
Abstract
Purpose of the Review:
Functional near-infrared spectroscopy (fNIRS) is a non-invasive, portable, and cost-effective neuroimaging tool for monitoring brain activity in real-world settings. Its advantages make it promising for clinical use in assessing major depressive disorder (MDD). This review evaluates current literature on the utility of fNIRS in MDD.
Collection and Analysis of Data:
Following PRISMA guidelines, English-language studies (2011–2025) from MEDLINE, ScienceDirect, and EMBASE were reviewed. Inclusion criteria: Studies using fNIRS to (a) differentiate MDD from controls, (b) correlate cerebral activity with symptoms, (c) monitor treatment response, or (d) distinguish MDD from other psychiatric disorders.
Results:
Of 6,312 records, 166 studies met the inclusion criteria. Most found reduced oxygenated hemoglobin (oxy-Hb) responses in prefrontal regions during cognitive and emotional tasks in MDD, especially on verbal fluency. Greater depression severity correlated with lower oxy-Hb, which increased as symptoms improved. fNIRS may also help distinguish MDD from other psychiatric disorders.
Conclusions:
fNIRS reliably detects reduced prefrontal activation in MDD, reflecting illness severity and treatment response. However, methodological differences limit broader clinical use. Standardized protocols and larger studies are needed for routine clinical adoption.
Major depressive disorder (MDD) is a top contender for mental health issues, causing substantial morbidity and mortality globally.1,2 Functional brain imaging techniques such as quantitative electroencephal ography (qEEG), functional magnetic resonance imaging (fMRI), single-photon emission computed tomography (SPECT), positron emission tomography (PET), and magnetoencephalography (MEG) provide insight into cortical and subcortical brain activity patterns associated with MDD, enabling the development of putative biomarkers for diagnosis and prediction of therapeutic outcomes. 3 Hemodynamic imaging studies using PET, SPECT, and fMRI consistently report reduced activity in the prefrontal cortex (PFC) and cingulate cortex in MDD, findings that align with observed deficits in cognitive performance and diminished prefrontal activation during cognitive tasks. 4 However, the widespread clinical application of these techniques is limited by high cost, lack of portability, and operational complexity.
Functional near-infrared spectroscopy (fNIRS) has emerged as a non-invasive alternative to functional neuroimaging for assessing cerebral hemodynamics in psychiatric populations. It operates in the near-infrared spectral range (650–1,000 nm), enabling estimation of oxygenated (oxy-Hb) and deoxygenated (deoxy-Hb) hemoglobin concentrations by differential light absorption, using the modified Beer–Lambert law. Although fNIRS is limited by relatively low spatial resolution and shallow penetration depth, it offers notable advantages, including lower cost, portability, ease of use, absence of ionizing radiation, and tolerance for movement. These features make it particularly suitable for psychiatric patients who may be sensitive to confinement or scanner noise. 5
fNIRS studies in MDD commonly employ cognitive activation paradigms such as the verbal fluency task (VFT) and the working memory task (WMT) to elicit prefrontal hemodynamic responses. 6 Beyond depression, fNIRS has been used to characterize prefrontal hemodynamic patterns across various psychiatric conditions, facilitating differentiation between MDD and disorders such as schizophrenia (SCZ) and bipolar disorder (BD). 7 Recent research, including meta-analyses and systematic reviews, indicates that individuals with MDD show consistently reduced prefrontal activation during cognitive tasks, reflected by attenuated increases in Oxy-Hb compared with healthy controls (HCs). These findings support the potential of fNIRS as an objective tool for diagnosing MDD and monitoring treatment response.5,7,8 Given the substantial increase in published studies, further systematic evaluation of the accumulating evidence is warranted. In particular, there is a need to assess the utility of fNIRS in differentiating MDD from HCs and other psychiatric disorders, as well as to clarify its relevance to specific symptom dimensions and treatment response.
Hypotheses and the Objectives of the Review
There has been intensive research in this field over the past few years, and thus we decided to update on the use of fNIRS in MDD. This review aims to systematically examine: (a) the utility of fNIRS in distinguishing individuals with depression from healthy individuals; (b) the associations between fNIRS-derived hemodynamic signals and depressive symptomatology; (c) the application of fNIRS in monitoring and predicting treatment response in depression; and (d) the capacity of fNIRS to differentiate depression from other psychiatric disorders.
Methods
Data Sources and Search Strategy
This study was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) and was registered at PROSPERO (registration number: CRD420250651250). The systematic review includes peer-reviewed, English-language publications published between 2011 and March 2025. The electronic databases searched were MEDLINE, ScienceDirect, and EMBASE. The MeSH terms used were ‘spectroscopy’ OR ‘near-infrared’ OR ‘near-infrared spectroscopy’ OR ‘optical topography’ OR ‘fNIRS’ OR ‘NIRS’ AND ‘depression’ OR ‘major depressive disorder’ OR ‘depressed’ OR ‘depressive disorder’ OR ‘mood disorder’ OR ‘affective disorder’. Terms were searched as both text words and subject headings. Bibliographies of relevant articles were also manually reviewed to identify related publications. Details of the systematic search approaches have been provided in the supplementary data.
Eligibility Criteria and Data Extraction
Studies were eligible if they assessed cerebral hemodynamic variations using fNIRS in individuals with MDD across any age group. Full-text articles were retrieved for detailed evaluation when applicable. Conference proceedings and gray literature were excluded. Studies meeting the inclusion criteria underwent full-text review, and study characteristics and results were extracted. Discrepancies in study selection were resolved through discussion between both reviewers (RV and SK). Where necessary, corresponding authors were contacted for supplementary data or full-text access.
