
Abstract
Background:
Executive function (EF) and emotion regulation (ER) deficits are prevalent in depressive and anxiety disorders, suggesting a transdiagnostic role. Given their role in treatment engagement, symptom reduction, and relapse prevention, we examine EF and ER interrelationships in these disorders.
Methods:
Participants (n = 27 depressive/anxiety disorders, n = 27 nonclinical group) underwent psychiatric screening and assessments of symptom severity, EF (set-shifting, response inhibition [RI], working memory [WM], verbal fluency, planning), and ER (severity, strategies, situational ER following emotion induction). Mann–Whitney U-test/t-test was used for group comparisons, and Pearson’s/Spearman’s test was used for correlations.
Results:
The clinical group showed lower WM (Cohen’s d = 0.94, p = .001), verbal fluency (Cohen’s d = 0.7, p = .01), and RI (Cohen’s d = 0.35, p = .02); greater ER difficulties (Cohen’s d = −1.40, p < .001), greater negative ER strategy use of catastrophizing (Cohen’s d = 0.55, p < .001); and on the emotion-induction task—higher use of acceptance, other-blame, but no positive reappraisal. The nonclinical group showed greater positive ER strategy use of refocus on plan (Cohen’s d = 0.53, p < .001) and no use of rumination on the emotion-induction task. The severity of ER difficulties correlated with poorer WM (p = .006); acceptance as an ER strategy correlated with poorer RI (p = .02). EF and ER difficulties and maladaptive strategies were significantly higher in the depression/anxiety group.
Conclusions:
The findings extend prior research by providing actionable insights for tailored interventions and merit testing in larger samples. With poorer WM linked to greater ER difficulties and inefficient RI to passive acceptance, interventions such as cognitive training may enhance ER.
Difficulties in emotion regulation correlate with poorer executive functions. Individuals with depression and anxiety demonstrate difficulties in executive functions and emotion regulation. Emotion-induction tasks may help assess state-based emotion regulation difficulties. The findings indicate a potential role for cognitive training to enhance EF and ER.Key Messages:
Depressive and anxiety disorders, collectively known as common mental disorders (CMDs) according to the World Health Organization, are highly prevalent across age groups, genders, and cultures. They are associated with 50%–70% disability. 1 While distinct, depression and anxiety often co-occur, with comorbidity rates of up to 80% and overlapping risk factors and mechanisms. 2 This comorbidity intensifies symptom severity, prolongs illness, and complicates treatment, necessitating integrated approaches. 3 Thus, a transdiagnostic approach to conceptualization and management has been proposed, with executive functions (EFs) and emotion regulation (ER) implicated in development, maintenance, and treatment.2,4 Banich 5 describes EF as a set of abilities required to effortfully guide behavior toward a goal, especially in nonroutine situations. EF deficits have been identified by the Research Domain Criteria 4 as a contributing factor to pathophysiology in CMDs, possibly through shared underlying mechanisms. Both depressive and anxiety disorders exhibit deficits in working memory (WM), response inhibition (RI), cognitive flexibility, and verbal fluency. 6 ER involves using strategies to alter emotions’ intensity, duration, and quality. 7 Individuals with both depression and anxiety exhibit reduced emotional clarity, heightened emotional reactivity, and use of maladaptive strategies, 8 which amplify unpleasant emotions. 9 Conversely, adaptive strategies like positive reappraisal (PRA) have been found to reduce depressive symptoms. 9 EF and ER are closely linked, as EF, like WM, are essential for effective ER; meanwhile, ER difficulties may further strain cognitive resources. It is suggested that EF and ER may involve shared processes like tracking and reducing discrepancies between current and goal states, 10 as well as shared brain circuits like the prefrontal cortex and cingulate cortices. 11 EF, specifically verbal fluency and WM, may predict ER abilities. Studies suggest that deficits in WM may hinder the ability to use adaptive ER strategies like PRA, 12 leading to reliance on maladaptive strategies such as rumination. This highlights the interplay between EF and ER (specifically WM and PRA). 6 The transdiagnostic role of these deficits is increasingly recognized as they influence emotional processing and perpetuate symptoms across diagnoses. EF deficits may impair cognitive functions needed for adaptive emotional responses, while maladaptive ER strategies may exacerbate cognitive dysfunction, creating a vicious cycle that underlies CMDs across diagnostic boundaries. This highlights possible overlapping pathways in CMDs, underscoring EF and ER as key therapeutic targets that may reduce the comorbidity burden.6,13 While ER is usually assessed through self-report 14 of trait ER, the dynamic nature of state-based ER may not be fully captured. Mood-induction tasks (e.g., viewing emotional pictures, videos, words, or statements) are designed to evoke particular emotional states in the participant. This provides a more accurate, proximal, state-based measure of participants’ reactions to emotion in real-time (e.g., what they felt, intensity ratings, and ER strategies) compared to a more distal, retrospective self-report. Among mood-induction procedures, interactive or situational procedures (e.g., participating in a game or situation designed to evoke emotion) are considered more effective than passive viewing of visual stimuli. 14 Utilizing such procedures allows for a nuanced understanding of how individuals regulate emotions in response to dynamic and socially meaningful stressors, thereby addressing limitations of more passive approaches or self-report measures prone to biases such as social desirability.
Given the significant impact of CMDs on everyday functioning and quality of life, there is a critical need to explore how EF and ER interact specifically in clinical populations. The existing literature is dominated by nonclinical studies and reviews, with few empirical studies on clinical samples. Additionally, most research focuses on trait measures rather than the dynamic processes of ER, leaving a gap in understanding the real-time ER strategies employed by those with CMDs. Thus, exploring EF and ER at both trait and state levels—in clinical and nonclinical populations—and the potential link between them can inform our understanding of risk factors, protective factors, and potential intervention targets. A possible interplay between EF and ER (WM and PRA) could have significant implications for clinical interventions. Cognitive training enhancing EF might improve adaptive ER strategies like PRA, leading to better emotional outcomes and potentially more effective treatments for CMDs. 13 Such interventions may improve quality of life and foster relapse prevention and maintenance of gains over time.8,13 To this end, this study aims to compare EF and ER performance between clinical (depression and anxiety disorder) and nonclinical groups and explore their associations. ER will be assessed via self-report as a trait measure and through a state-based mood-induction task.
We hypothesized that (a) EF and ER performance will be poorer in the clinical group compared to the nonclinical group, and (b) a significant association will exist between EF (specifically WM) and ER (specifically PRA).
Methods
This cross-sectional study was conducted following the Strengthening the Reporting of Observational Studies in Epidemiology checklist, which has been uploaded as Supplementary Material. 15 Ethical approval was obtained from the Institutional Ethics Committee, and informed consent was obtained from all participants. Given the mood-induction task, the informed consent form asked participants to report any subsequent distress. Any emergent psychological difficulty was addressed in-session using psychological first aid and grounding techniques by the first author, a clinical psychologist in training. If distress persisted after consultation with the second or third authors (clinicians with over 15 years of experience), further referrals were made to the institute’s multidisciplinary treatment team or emergency services. After the task, participants were debriefed to address any unpleasant emotions and lingering effects.
