
Abstract
Background:
Geriatric depression is a prevalent mental health concern that impairs daily functioning, quality of life (QoL), and cognitive performance. Maladaptive metacognitive beliefs and executive dysfunction are hypothesized to contribute to depressive symptomatology in older adults.
Methods:
Participants were assessed using the Metacognitions Questionnaire-30 (MCQ-30), the Indian Council of Medical Research Neurocognitive Toolbox (verbal episodic memory, verbal fluency, and set-shifting), and World Health Organization Quality of Life–BREF (WHOQOL-BREF). Depression severity and suicidality were measured using the Geriatric Depression Scale-15 (GDS-15) and the Columbia-Suicide Severity Rating Scale (C-SSRS), respectively. Group differences were analyzed using Mann–Whitney U tests, associations using Spearman’s rho, and predictors using binary logistic regression (95% confidence interval).
Results:
Compared to controls, older adults with depression showed higher negative beliefs about uncontrollability and danger, which significantly predicted depression (OR = 1.81, p < .01), while need to control thoughts was protective (OR = 0.48, p < .01). The depression group demonstrated poorer verbal episodic memory, verbal fluency, and set-shifting (p < .05–.01). Depression severity was positively correlated with suicidality (r = 0.68) and negatively with QoL (r = −0.54; p < .001).
Conclusion:
Maladaptive metacognitive beliefs and executive dysfunction are associated with geriatric depression. Interventions integrating metacognitive therapy (MCT) with cognitive flexibility and verbal fluency training may improve emotional well-being, functional independence, and QoL in older adults.
Older adults with depression exhibit maladaptive metacognitive beliefs and executive dysfunction. Negative beliefs about uncontrollability and danger heighten depression risk. Greater perceived control over thoughts may be associated with lower depression. Cognitive and metacognitive impairments are linked to poorer quality of life (QoL), especially in psychological and social domains.Key Messages:
Geriatric depression is a common and disabling mental health condition that significantly affects functional ability, cognitive performance, and quality of life (QoL) in older adults, particularly in low- and middle-income countries where it is often underdiagnosed because of stigma and limited mental health services. 1 Depression in later life has been consistently associated with deficits in executive functioning, processing speed, and episodic memory, which may persist beyond symptomatic improvement.2,3 Normal aging is accompanied by mild cognitive decline; however, compensatory neural mechanisms usually support everyday functioning. The Scaffolding Theory of Aging and Cognition posits that neural decline is buffered by compensatory scaffolding. 4 In contrast, late-life depression is characterized by impaired cognitive flexibility, set-shifting, and memory, which compromise autonomy and daily functioning. 5 Metacognition, 6 or “thinking about thinking,” defined as beliefs and processes related to thinking about one’s own thoughts, plays an important role in emotional regulation. While metacognitive abilities may remain relatively preserved in healthy aging, depressive disorder has been associated with maladaptive metacognitive beliefs, including excessive worry about thoughts and reduced confidence in memory.7,8
Neurocognitive domains such as episodic memory, verbal fluency, and cognitive flexibility are especially vulnerable to both aging and depression. 9 The Hemispheric Encoding/Retrieval Asymmetry and Hemispheric Asymmetry Reduction in Older Adults models suggest compensatory bilateral activation during memory tasks. 10 Geriatric depression also reduces QoL, particularly in psychological and social domains.11,12
The Self-Regulatory Executive Function (S-REF) model (Wells and Matthews, 1994) provides an integrative framework linking maladaptive metacognitive beliefs, executive dysfunction, and emotion regulation. 13 The present study aims to examine metacognitive beliefs, neurocognitive functioning (verbal episodic memory, verbal fluency, and set-shifting), and QoL in older adults with depression compared with healthy controls and to identify predictors of depressive disorder.
Rationale for the Study
In low- and middle-income settings such as India, geriatric depression is underdiagnosed due to stigma, low mental health literacy, and limited geriatric services, underscoring the need to examine its cognitive and metacognitive correlates. This cross-sectional case-control study examines the underexplored interplay among metacognition, neurocognition (verbal episodic memory, verbal fluency, and set-shifting), and QoL by comparing older adults with depression with matched controls.
Hypothesis
Compared to healthy controls, older adults with depressive disorder will show significant differences in metacognitions, neurocognitive functions (verbal episodic memory, verbal fluency, and set-shifting), and QoL. Additionally, metacognitions, neurocognitive functions, and QoL will be significantly associated with depression severity, suicidality, age, and gender, while metacognitions and neurocognitive functions will significantly predict depressive disorder.
Aims
To study metacognitions, neurocognitive functions, and QoL among older adults with depressive disorder and compare them with a healthy control group.
Objectives
Primary Objectives
To assess metacognitions, neurocognitive functions, and QoL among older adults with depressive disorder.
To compare metacognitions, neurocognitive functions, and QoL among older adults with depressive disorder and a matched healthy control group.
Secondary Objectives
To assess the associations among metacognitions, neurocognitive functions, QoL, severity of depression, and suicidality among older adults with depressive disorder.
To assess associations among metacognitions, neurocognitive functions, QoL, age, and gender of older adults with depressive disorder.
To examine metacognition and neurocognitive functions as predictors of depressive disorder.