Quality Assessment
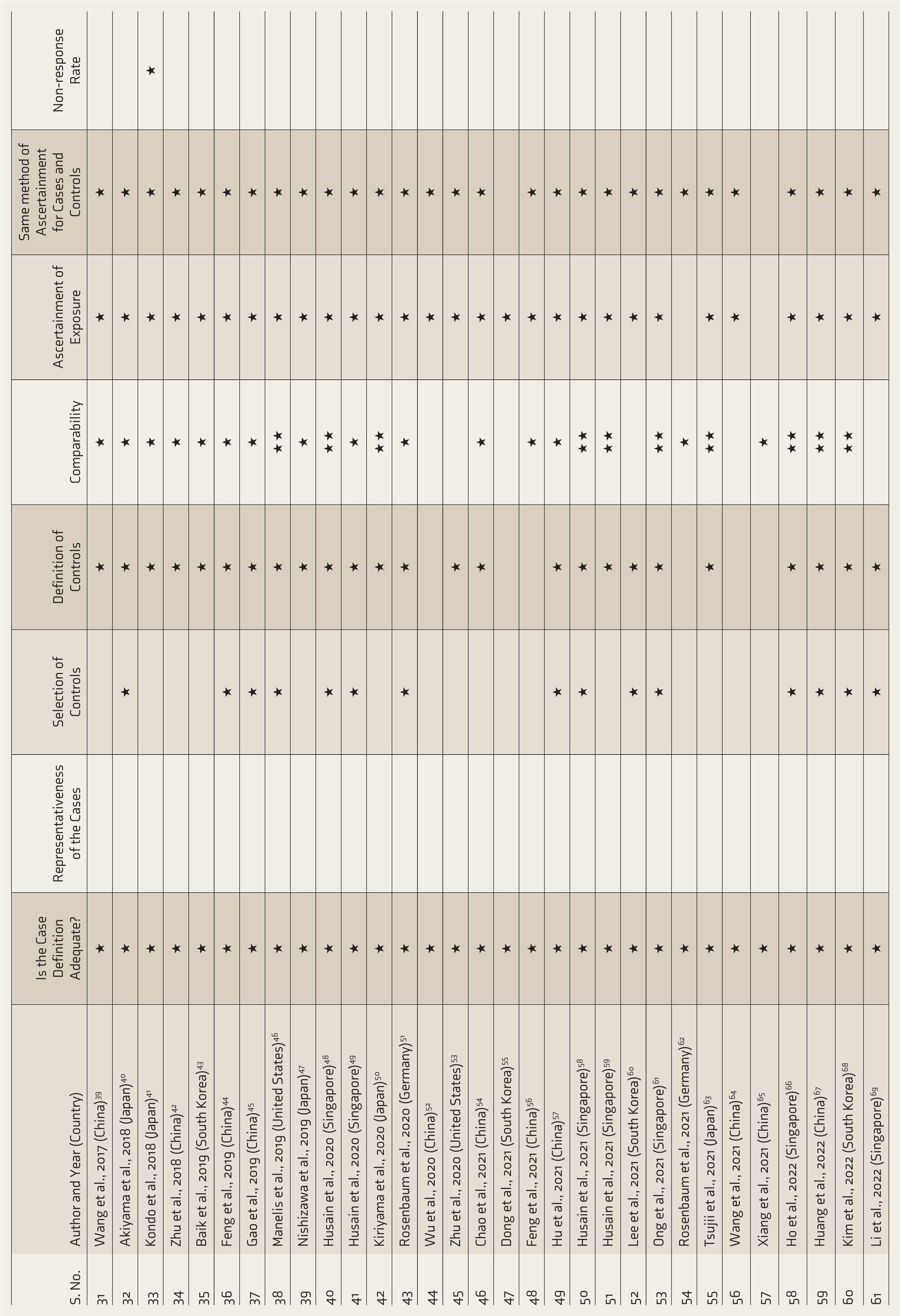
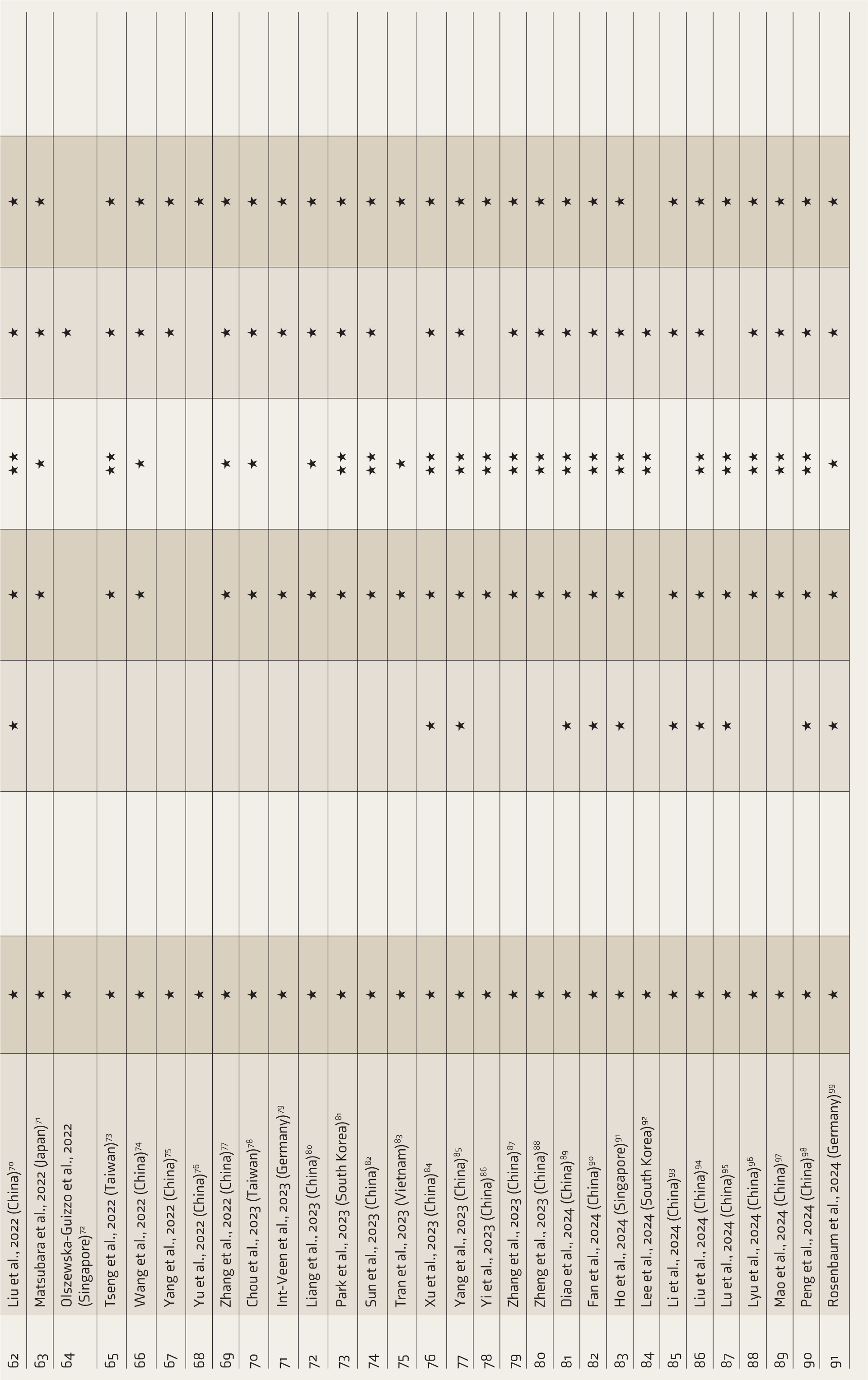
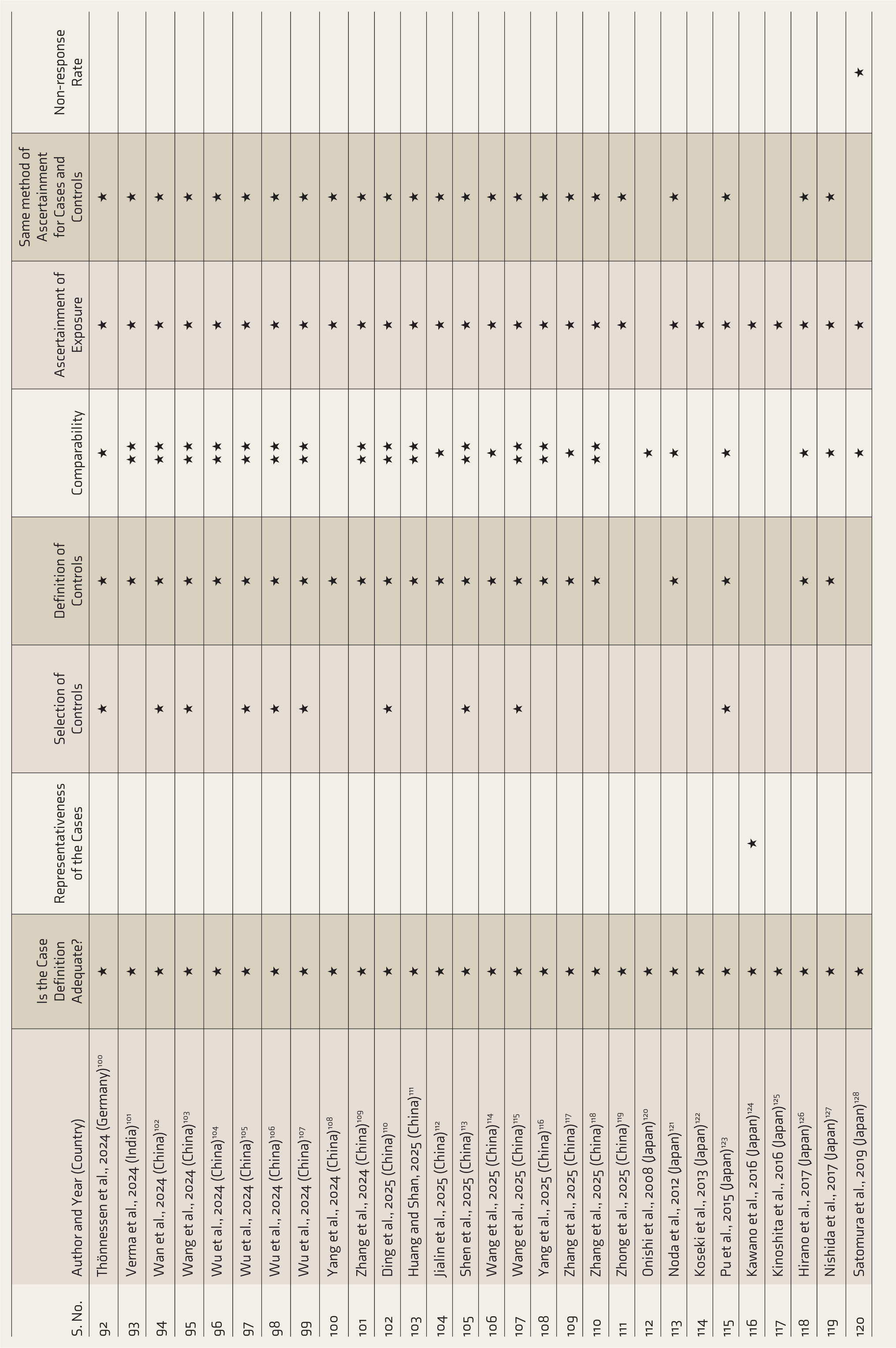
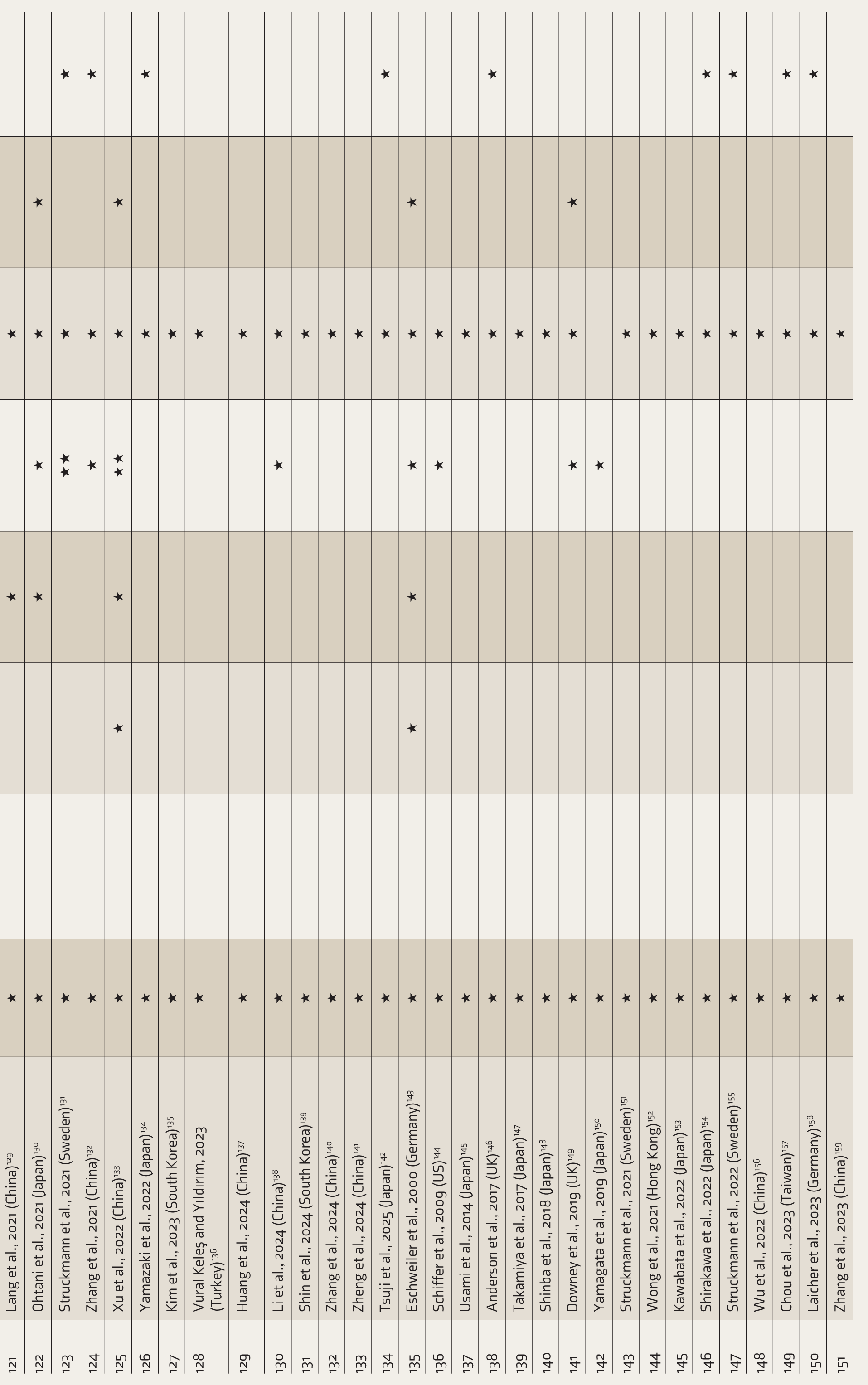
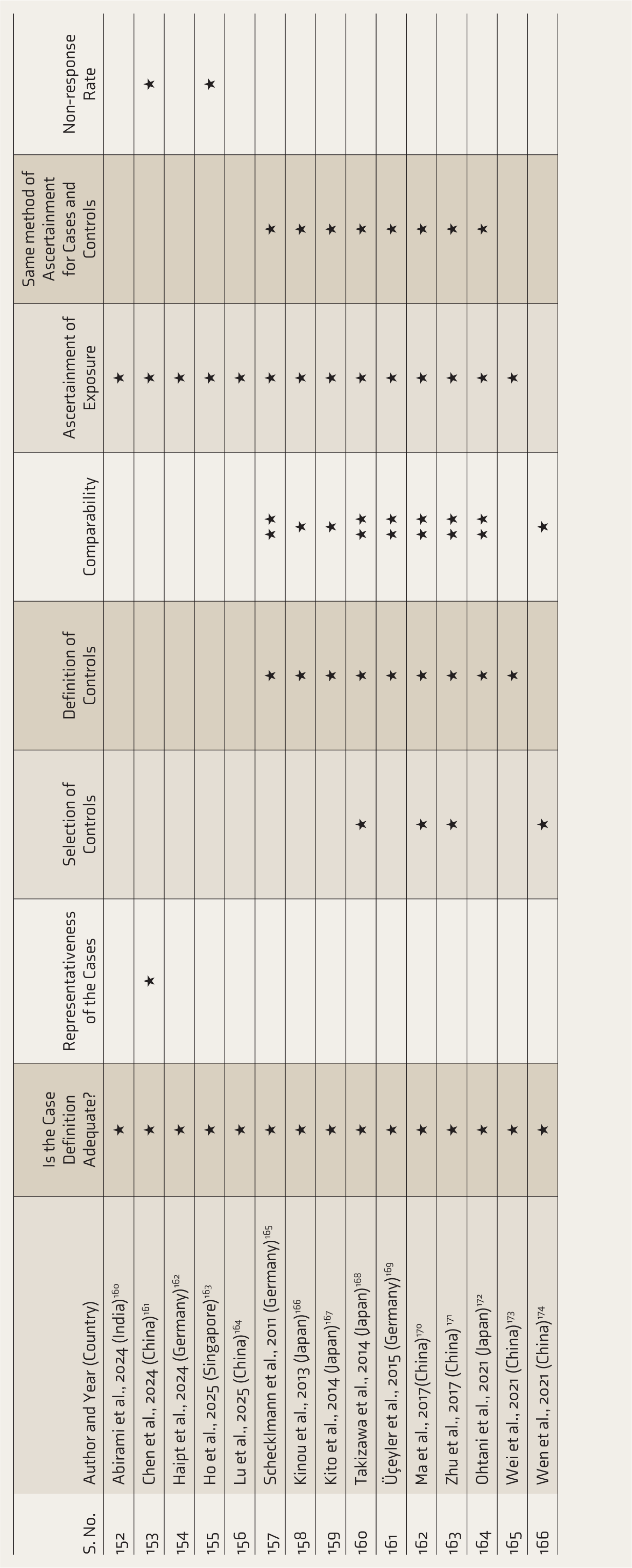
The methodological quality of the studies was assessed using the Newcastle– Ottawa Quality Assessment Scale (NOQAS), as shown in Table 1. It has eight items within three domains: selection (representativeness), comparability (ascribed to design or analysis), and outcomes (assessment and follow-up). A study can receive one star for meeting each criterion, except for comparability, which can receive a maximum of two stars depending on the number of controlling factors. While categories exist, there