Participants
The sample consisted of two groups: clinical and nonclinical. The clinical group comprised consecutive participants with an International Classification of Diseases, Tenth Revision 16 diagnosis of depressive or anxiety disorders (F32, F33, F34.1, F40, and/or F41) from in-patient and outpatient services. The inclusion criteria required individuals between the ages of 18 and 50, with a minimum of 7 years of education, and normal vision and hearing to ensure the validity of cognitive assessments. Participants were required to be right-handed, as per the Edinburgh Handedness Inventory, to control for variability in lateralization, 17 particularly in areas crucial for EF and ER, such as the prefrontal cortex. 18 Fluency in English, Hindi, or Kannada was mandatory, as the assessments were conducted in these languages to ensure accurate comprehension of instructions. Exclusion criteria comprised comorbid schizophrenia, bipolar affective disorder, neurological conditions, substance dependence, intellectual or specific learning disabilities, developmental disorders, or sensorimotor impairments. Participants with an active suicide risk were also excluded. The severity of depressive and anxiety symptoms (Hamilton Anxiety Rating Scale [HAM-A] and the Montgomery–Asberg Depression Rating Scale [MADRS]) was assessed objectively after participant selection and included in analyses.
The nonclinical group comprised community participants screened for psychiatric disorders using the Diagnostic Interview for Anxiety, Mood, and Obsessive-Compulsive and Related Neuropsychiatric Disorders (DIAMOND) self-report screener. This screener includes trauma- and stressor-related disorders, somatic symptom and related disorders, feeding and eating disorders, neurodevelopmental disorders, schizophrenia spectrum and other psychotic disorders, in addition to anxiety, mood, obsessive-compulsive, and related disorders. This group was frequency-matched with the clinical group for age, gender, and education (±2 years).
Sample Size Estimation
A sample size of 49 per group was calculated, expecting a minimal significant difference in WM total score of 5 between the clinical and nonclinical groups, with a standard deviation of 8, 19 for 80% power and a 5% significance level after Bonferroni correction. The study’s objective was to compare WM and PRA between both groups; therefore, the above sample size was computed to control the family-wise error rate using the Bonferroni method. However, due to the limited availability of eligible participants within the recruitment period (mainly due to other comorbidities in a hospital setting) and lengthy assessments, which were not feasible for many participants, the study was able to recruit 27 participants per group (Figure 1).
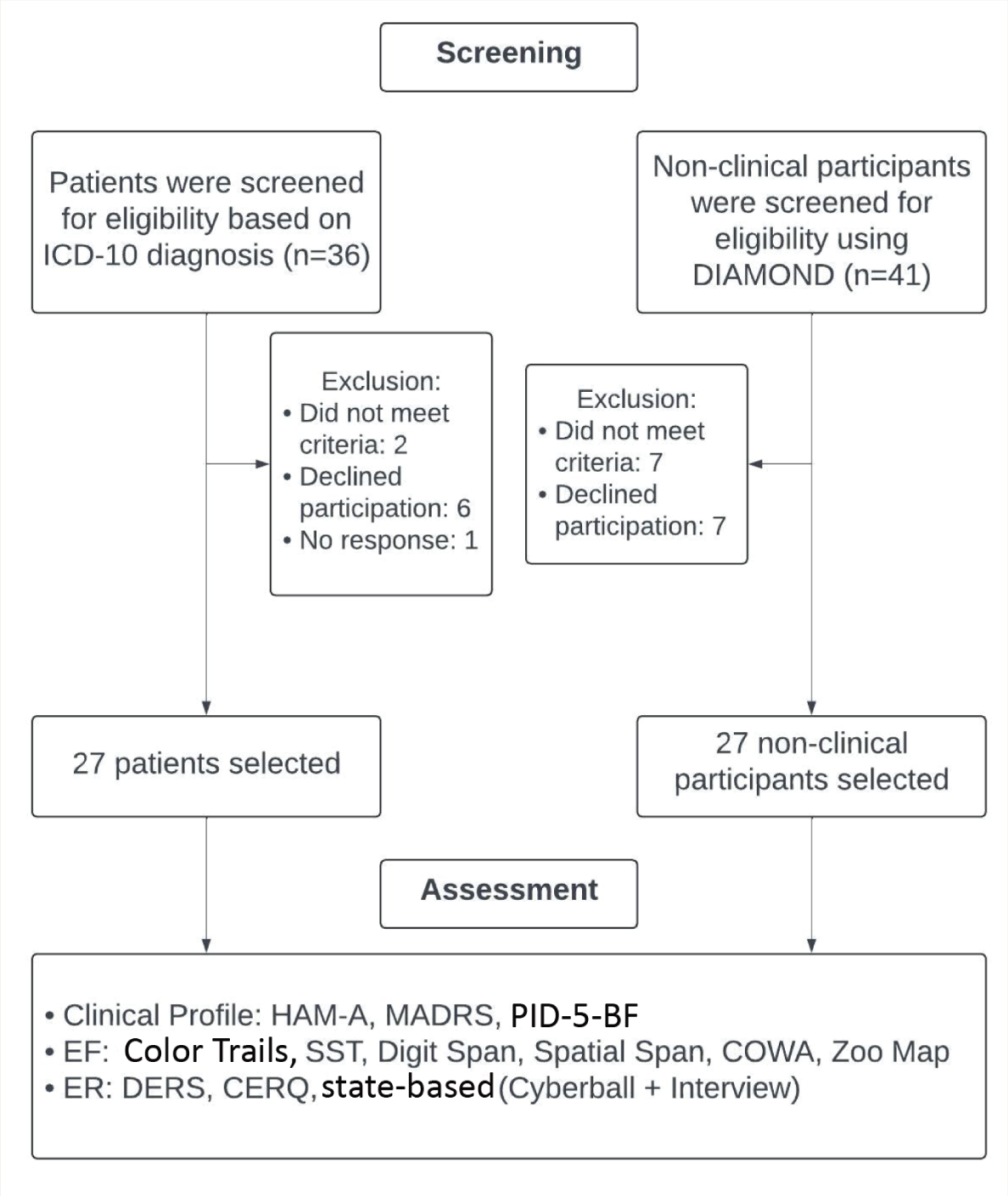
CERQ: Cognitive Emotion Regulation Questionnaire; COWA: Controlled Oral Word Association; DERS: Difficulties in Emotion Regulation Scale; DIAMOND: Diagnostic Interview for Anxiety, Mood, and Obsessive-Compulsive and Related Neuropsychiatric Disorders; HAM-A: Hamilton Anxiety Rating Scale; MADRS: Montgomery–Asberg Depression Rating Scale; PID-5-BF: Personality Inventory for Diagnostic and Statistical Manual for Mental Disorders-5-Brief Form; SST: Stop Signal Task.
Screening and Clinical Assessments
All participants were administered a sociodemographic data sheet and the Edinburgh Handedness Inventory-Short Form. DIAMOND was used to screen nonclinical participants. HAM-A and MADRS were administered as clinician-rated tools to measure symptom severity. The Personality Inventory for Diagnostic and Statistical Manual for Mental Disorders5-Brief Form—Adult (PID-5-BF) was administered as a self-rated tool to all participants.