Methods
This was a tertiary care, hospital-based, cross-sectional case-control study. The data collection was conducted from June 2023 to September 2023. Participants with depressive disorder were recruited from the outpatient department of a tertiary care hospital in India. Recruitment was conducted according to predefined inclusion and exclusion criteria for both the study and healthy control groups. For the study group, eligible participants were adults aged 60 years or older with a primary diagnosis of major depressive disorder by a psychiatrist according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria. Additional inclusion criteria were: A score of ≥5 on the Geriatric Depression Scale (GDS-15), medical stability, ability to provide written informed consent, and proficiency in reading and comprehending Hindi or English. Exclusion criteria included the presence of any psychiatric disorder other than depressive disorder, a Montreal Cognitive Assessment (MoCA) score <22 (based on previous studies) indicating cognitive impairment, any debilitating medical or organic illness, or inability or unwillingness to complete the assessment. For the healthy control group, inclusion criteria required participants to be 60 years or older, able to read and comprehend Hindi or English, and willing to provide written informed consent. Exclusion criteria included a current psychiatric illness other than depression, a MoCA score <22 (per previous studies), or inability or unwillingness to complete the assessment. Healthy controls were frequency-matched with the study group on age, gender, and education level.
Ethical Considerations
Ethical approval for the present research was obtained from the hospital’s Institutional Ethics Committee. Written informed consent was obtained from all participants before inclusion. Participants identified with significant depressive symptoms or neurocognitive dysfunction during assessment were referred to the geriatric mental health department for further clinical evaluation and management. All study procedures adhered to the ethical standards of the Institutional Ethics Committee and the Declaration of Helsinki, 2013. 14
Diagnosis
Participants in the depression group met the diagnostic criteria for major depressive disorder as per the DSM-5. 15
Tools
Depressive disorder status was the primary outcome variable. Metacognitive beliefs and neurocognitive test scores were treated as exposure and predictor variables. Age, gender, education, and socio-economic status were considered potential confounders. For the healthy control group, socio-economic status was assessed using the Modified Kuppuswamy Socio-economic Scale, 16 and general cognitive functioning using the MoCA. 17 Participants scoring below 22 on the MoCA were excluded. For the study group, clinical assessments included the GDS-15 to screen for depression, 18 and the Columbia-Suicide Severity Rating Scale (C-SSRS) to evaluate suicidality. 19
Metacognition was assessed using the Metacognition Questionnaire-30 (MCQ-30), a 30-item self-report tool rated on a four-point Likert scale assessing five domains: Positive beliefs about worry, negative beliefs about uncontrollability and danger of worry, cognitive confidence, need to control thoughts, and cognitive self-consciousness. The MCQ-30 has demonstrated good internal consistency (α = 0.72–0.93) and test–retest reliability (r = 0.59–0.87). 6
Neurocognitive functioning was assessed using three subtests from the Indian Council of Medical Research Neurocognitive Toolbox: The Verbal Learning Test, the Category and Phonemic Fluency Test, and the Trail Making Test-Black and White (TMT-B and W). The Verbal Learning Test evaluates episodic memory through immediate, delayed, and recognition recall. Category and Phonemic Fluency Tests assess language and semantic retrieval. The TMT-B and W measures attention, processing speed, and mental flexibility; longer completion time indicates poorer performance. 20
QoL was assessed using World Health Organization Quality of Life-BREF (WHOQOL-BREF, WHO, 1996), which measures overall QoL and four domains: Physical health (seven items), psychological health (six items), social relationships (three items), and environmental health (eight items). Each question on the WHOQOL-BREF is graded on a five-point ordinal scale, with scores ranging from 1 to 5. The scores are then linearly translated to a scale of 0–100. 21
Bias
Potential sources of bias included selection bias from hospital-based recruitment and information bias from self-report measures. These were minimized through matching, the use of validated instruments, standardized administration procedures, and the exclusion of participants with significant cognitive impairment.
Study Size
Sample size was estimated using G* Power with a power of 80%, a level of significance of 95%, and a medium effect size. The estimated total sample size was 72 (36 per group).
Statistical Analyses
Group differences were tested with the Mann–Whitney U test (non-normal data, confirmed by the Shapiro–Wilk test) and the chi-square test. Associations were assessed using Spearman’s rho; predictors were assessed using binary logistic regression (linearity via Box–Tidwell). All statistical analyses were performed using IBM SPSS Statistics for Windows, Version 24, 2017. (IBM Corp., Armonk, NY, USA). 22 Participants with incomplete assessments were excluded from the analyses, and no data imputation was performed. Variables entered into regression models were selected a priori based on theoretical relevance and existing literature to address potential confounding. No sensitivity analyses were conducted. Cases and controls were frequency-matched on age, gender, and education, and group comparability was statistically confirmed before analysis. As the study used a hospital-based purposive sampling strategy, no sampling weights or design-based analytical adjustments were applied.
