
Abstract
Background:
This study evaluated intramuscular (IM) ketamine’s efficacy and safety for rapid suicidal ideation reduction, addressing the critical need for fast-acting interventions in resource-limited settings where intravenous (IV) options are impractical.
Methods:
We conducted a pre-post-interventional study of IM ketamine (0.5 mg/kg) over one year after approval of the institutional ethics committee. Adult patients with suicidal ideation, as measured by the six-point Montgomery–Åsberg Depression Rating Scale-Suicidal Ideation (MADRS-SI), were included if their MADRS-SI score was >4. Post-injection monitoring of suicidal ideation and adverse effects (A/E) was done after two hours and on Days 1, 3, 7, 14, 21, and 28. A repeat injection of the same dose was given only if the MADRS-SI score became > 4 again. The paired-T-test and repeated-measure ANOVA test were used for statistical analysis.
Results:
Thirty-eight patients (mean age: 36.3 years) participated, with 66% diagnosed with major depressive disorder and a mean MADRS-SI score of 5.31. At two hours post-injection, the MADRS-SI score decreased by 4.13 points (78% reduction), with 76% (N = 29) of patients reporting no suicidal ideation (score 0–1). Of the 28 patients who completed a one-month follow-up, 89% (N = 25) maintained a reduction in suicidal ideation (mean reduction: 4.75 points). A total of 64% (N = 16) required only one injection, while 36% required multiple injections. Three patients did not recover even after six trials of ketamine. Among 21 patients who completed six months of follow-up, 8 (28%) patients had relapsed. A/E was reported in 87% of patients, with dizziness and sedation being the most common (57%). No serious or life-threatening adverse effects were noted.
Conclusions:
IM ketamine (0.5 mg/kg) is effective and safe for the rapid reduction of suicidal ideation.
This study evaluated the efficacy and safety of IM ketamine for suicidal ideation (SI). A significant reduction in SI (MADRS-SI≤4) was achieved within two hours in 79% of patients (N = 30), and this improvement was maintained at one-month in 89% of follow-up patients. These findings suggest IM ketamine offers a rapid, accessible treatment for SI in resource-limited settings.Key Messages:
Suicidal ideation represents a critical psychiatric emergency, with India reporting alarming increases in suicide rates (6.2% annual rise). 1 Current treatments—including conventional antidepressants, lithium, 2 and clozapine, 3 often require weeks to demonstrate therapeutic effects. 4 At the same time, electroconvulsive therapy (ECT) presents procedural and consent challenges. 5 This therapeutic gap underscores the urgent need for rapid-acting interventions. Ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, has emerged as a promising alternative due to its rapid antidepressant and anti-suicidal effects. While intravenous (IV) administration has been extensively studied, its requirement for hospitalization and anesthetic observation limits accessibility, particularly in resource-constrained settings. The intramuscular (IM) route offers distinct advantages, including simplified administration, reduced costs, and enhanced patient comfort, without compromising efficacy. 6
Existing literature primarily focuses on IV ketamine, but evidence for IM administration in suicidal ideation is limited. Prior research shows that ketamine is rapidly effective, but most studies used complex infusion protocols requiring medical supervision.7–9 To address this gap, we evaluate a practical, outpatient-based IM ketamine protocol, which examines the efficacy and safety of IM ketamine (0.5 mg/kg) across diverse psychiatric diagnoses, with particular attention to the speed of anti-suicidal response as the primary outcome, the duration of the therapeutic effect, and its safety profile in real-world clinical settings.
Unlike prior research, our study introduces novel elements: extended follow-up (six months), flexible dosing based on clinical need rather than fixed schedules, and inclusion of patients with co-morbidities typically excluded from previous ketamine trials. Our findings aim to establish IM ketamine as a feasible and accessible treatment for acute suicidality, particularly in resource-limited settings.
Methods
This was an open-label, prospective, non-randomized, single-arm interventional study (pre-post design). The study was approved by the institutional ethics committee and registered in the clinical trial registry. All patients aged between 17 and 55 years with suicidal ideation who presented to the psychiatry outpatient department (OPD) were assessed using the Montgomery–Åsberg Depression Rating Scale-Suicidal Ideation (MADRS-SI). Written informed consent was obtained from all participants after a detailed explanation of the proposed treatment and its advantages and disadvantages. The recruitment period was from June 2021 to December 2022 (19 months).
Assessment Criteria
Patients with current suicidal ideation and a MADRS-SI score ≥4 who gave consent for participation were included. Patients with severe medical and surgical illnesses such as cardiovascular disorders (stroke, heart attack, etc.), a present or past diagnosis of glaucoma or intracranial hypertension, pregnancy, hypersensitivity to ketamine, a diagnosis of schizophrenia, delirium, or a hemodynamically unstable status were excluded.
