and post-assessment.
As part of the current study, the Barriers to Seek Professional Help for Mental Health Scale (BSPH-MH), was developed and administered both at baseline and post-assessment. 37 The 28 items in the scale measured the reasons for not seeking professional help for current psychological distress. A five-point Likert scale, ranging from “not at all” to “to a great extent,” was used to score each item. The sub-scales consisted of stigma (eight items), distress perception (five items), apprehensions about service utilization (10 items), and instrumental barriers (five items). The scale’s overall reliability was good (α = 0.90), with sub-scale reliability ranging from α = 0.69 to 0.85. The total scores on the BSPH-MH scale showed a significant moderate positive correlation with the total K10 scores of the sample (ρ = 0.42, P < .001), which is in line with the available literature on the relationship between distress and barriers to seeking mental health-related help, 38 supporting the convergent validity of the tool.
Help-seeking behavior. At post-, one-month, and two-month follow-up assessments, a single-item question on MHP’s help-seeking behavior was asked, with a yes/no choice format depending on when they sought help. Data from all time points were combined for the analyses.
Procedure
The Institute Ethics Committee’s approval was obtained, and written informed consent was taken from participants before initiating the study. After conducting the baseline assessment, ReachOut was delivered in a spaced-out manner based on participants’ preferred communication mode over six to eight weeks. Google Forms was used to deliver