Results
Sample Characteristics
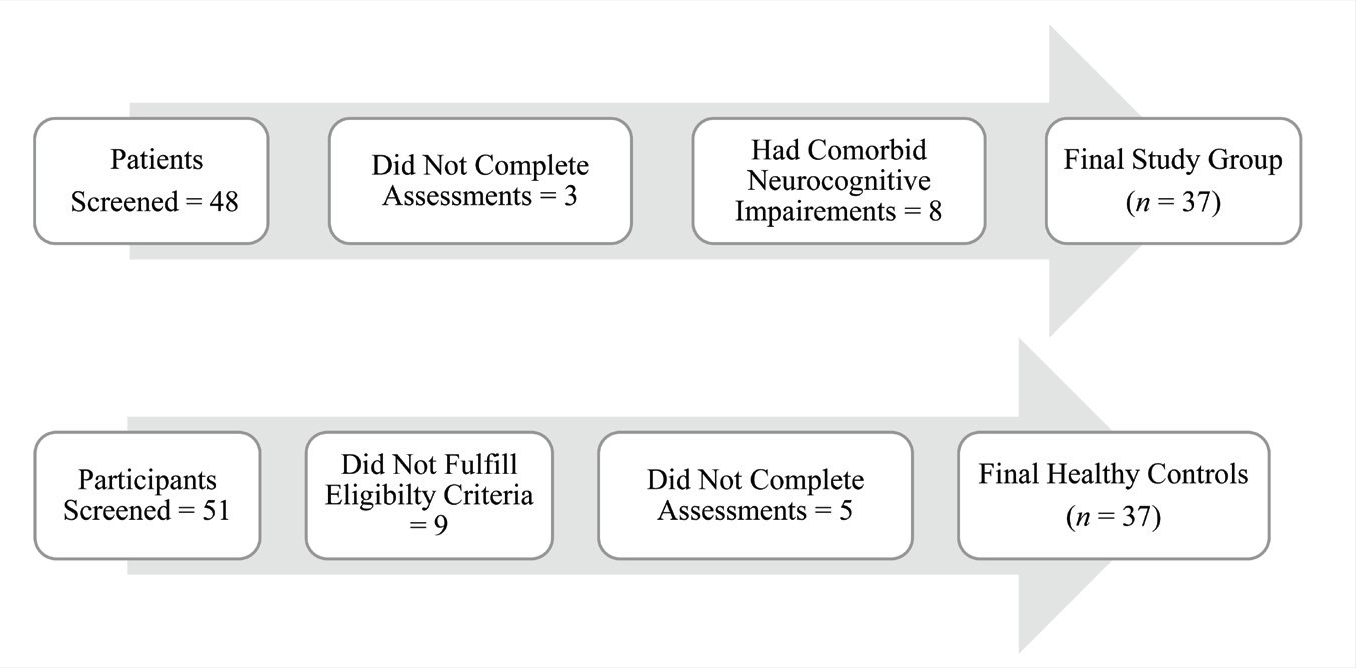
A total of 48 patients were screened for the study group, of whom 11 were excluded (eight with comorbid neurocognitive impairments and three who did not complete the assessment). In the healthy control group, 51 individuals were screened, of whom 14 were excluded (nine did not meet selection criteria, and five did not complete the assessment). The final sample comprised 37 patients with depressive disorder (mean age = 71.78, SD = 7.41) and 37 healthy controls (mean age = 70.95), yielding a total of 74 participants. No significant age difference was observed between the groups (t = −0.83, p = .63). Figure 1 presents a flow diagram detailing participant recruitment, exclusion, and final inclusion.
Sample Recruitment.
Socio-demographic Characteristics
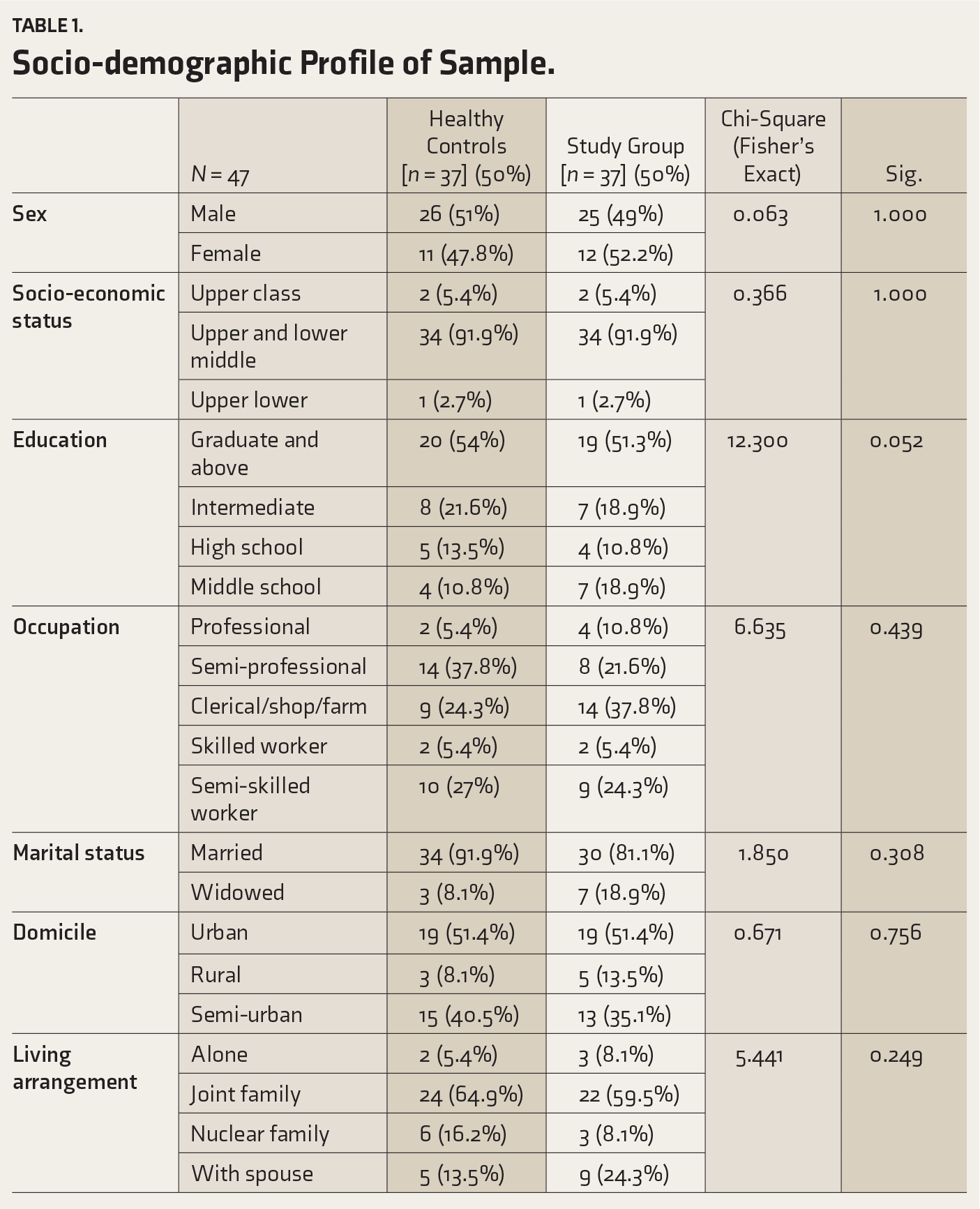
Table 1 summarizes participant characteristics. The study and control groups did not differ significantly in age. Males predominated in both groups. Most participants belonged to the upper or lower middle socio-economic classes. Educational attainment was mainly at the graduate or intermediate level. Semi-professional and semi-skilled occupations were most common, followed by professionals, and clerical, shop, and farm workers. The majority were married, with a higher proportion of widowed individuals in the study group. Most lived in urban or semi-urban areas, predominantly in joint families. Depression severity (GDS-15) ranged from mild to severe (mean = 11.59, SD = 2.10; Table 2), with most cases being first-episode geriatric onset. Suicidality scores (C-SSRS) ranged from 1 to 6 (mean = 4.21, SD = 1.53). No missing data were reported for key variables.