is no single, universally agreed-upon cutoff for ‘good’ and ‘poor’. Some researchers have categorized ratings as of poor quality (0–2), fair quality (3–5), and good/high quality (6–9). The reviewers worked independently, and discrepancies were resolved by discussion.
Assessment of Risk of Bias Using the Newcastle–Ottawa Quality Assessment Scale (NOQAS).

Results
Study Selection
A total of 6,312 records were identified through database searches in MEDLINE, ScienceDirect, and EMBASE. After removing duplicates, 1,744 articles remained for title and abstract screening. Of these, 166 studies met the inclusion criteria and were included in the analysis. The selection process is illustrated in Figure 1, following the PRISMA guidelines. Sixty-five studies were from China, 55 studies were from Japan, 13 studies were from Germany, 10 were from Singapore, eight were from South Korea, three from Sweden, three from Taiwan, two from the United States of America (USA), two from the United Kingdom (UK), two from India, one from Vietnam, one from Turkey and one from Hong Kong.
PRISMA Flow Diagram Depicting the Literature Search.

Sixty-nine types of devices have been used in these studies to measure changes in oxy-Hb concentration. The vast majority of studies have used a continuous-wave (CW) fNIRS system. The details of devices and associated wavelengths utilized are provided in the supplementary file (Supplementary Table S1).