each component as an attachment to verify engagement. Each component had a delivery window of five to nine days, with an average of seven days, depending on when the participant interacted with it. If any participant reported seeking professional help at any point during the study, the intervention was terminated. Post- and follow-up assessments were conducted at one-month intervals each while help-seeking behavior was also elicited by two-month follow-up. January 2021 marked the beginning of the data collection process, which ran until December 2021. The checklist on STROBE cohort reporting guidelines 39 has been included as a supplementary file 2.
Data Analyses
The analyses involved computing descriptive statistics such as mean and standard deviation. Further, inferential statistics, including Spearman’s rho correlation, logistic regression, and path analysis, were computed through IBM SPSS 20.0 and AMOS 23.0.
Results
During the baseline assessment, data was collected from 172 participants. Of these, 109 engaged with at least one of the intervention components. All subsequent analyses were carried out with these participants. A total of 73 participants completed post- and follow-up assessments. Table 1 shows the sample characteristics.
Sample Characteristics (N = 109).

Spearman’s correlation analyses were computed for the study variables, as shown in Table 2.
Spearman’s Correlation Analyses Among the Variables (N = 73).
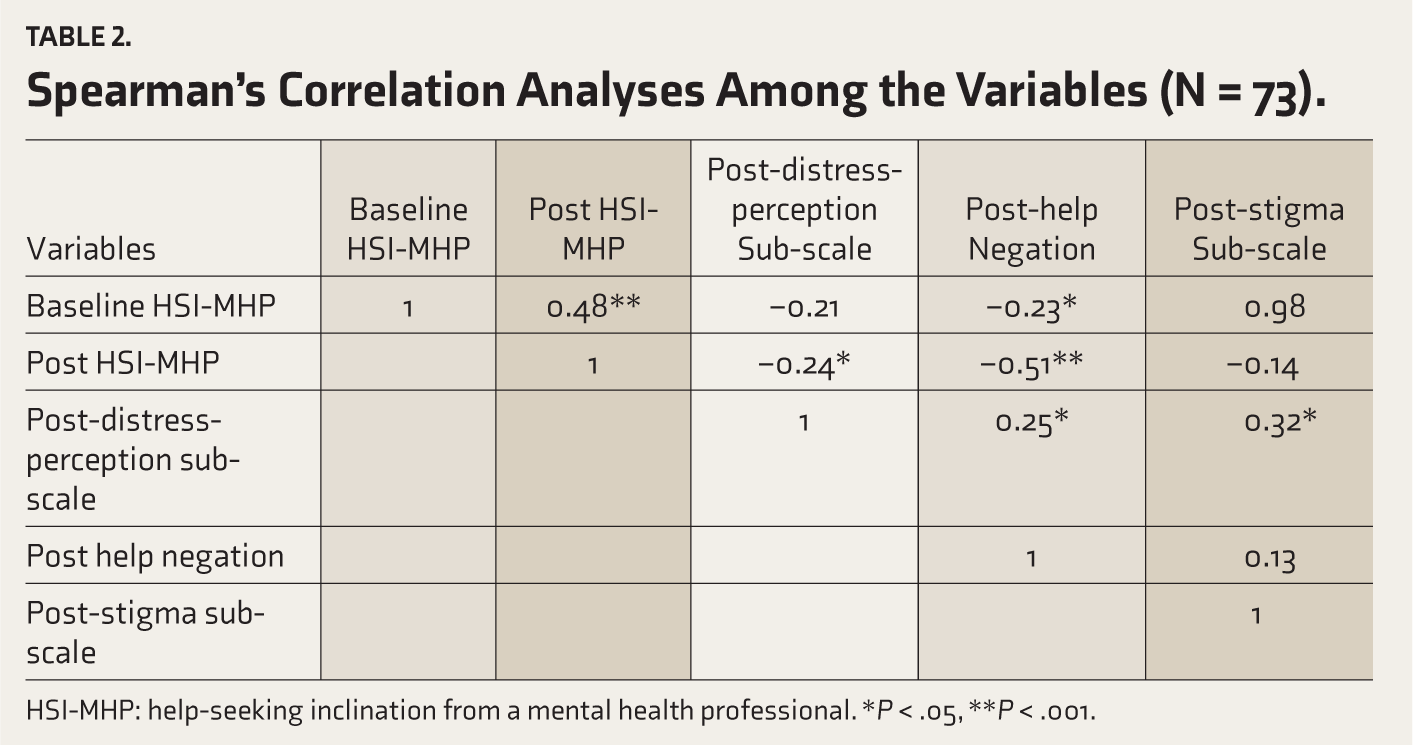
HSI-MHP: help-seeking inclination from a mental health professional. *P < .05, **P < .001.