Socio-demographic Profile of Sample.
Episode and Severity of Depression and Suicidality.
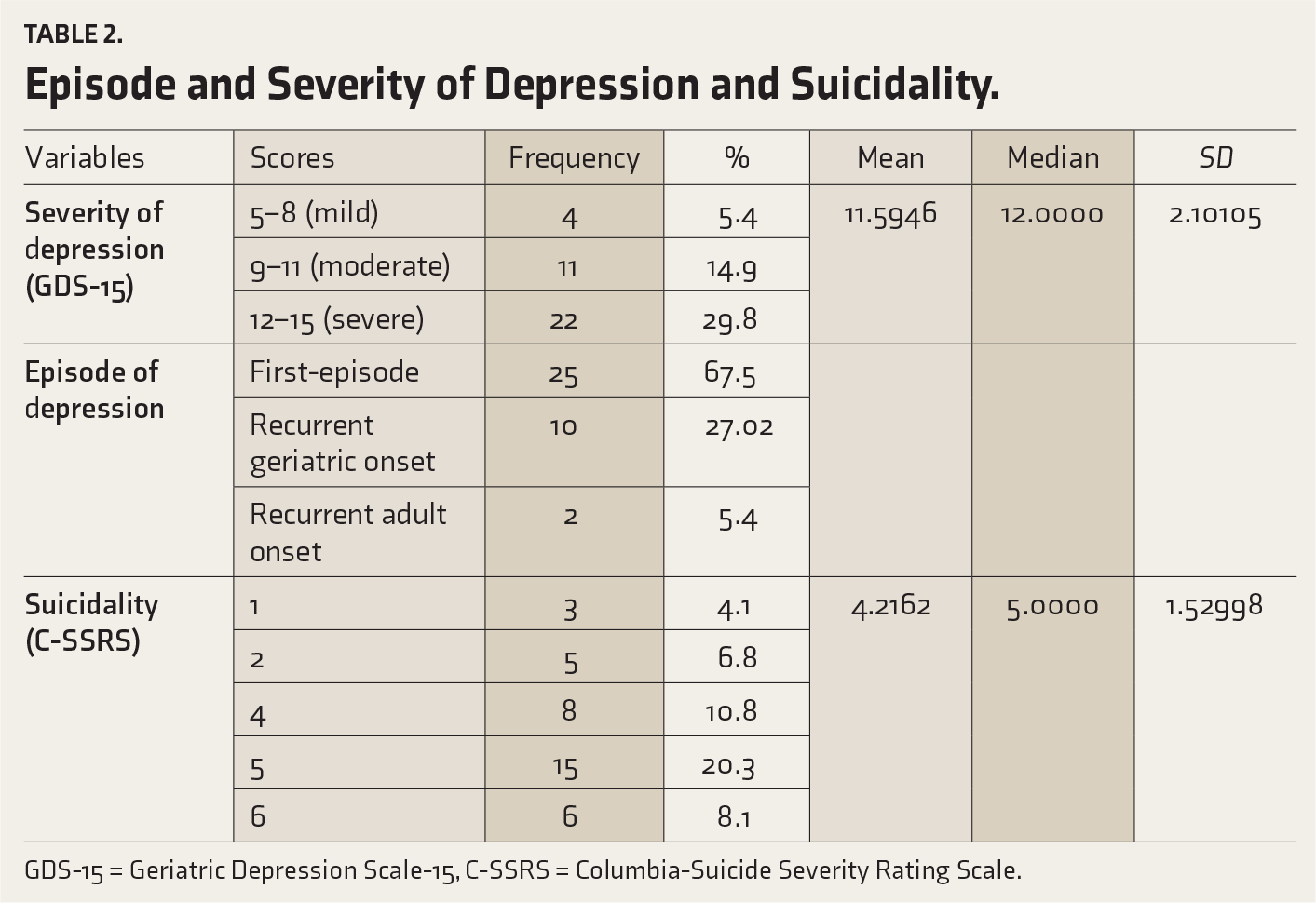
GDS-15 = Geriatric Depression Scale-15, C-SSRS = Columbia-Suicide Severity Rating Scale.