Assessment of EFs (Clinician-Administered)
Cognitive Flexibility
Color Trails (CTs) is a culture-fair test of visual scanning and cognitive flexibility. It requires switching attention and adapting to new information. The score represents the time taken (in seconds) to complete the trials, with longer times indicating greater difficulties with cognitive flexibility (reliability r = 0.79–0.89). 20
RI
A computerized Stop Signal Task (SST) was used for motor RI to assess self-regulation and impulse control challenges. The score is the reaction time, which reflects the time taken to inhibit a response, as well as omission and commission errors. Higher reaction time and higher errors indicate poorer inhibitory control (reliability r = 0.60–0.80 in clinical populations). 21
WM
The Digit Span (DS) test was used for verbal WM through forward and backward conditions, and the Spatial Span (SS) test was used for visual WM. Verbal and visuospatial WM are key components of EF associated with higher-order cognitive processes. The score is the number of correctly recalled digits (Forward and Backward) and spatial sequences accurately reproduced. Higher scores indicate better verbal and visual WM, respectively (DS: reliability r = 0.83; SS: r = 0.62). 22
Verbal Fluency
The Controlled Oral Word Association test was used for phonemic fluency, with an Indian vernacular adaptation to ensure relevance and accuracy across linguistic variations in the study population. The score is the average number of words generated per minute for three letters (reliability r = 0.70–0.80). 23
Planning
The Zoo Map Test (ZMT) was used for its focus on planning, problem-solving, and error monitoring. The score is the total time (in seconds) taken to complete the test, with faster completion times reflecting better planning and problem-solving abilities (reliability r = 0.94). 24
Assessment of ER
ER
The Difficulties in Emotion Regulation Scale (DERS) was used to evaluate trait-based difficulties in ER through a 36-item self-report scale. The score is the sum of responses across six subscales, with higher scores indicating greater difficulties in ER. 25
ER Strategies
The Cognitive Emotion Regulation Questionnaire (CERQ) was used to gain detailed insights into participants’ regulatory patterns. It measures the use of adaptive and maladaptive ER strategies across nine domains through a 36-item self-report. The scores reflect the frequency of adaptive and maladaptive ER strategies, with higher subscale scores indicating greater use of a specific strategy (Cronbach’s α: 0.7 for CMD-related samples). 26
Emotion-induction Task
A virtual game of Cyberball 27 was used. Participants engaged in a virtual ball-tossing game with pre-programmed players and were “excluded” after only one toss. Cyberball has been widely and successfully used to simulate social exclusion, which is a potent trigger for inducing emotional states requiring regulation. 28 While participants were not explicitly informed about this potential distress, as it could influence their response to the task, they were informed they could request to stop at any point if they felt too distressed and that support would be provided. Participants were also debriefed after the task, and any lingering effects were addressed (Cronbach’s α: 0.88). 28
State-based ER
A self-rated Visual Analog Scale (VAS) was used to assess distress levels following the emotion-induction task for further analysis to explore associations between induced distress and ER. The researcher administered an interview schedule to explore emergent emotions and their intensity and to identify ER strategies employed by participants. The score is the participant’s self-rated distress level on a 1–6 scale, with higher scores indicating greater distress.
Procedure
The study was conducted per the guidelines of the Institute Ethics Committee (Behavioral Sciences Division), and data were collected between September 2022 and February 2023. Potential participants identified from medical records (individuals accessing in-patient/outpatient services at the institute) were contacted by the researcher and introduced to the study aims, procedures, duration, and the voluntary nature of participation. Those willing to participate provided written informed consent after the researcher explained potential risks, benefits, confidentiality measures, and their rights as participants. Following screening and informed consent (Figure 1), participants underwent individual testing in a quiet room free of distractions, with a predetermined order of tests. Assessments were scheduled at mutually convenient times to maximize engagement, with breaks offered according to participants’ preference to minimize fatigue. The EF tasks required approximately 30 (±10) min, while the ER assessments, including the state-based measure, required 40 (±10) min. A single examiner conducted all assessments. The first author, a clinical psychology trainee with appropriate training, supervision, and experience, minimized tester effects. Following Cyberball, participants were debriefed to clarify its purpose and address any persisting emotional effects.
Statistical Analysis
Data analysis was conducted using the software packages STATA 15 29 and Jamovi version 2.3.26, 30 which were used to calculate effect sizes for each variable. The normality of data was tested for all variables using the Shapiro–Wilk test. Group comparisons were done using t-tests for normally distributed data and the Mann–Whitney U-test for non-normally distributed data. The effect size was estimated using Cohen’s d and rank-biserial correlation, respectively, for parametric and nonparametric tests. Cohen’s d was selected for parametric tests due to its ability to quantify the magnitude of mean differences, which is relevant when comparing EF and ER in clinical and nonclinical populations. The rank-biserial correlation was utilized to compare quantitative variables using a nonparametric test, as it is well-suited for assessing the strength of associations in datasets that do not meet parametric assumptions. Based on the normality of data, Pearson’s correlation test and Spearman’s rank-order correlation test were used for correlation analysis.
Results
Sample Characteristics
Supplementary Table 1 illustrates the sociodemographic profile of all participants. The matched groups were predominantly female, with a mean age of 26 and approximately 16 years of education. Most participants in both groups were students and unmarried. The clinical group also included some unemployed participants. Table 1 also presents the diagnostic and treatment details of the clinical sample. The clinical group had a median illness duration of 2 months, with about half the participants diagnosed with depression. The majority were outpatients on medication, predominantly selective serotonin reuptake inhibitors (SSRIs), with less than half receiving augmentation. The majority were also receiving psychotherapy. The clinical group also exhibited higher median scores on the PID-5 total score (clinical: 27; nonclinical: 12) and all domain scores except Antagonism and Psychoticism.
Sociodemographic (n = 54) and Clinical Profiles (n = 27).