Following the correlational analyses, logistic regression was computed with help-seeking behavior at follow-up as the dependent variable (Table 3). The dependent variable, help-seeking behavior, had two outcomes (yes/no). The overall regression model results were found to be significant (χ 2 = 34.53, P < .001).
Logistic Regression Model Result for Help-seeking Behavior at Follow-up (N = 70).
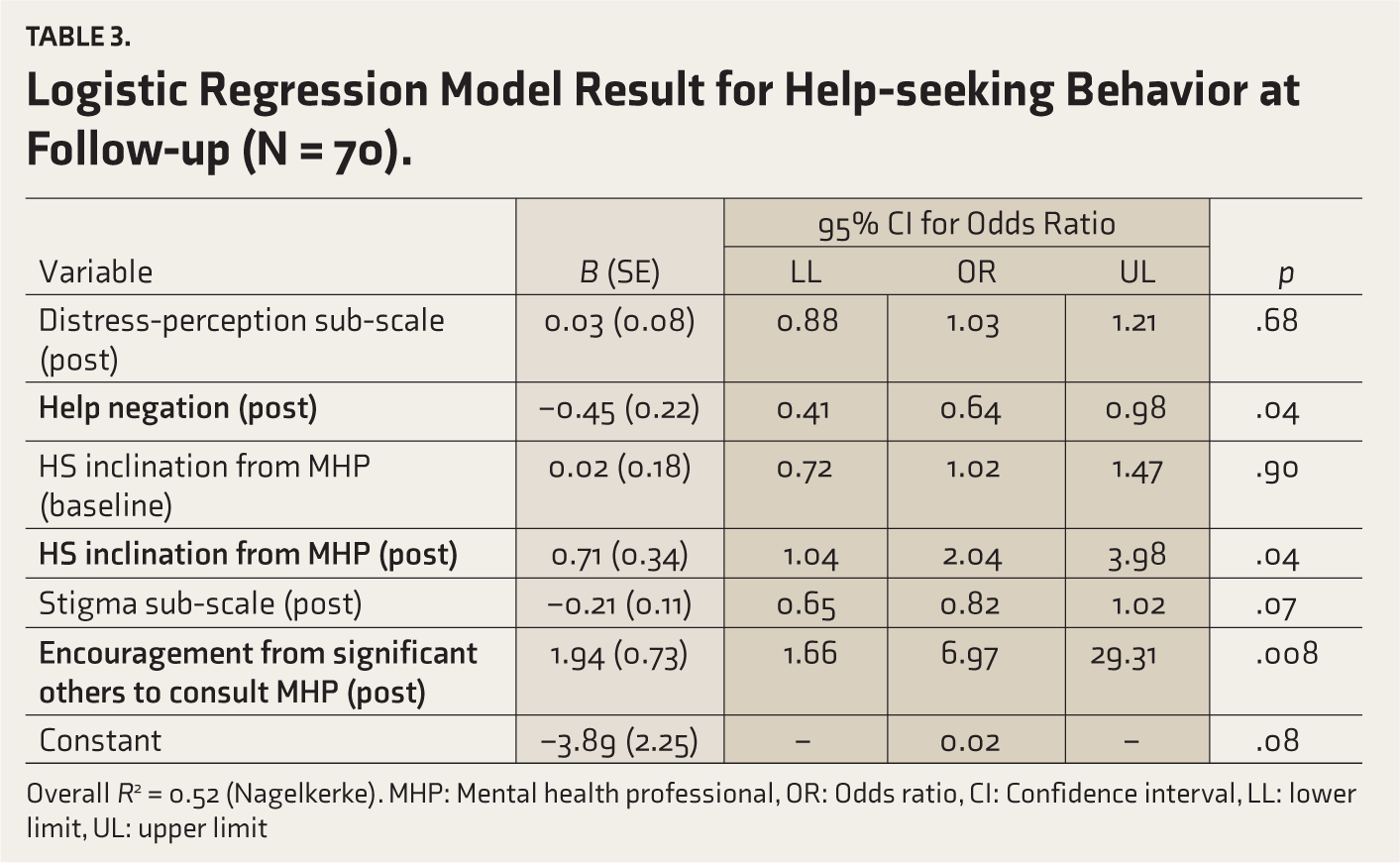
Overall R2 = 0.52 (Nagelkerke). MHP: Mental health professional, OR: Odds ratio, CI: Confidence interval, LL: lower limit, UL: upper limit
To identify factors influencing help-seeking behavior from MHPs among D-NTS following the ReachOut intervention, a path analysis for the hypothesized model shown in Figure 1 was conducted. We hypothesized that the distress-perception barrier, help negation, and help-seeking inclination from MHPs predict help-seeking behavior among D-NTS. Additionally, we proposed that help-seeking inclination, encouragement from SO to consult MHP, and stigma as barriers act as moderating variables. At the same time, help negation would have a direct relationship with help-seeking behavior. The goodness-of-fit (GOF) indices were used to assess the model’s fit, and the observed values indicated a good fit model based on the calculated values for the default model (Table 4). Figure 3 illustrates the relationship between the variables considered for the path analysis model.
Goodness-of-fit Indices of the Model.
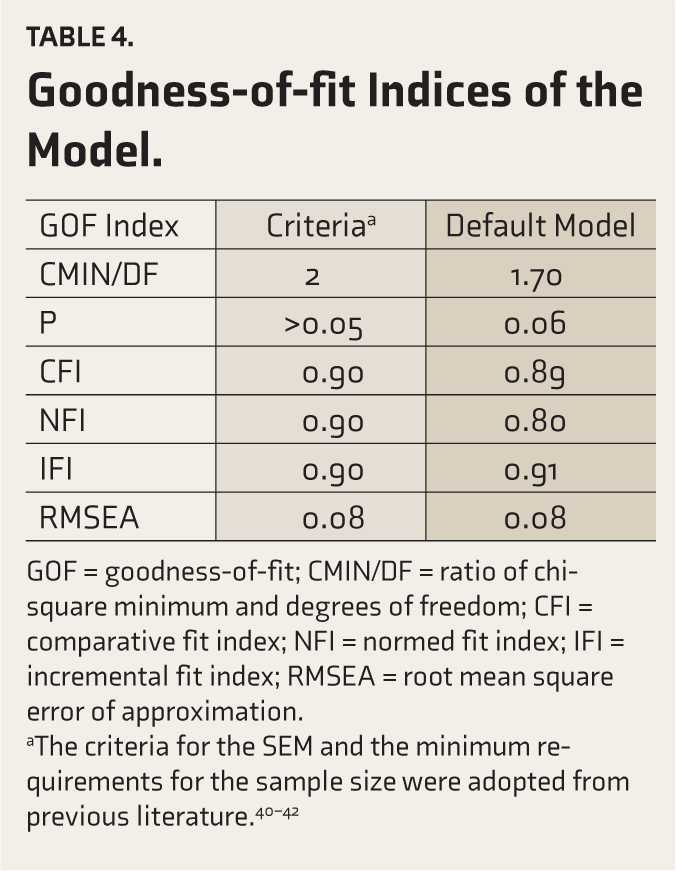
GOF = goodness-of-fit; CMIN/DF = ratio of chi-square minimum and degrees of freedom; CFI = comparative fit index; NFI = normed fit index; IFI = incremental fit index; RMSEA = root mean square error of approximation.