Comparison of Study and Control Groups
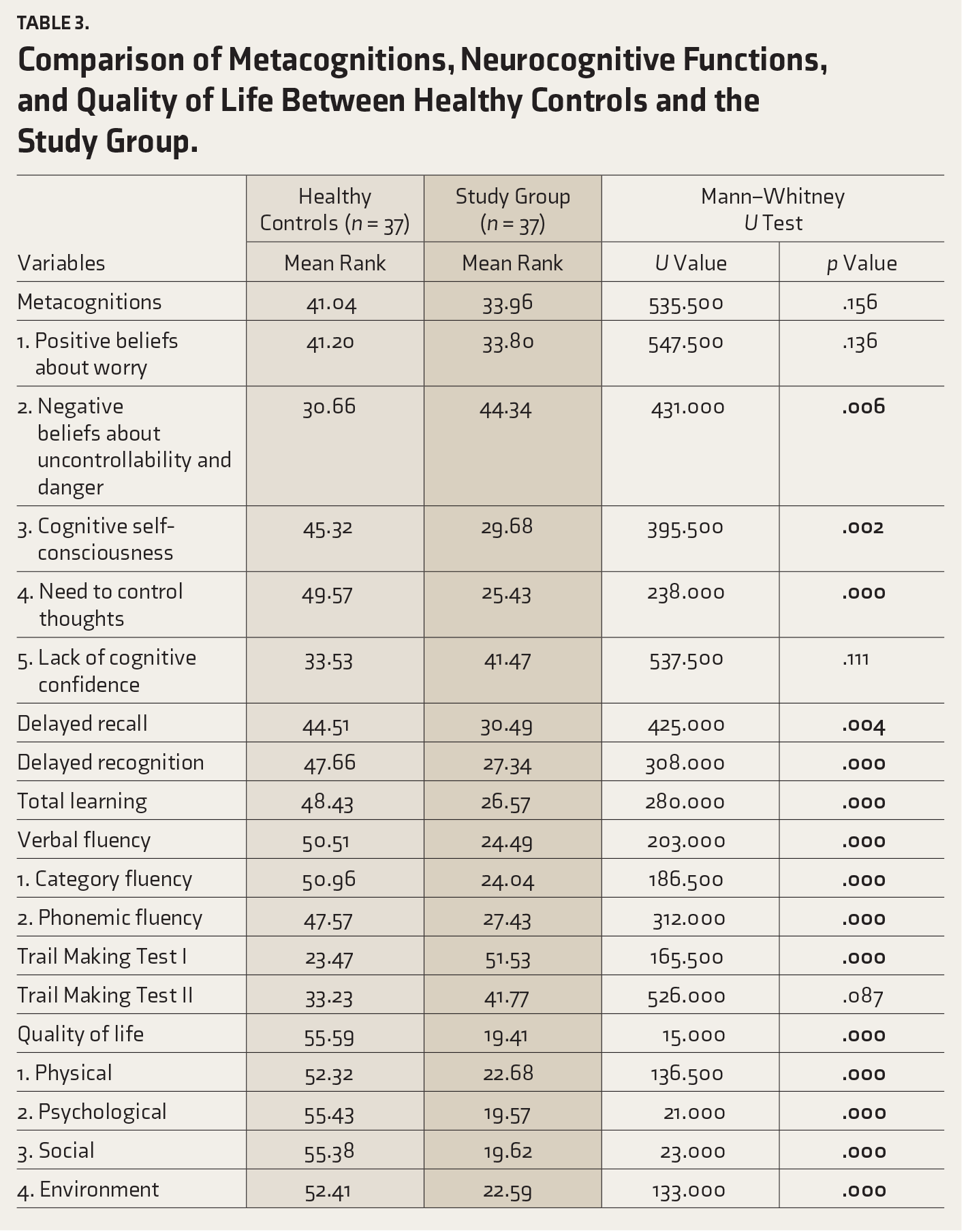
Table 3 presents the comparison of metacognition, neurocognitive functions, and QoL between the study group and healthy controls. No significant difference was observed in overall metacognition. However, significant differences emerged in subdomains: Negative beliefs about uncontrollability and danger (U = 431.00; p = .01), cognitive self-consciousness (U = 395.500; p < .01), and need to control thoughts (U = 238.00; p < .001). Significant deficits were observed in the study group compared to controls in verbal episodic memory (delayed recall [U = 425.00; p < .01], delayed recognition [U = 308.00; p < .001], total learning [U = 280.00; p < .001]), verbal fluency (verbal fluency [U = 203.00; p < .001], category fluency [U = 186.50; p < .001], phonemic fluency [U = 312.00; p < .001]), and set-shifting (TMT I [U = 165.50; p < .001]), whereas no significant difference was found in TMT II. QoL was significantly lower in the study group across total score (U = 15.00; p < .001) and all subdomains: Physical (U = 136.50; p < .001), psychological (U = 21.00; p < .001), social (U = 23.00; p < .000), and environment (U = 133.00; p < .001). The study group demonstrated significantly poorer performance across several cognitive and QoL domains compared to healthy controls.
Comparison of Metacognitions, Neurocognitive Functions, and Quality of Life Between Healthy Controls and the Study Group.
Correlational Analyses
Correlation among variables was assessed using Spearman’s rho. It examined the relationships among clinical variables (age, depression, suicidality), metacognitions, neurocognitive functions, and QoL. Key findings include: Depression severity was strongly associated with suicidality (r = 0.70, p < .001), negatively correlated with QoL (r = −0.31, p < .001), and inversely associated with delayed verbal episodic memory recall (r = −0.25, p < .001). Suicidality showed moderate negative correlation with verbal episodic memory recognition (r = −0.29, p < .001), and weak negative associations with metacognition (r = −0.23, p < .001) and QoL (r = −0.29, p < .001). Total MCQ-30 scores were strongly correlated with all subdomains: Positive beliefs about worry (r = 0.69), negative beliefs about uncontrollability and danger (r = 0.55), cognitive self-consciousness (r = 0.59), need to control thoughts (r = 0.63), and lack of cognitive confidence (r = 0.60; all p < .001). Metacognition was weakly positively associated with verbal fluency (r = 0.22, p < .001). Regarding neurocognitive functioning, delayed recall of verbal episodic memory was moderately positively correlated with verbal fluency (r = 0.45) and QoL (r = 0.27), but negatively with set-shifting TMT I (r = −0.39, p < .001). Delayed recognition showed similar associations: verbal fluency (r = 0.33), QoL (r = 0.35), and TMT I (r = −0.33; all p < .001). Delayed recall and recognition were strongly correlated (r = 0.56, p < .001). Verbal fluency correlated strongly negatively with TMT I (r = −0.67, p < .001) and moderately with TMT II (r = −0.20, p < .001), while showing strong positive correlations with all QoL domains (physical r = 0.52, psychological r = 0.53, social r = 0.59, environmental r = 0.55; all p < .001).