Use of fNIRS to Differentiate Depressed from Healthy Individuals
Of the 111 articles that used fNIRS to differentiate between depressed patients and HCs (Supplementary Table S2), most were conducted in China (n = 50) and Japan (n = 32). The entire sample included a total of 7,465 individuals with depression and 6,040 HCs. fNIRS has been extensively applied to differentiate individuals with depression from HCs across task-based, resting-state, and machine learning (ML)–driven paradigms, with consistent evidence of altered prefrontal and frontotemporal hemodynamics.
Differentiation Through VFT-based fNIRS
VFT is the most widely used paradigm, with the majority of studies reporting reduced oxy-Hb concentrations in depressed individuals compared with HCs. This hypofrontality is observed in major and minor depression, first-episode and recurrent depression, and in medication-naïve samples, though effects are typically more pronounced in MDD.16,24,60,73,75,80,93,109 Reduced activation commonly involves the dorsolateral prefrontal cortex (DLPFC), frontopolar cortex (FPC), inferior frontal gyrus (IFG), ventrolateral PFC (VLPFC), and Broca’s area.56,63,84,109,115 Gender differences have been noted, with females often showing greater frontal reductions.52,96,117 Treatment-resistant depression (TRD) exhibits distinct activation patterns but remains hypoactive relative to HCs. 73 Large-sample studies confirm that hemodynamic reductions scale with diagnostic certainty and severity. 105
Differentiation Through Emotion Tasks Based on fNIRS
Emotion-related paradigms reliably distinguish depressed individuals from HCs, particularly through abnormal frontal activation to emotional stimuli. Depression is associated with reduced left frontal activation to negative stimuli and reduced right frontal activation to positive stimuli, with task and emotion-specific asymmetries.25,47 Differences are also observed in facial emotion recognition, autobiographical memory, and emotional picture description tasks.46,75,77,87,88,118 Bilateral differential activity in the frontal region, particularly the FPC, for depression and HCs has also been reported by others using a facial emotion recognition task or emotion word test.66,97;71,102 Functional connectivity (FC) analyses reveal altered frontal–temporal coupling during emotional processing. 108 These findings highlight disrupted emotional regulation networks in depression.
Differentiation Through Other Cognitive Tasks Based on fNIRS
During Stroop,23,83,101 working memory,18,21,42,94,111 trail-making, 28 and decision-making tasks, depressed individuals generally show reduced frontal oxy-Hb responses compared with HCs. However, some tasks reveal compensatory hyperactivation under higher cognitive load. Reduced FC in frontoparietal networks during tasks and altered resting-state connectivity have also been reported. 33 Less commonly used paradigms (e.g., conversation, motor, gambling, and auditory tasks) consistently indicate frontal hypoactivation in MDD.26,59,73,100,107
Differentiation Through Resting State-based fNIRS
Resting-state studies largely focus on FC, reporting reduced prefrontal and frontotemporal connectivity in depression, particularly in individuals with non-suicidal self-injury (NSSI).95,98,106 Network analyses suggest altered efficiency and small-world properties of prefrontal networks in MDD. 52
Differentiation Through the Parietal and Occipital Regions Related to fNIRS
Parietal fNIRS studies show disrupted connectivity within the frontoparietal and default mode network (DMN), especially during rest and stress-related tasks.33,37,48,51,62,79,99 Occipital region studies are limited but suggest altered connectivity related to prenatal depression exposure and reduced activation during environmental interventions.72,74,100
Differentiation Through fNIRS-based ML
ML approaches using fNIRS data have achieved high accuracy in distinguishing between depressed individuals and HCs. Models using VFT, emotion-based, and multimodal data (combining fNIRS with clinical variables or EEG) report accuracies ranging from ~83% to >95%.66,86,92,97,113,114 Advanced methods, including convolutional neural networks, graph neural networks, and ensemble models, identify key frontal regions (FPC, DLPFC, IFG) as critical biomarkers, supporting fNIRS as a promising objective screening and diagnostic adjunct.53,76 By integrating phase space reconstruction (PSR) and multi-objective metaheuristic optimization (MOMVO), researchers have achieved a classification accuracy of 0.96 on emotion-based task fNIRS data. 119
Overall, fNIRS consistently reveals task and region-specific hypoactivation and connectivity abnormalities in depression, with growing evidence for its clinical utility when combined with ML techniques.
Use of fNIRS Signals in Assessing Depression Symptoms
We identified 62 papers on the utilization of fNIRS to study cerebral hemodynamic changes with depression symptomatology (Supplementary Table S3), with a total of 3,980 patients with depression, mostly from Japan (n = 27) and China (n = 23). fNIRS has been extensively used to evaluate illness severity and associated clinical dimensions in MDD, particularly through prefrontal hemodynamic responses.
Evaluating Illness Severity Using fNIRS
Most studies report a significant negative correlation between oxy-Hb concentrations, especially in the DLPFC, and depressive symptom severity. However, some findings show positive or nonsignificant correlations,29,30,33,34,43,73,93 possibly due to small sample sizes or methodological variability. Reduced prefrontal activation has also been associated with greater suicidal severity.31,82,103,139 Differences have been observed between melancholic and non-melancholic depression, suggesting distinct neurophysiological subtypes. 27 Severity-related reductions in activation have been documented in the FPC, DLPFC, and inferior PFC, with more pronounced hypofrontality in severe versus mild depression. 142 Family history of psychiatric disorders has been linked to greater prefrontal dysfunction. 36 ML models combining temporal and correlation features of fNIRS signals have demonstrated improved accuracy in distinguishing mild from severe depression. 137
Evaluating Suicidality in MDD Using fNIRS
Prefrontal asymmetry and altered activation patterns are strongly associated with suicidal ideation and behavior. 43 Reduced oxygenation in the PFC, particularly the left VLPFC, mediates the relationship between depression severity and suicidal ideation.60,68 High suicide-risk groups exhibit distinct activation patterns in the DLPFC, OFC, FPC and left precentral gyrus.31,38,135 Individuals with prior suicide attempts or NSSI show altered frontotemporal FC and reduced hemodynamic responses in motor and frontal regions, suggesting potential biomarkers for suicide-risk stratification. 56 The right MFR was reported to be more activated in the self-harm group than in the non-self-harm group during the VFT assessments. 140
Evaluating Sleep in MDD Using fNIRS
Sleep disturbances in MDD are associated with altered prefrontal activation. Some studies report increased oxy-Hb in the right DLPFC in depressed individuals with insomnia, 84 whereas others show reduced bilateral DLPFC and medial PFC activation. 138 Sleep quality scores correlate with prefrontal reactivity, indicating that cortical oxygenation is sensitive to sleep complaints. 127
Appraising Psychomotor Retardation in MDD Using fNIRS
Psychomotor retardation correlates with region-specific hemodynamic changes, differing between melancholic and non-melancholic subtypes: It shows a positive correlation with mean oxy-Hb changes in the right temporal region in melancholic subtypes and a negative correlation with mean oxy-Hb changes in the frontal and left temporal regions in non-melancholic subtypes. 27
Appraising the Impact of Coexisting Anxiety Symptoms in MDD Using fNIRS
Coexisting anxiety and obsessive-compulsive symptoms are linked to prefrontal hypoactivation and altered resting-state FC, including disruptions in DMN and frontoparietal networks.24,33,37
Evaluating the Relationship of Social Functioning in MDD Using fNIRS
Prefrontal and temporal activation patterns correlate with social functioning scores, 26 with reduced activation associated with poorer adaptation. 123 Improvements in social functioning are linked to longitudinal increases in VLPFC and anterior temporal cortex (aTC) activation. 30
Appraising the Relationship of Cognitive Functioning in MDD Using fNIRS
Cognitive performance, including working memory and verbal learning, shows associations with prefrontal activation and frontotemporal connectivity.95,136 Oxy-Hb levels may also partially mediate the relationship between anhedonia and cognitive impairment. 80
Evaluating the Impact of Coping Strategies in MDD Using fNIRS
Task-oriented coping styles correlate positively with prefrontal hemodynamic responses. 20 Early-life emotional abuse is negatively associated with cortical oxygenation. 99
Evaluating Impact of Age and Gender in MDD Upon fNIRS
Age-related differences reveal opposite DLPFC activation trends in younger versus older individuals as severity increases. 139 Gender differences have also been observed, with females showing lower bilateral DLPFC activation compared to males. 141
Overall, fNIRS provides valuable neurophysiological markers associated with symptom severity, suicidality, sleep disturbance, cognitive and social functioning, and demographic factors in MDD, supporting its role as a potential objective adjunct tool in clinical assessment.