aThe criteria for the SEM and the minimum requirements for the sample size were adopted from previous literature.40–42
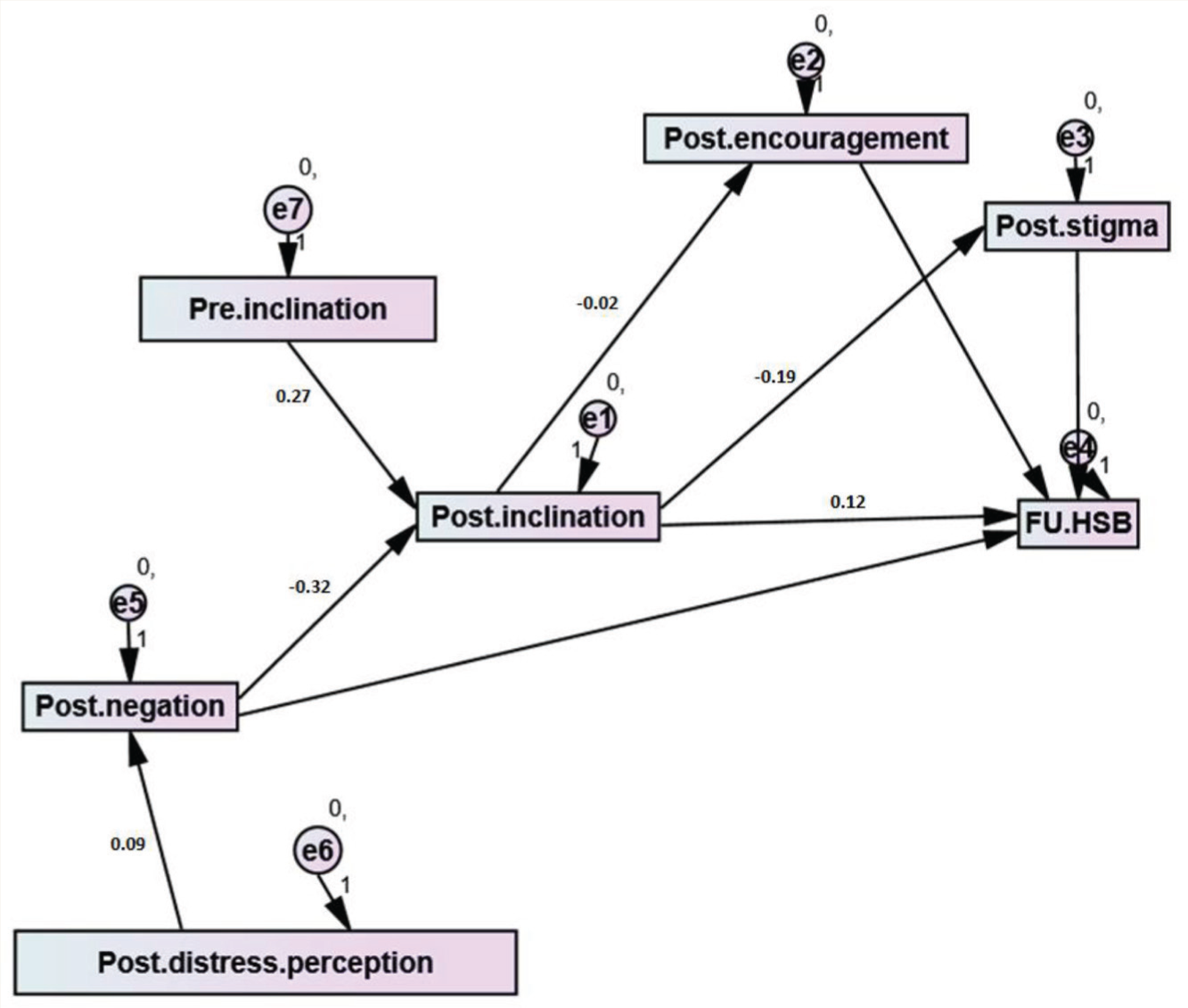
Post-distress perception = distress-perception barrier sub-scale at post-assessment; Post-negation = Help negation at post-assessment; Pre-inclination = Help-seeking inclination from MHP at baseline assessment; Post-inclination = Help-seeking inclination from MHP at post-assessment; Post-encouragement = Encouragement from nominated significant other at post-assessment; Post-stigma = Stigma barrier sub-scale at post-assessment; FU.HSB = Help-seeking behavior at follow-up.
Discussion
This study examined factors influencing help-seeking behavior from MHPs among D-NTS following the ReachOut intervention. The factors considered included barriers to distress perception and stigma, help-seeking inclination, help negation, and encouragement from SO.
Out of 172 D-NTS recruited for the present study, 109 engaged with at least one intervention component and were considered for further analysis. The majority of the participants were women. The sample was heterogeneous with regard to education, occupation, income, marital, and residential status, ensuring that the data included perceptions from a fairly diverse group of young adults.
Around two-thirds of them experienced severe distress, as reported on K10, and half of them received encouragement from their SO to consult MHP. Similarly, Santhya et al. 43 found that most young individuals who indicated the presence of mental health problems did not consider it “serious” enough to seek help. Normalization of distress has been one of the repeated themes described as a barrier in the theoretical and empirical literature on help-seeking.4,9 Denial and normalization of distress delay the awareness and recognition of one’s mental health problem. Other reasons include internal and external barriers, as well as how an individual evaluates the consequences of the decision to seek professional help. 9