Among the metacognitive domains and QoL/neurocognition, positive beliefs about worry were positively associated with other metacognitive domains (r = 0.18–.47, p < .001), verbal fluency (r = 0.24, p < .001), and negatively with TMT I (r = −0.67, p < .001). Negative beliefs about uncontrollability and danger were negatively associated with set-shifting (r = −0.09) and QoL domains (r = −0.37 to −0.41), and positively with lack of cognitive confidence (r = 0.28; all p < .001). Cognitive self-consciousness correlated positively with verbal fluency (r = 0.30), delayed recall (r = 0.28), and moderately with all QoL domains (r = 0.33–0.44; p < .001). Need to control thoughts was positively associated with verbal fluency (r = 0.43) and delayed recognition (r = 0.35) and was moderately associated with all QoL domains (r = 0.37–0.43; p < .001). Lack of cognitive confidence was negatively associated with physical (r = −0.27), psychological (r = −0.29), and social QoL (r = −0.24; p < .001). Depression was negatively associated with positive beliefs about worry (r = −0.24), cognitive self-consciousness (r = −0.25), and psychological QoL (r = −0.43; p < .001). Suicidality was moderately negatively correlated with phonemic (r = −0.35) and verbal fluency (r = −0.38), and environmental QoL (r = −0.38; p < .001).
The QoL domains were highly interrelated, showing strong positive correlations with verbal fluency and moderate positive associations with delayed recall and recognition. Set-shifting performance was negatively associated with all QoL domains, particularly the physical, psychological, and social domains. In addition, depression severity (GDS-15) was positively correlated with suicidality (r = 0.78, p < .001) and negatively correlated with QoL (r = −0.54, p < .01). Verbal fluency correlated positively with QoL (r = 0.62, p < .001). A Bonferroni correction (α = 0.002) was applied to adjust for multiple comparisons, and variables were selected a priori based on theoretical relevance and prior research.
Regression Analyses
A binary logistic regression was conducted to examine whether specific metacognitive beliefs and neurocognitive functions predicted the likelihood of depressive disorder. Variables included were negative beliefs about worry, need to control thoughts, cognitive self-consciousness, verbal episodic memory (delayed recall and recognition), and set-shifting (TMT I). Verbal fluency and QoL were excluded due to multicollinearity. Table 4 presents the binary logistic regression results examining how specific metacognitive beliefs and neurocognitive functions predict the likelihood of depressive disorder. Significant predictors of depressive disorder included: Negative beliefs about uncontrollability and danger: Exp(B) = 1.81, p < .01; a one-unit increase was associated with an 80.6% higher likelihood of depression; need to control thoughts: Exp(B) = 0.48, p < .01; a one-unit increase reduced depression odds by 52%, suggesting a protective effect; verbal episodic memory (delayed recognition): Exp(B) = 0.00, p = .03; better memory recognition was associated with lower depression risk; set-shifting (TMT I): Exp(B) = 1.16, p = .01; slower performance increased depression odds by 15.6%. Cognitive self-consciousness approached significance (Exp(B) = 0.79, p = .06), while delayed recall was not significant (Exp(B) = 783,134.92, p = .09).
Predictor Analysis.
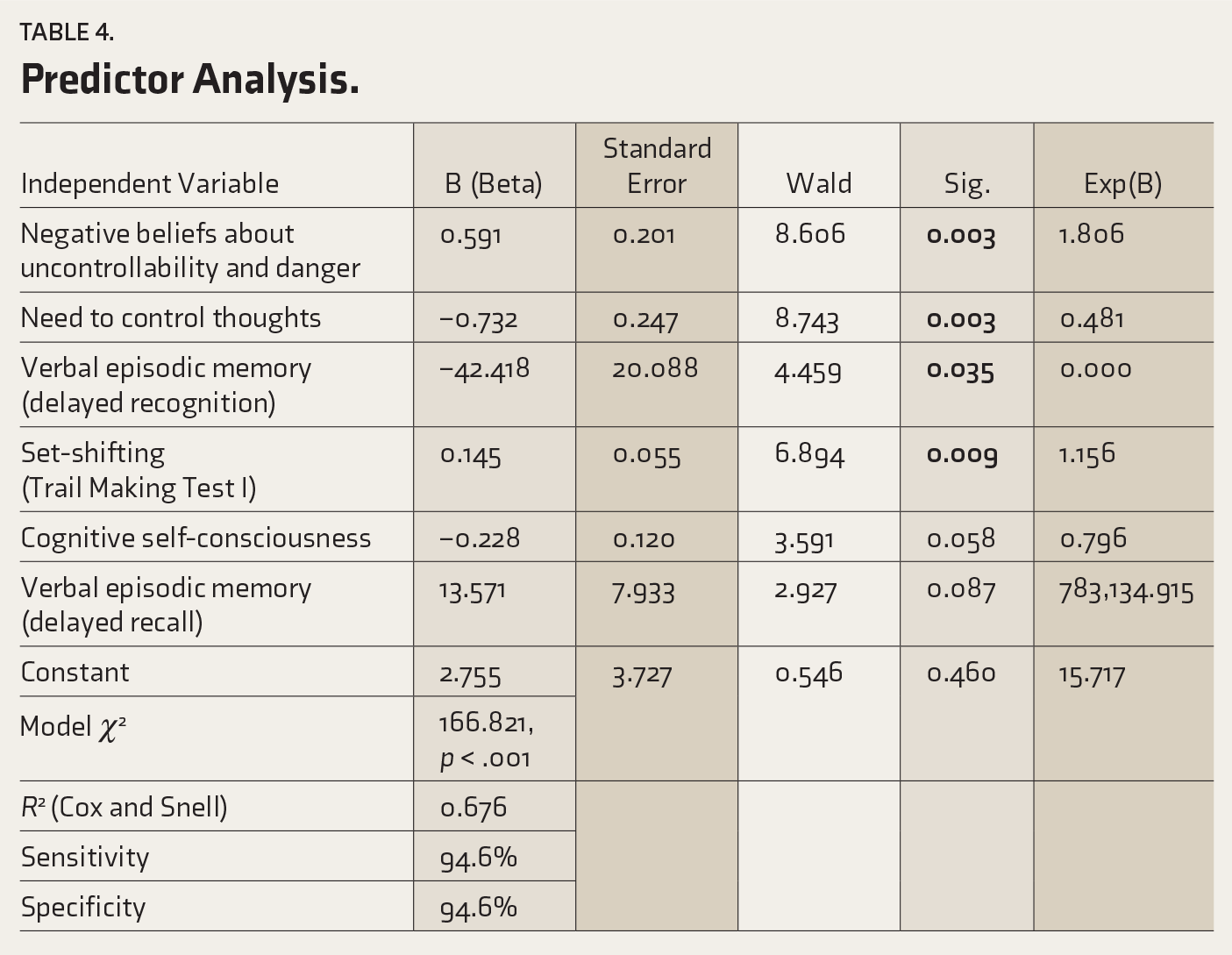
The overall model was significant (χ² = 166.82, p < .001), explaining 67.6% of variance (Cox and Snell R² = 0.6), with high classification accuracy (sensitivity and specificity = 94.6%). These results highlight that maladaptive metacognitive beliefs and executive function deficits, particularly negative beliefs about worry and impaired set-shifting, increase depression risk, whereas adaptive metacognitive regulation appears protective.
Discussion
This study highlights the link between geriatric depression, metacognition, neurocognitive functioning, and QoL. Compared to healthy controls, older adults with depressive disorder exhibited more negative beliefs about uncontrollability and danger, reduced cognitive self-consciousness, and a lower need to control thoughts, reflecting maladaptive metacognitive patterns. 23 They also demonstrated significant deficits in verbal episodic memory, verbal fluency, and set-shifting—cognitive profiles often observed in mild cognitive impairment and early neurodegenerative disorders—which may contribute to impaired daily functioning.2,3,24 These findings underscore the importance of interventions targeting executive dysfunction, such as cognitive flexibility and task-switching training,25,26 and support the use of metacognitive therapy (MCT) to address maladaptive beliefs. 27 Combining MCT with cognitive training may enhance both emotional and functional outcomes in geriatric populations. 28