Procedure
Ketamine at a dose of 0.5 mg/kg body weight was given intramuscularly by the doctor without anesthetic supervision after taking baseline vitals like blood pressure (BP) and pulse rate (PR). We monitored changes in MADRS-SI scores, treatment-emergent adverse events (A/E), and changes in vital signs post-injection and in follow-ups. Post-injection monitoring was done at two hours, and on Days 1, 3, 7, 14, 21, and 28. A repeat injection was given if the patient acquired a MADRS-SI score ≥4 any time after the first injection, with a minimum 24-hour gap between two consecutive injections (maximum of up to six injections). The same evaluation process was repeated every time. During this period, participants were allowed to continue their ongoing and indicated first-line medications, and dose adjustments in ongoing medicines were made for some patients as needed. Patients were also followed for up to six months to document any self-reported recurrence of SI. Relapse assessments were incidental and not part of the original protocol.
Tools
The MADRS is a 10-item diagnostic questionnaire designed to measure the severity of depressive episodes in patients with mood disorders, along with assessing suicidal ideation. 10 It has high inter-rater reliability (intra-class correlation coefficients [ICCs] ≥ 96). 11 Suicide risk assessment rating can be done on a scale of 0–6, and severity increases with the score.
Data Analysis
Data analysis was performed using the social science statistics website, 12 along with Microsoft Excel version 2013. The study was done assuming a two-sided test of group effect at the α = 0.05 significance level and at the 95% confidence level. Changes in MADRS-SI scores and vitals after the first injection were confirmed by a paired t-test. The sustained effect of the first injection over a month was confirmed by a repeated measures analysis of variance (ANOVA) test.