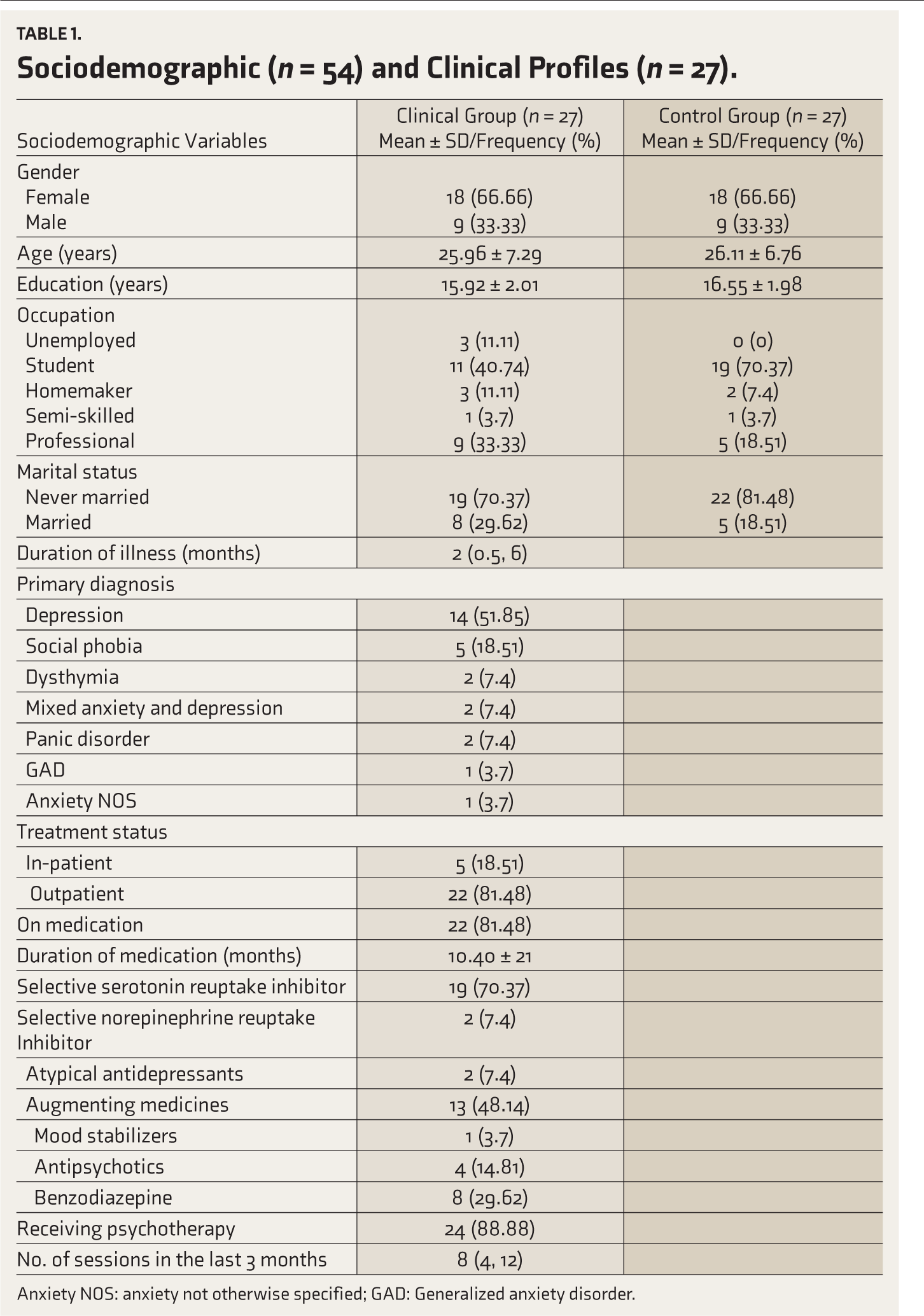
Anxiety NOS: anxiety not otherwise specified; GAD: Generalized anxiety disorder.
Comparison of the Performance of Clinical and Nonclinical Groups
Supplementary Table 2 illustrates the performance of both groups on EF tasks. The clinical group showed lower WM, verbal fluency, and RI. Based on standard effect size thresholds (small: ≤0.2; medium: 0.3–0.5; large: ≥0.8), 31 findings indicate a significant effect for WM, medium for verbal fluency, and moderate for RI. Table 2 also illustrates the ER profile of participants in both groups. The clinical group showed more severe difficulties in ER (Cohen’s d = -1.40; p =<.001). Regarding strategies, the nonclinical group reported greater use of refocus on plan, while the clinical group reported increased use of the negative ER strategy, catastrophizing.
Executive Function and Emotion Regulation Scores of the Clinical (n = 27) and Nonclinical (n = 27) Groups.
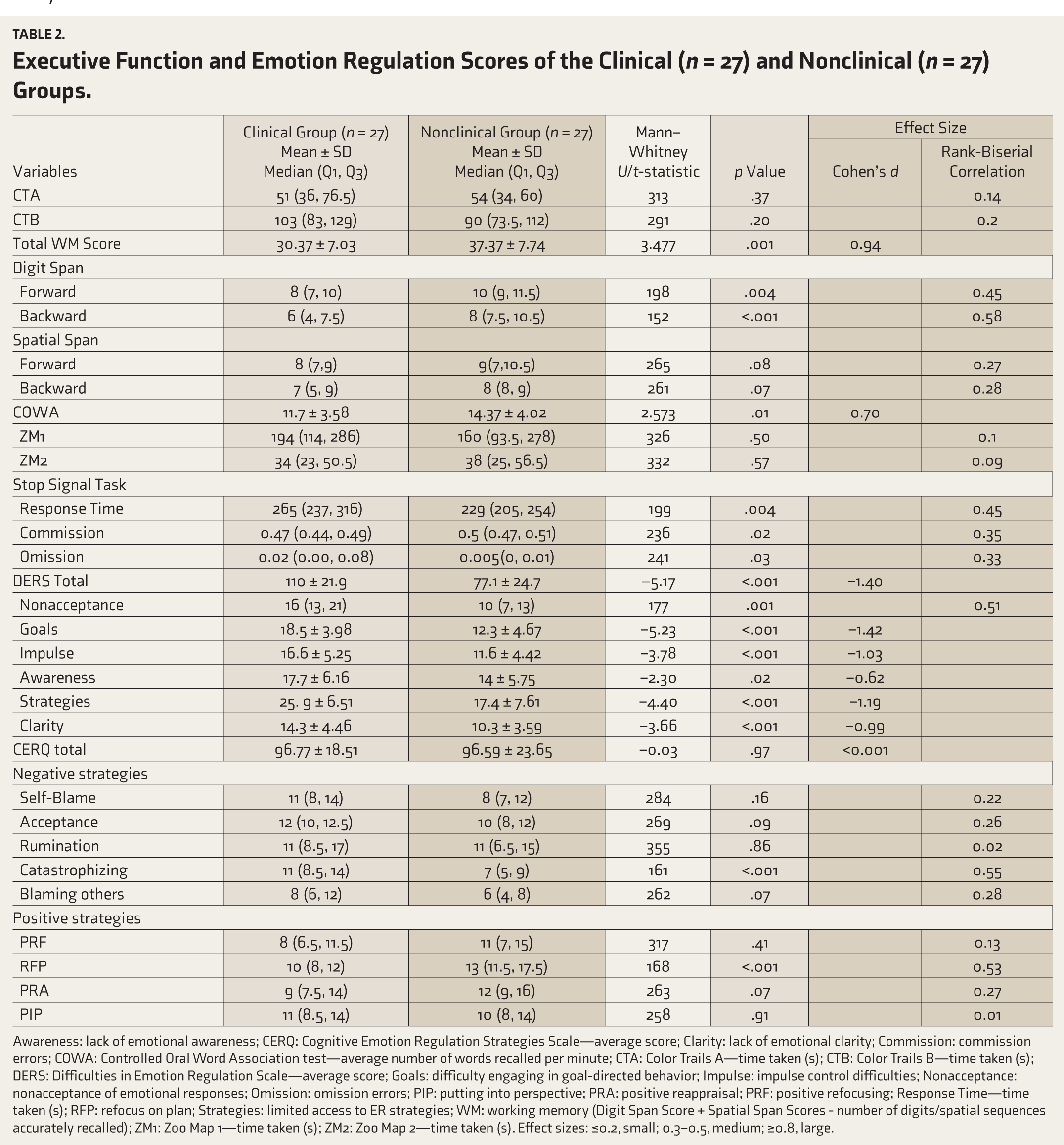
Awareness: lack of emotional awareness; CERQ: Cognitive Emotion Regulation Strategies Scale—average score; Clarity: lack of emotional clarity; Commission: commission errors; COWA: Controlled Oral Word Association test—average number of words recalled per minute; CTA: Color Trails A—time taken (s); CTB: Color Trails B—time taken (s); DERS: Difficulties in Emotion Regulation Scale—average score; Goals: difficulty engaging in goal-directed behavior; Impulse: impulse control difficulties; Nonacceptance: nonacceptance of emotional responses; Omission: omission errors; PIP: putting into perspective; PRA: positive reappraisal; PRF: positive refocusing; Response Time—time taken (s); RFP: refocus on plan; Strategies: limited access to ER strategies; WM: working memory (Digit Span Score + Spatial Span Scores - number of digits/spatial sequences accurately recalled); ZM1: Zoo Map 1—time taken (s); ZM2: Zoo Map 2—time taken (s). Effect sizes: ≤0.2, small; 0.3–0.5, medium; ≥0.8, large.