Significant associations were observed among metacognition, neurocognitive functions, and QoL within the depressed group. Depression severity showed a strong positive association with suicidality, while suicidality was negatively correlated with delayed recognition and metacognition, suggesting that impaired cognitive processing may accompany elevated suicide risk. Metacognitive beliefs—including positive and negative beliefs about worry, cognitive self-consciousness, and the need to control thoughts—were strongly interrelated and correlated with verbal episodic memory, particularly delayed recall, indicating their influence on memory performance in depression. Delayed recall and recognition were strongly correlated, suggesting consistent memory deficits across tasks, though they were not directly related to depression severity or suicidality.
Verbal fluency demonstrated moderate positive correlations with QoL but was negatively associated with set-shifting, suggesting a possible trade-off between fluency and cognitive flexibility. Set-shifting also negatively correlated with QoL domains, whereas cognitive self-consciousness and need to control thoughts were positively associated with all domains. In contrast, negative beliefs about uncontrollability and danger were inversely related to QoL, particularly in psychological and social dimensions, indicating that maladaptive metacognitive patterns contribute to reduced well-being. These findings may reflect underlying neurobiological mechanisms, such as prefrontal–limbic dysregulation, hippocampal atrophy, and Hypothalamic–Pituitary–Adrenal (HPA) axis dysfunction, which collectively affect memory, executive control, and emotional regulation. Psychosocially, reduced verbal fluency and cognitive rigidity may hinder social adaptability, while maladaptive metacognitive beliefs perpetuate rumination and limit recovery—consistent with the S-REF model.
Binary logistic regression identified key predictors of depressive disorder in older adults, with the model explaining 67.6% of the variance (R² = 0.68) and showing high sensitivity and specificity (94.6%). 29 Findings align with the S-REF model, 30 which posits that maladaptive metacognitive beliefs and executive dysfunction interact to sustain depression. Negative beliefs about the uncontrollability and danger of thoughts markedly increased depression risk by activating the Cognitive Attentional Syndrome of worry, rumination, and unhelpful coping. Conversely, a higher need to control thoughts appeared protective, suggesting adaptive regulation of intrusive cognitions. Cognitive self-consciousness approached significance but was not a strong predictor. Among neurocognitive variables, impaired set-shifting (cognitive flexibility) heightened depression risk, indicating the role of cognitive rigidity. At the same time, reduced delayed recognition suggested that episodic memory deficits may also influence mood regulation. Overall, these results emphasize the potential benefit of integrating MCT with cognitive flexibility and memory-enhancement strategies to improve emotional, cognitive, and functional outcomes in late-life depression. These results suggest that combining MCT, which targets maladaptive beliefs and promotes flexible cognitive regulation, with cognitive flexibility and memory-focused interventions may improve emotional and functional outcomes in older adults. 27
Strengths
This is among the few published studies to simultaneously examine metacognitive beliefs, neurocognitive functioning, and QoL in older adults with depressive disorder. The inclusion of an age-, gender-, and education-matched healthy control group enhances the internal validity of group comparisons. The use of standardized, validated assessment tools ensures robust, comparable measurement across domains, while integrating cognitive, metacognitive, and psychosocial perspectives provides a comprehensive understanding of geriatric depression.