Use of fNIRS to Monitor Treatment Response
We identified 36 papers on the utilization of fNIRS to monitor various treatment responses for MDD (Supplementary Table S4) with a total of 1,083 individuals with MDD, mostly from Japan and China. fNIRS has been widely used to evaluate neurophysiological changes associated with treatment response in MDD, particularly in relation to symptom reduction, social functioning, and alternative interventions.
Evaluating Impact of Symptom Reduction After Treatment Using fNIRS
Most studies report increased prefrontal hemodynamic responses alongside reductions in depressive symptoms following pharmacological and non-pharmacological treatments. However, some exceptions exist. Ketamine augmentation of electroconvulsive therapy (ECT) did not improve depressive symptoms in one study, 146 and intermittent theta-burst stimulation (iTBS) showed no meaningful changes in cognitive performance or oxy-Hb levels. 131 Similarly, reduced oxy-Hb responses during VFTs were observed after ECT without corresponding mood or cognitive improvements. 149 Conversely, several studies found that responders to repetitive transcranial magnetic stimulation (rTMS) or antidepressant treatment exhibited significant reductions in prefrontal activation during VFT, suggesting normalization of hyperactivation.154,164 Antidepressant dosage was negatively correlated with oxy-Hb in temporoparietal regions, indicating that medication load influences fNIRS findings. 147 Most participants across studies were medicated, though a few investigations included medication-naïve or medication-free individuals. In medication-naïve patients, early oxy-Hb changes predicted later improvements in HAMD scores. 150 After cognitive behavioral therapy (CBT) and hypnotherapy treatments, results showed a significant reduction in both groups on a symptom level. 162
Baseline fNIRS measures may also predict treatment response. Greater pre-treatment oxy-Hb concentrations in temporal and prefrontal regions were associated with better clinical outcomes. 32 Repeated findings of persistent prefrontal hypoactivation during VFT suggest that hypofrontality may represent a trait marker of depression rather than solely a state-dependent change.35,67,145,148,153,163,164
Evaluating the Impact of Social Functioning Improvement After Treatment Using fNIRS
fNIRS has also been linked to improvements in social functioning. Increased social adaptation scores were positively correlated with symptom improvement and negatively correlated with pre-treatment right VLPFC activation. 123 These findings suggest that baseline prefrontal activation patterns may help predict functional recovery, particularly in late-onset depression.
Evaluating the Impact of Alternative Treatment Strategies Using fNIRS
Emerging research has explored neural changes following alternative interventions. Mindfulness-based emotion regulation training was associated with increased activation in bilateral IFG and DLPFC, 158 with gradual reductions in DLPFC oxy-Hb across sessions, potentially reflecting improved neural efficiency. In a case study examining yoga, decreased deoxy-Hb and increased oxy-Hb were observed in the PFC during and immediately after practice. 160 fNIRS has also been utilized to predict treatment responses from other treatments such as therapeutic garden, 72 music therapy, 44 acupuncture, along with antidepressants, 152 solution-focused brief therapy and psychodynamic psychotherapy, 161 and hypnotherapy. 162
Overall, fNIRS demonstrates sensitivity to treatment-related neurophysiological changes in MDD, with potential utility in predicting treatment response, monitoring symptom and functional improvement, and evaluating novel therapeutic approaches.
Use of fNIRS to Differentiate MDD from Other Psychiatric Disorders
All 34 studies focused on using fNIRS to differentiate between cerebral hemodynamic changes in depression with changes in other psychiatric disorders (Supplementary Table S5), with a pooled sample of 1,314 individuals with MDD and 2,064 HCs. Most of the studies were conducted in China and Japan. fNIRS has demonstrated utility in differentiating MDD from other psychiatric and neurological conditions based on distinct hemodynamic response patterns, particularly within the PFC.