Analysis of Situational ER in the Clinical (n = 27) and Nonclinical (n = 27) Groups
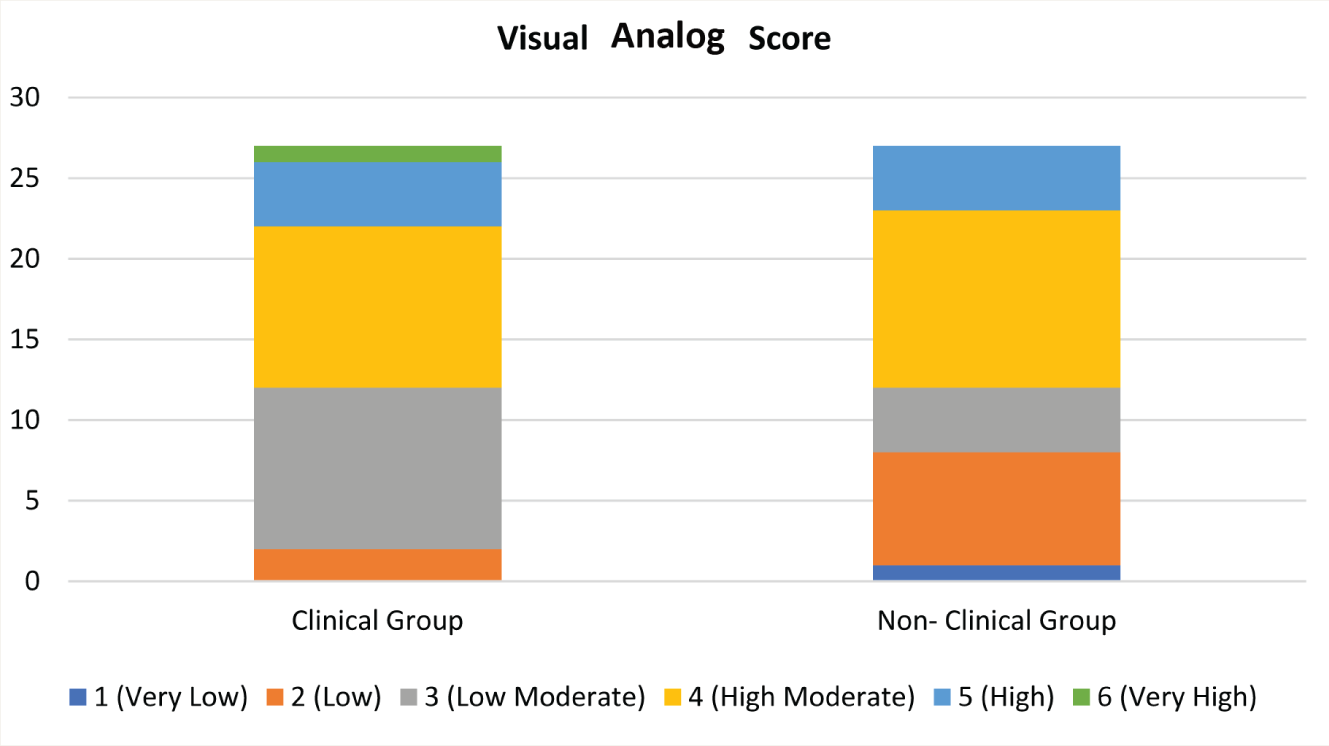
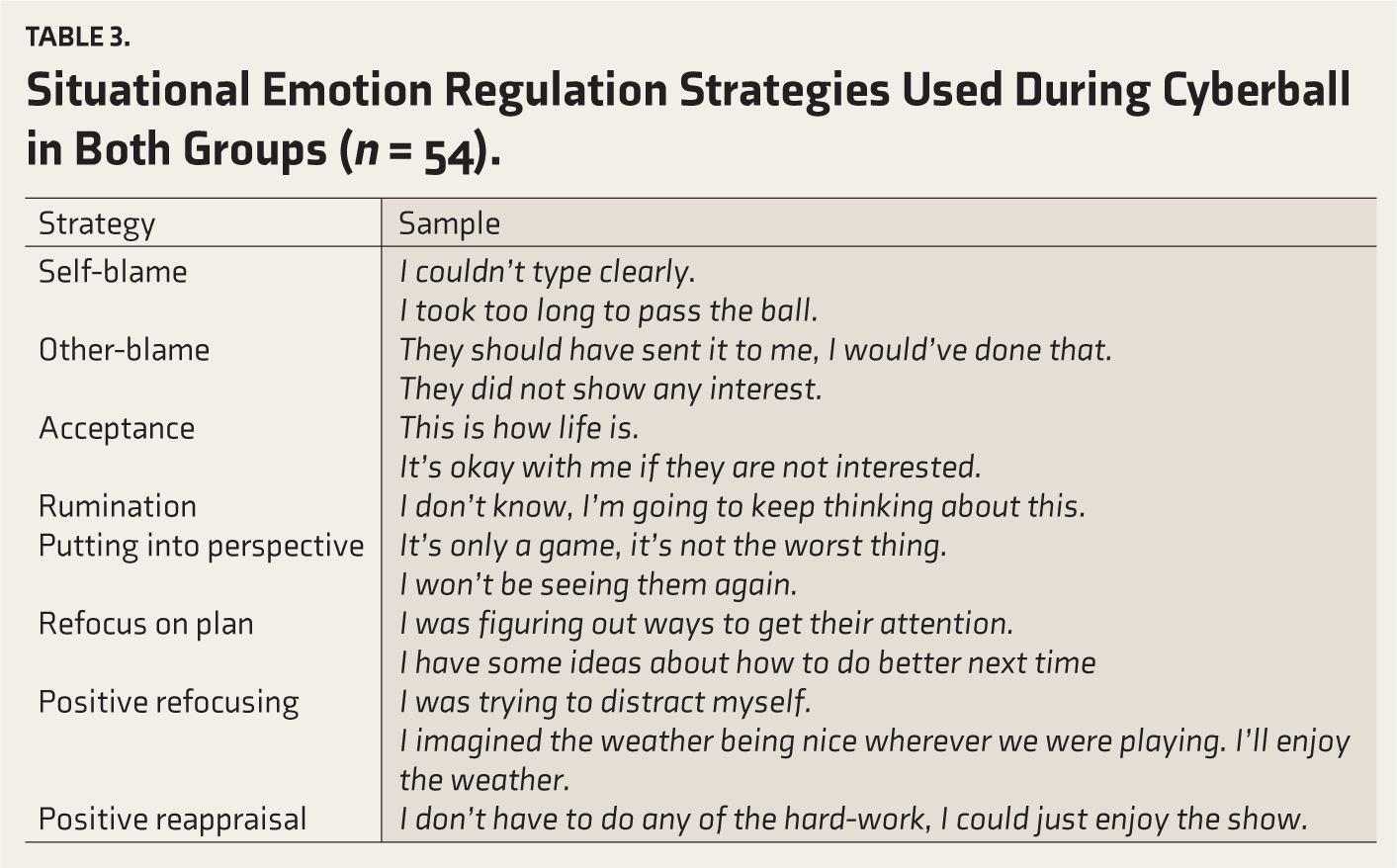
Figure 2 shows that following the Cyberball task, the nonclinical sample predominantly rated distress as low to moderate, with no ratings of very high, while the clinical group predominantly rated distress as moderate, with no ratings of very low. Table 3 shows the ER strategies described by participants following the Cyberball task. Figure 3 demonstrates that the clinical group used more negative ER strategies, whereas the nonclinical group used more positive strategies. Importantly, the clinical group did not report using PRA, an adaptive ER strategy. In contrast, the nonclinical group did not report the use of rumination, a maladaptive ER strategy frequently reported by the clinical group.