Results
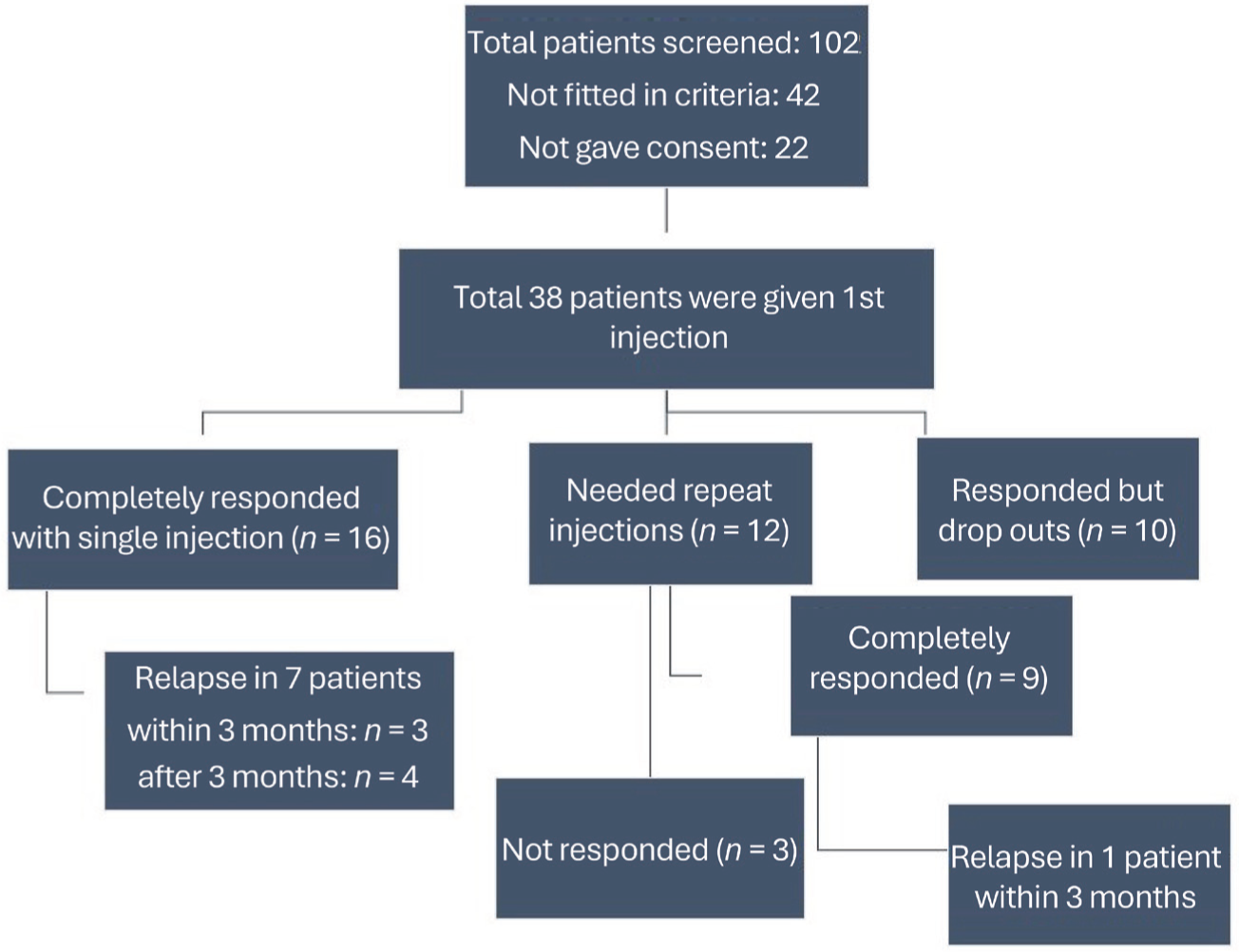
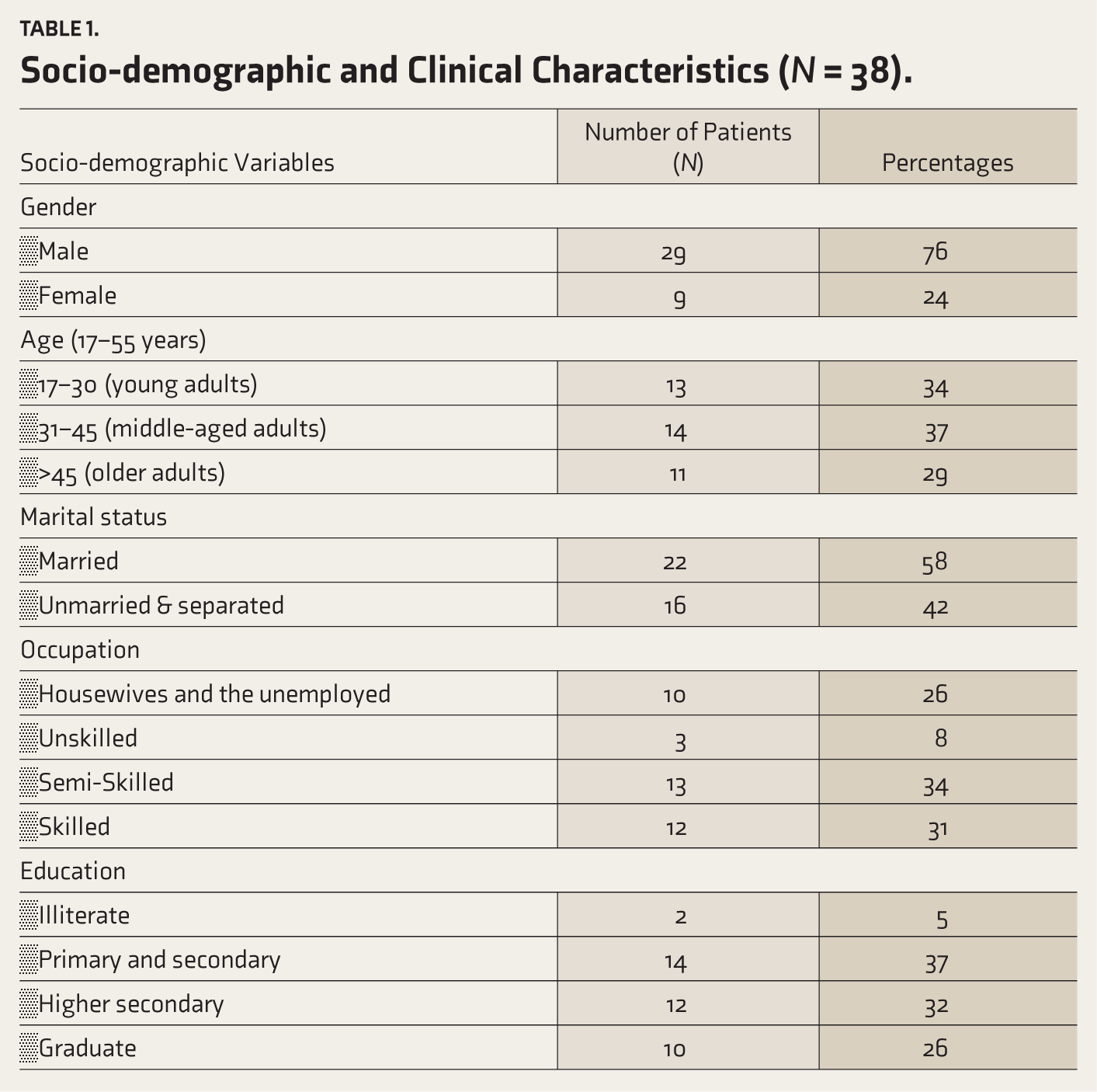
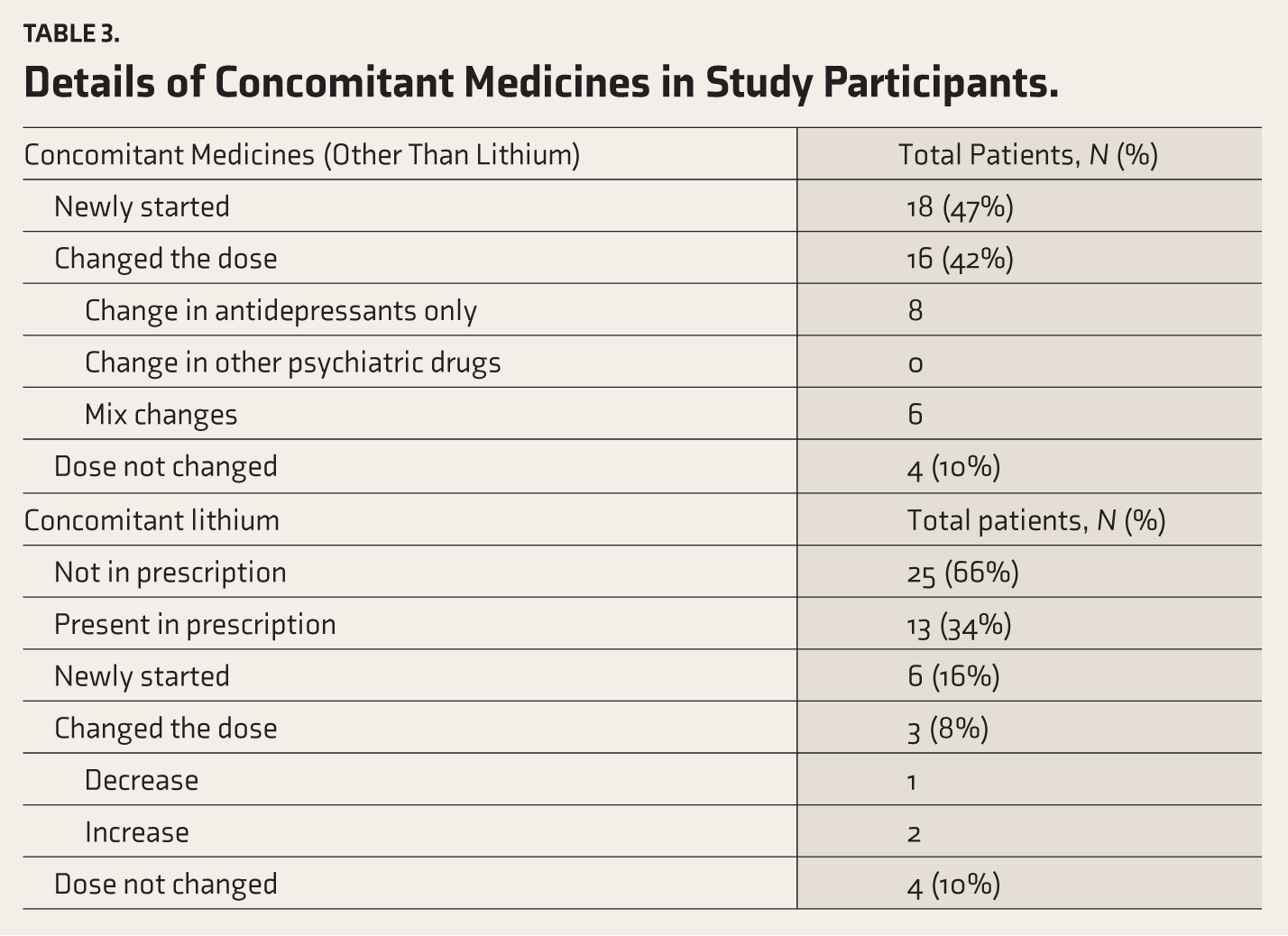
A total of 38 patients participated in the study (Figure 1). The majority of patients were male (76%), aged >35 years (mean = 36.3 years ± 5.2), married, educated (more than secondary schooling), had no medical co-morbidities, and no positive psychiatric family history (Table 1). The majority of patients (66%, N = 25) had major depressive disorder, including various specifiers, such as anxious features, psychotic features, dysthymia, along alcohol use (Table 2). A total of 52% (N = 20) of patients were already on medication. Among them, the majority required a change in medication according to their needs. In terms of lithium, 34% of patients had lithium in their prescription (Table 3). Moreover, a total of 16% (N = 6) of the patients had previously received ECT.