Differentiation from SCZ Utilizing fNIRS
Most studies report significant differences in prefrontal hemodynamic responses between MDD and SCZ. Distinct regional patterns have been observed, with altered FPC activation more characteristic of SCZ, as well as DLPFC and VLPFC alterations more prominent in MDD. 166 SCZ has also been associated with reduced DLPFC activation and lower activity in temporal regions compared to MDD.65,89 Network-based metrics derived from FC analyses further enhance classification among MDD, SCZ, and HCs. 52 Additionally, reduced prefrontal activity in individuals with a family history of SCZ suggests that greater genetic loading may contribute to more pronounced prefrontal dysfunction in major psychiatric disorders. 36
Differentiation from BD Utilizing fNIRS
Several studies indicate that frontal hemodynamic patterns can distinguish MDD, BD, and SCZ with reasonable accuracy.168,173 Distinct activation profiles, particularly in the frontopolar and frontotemporal regions, have been reported between BD and MDD.42,71 BD is often characterized by broader or more pronounced PFC dysfunction. 58 Emotional processing tasks, such as the Emotional Stroop Test, reveal differential oxy-Hb and deoxy-Hb responses between BD and MDD, particularly in response to positive stimuli, suggesting possible trait-related neural differences. 25 The left OFC has been identified as a sensitive region for differentiating BD from HCs during VFT, supporting the potential of fNIRS as an adjunct diagnostic tool, especially in low-resource settings. 83 However, some cognitive paradigms, such as WMTs, have shown limited specificity in distinguishing BD from MDD. 165
Differentiation from Anxiety Disorder Utilizing fNIRS
In generalized anxiety disorder (GAD), right-lateral PFC oxy-Hb changes correlate with anxiety severity, whereas bilateral and anteromedial PFC activation is more closely linked to depressive severity. 24 Both MDD and GAD show reduced activation in the DLPFC, OFC, and left VLPFC, though subtle regional differences may exist.103,113 High classification accuracies have been reported when distinguishing anxiety, depression and HCs using predictive models. 114 Emotion-processing studies further suggest dissociable patterns: The right DLPFC appears insensitive to positive stimuli in high-anxiety individuals but to negative stimuli in those with depressive symptoms. 77 More cognitively demanding paradigms may improve differentiation and reflect illness progression in comorbid anxiety and depression. 129
Differentiation from Other Disorders Utilizing fNIRS
fNIRS has also been used to distinguish MDD from autism spectrum disorder (ASD), Alzheimer’s disease, fibromyalgia syndrome (FMS), and menopausal depression. For example, right VLPFC and aTC activation patterns can differentiate ASD adolescents with and without depressive symptoms.130,172 Compared with Alzheimer’s disease, MDD shows lower cortical activation during visuospatial tasks. 167 Divergent patterns of cortical activation during VFT have also been observed between MDD and FMS. 169 Abnormal left DLPFC hemodynamics have been proposed as a marker to distinguish MDD from menopausal depression. 170
Overall, fNIRS reveals disorder-specific prefrontal and temporal activation signatures, supporting its potential as a non-invasive adjunct tool for differential diagnosis across psychiatric conditions.
Quality Assessment of the Included Studies
NOQAS was used to assess the risk of bias in the included studies, and the results are shown in Table 1. More than two-thirds of the studies had acceptable quality, receiving three or more stars (n = 137 studies). Twenty-nine studies fared worse in quality, receiving two stars, mostly due to non-reporting of case representativeness, control definition and selection, comparability issues, and ascertainment method for cases/controls. Summarization of studies for awarding the stars in the three domains of NOQAS is mentioned in Supplementary Table S6.
Discussion
This study represents one of the first published systematic reviews examining the application of fNIRS in depression, addressing four key clinical domains: its utility in distinguishing depressed individuals from HCs, its association with symptom severity, its role in monitoring treatment response across therapeutic modalities, and its capacity to differentiate depression from other psychiatric disorders. By focusing on these aspects, we aim to ascertain the applicability and utility of fNIRS as a tool in clinical practice, which can assist in diagnosis, prediction of symptomatology, monitoring treatment responses and early identification and differentiation with other psychiatric disorders.
Advances in neuroimaging techniques such as qEEG, fMRI, PET, and fNIRS have expanded efforts to identify objective biomarkers for diagnosing and predicting outcomes in depression; however, no definitive test has yet been established. Structural MRI meta-analyses show reduced gray matter volume in emotion-related regions, including the frontal cortex, OFC, cingulate cortex, hippocampus, and striatum, with evidence of pituitary enlargement in unipolar depression. 175 PET and fMRI studies further demonstrate reduced prefrontal blood flow and decreased cingulate activity during cognitive tasks. 176 Compared with these modalities, fNIRS is more portable, cost-effective, and easier to use, though it has limited spatial resolution and penetration depth, restricting assessment of subcortical regions. Its signals are also influenced by systemic physiological factors, but methodological rigor and standardized protocols can help mitigate these limitations.177,178
Approved in Japan in 2009 and later recognized in 2013 as an adjunct diagnostic tool for MDD, 5 fNIRS has emerged as a widely used, non-invasive method to measure cortical hemodynamic responses in psychiatric research. In depression research, fNIRS mostly measures task-evoked changes in oxy-Hb in frontal cortical regions and examines their relationship to clinical symptom severity using common scales such as the HAMD and BDI. Among the reviewed studies, the majority were conducted in Japan and China, with a growing number emerging from Singapore, Germany, and other countries. The VFT was the most frequently employed paradigm, given its widespread use as a bedside neuropsychological assessment of executive function and lexical retrieval, its feasibility, and its brief administration time. 179 However, performance may be influenced by linguistic and cultural factors. One of the most common symptoms of depression is cognitive and executive dysfunction, wherein processing speed, learning, memory and an individual’s ability to concentrate are impaired. 180 VFT recruits left lateral and frontopolar prefrontal regions involved in lexical retrieval, working memory, and cognitive control. Its structure yields a robust, replicable frontal oxy-Hb increase in healthy participants, which makes attenuations in patient groups easier to detect. Consequently, many of the negative severity correlations in the dataset are measured during the VFT and concentrated in left prefrontal channels, consistent with a body of literature linking left PFC dysfunction with cognitive-executive symptoms of depression. 179 However, exclusive reliance on the VFT as the primary paradigm for evaluating cognitive impairment may yield inconsistent interpretations, as depression is often characterized by generalized cognitive deficits, such as psychomotor slowing, rather than isolated executive dysfunction. 181 Other researchers have also suggested that neurophysiological methods may be more sensitive to measuring verbal fluency in patients with depression than behavioral performance, and VFT performance cannot be used as the gold standard for diagnosing depression.179,181
Across the studies, a few dominant patterns are evident. First, many studies report ‘task-evoked hypofrontality’ in depressed patients, that is, lower oxy-Hb increases in prefrontal channels during cognitive or emotional tasks compared with HCs. Second, a sizable subset of studies reports a ‘negative correlation between prefrontal oxy-Hb magnitude and depression severity’: higher clinical scores are associated with smaller oxy-Hb responses. Third, the blunted oxy-Hb response during frontal-engaging tasks increase and depressive symptoms attenuate after various forms of treatment in MDD. And fourth, there is potential utility of fNIRS in differentiating MDD from other psychiatric disorders.