Limitations
The cross-sectional design precludes causal inference regarding the relationships among metacognition, cognitive functioning, and depression. The relatively small sample size may limit the generalizability of findings to wider older adult populations. The absence of neuroimaging or biomarker data restricts the interpretation of underlying neural mechanisms. Potential confounding effects of medication use, and comorbid medical conditions were not fully controlled, and reliance on self-report measures for metacognition and QoL may introduce response bias related to insight or reporting accuracy. Because this research was conducted in an urban area among treatment-seeking older adults attending tertiary care settings, it may not be generalizable to community-dwelling or rural older populations.
Clinical Implications
These findings highlight the importance of integrated interventions that target both maladaptive metacognitive beliefs and cognitive control deficits in older adults with depression. MCT can directly address negative beliefs about worry, uncontrollability, and danger, core features observed in this study.26,27 Incorporating MCT strategies, such as detached mindfulness and attention training techniques, may reduce executive burden associated with perseverative thinking while promoting cognitive flexibility. Cognitive flexibility training may help older adults overcome set-shifting deficits and reduce depressive symptoms. Executive function training and cognitive remediation programs have been shown to improve adaptive coping, problem-solving, and daily functioning in geriatric populations.25,26 Verbal fluency interventions, including semantic category retrieval exercises, may enhance language skills, cognitive engagement, and social participation, thereby improving QoL. 31 Future research should evaluate the efficacy of combining MCT with cognitive flexibility and executive function training in late-life depression, particularly in community-based or resource-limited settings, to develop scalable interventions. 29
Conclusion
This study demonstrates that geriatric depression is closely associated with maladaptive metacognitive beliefs, executive dysfunction, and reduced QoL. Older adults with depression exhibited firmer negative beliefs about the uncontrollability and danger of thoughts, lower cognitive self-consciousness, and reduced need to control thoughts, alongside deficits in verbal episodic memory, verbal fluency, and set-shifting, reflecting impaired cognitive flexibility. These impairments were linked to higher depression severity, suicidality, and lower QoL across physical, psychological, social, and environmental domains, highlighting the functional impact of both cognitive and metacognitive dysfunction. Binary logistic regression identified negative beliefs about uncontrollability and danger, reduced set-shifting, and poorer delayed recognition as significant predictors of depression. At the same time, a higher need to control thoughts appeared protective, supporting the S-REF model. These findings underscore that both maladaptive metacognitive processes and executive dysfunction contribute to late-life depression and its associated functional decline. Clinically, the results emphasize the importance of integrated interventions targeting both metacognitive and cognitive domains. MCT can modify maladaptive beliefs and reduce perseverative thinking, while cognitive flexibility and verbal fluency training can enhance executive control, adaptive coping, and social participation. Future research should explore the combined efficacy of MCT with cognitive remediation in community and resource-limited settings to optimize emotional and functional outcomes in older adults. This study provides evidence of significant associations between maladaptive metacognitive beliefs, executive dysfunction, and geriatric depression.
Supplementary Material
Supplemental material for this article is available online.
Footnotes
Acknowledgements
The authors gratefully acknowledge the participants for their time and cooperation. We also thank the staff and faculty members at the Department of Geriatric Mental Health, King George’s Medical University, Lucknow, for their support during data collection.
Appropriate Permissions from the Concerned Authorities
Prior permission was obtained from the institutional and administrative authorities of King George’s Medical University, Lucknow, UP, before data collection. Ethical approval was granted by the Institutional Ethics Committee (Approval No. XVIII-PGTSC-II B M.Phil./PI). Written informed consent was obtained from all participants.
Data Sharing Statements
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
No part of this article was written or generated by a generative AI tool. The authors take full responsibility for the accuracy, integrity, and originality of the published article.
Ethics Committee Details
Name of the Institutional Ethics Committee/Independent Review Board: Institutional Ethics Committee, King George’s Medical University, Lucknow, Uttar Pradesh, India. Approval Reference No.: XVIII-PGTSC-II B M.Phil./PI. Date: 26 June 2023.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Informed Consent/Assent
Informed consent was obtained from all the participants included in the study in writing. Participants were provided informed written consent before inclusion in the study. The consent form detailed the study’s purpose, procedures, and participants’ roles, and included information on potential risks and benefits, possible complications, confidentiality, rights of participants, compensation, and alternatives to participation.
Patient Consent
Written informed consent was obtained from all the participants included in the study. The consent form detailed the study’s purpose, procedures, and participants’ roles, and included information on potential risks and benefits, possible complications,confidentiality, rights of participants, compensation and alternatives to participation.
Prior Presentations
Not applicable.
PROSPERO/CTRI Details
Not applicable.
Registration
Since the current study is not interventional. It was not registered.
Trial registry name: Not applicable. URL: Not applicable. Registration number: Not applicable.
Simultaneous Submission to Another Journal or Resource
Not applicable.
Status of Your Study (for Study Protocol)
Not applicable.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.