MADRA-SI: Montgomery-Asberg Depression Rating Scale-Suicidal ideation.
Socio-demographic and Clinical Characteristics (
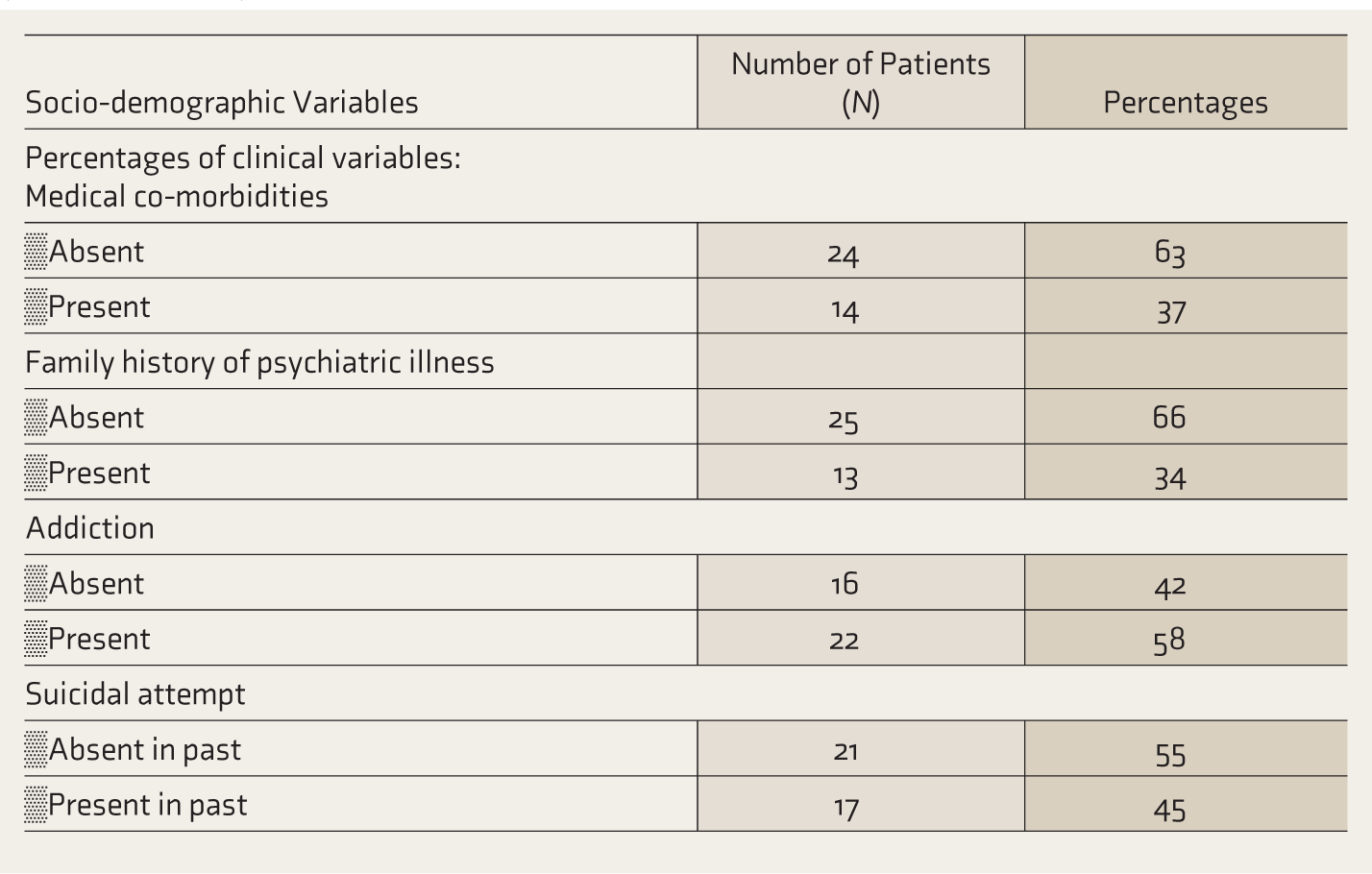
Clinical Diagnosis of Study Participants.
*MDD: Major depressive disorder; BMD: Bipolar mood disorder; OCD: Obsessive-compulsive disorder.
Details of Concomitant Medicines in Study Participants.