Based on the findings of the current studies and given the ability to identify hemoglobin concentration changes based on light-intensity signals, fNIRS could be used as a clinical tool to evaluate MDD and eventually develop a biomarker that addresses our four pertinent questions. The prefrontal region of the human brain is rapidly evolving, and studies have demonstrated that patients with mood disorders have structural and functional abnormalities in the FPC (BA 10).5,182 Furthermore, even though the occipital and parietal regions of the brain are also implicated in depression, there were very few studies in the present review which focused on these areas.
In line with the findings of the research included, our systematic review demonstrated a persistent attenuated pattern of cerebral hemodynamic activation in individuals with depression using fNIRS while performing a cognitive task. Notwithstanding these results, a mix of other emotional states in patients with mood disorders can mask the group differences in brain activation. 26 And, different research paradigms activate different cognitive functions in the brain, resulting in different activation states of the FPC. Further, because many studies have not stated the sensitivity and specificity data that compared depressed patients with HCs, it may be difficult to clarify the validity of the finding that fNIRS can be used as a diagnostic tool. Thus, a standardization of analysis may need to be considered by future studies to have more successful comparisons.
Many studies in this review also focused on a range of clinical symptoms such as alterations in sleep patterns, suicidality, and psychomotor retardation, which can allow a further in-depth profiling of subjective depressive symptomatology and aid in identifying issues in management and treatment. However, the small sample sizes in many of the selected studies reduces its power and the utilization of varying methodologies, devices, paradigms and brain areas, further making it difficult to ascertain and combine the results of the studies. Due to the lack of long-term longitudinal studies, the potential ability of fNIRS to identify changes in severity over time was also limited, making monitoring the prognostication of the disease difficult. Long-term longitudinal studies would also solve the long-running question about whether the hemodynamic responses recorded through fNIRS are a state- or trait-dependent marker of depression.
A high number of studies were cross-sectional in nature, with scans being performed monthly or at a single time point and either did not control for the total duration of illness and number of episodes or included small samples of medication-naïve patients leading to the current evidence being conflicting for reasons such as, a high possibility of interference of antidepressant on fNIRS signals and differences in cognitive impairment in first-episode depression and recurrent depression. More frequent fNIRS measurements and larger sizes of medication or antidepressant naive patients, along with consistencies in factors such as total duration of illness, would help in providing a better understanding of changes in brain activity over time and reduce the effect of the confounding factors.
Researchers have also argued that the positive correlations between the activation of the frontal cortex and the severity of depressive symptoms, that is, the more severe the depression, the higher the hemodynamic activation of the FPC are due to conflicting factors such as, inconsistencies in inclusion criteria, wherein, patients with anxiety and other mood disorders were also included and lack of a uniform criteria for longitudinal comparisons of brain activation at different severities of depressive symptoms.24,183
Investigating similarities and differences in prefrontal abnormalities among depression, SCZ, and BD is crucial for elucidating disorder-specific pathophysiology. Longitudinal fNIRS studies may support clinical evaluation, diagnosis, treatment monitoring, and prognostication. Prior research indicates reduced PFC activation in both SCZ and MDD, with differences in affected regions and magnitude of signal reduction. 166 Spatiotemporal patterns and functional relevance of prefrontal hemodynamic responses may further distinguish these disorders. However, their relationship with functional impairment remains unclear. Large-scale studies are required to enhance clinical translation and the implementation of imaging-guided differential diagnosis.
From a clinical standpoint, wider implementation of fNIRS as a diagnostic tool for depression requires improved practical utility and stronger validation. Although preliminary findings support the development of ML, deep learning, PSR, and general linear model approaches, these frameworks remain in early stages of integration with fNIRS data. Nonetheless, integrative biomarker approaches that combine neuroimaging, neuropsychological, and genetic data may offer a more comprehensive understanding of depression’s neurobiology and improve diagnostic and prognostic precision.86,184
The findings from this review should be interpreted in the context of important limitations. First, the observational studies selected have small sample sizes (including some being single case studies), which increases the risk of confounding biases and a small effect size due to reduced power, limiting generalizability of findings. Second, only studies in English were included, and four databases were searched. It is important to recognize that many studies conducted in China and Japan may not be published and translated into English or indexed in the four databases. Thus, it is leading to potential publication bias. Third, variability in the included studies, such as data preprocessing, statistical processing, devices and channel montages, methodologies and varying clinical variables (such as medication status, comorbid anxiety, and episode history) and populations (such as age and gender) can contribute to heterogeneity. About one-third of studies failed the quality assessment.
Regardless, this review is one of the first in recent years to combine four significant questions concerning fNIRS as a potential biomarker. The past few decades have seen an increase in the availability and utilization of fNIRS, and this study serves as an update in the expansive landscape of fNIRS utility in depression. However, clinical translation requires larger, reproducible multicenter longitudinal designs, standardized task paradigms (VFT variants), harmonized montages or channel-to-region mapping, and transparent preprocessing/reporting pipelines. Future research should prioritize sample sizes that permit reliable estimation of correlation magnitudes and replication of symptom-cluster associations.
Conclusions
The fNIRS technique may have potential utility in identifying cerebral hemodynamic differences between individuals with depression and HCs. fNIRS has also been explored as a tool for differentiating MDD from other psychiatric disorders, with some evidence pointing to involvement of specific neuroanatomical regions. Interest in fNIRS as a possible diagnostic and prognostic aid in depression is growing, although its clinical role is not yet well established. Several studies report post-treatment increases in task-evoked frontal oxy-Hb levels following pharmacological interventions, psychotherapy, or neuromodulation, often parallel with symptom improvement. Additionally, some findings indicate associations between frontal oxy-Hb responses and particular symptom dimensions, such as psychomotor retardation, cognitive slowing, or suicide-related features. While these associations are not consistently replicated, they suggest that fNIRS may be sensitive to clinically relevant aspects of depression beyond overall symptom severity.
Supplemental Material
Supplemental material for this article is available online.
Supplemental Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
None.
Data Availability Statement
Not applicable. This study is a systematic review, and no new datasets were generated.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Approval
Not applicable. This study is a systematic review and did not involve human participants or animals.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Not applicable. This study is a systematic review.
Prior Presentation
The authors declare that this manuscript has not been presented previously.
Registration
The study protocol was registered with PROSPERO (registration number: CRD420250651250). Available at: https://www.crd.york.ac.uk/PROSPERO/view/CRD420250651250.
Reporting Guideline
The completed PRISMA 2020 checklist (PRISMA_2020_checklist) is provided as Supplementary Online Material.
Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71. DOI:
Simultaneous Submission
The authors confirm that this manuscript is not under consideration for publication elsewhere.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.