The intercorrelations among the study variables suggest that they are significantly related to each other, and findings from logistic regression revealed help-seeking inclination from MHP, help negation, and encouragement from SO to consult MHP as significant predictors of help-seeking behavior. These results indicate that the ReachOut intervention could have influenced these outcomes. In the current study scenario, help negation can be interpreted against the backdrop of a strong propensity for self-reliance while handling mental health issues. It has been recognized as one of the main obstacles preventing young adults in India and throughout the world from seeking professional assistance.20,36 Self-reliance, however, is also seen as a component of resilience, having a favorable impact on recovery. 44 Therefore, ReachOut concentrated on using a range of resources to deal with distress and reducing the need to rely solely on self-reliance.
In the present study, stigma was one of the moderating variables leading to help-seeking behavior. Studies have often assessed stigma as a barrier in help-seeking interventions, 45 probably because perceived stigma and embarrassment are reported to be some of the most common barriers among young people. 46 Stigmatizing attitudes differ depending on the nature and severity of the illness. 47 In a randomized controlled trial, Stanley et al. 48 examined the impact of an intervention based on cognitive bias modification on stigma to seek help as a barrier among students. Their results revealed significant stigma reduction and improved help-seeking behavior among 25% of the participants at follow-up. Similar findings were obtained in studies assessing change in stigma or overall perceived barriers among adolescents following the intervention. 49 Based on the systematic review of the impact of stigma on help-seeking, 50 the authors noted the relationship between stigma and help-seeking in terms of (a) the dissonance that arises when an individual’s self- or social identity conflicts with prevalent stereotypes regarding mental health, (b) expectation/encounter of adverse outcomes, (c) desire/inclination for concealment of information, (d) strategies utilized to facilitate help-seeking, and (e) aspects of care that enable help-seeking. They also found strong evidence to support the premise that stigma related to mental health has a small to moderate impact on help-seeking in a negative manner.