The mean pre-MADRS-SI score was 5.31 ± 0.60, which decreased to a score of 1.18 ± 1.10 points (mean reduction of 4.13 ± 0.50; 78% reduction), which was statistically significant (t value = -12.47, p < .001). A total of 92% (N = 35) of patients showed immediate improvement in two hours in the form of a decreased SI score, while 79% (N = 30) of patients had an SI score below 4 (full remission). A total of 76% (N = 29) of patients received a MADRS-SI score of 0–1 post-injection.
There were reductions in all mean vitals, PR, systolic BP, and diastolic BP with ketamine; among them, the mean reduction of 7.3 ± 3.6 pulses/min in PR was statistically significant (t = –3.2675, p = .01). Moreover, the reduction in vitals after ketamine was greater when patients had a history of alcohol use and hypertension compared to patients without these conditions.
Among the 38 participating patients, a total of 28 patients completed a one-month follow-up. Among them, 89% of the patients (N = 25) experienced a sustained anti-suicidal effect of ketamine for a month. This reduction was statistically significant (4.75 ± 1.30 points mean reduction; p < .001, F ratio value = 56.69) according to repeated ANOVA tests. The sustained effect of a single injection lasted up to one-month in 64% (N = 16) of patients and 36% (N = 9) of patients given multiple injections (Figure 1). Among the patients receiving multiple injections, two, three, and six injections were needed in six, two, and one patient, respectively. The mean number of injections per patient was 1.8 ± 1.2 (range: 1–6).
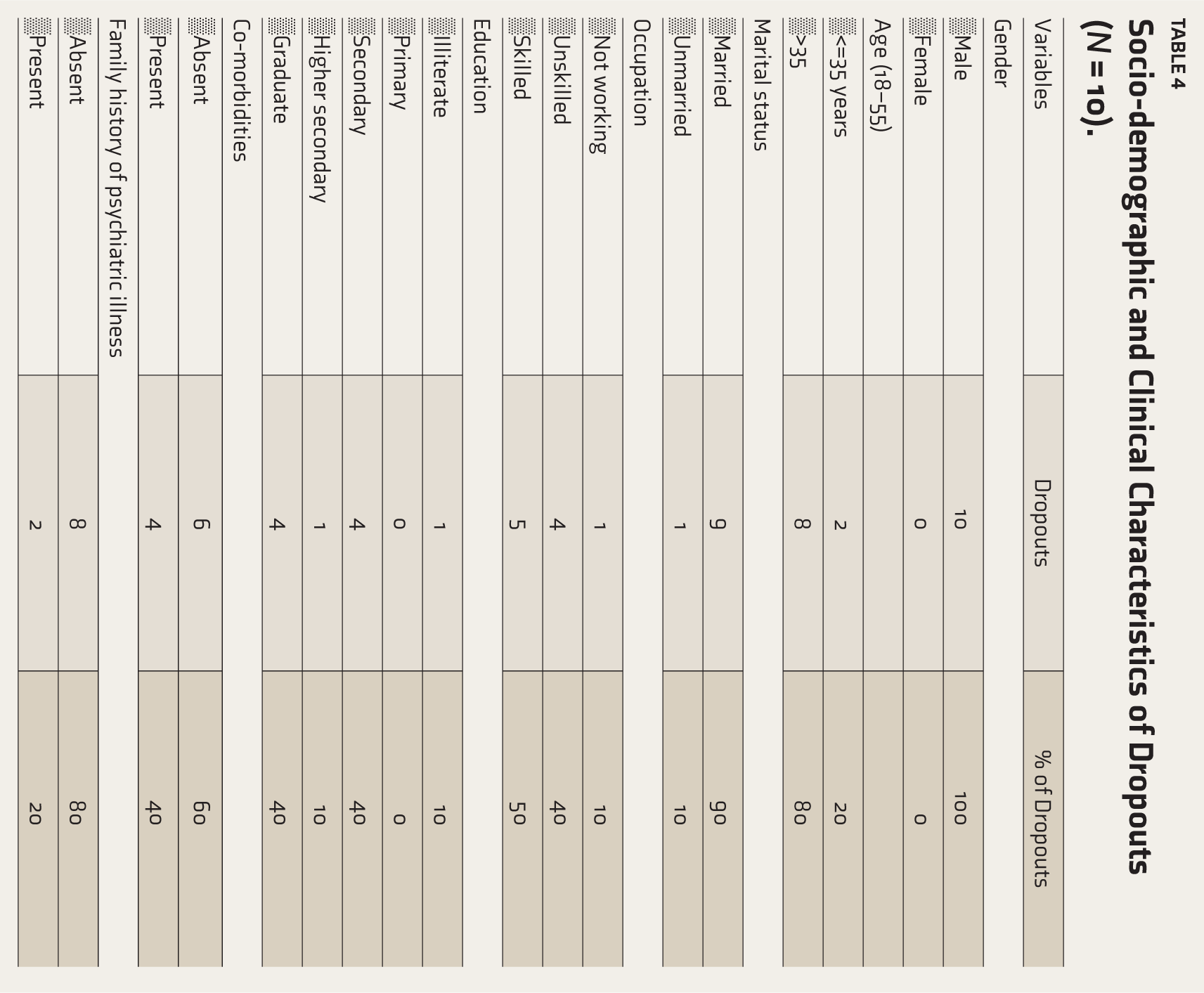
Among 21 patients completing a six-month follow-up, 28% (N = 8) reported SI recurrence (MADRS-SI score ≥ 4), with half occurring within three months. Factors associated with relapse include poor family support (N = 2), poor medication adherence (N = 1), substance use relapse (N = 1), and unresolved depression (N = 2). No suicide was reported during the follow-up. There was a total of 10 dropouts after the first injection (Table 4). Reasons for dropouts were restarting substance use/withdrawal delirium, ECT, side effects, and loss to follow-ups.