Distribution of Visual Analog Score of Distress During Cyberball in the Clinical (n = 27) and Nonclinical (n = 27) Groups.
Situational Emotion Regulation Strategies Used During Cyberball in Both Groups (n = 54).
Frequency of Emotion Regulation Strategies Used in Clinical (n = 27) and Nonclinical (n = 27) Groups.

Correlation of Severity of Deficits on ER with Performance on EF Tasks
Table 4 shows a significant correlation, with lower scores on WM associated with greater difficulties on ER (Spearman’s p = –0.371; p = .006).
Correlation Matrix of the Severity of Emotion Regulation Deficits and Emotion Regulation Strategies with Performance on Executive Function Tasks.
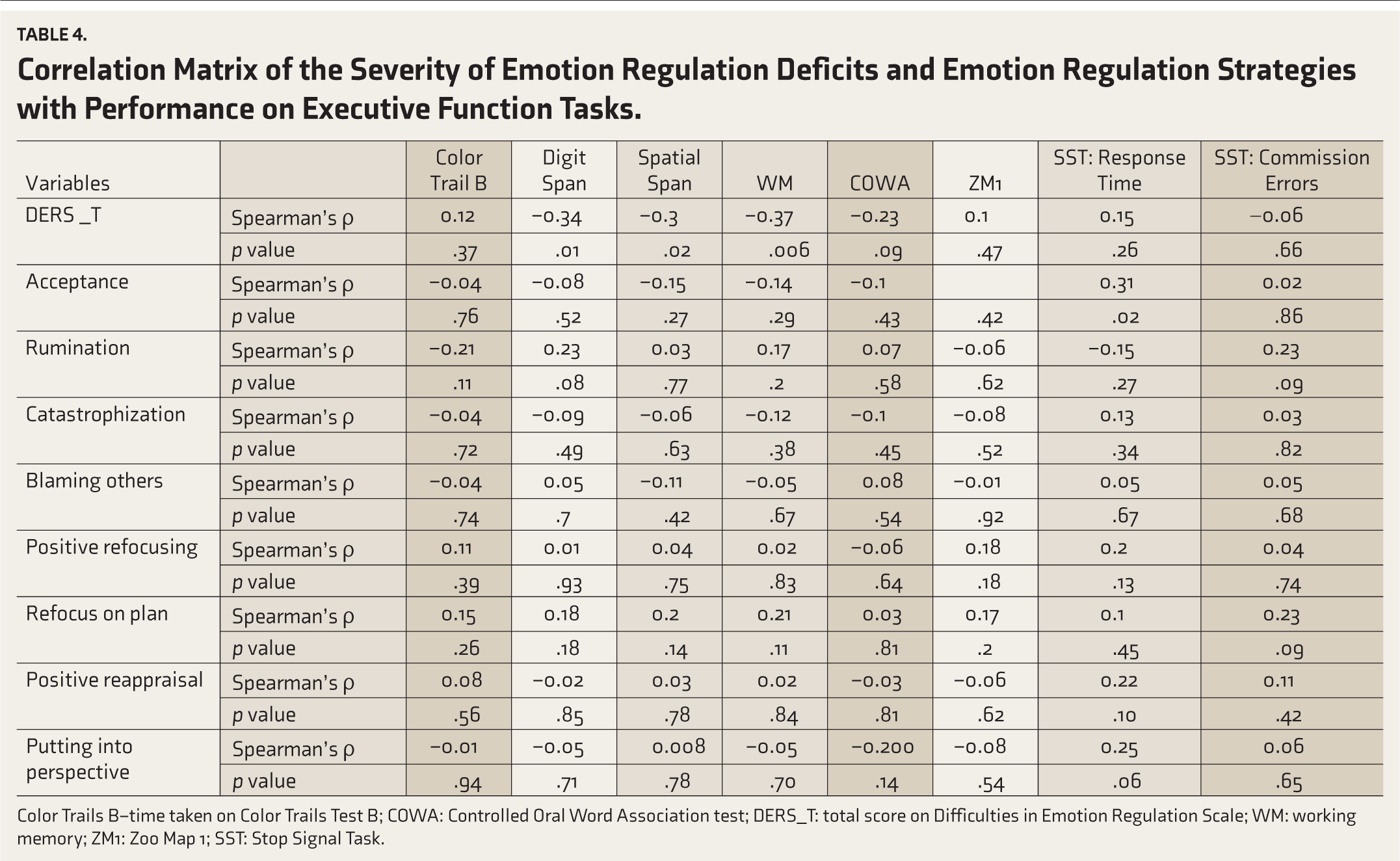
Color Trails B–time taken on Color Trails Test B; COWA: Controlled Oral Word Association test; DERS_T: total score on Difficulties in Emotion Regulation Scale; WM: working memory; ZM1: Zoo Map 1; SST: Stop Signal Task.
Correlation of ER Strategies with Performance on EF Tasks
Table 4 also shows a significant correlation, with slower response times on the EF measure of the SST being associated with higher acceptance levels as an ER strategy (Spearman’s ρ = 0.316; p = .02).
A post hoc power analysis of the study, with a significant difference in WM of 7 points and a standard deviation of >7, showed that the study had a power of 93% for an effect size of 0.95.
In summary, the results highlight group differences in EF and ER (as per H1), with the clinical group exhibiting significant deficits in WM and verbal fluency, increased severity of ER difficulties, and use of maladaptive ER strategies, particularly under situational distress. We did not find the expected associations between WM and PRA (H2); however, inhibitory control, as indicated by slower response times, was associated with the ER acceptance strategy.
Discussion
The present study aimed to compare EF and ER between clinical and nonclinical groups, explore situational ER, and examine the relationship between EF and ER within the sample. Findings demonstrate that the nonclinical sample demonstrated better EF and ER, with specific associations between EF and ER (inhibitory control and acceptance of ER strategy, but not between WM and PRA, as hypothesized). These findings provide insights into the cognitive and emotional profiles of individuals with CMDs, supporting the perspective that deficits in EF and ER play a central role in these disorders. By documenting these shared transdiagnostic impairments, the study adds to the theoretical understanding of CMDs as disorders of impaired self-regulation. It highlights implications for developing integrative therapeutic approaches targeting cognitive and emotional domains.