Another moderating element in the current study was the encouragement of important others to consult MHP. Being in a collectivist culture like India may make it difficult to express one’s emotional issues and encourage others to get professional assistance. Poor psychological health can be linked to the ambivalence of wanting to express feelings and seek support for professional help but also being afraid of the repercussions of such expressions from loved ones. 51 Therefore, more research is required to develop strategies that can empower informal support providers—especially family members of young adults and youth experiencing distress—to encourage their loved ones to seek professional care. Encouragement from SO of distressed individuals to seek professional help can be improved through educative and promotive programs. Interventions directed at them can lead to higher encouragement to seek professional help.
We hypothesized that the distress-perception barrier, help negation, and help-seeking inclination from MHPs at post-assessment predict help-seeking behavior at follow-up among D-NTS. Additionally, baseline help-seeking inclination, encouragement from SO to consult, and stigma as a barrier at post-assessment act as moderating variables. At the same time, help negation would have a direct relationship with help-seeking behavior. Path analysis revealed that this model was a good fit, suggesting a complex process to decide to seek professional help. There appears to be a strengthening inclination to seek help from MHPs through the course of the intervention. However, there are a host of factors that may influence whether intentions are translated into behaviors/actions. Goal desire and commitment, goal difficulty, goal priority, and conflict are some of the moderators of the intention-behavior gap, and as the goal difficulty increases, the strength of intention to predict the behavior reduces. 52 The strength of the intention itself can be an important variable. It has been operationalized as “the quantity of personal resources that an individual is prepared to invest in executing a behavior.” 53 Intentions characterized by low strength may be temporally unstable and less resistant to external challenges and thus result in more intention-behavior gap.
The present study has certain limitations. Considering that the participation was voluntary, the intervention could have appealed more to those who were at least slightly inclined to seek professional help, thereby introducing some self-selection bias. Despite the sample’s heterogeneity, more research is required to determine whether the results are applicable to young adults from disadvantaged and rural areas who speak regional languages. The follow-up duration was chosen to balance attrition and sufficient time to engage in help-seeking behavior since longer follow-ups may lead to higher attrition. However, this period may not have been adequate for all participants who might require a longer duration to demonstrate help-seeking behavior following exposure to the intervention.
Nonetheless, the results have important implications for research, treatment, and policies that depend on proactive help-seeking processes initiated by distressed persons. 13 The evidence presented in this study is preliminary. A large randomized controlled trial would help to systematically examine the intervention’s effects by including help-seeking behavior as the primary outcome variable. The results indicate that to encourage young adults to seek professional assistance, it is crucial to realize the importance of developing trustworthy relationships that allow them to freely express their problems in their informal networks. Systematic and sustained attention is required to reduce demand-side barriers (in addition to supply-side barriers) related to the treatment gap in the country. Governmental support for implementation and impact assessment of large-scale public health interventions to improve help-seeking in young adults as a complementary strategy to addressing the shortage of qualified healthcare providers can go a long way in reducing the hidden disease burden in mental health and associated productivity and economic loss in the country.
Conclusion
The help-seeking decision is a complex process impacted by the intricate interplay of various internal and external factors. A comprehensive examination of these factors simultaneously provides valuable insights for tailoring interventions and support strategies aimed at enhancing help-seeking behavior among D-NTS.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
The first author gratefully acknowledges the grant provided by the Indian Council of Medical Research, New Delhi for her doctoral work on help-seeking in distressed young adults.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Declaration Regarding the use of Generative AI
None used.
Funding
The first author received a fellowship from the Indian Council of Medical Research to pursue her PhD course under the supervision of the third and fourth authors and the present study forms a part of the PhD work. However, the funder had no role in study design, data collection, analysis, decision to publish or preparation of the manuscript.
Ethical Approval
Ethics approval was obtained from the Institute Ethics Committee of NIMHANS (Approval no.: NO.NIMH/DO/IEC (BEH. Sc. DIV)/2019).
Informed Consent
A written informed consent was solicited from the study participants before initiation.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.