Socio-demographic and Clinical Characteristics of Dropouts (
Adverse effects were reported in 87% (N = 33) of patients (Figure 2), most commonly dizziness, sedation, heaviness of the head, dissociation, paresthesia, and numbness. Psychotic events, like muttering alone and auditory hallucinations, were also noted. Other adverse events were nausea, restlessness, a feeling that “the mind is not working or the mind is blank,” flashbacks, increased anxious thoughts, crying episodes, childish talk, talkativeness, blurred vision, mild body pain, conversion episode precipitation, and a feeling of dying. All adverse events subsided within two to three hours. They were mild and transient. No life-threatening or persistent adverse effects were noted. No suicide attempts occurred as an adverse event. There were no psychotic, manic, or dissociative symptoms indicated in patients with obsessive-compulsive disorder (OCD) and bipolar mood disorder (BMD). Moreover, ketamine was safely administered to patients with a maximum BP of 170/110 mmHg and a maximum PR of up to 115 beats/minute.
Adverse Event Frequency (%) Following Intramuscular Ketamine Administration (0.5 mg/kg).

Discussion
To our knowledge, this is the first published study to demonstrate the anti-suicidal effect of IM ketamine in such a large group (N = 38) of patients, regardless of diagnosis, within the Indian population. Moreover, this is the most extensive follow-up study published for this purpose. The main findings of our research are that there was a significant, rapid reduction in suicidal ideation within two hours with a fixed sub-anesthetic dose of IM ketamine injection, irrespective of diagnosis. Furthermore, IM ketamine is safe and can be given as an outpatient department (OPD) procedure, with no need for an anesthetic setup or anesthetic supervision while giving the injection. Additional findings indicate that the majority of patients responded immediately with a single injection only. The sustained effect lasted up to one-month in 64% of patients (N = 16) who received a single injection and in 36% of patients (N = 9) who received multiple injections. The infusion was safely given to patients with alcohol withdrawal, comorbid psychotic features, and patients with high BP up to 170/110 mmHg and PR up to 115 beats/minute.
The mean MADRS-SI score decreased from 5.31 ± 0.6 to 1.18 ± 1.1 within two hours of the first injection. Therefore, the average reduction was 4.13 ± 0.5 (78% reduction). A total of 92% of patients (N = 35) showed immediate improvement in two hours in the form of a decrease in SI score, while 79% of patients (N = 30) achieved an SI score below four. A total of 76% (N = 29) of patients received a MADRS-SI score of 0–1 post-injection. The case report by Harihar C, 13 also showed a 70% improvement in suicidality after two hours with a single IM ketamine (0.5 mg/kg) injection in one patient, while two injections were administered in another patient, compared to the 79% improvement in our study with a single injection.
A study of Price RB conducted on suicidal patients using the MADRS-SI scale, 7 also showed an average 2.08-point reduction of MADRS-SI scores within 24 hours. These reductions were sustained for 12 days by repeated-dose IV ketamine infusions, whereas in our IM study, a mean decrease of 4.13 points was observed within two hours. The reductions were sustained for one-month without the need for repeat injections in 57% of patients. In this study, 76% of patients received a rating of 0 or 1 after the IV ketamine injection, compared to 81% in Price’s study. The study by Larkin was conducted on 14 patients who presented to the emergency department with suicidal ideation, 14 irrespective of diagnosis, in a comparatively lower dose (0.2 mg/kg) of IV bolus ketamine over 1–2 minutes. They observed an 84% improvement in SI after 40 minutes post-administration, without any serious adverse events. Improvements were traced again after 10 days. A recent Randomized-Controlled Trial (RCT) conducted by Umesh Pathak in Madhya Pradesh in 2021, 15 using different doses, routes, and scales, also showed a 57% reduction in the Modified Scale for Suicidal Ideation (MSSI) score within six hours with IV ketamine infusion, which was significantly higher than the placebo group. The improvement in scores persisted for a week with two more repeated infusions.