EFs
The clinical group’s performance on EF tasks aligns with findings from several studies, 32 and is comparable to Indian studies with a similar sample. 25 The clinical group demonstrated poorer performance across all EF tests, consistent with research linking EF deficits to CMDs. 6 Performance was correlated with the severity of symptoms. The nonclinical group outperformed the clinical group in WM, aligning with previous studies highlighting impaired WM in CMDs. 6 The observed large effect size for WM underscores substantial impairment in the cognitive processes required for holding and manipulating information among individuals with CMDs. Difficulties in WM have been linked with prominent symptoms of CMDs, such as difficulties with set-shifting, rumination, and lower use of adaptive ER strategies. 33 This may hinder the ability to manage complex tasks, follow conversations, or adapt to changing demands. 34 Consequently, WM has been chosen as a treatment target in cognitive training.
The medium effect size for verbal fluency highlights notable impairments in cognitive processing and linguistic skills. This finding is supported by research demonstrating reduced verbal fluency and cognitive impairment in psychiatric conditions. 6 Linguistic skills, as evidenced by verbal fluency, are integral to broader cognitive functioning because they reflect the ability to retrieve and organize information efficiently. In CMDs, diminished verbal fluency may indicate underlying deficits in executive processes such as cognitive flexibility, processing speed, and inhibitory control. 35 These impairments can affect communication and social interactions, which may, in turn, affect help-seeking and social support, compounding socio-emotional challenges. Regarding RI, as assessed by the SST, the clinical group took significantly longer to respond, suggesting potential RI difficulties. The moderate effect size for RI suggests that while inhibitory control deficits are less pronounced, they are relevant for understanding maladaptive ER strategies observed in this population. Existing research also links poor RI with impaired stress regulation 13 and greater difficulties with rumination. 36 Interestingly, the clinical group’s slower response times were associated with more omission errors, while the nonclinical group made more commission errors. Typically, commission errors suggest inhibitory difficulties, while slower response times may indicate a cautious response style. 37 This aligns with research indicating that individuals with CMDs often adopt a cautious approach, potentially reflecting heightened self-monitoring or anxiety about making errors. 38 However, this strategy may compromise efficiency, leading to lapses in attention and subsequent omission errors. This pattern highlights the need to address sustained attentional control in interventions, as these deficits can exacerbate daily functioning and ER challenges.
ER
The clinical group displayed higher median scores across all ER domains, suggesting more pronounced difficulties. 8 This aligns with studies emphasizing greater ER difficulties in clinical populations. 37 The clinical group tended to engage in negative ER strategies on the trait-based measure, while the nonclinical group utilized positive ER strategies more often. The inclination toward catastrophization was significantly higher in the clinical group, as consistently corroborated by existing research. 39 Conversely, the nonclinical group showed significantly higher use of the positive ER strategy of refocus on plan, which is associated with resilience and positive mental health outcomes. 39 The present study employed a mood-induction task, followed by an interview, to explore situational ER—a method infrequently used in prior clinical research. In contrast to the predominant reliance on self-report measures or less immersive methods of mood induction, 14 this approach offers a nuanced examination of ER in real-time contexts. The study aimed to demonstrate the complexities of adaptive ER in response to situational demands by placing participants in a simulated social scenario and assessing their emotional responses. Situational mood induction provides a unique opportunity to observe ER in action, allowing for direct observation of how individuals modulate their emotions in response to specific environmental cues instead of trait ER.
The clinical group rated significantly higher levels of distress compared to the nonclinical group. Nearly three-quarters of the clinical group reported moderate distress (rated 3 or 4), while only about half of the nonclinical group reported the same. None from the clinical group reported very low distress (rated 1), while none from the nonclinical group reported very high distress (rated 6). These findings confirm that individuals with CMDs have difficulties regulating unpleasant emotions, leading to possible amplification and persistence of these emotions and reduced access to positive emotions, as indicated by existing research.8,9 The absence of minimal distress ratings further underscores the heightened emotional reactivity and distress experienced by these individuals. Both groups predominantly used self-blame on the situational measure, consistent with prior research suggesting a self-blaming tendency as a way of ER in individuals with psychiatric conditions.22,40 The clinical group also relied significantly on other-blame following mood induction, despite a low score on this strategy on the self-report CERQ. While this contrasts with some findings, 40 it may be influenced by social desirability within a collectivistic culture. Collectivistic cultures may encourage adaptive interpretations of strategies such as acceptance and self-blame to prioritize interpersonal harmony, which may be considered maladaptive in Western contexts. 41 For example, shame is often cultivated in India to promote self-improvement–self-blame is used as a constructive strategy for personal growth, helping individuals align with communal expectations. 42 Hence, the cultural context may contribute to downplaying strategies like other-blame on self-report measures while favoring more socially acceptable responses, such as self-blame, although situational measures may reveal otherwise. Such discrepancies highlight the contrast between self-reported trait measures and situational responses reported during the mood-induction task, where the participants may have reacted differently due to the immediacy and dynamic nature of the task. These findings support literature recommendations to use both trait- and state-based measures, as ER at these two levels can interact to produce different outcomes, such as trait strategies moderating the effects of state regulation. 8 Furthermore, despite similar scores for rumination on the CERQ, the nonclinical group did not demonstrate its use on the situational measure, aligning with previous 22 findings of significant differences between clinical and nonclinical groups. This suggests that state measures better capture group differences in ER strategy use, which may not be apparent through self-report alone.
Regarding positive strategies, PRA was reported exclusively by the nonclinical group, which is consistent with previous findings. 22 The absence of reported PRA in the clinical group confirms a significant limitation in their ability to utilize adaptive ER strategies. 9 PRA is an integral technique used across different schools of therapy, with a role in reframing negative appraisals to reduce emotional distress and enhance adaptive coping strategies. 43 The absence of PRA in the clinical group may explain their reliance on rumination, as noted in the situational measure. Studies suggest that by fostering adaptive reframing, PRA can counteract the maladaptive patterns of rumination. 44 Research has also shown that higher use of PRA is associated with decreased depressive symptoms, suggesting that the inability to engage in PRA effectively may be an important factor in the exacerbation of symptoms and the chronicity of these disorders. 8 Due to this, therapeutic approaches such as cognitive behavioral therapy often focus on teaching reappraisal skills. 8 In our study, not all participants had received psychotherapy, and among those who had, the number of therapy sessions ranged from 4 to 12, with possibly limited exposure to PRA techniques. Additionally, it was also noted that positive refocusing was found to be one of the least used strategies in both groups, across both measures—mirroring previous findings. 40
Our findings indicate that while several strategies may be available at a trait level, in emotionally provocative situations, the nonclinical group mainly relied on positive strategies in the moment, potentially contributing to their better modulation of distress duration. Moreover, the observed difference in distress ratings may suggest a potential threshold disparity between the groups, with the nonclinical group demonstrating a higher threshold for emotional distress that triggers rumination, as seen on the situational task.