A study by Can conducted on 32 adults with suicidal ideation found that six weeks of oral ketamine treatment in participants with chronic suicidality led to a significant reduction in suicidal ideation. 16 Sixty-nine percent of participants achieved improvement in the first six weeks, whereas 50% achieved a significant improvement by the follow-up 10-week time plot.
Here, we decided to administer repeated injections only when necessary, rather than following the popular schedule method,7–9 to better determine how long a single injection remains effective and the actual number of injections needed for a complete response.
Moreover, the use of ketamine as an anti-suicidal agent has focused on IV infusion administration of the drug. However, the drug has been safely administered intramuscularly, as an IV bolus, and orally, and it has shown a significant anti-suicidal effect.14,17–19 Tried doses of ketamine via different routes as an antidepressant, antianxiety, and anti-suicidal drug were 0.5 mg/kg daily for 4 weeks orally, 17 10 mg once a day for two to seven days sublingually, 20 0.1–0.5 mg/kg subcutaneously, 21 and 10% intranasally. 22
The most common adverse events reported in the Mocrane study with IV ketamine were sedation, dizziness, depersonalization/derealization, and nausea, 23 which were also observed in our study. However, in their study, only 10% of patients experienced these adverse events, whereas in our study, 87% of patients experienced adverse events. They did not include patients with psychotic symptoms and substance abuse. Patients with OCD, bipolar depression, benzodiazepine, and alcohol use disorder with suicidal ideation have been given ketamine injections safely in studies by Chilkuri, Anees Bahji, and Liebrenz, respectively.8,24,25 Studies by Krystal and Wan observed a slight dose-dependent increase in BP with IV Ketamine,26,27 while we observed a decrease in BP with IM ketamine, although not significant.
Clinical Application
A single-dose IM ketamine (0.5 mg/kg) is applicable for emergency care by providing rapid suicidal ideation reduction within two hours, effectively bridging the gap until conventional treatments take effect. Its utility in resource-limited settings is pronounced, as it requires no IV infrastructure or anesthesia, making it feasible in primary care clinics. Furthermore, for treatment protocols, its flexible “as-needed” dosing strategy is advantageous, reducing the number of injections and hospital visits while simultaneously minimizing the potential for dependence.
Limitations
Non-blinded assessment, non-randomized design, use of MADRS-SI (vs. dedicated suicidality scales), and small sample size may limit generalizability. Variations in ongoing medications and changes made to them may have led to treatment bias. A suicide risk assessment immediately before giving an injection would have provided more specific pointers.
Conclusions
A sub-anesthetic fixed dose (0.5 mg/kg), IM ketamine injection is effective and safe for the rapid reduction of suicidal ideation, irrespective of diagnosis. Nevertheless, larger controlled trials are needed to confirm efficacy. The effectiveness can persist for a month. Thus, we may give the injection as required when the risk of suicide re-emerges, rather than administering a fixed twice or thrice-weekly injection course for its anti-suicidal properties, which may ultimately reduce the risk of dependence. The brief efficacy is not necessarily a disadvantage here because the time bought could allow the implementation of other psychopharmacological and psychosocial interventions.
Supplemental Material
Supplemental material for this article available online.
Footnotes
Acknowledgements
I acknowledge Mr. Ebbie Thomas, Assistant Professor of the Department of Community Medicine, for his guidance in statistical analysis. I also acknowledge my hospital nursing staff and interns for helping me monitor patients.
Data Sharing Statement
Deidentified individual participant data will not be made available.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration Regarding Use of Generative Artificial Intelligence (AI)
We utilized AI-assisted tools (e.g., DeepSeek, grammar checker) for language editing and refinement. The research design, data, analysis and conclusions remain entirely the authors’ own work.
Ethical Approval
Approval by the Institutional Human Ethics Committee, GMERS Medical College, Gotri, Vadodara. (Approval number: BHR/21/2021; Approval date: June 9, 2021).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient Consent
Written informed consent was obtained from all individual participants included in the study.
Prior Presentation at a Meeting
In 51th annual conference of IPS-GSB at Indore, MP, as a paper presentation in August 2022 (as a continuing study).
Simultaneous Submission to Other Journal
No.
Trial Registration
Registered at Clinical trial registry-India (CTRI/2022/09/045713).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.