This study attempted to understand these differences in the use of ER strategies at the trait and state levels. The situational and trait (CERQ) measurements revealed contrasting findings on negative strategy use between clinical and nonclinical groups. The trait scores significantly differed only for catastrophizing. Meanwhile, on the situational measure, the clinical group consistently reported higher use of negative strategies, aligning with their higher distress levels and existing research linking less adaptive ER strategies with CMDs. 9 This distinction between situational and trait findings is more pronounced in rumination. Despite nearly identical CERQ scores, the nonclinical group did not report the use of rumination during the situational measure. This may be due to their higher positive strategy scores, which suggest greater awareness and utilization of adaptive ER to buffer distress and promote well-being.8,22 These results reflect the nonclinical group’s ability to capitalize on adaptive ER techniques, contributing to their lower overall distress. Furthermore, the discrepancies in trait and state findings may highlight distinct processes in ER. Gross’s Process Model suggests that antecedent-focused ER operates before or during an emotion, while response-focused ER operates after. The former may explain trait ER, as it involves executing habitual patterns. Meanwhile, the latter may correspond to state ER, reflecting real-time strategies shaped by situational demands. 45 Findings from this study support this distinction. While trait ER indicated similar rumination levels across groups, only the clinical group engaged in it situationally. Likewise, despite reporting PRA as a trait strategy, they did not demonstrate its use situationally.
EFs and ER
The study utilized a cross-sectional design, which offers insights into the associations among these variables; however, it does not allow for inferences about causality or the direction of these associations. Findings suggest that individuals with higher severity of ER difficulties may experience compromised EF abilities, particularly in tasks assessing verbal and visual WM. The significant relationship between WM and ER difficulties underscores the importance of WM in facilitating adaptive ER. This finding is consistent with existing literature, 5 which indicates that individuals with better WM were more adept at appraising emotional stimuli impartially, leading to reduced emotional responsiveness. Conversely, impaired WM can hinder the CC required to appraise emotional stimuli objectively, leading to heightened emotional reactivity and reliance on maladaptive strategies. 13
However, contrary to our hypothesis, no significant associations between WM and PRA were identified. These results diverge from existing research. 46 However, these variables were not investigated in isolation. Moreover, other factors, such as individual differences in cognitive flexibility or emotional awareness, might account for the absence of a significant correlation. Cognitive flexibility, closely tied to WM, has been shown to influence the ability to shift perspectives effectively during reappraisal tasks. 47 Additionally, variations in emotional awareness might mediate the relationship between WM and PRA, as individuals with higher awareness can better identify and label emotions, facilitating positive strategies like PRA. 48 Advanced statistical techniques, such as mediation or moderation analyses, could clarify whether cognitive flexibility, emotional awareness, personality, metacognition, or other contextual variables mediate the observed relationships. Furthermore, longitudinal designs could track changes in these relationships over time, especially in response to interventions targeting WM or PRA. Such approaches help identify EF factors that may act as barriers or facilitators for maximizing therapeutic engagement and improving ER within therapy. 10
A significant association was found between acceptance, considered a maladaptive ER strategy according to the CERQ, and a measure of RI. Specifically, slower response times on the SST were related to higher acceptance levels. This suggests that individuals who respond more cautiously score higher on acceptance. These observations support previous research highlighting the interplay of ER and EF. 34 For instance, research indicates that deficits in WM hinder updating emotional information, leading to maladaptive strategies like rumination. 12 At the same time, poor RI may prevent the inhibition of intrusive negative thoughts. 49 Additionally, poor inhibitory control in mothers with CMDs correlated with weaker infant–mother bonding, suggesting that inhibitory control may be linked to many affective processes. 50 This provides preliminary evidence for integrating cognitive control (CC) training, especially targeting WM, with standard treatment to improve depressive symptoms. 51 Strategies such as acceptance and PRA implicate the presence of CC by way of effortful regulation, and as such, CC has been identified as an “active ingredient” in psychotherapy. 10
Strengths
The study’s cross-sectional design enabled a comparison of EF and ER between clinical and nonclinical samples. Although the study could not recruit the initially estimated sample. However, a significant difference of 7 was found in WM, and a post hoc power analysis demonstrated that the study achieved a power of 93%, indicating that, though the sample size was small, it had adequate power.
Limitations
The smaller sample size may limit the generalizability of these findings, although the effect sizes indicate meaningful differences. The majority (>80%) of participants in the clinical group were undergoing treatment with SSRIs and/or psychotherapy. Both treatments influence cognitive processing and ER, 52 further limiting generalizability, as this can bias EF and ER measures by masking or altering deficits typically observed in CMDs. Future studies with treatment-naïve individuals or controls for treatment duration and type will allow for subgroup analyses that will help clarify the nature of deficits. Relying on self-report measures for trait ER introduces potential limitations. While widely used and validated, these measures are susceptible to biases, 53 such as social desirability, which may lead individuals to downplay maladaptive ER strategies and overestimate adaptive ones, distorting results. While the Cyberball task is a well-established mood-induction tool, its ecological validity is limited. Generalizing findings from Cyberball requires caution. Real-world rejection often involves prolonged interactions, nuanced social cues, and contextual factors that this short-term digital interaction may not fully capture. This may be particularly relevant for individuals with CMDs, who may frequently experience chronic interpersonal stressors and social withdrawal. The task may overestimate ER abilities by focusing on a single instance of rejection or underestimate ER strategies like seeking social support. Nevertheless, it provides valuable insights into immediate ER processes, which can serve as a foundation for understanding more complex situational ER.
Future Directions
Future studies should prioritize recruiting more diverse samples, considering age, education, and treatment-naïve participants to enhance generalizability. In parallel, incorporating objective ER measures, such as physiological indicators (e.g., heart rate variability, skin conductance) or observational methods, can complement self-report data and reduce biases, as beyond comorbidity, other factors may influence EF and ER. For instance, personality disorders, especially those involving emotional dysregulation (e.g., borderline personality disorder), are strongly associated with deficits in EF. 54 Psychopathy, characterized by deficits in affective empathy and emotional processing, has also been linked to altered EF. 55 Additionally, those with cognitive challenges or emotional dysregulation may struggle with accurately assessing their ER processes. Furthermore, the identification of ER strategies during the situational measure relied on the researcher’s analysis of verbal reports, which may lack standardization and objectivity (although these were coded, analyzed, and reviewed according to standard qualitative analysis procedures). An objective measure for emotion induction and regulation could help address these limitations. In the long term, intervention research should study the efficacy of CC-based approaches in improving ER. Several studies have identified CC as essential for effective ER and suggested that it may be used as an adjunct to therapy. 10 Several existing methods have demonstrated promise, including the Paced Auditory Serial Addition Test, 56 Goal Management Training, 57 Integrated CC training, 58 and Mindfulness-based interventions, 59 which target deficits in EF, leading to better self-regulation of emotions and symptom reduction. Longitudinal studies can also track how interventions targeting EF—specifically WM—improve adaptive ER strategies like PRA over time, or mediational analysis can be used to explore linking factors.
Conclusion
The transdiagnostic findings of the study highlight significant EF and ER difficulties and a potential reciprocal relationship between them, emphasizing the need for tailored clinical interventions targeting specific cognitive impairments and promoting adaptive coping mechanisms. Additionally, as evinced by the differences between trait and situational measures of ER, it is essential to consider real-time ER in interventions. The study also highlights the critical role of cultural considerations in cognitive assessments, identifying the need to develop standardized procedures and norms to enhance the applicability of research findings to diverse populations. The study provides valuable insights into the cognitive and emotional differences between clinical and nonclinical groups, with implications for targeted interventions. Further research using longitudinal designs could deepen understanding of these relationships.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Data Availability Statement
Data will be made available on request.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding the Use of Generative AI
None used.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
The study has been approved by the Institute Ethics Committee (Behavioural Sciences Division), National Institute of Mental Health and Neurosciences (NIMHANS), No. Nimh/Do/Beh.Sc. Div./2021-22.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.